6.4-Homeostasis
1/40
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
41 Terms
When is BG conc higher than normal?
what happens in relation to insulin?
After a meal high in carbs, BG conc. is above normal
Detected by receptors on B cells- secrete insulin
Released into the blood and travels to target cells e.g liver and muscle
Insulin then binds to specific receptors on the target cell membrane
How does insulin cause a reduction in BG conc.? (4)
1) Increasing the uptake of glucose by the cells
2) Activate enzymes which convert glucose into glycogen (in the liver and muscle cells which can then be stored)- glycogenesis
3) Activates enzymes which convert glucose to fats for storage
4) Increasing respiration rates in cells
how does glucose usually enter the cell?
what is present in the cell’s cytoplasm?
how does insulin increase the uptake of glucose by cells?
Glucose usually enters cells by facilitated diffusion through specific channel protein molecules
extra channel protein molecules are present in the cells cytoplasm
insulin causes these to be inserted into the cell membrane, so the permeability increases
What happens if BG conc. is lower than normal?
what is the main target cell of the hormone?
what does glucagon do?
Islets of Langerhan detect fall in BG conc. and a cells secrete glucagon
Hormone’s main target cells are liver cells
Glucagon binds to specific protein receptors on the target cell membrane
How does glucagon cause an increase in BG conc?
1) Activating enzymes which catalyse the conversion of glycogen into glucose- glycogenolysis
2) Stimulates conversion of amino acids and glycerol to glucose- gluconeogenesis
What is the role of adrenaline in controlling BG conc? i.e when is it released and what does it do?
Secreted from adrenal glands when BG conc is low, during stress and during exercise
Binds to receptors on the cell membrane of liver cells
How does adrenaline increase the BG conc?
1) Activates enzymes that causes conversion of glycogen to glucose- glycogenolysis
2) Inactivates enzymes that synthesis glycogen from glucose- glycogenesis
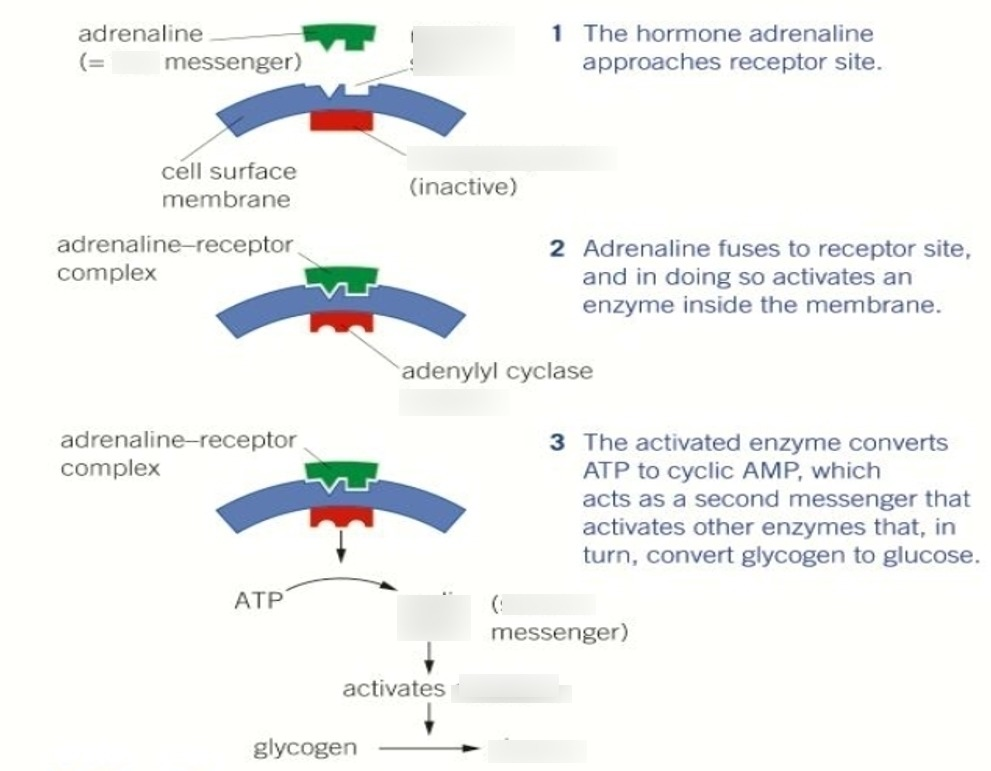
What is the second messenger model of hormone action?
Both glucagon and adrenaline act via a second messenger
How adrenaline causes glycogenolysis:
1) Adrenaline approaches receptor site on liver cell
2) Adrenaline attaches to receptor site, and so activates the enzyme adenylate cyclase inside the membrane
3) The activated adenylate cyclase converts ATP to cyclic AMP (cAMP) which acts as a second messenger that activates the enzyme kinase A
4) Kinase A activates a chain of reactions that breaks down glycogen to glucose (glycogenolysis)
What are the two main functions of the kidneys?
1) Excretion i.e. filtration of the blood to remove urea
2) Osmoregulation i.e. maintaining the blood at a constant water potential- e.g of homeostasis
What is a nephron?
Each kidney is made of about one million fine tubules called nephrons
It is the functional unit of the kidney
What occurs during ultrafiltration?
High hydrostatic pressure in glomerulus (afferent wider than efferent)
Pushes water and smaller molecules e.g. glucose, urea and amino acids through the basement membrane then through the podocytes
Large molecules e.g red blood cells, plasma proteins and platelets are too large to pass through
what carries out selective reabsorption?
why do these cells have many microvilli and mitochondria
what is reabsorbed and why?
what are the transport processes involved?
1) Carried out by cells lining the PCT
2) microvilli - increase SA for reabsorption of glucose from PCT
mitochondria- ATP for active transport
3) these substances reabsorbed by pct cells are those which the body needs e.g. glucose and water (and Na+ and amino acids)
4) Reabsorption of solutes is by a combination of active transport and facilitated diffusion
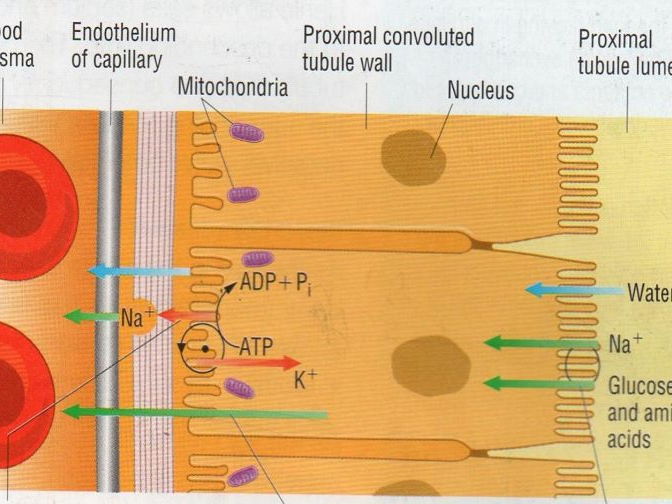
What happens during the reabsorption of glucose?
Na+ leave PCT cells and enter blood- sets up conc. gradient of Na+
Glucose and Na+ ions enter the PCT cells together from the filtrate using specific carried proteins (co-transport)
Glucose leaves the PCT cell at the other end via a carrier protein and enters the blood flowing through the efferent arteriole
Low glucose conc, in efferent arteriole + higher conc. in PCT cell- glucose enters blood by facilitated diffusion
What is the role of the loop of Henle in the maintenance of a Na+ gradient in the medulla?
what then happens to the water?
what does the gradient of Na+ in the medulla do?
1) Top of AL- Na+ and Cl- leave by active transport
Impermeable to water + low WP in tissue fluid- greater conc. of Na+
DL- water moves out by osmosis and enters tissue fluid
Filtrate of DL more concentrated- lowers water potential
Permeable to water, but impermeable to Na+ and Cl-
2) Water in tissue fluid of medulla reabsorbed into blood capillaries by osmosis
3) allows water to be reabsorbed from collecting ducts
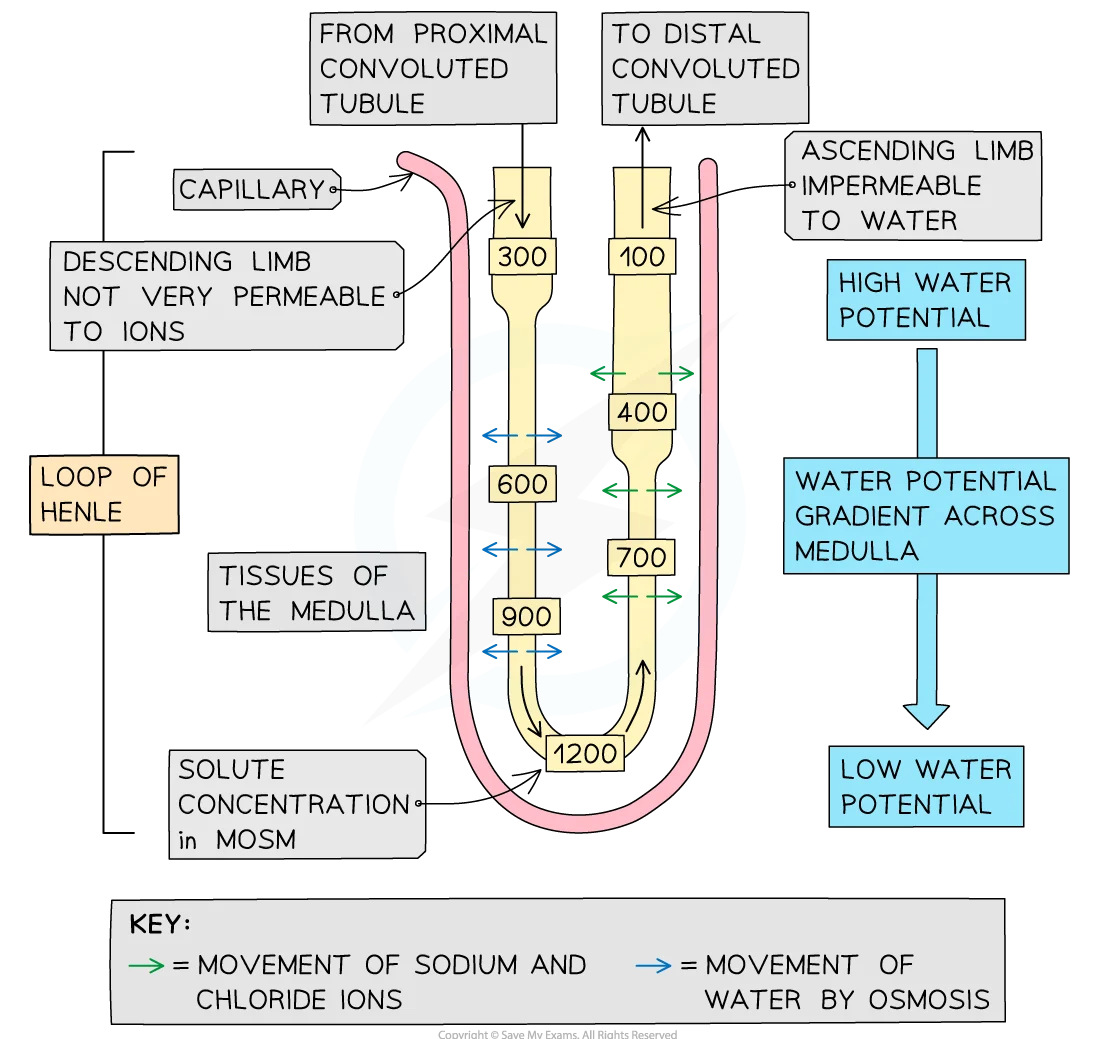
What is the loop of Henle known as and why?
what happens as the deeper into the medulla the loop of Henle goes,
Countercurrent multiplier as the fluid flows in opposite directions in the two sides of the loop
the more there is a chance of creating a low water potential
Where does the filtrate move into next?
DCT and then the collecting duct
The tissue fluid is more concentrated and lower water potential. What does this allow?
Water to move out of the filtrate in the collecting ducts by osmosis, into the medulla and to be reabsorbed by the vasa recta
What does it mean if the loop of Henle is longer?
More water can potentially be reabsorbed from the filtrate into the blood
what is osmoregulation?
What are some ways in which water can be lost from the body?
1) homeostatic mechanism that controls water potential of the blood
2) Sweating
Egestion
Lactation
Exhalation
Urination
Where is ADH synthesised?
where is ADH stored?
In the hypothalamus
In the posterior pituitary
What happens after eating a salty meal or sweating a lot?
WP drops (becomes more negative)
Osmoreceptors in the hypothalamus detect this and release more ADH
ADH makes cells of collecting duct more permeable to water
Lower WP causes water to move by osmosis from the filtrate
As a result, a small volume of concentrated urine is produced
Helps the body to conserve water
What happens after a lot of water has been drunk?
WP of the blood increases (becomes less negative)
Osmoreceptors detect this and release less ADH
ADH causes cells of collecting duct to become less permeable to water
Far less water is reabsorbed by osmosis into the blood
As a result, large volumes of dilute urine is produced
Helps the body to excrete excess water
How does ADH increase the permeability of the collecting duct and DCT cells?
By increasing transcription and insertion of aquaporins into the membranes of these cells
What are aquaporins?
Protein water channels that allow water molecules to move down their WP gradient and out into the medulla and then into the vasa recta, incerasing the amount of water reabsorbed from the filtrate
What happens to the aquaporins when ADH levels fall?
They are removed from the membranes and the collecting ducts becomes less permeable to water
3 symptoms you would expect to find in a person with a lack of ADH
dehydration, frequent urination, discoloured urine
what is the cause of type 1 diabetes?
when does it usually appear?
why is it an autoimmune disease?
inability to produce insulin
childhood
body’s own immune system may destroy the B cells
what is the treatment for type 1 diabetes?
BG must be monitored regularly- can be done using a glucose biosensor
insulin injections
manage diet + exercise
why can insulin not be given orally in tablet form?
insulin is a protein and will therefore be hydrolysed by proteases in the stomach and SI
what is the cause of type 2 diabetes?
what is it often linked with?
what are some other risk factors?
gradual loss of responsiveness of target cells to insulin due to receptor abnormalities
obesity
age, lack of exercise and poor diet
what is the treatment for type 2 diabetes?
careful regulation of diet esp sugar intake + balance exercise
insulin injections may be necessary
what are some diagnostic features of diabetes?
High concentrations of BG
Persistent thirst
Frequent urination
Craving for sweet foods
what is gluconeogenesis?
what is glycogenesis?
what is glycogenolysis?
formation of glucose from non carb sources e.g. amino acids and glycerol
formation of glycogen from glucose in the liver
the breakdown of glycogen into glucose in the liver
what is homeostasis?
maintenance of constant internal environment (within certain limits) despite changes in the external environment
what happens if blood pH is too high or too low OR if the core temp is too high
enzymes become denatured
hydrogen bonds that hold tertiary structure can be broken, changing the shape of the active site
ES complexes can’t be formed and enzyme no longer works as catalyst
metabolic reactions less efficient
why is high BG potentially dangerous?
why is low BG potentially dangerous?
1) Decreases WP in blood- cells dehydrate
Water enters blood by osmosis from tissue- increase blood pressure
2) Less ATP released from respiration
WP increase- decrease blood pressure
what is a negative feedback system?
why is there a set point?
what do negative feedback systems maintain?
1) A change from a set point is detected and this brings about physiological mechanisms to return to the set point
2) acts as a target value or "normal range" for internal conditions (like temperature or blood pressure), enabling the body to maintain stability and function optimal
3) maintains the value of an important physiological variable e.g core temperature set point of 37C
what is a positive feedback system and what does it do?
Not homeostatic mechanism, it’s a mechanism for change
Any change away from norm creates more change
Core temperature drops below 37C, mechanism develops that makes temperature fall even further
what are the three sources that blood glucose comes from?
Directly from the diet
From the hydrolysis of glycogen stored in muscle and liver- glycogenolysis
Production of glucose from amino acids and/or glycerol- gluconeogenesis
what is the role of the pancreas?
what are the two types of islet cells and what do they do?
Contains Islets of Langerhans- contain receptors that are sensitive to changes in BG concentration
A cells- produce hormone glucagon in response to low BG
B cells- produce hormone insulin in response to high BG
what are hormones produced by, and where are they transported to in the blood?
what makes a receptor protein specific?
1) produced by endocrine glands and transported in the blood to target cells in other organs of the body
these target cells have specific receptor proteins
2) hormone with complementary shape will be able to bind to receptor’s specific binding site