dementia and delirium
1/32
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
33 Terms
normal aging
mild changes in memory and rate of information processing
deficits are generally not very progressive and usually do not affect daily function
learning or acquisition performance declined uniformly w/increasing age
delayed recall or forgetting remained relative stable w/aging
dementia
disorder characterized by impairment of cognition typically involving memory and at least one other cognitive domain (language, visuospatial-connection/sequencing, executive function)
must represent a decline from previous level of function and be severe enough to interfere w/daily function and independence
7th leading cause of death
dementia presentation
difficulty in
retaining new information
handling complex tasks
reasoning
spatial ability and orientation
language
behavior
dementia prevalence
more than 55 mil have dementia worldwide
every year there are nearly 10 mil new cases
currently the seventh leading cause of death
in the US, 1 in 3 seniors dies w/alzheimer’s or another dementia
dementia causes
neurodegenerative disease
alzheimers disease
dementia w/lewy bodies
frontotemporal dementia
parkinson disease dementia
less common neurodegenerative disorders (ex: Huntingtons disease)
non-neurodegenerative dementia (vascular dementia)
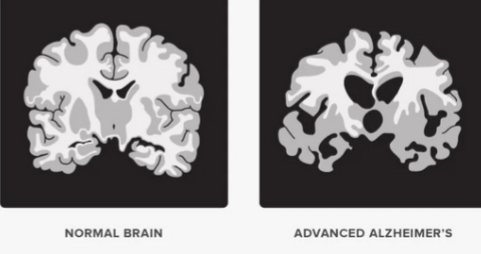
alzheimer’s pathology
accumulation of beta-amyloid plaques and neurofibrillary tangles distributed throughout the brain which degenerates neurons and synapses leading to atrophy of the cerebral cortex
dementia w/lewy bodies
produces a gradual, progressive decline in cognitive abilities w/motor parkinsonism
rapid eye movement sleep behavior disorder
visual hallucinations
fluctuations in level of alertness
prominent visuospatial dysfunction
manifests parkinsonism and cognitive decline contemporaneously
frontotemporal dementia
damage to the frontal and temporal lobes of the brain
symptoms include unusual behaviors
emotional problems
communication difficulties
difficulty w/work
difficulty walking
occurs at a younger age (45-60)
parkinson disease dementia
cognitive dysfunction dementia are common in parkinson disease
cognitive impairment in parkinson disease exists on a continuum of severity to the extent it interferes w/daily activities
visual hallucinations and delusions are a frequent manifestation
dementia emerges five to eight yrs after the onset of movement disorder
huntington disease
inherited progressive neurodegenerative disorder characterized by choreiform movements, psychiatric problems, and dementia
caused by a trinucleotide repeat in the huntingtin (HTT) gene and inherited in an autosomal dominant pattern
pathophysiology still not fully understood
NO KNOWN CURE, treatment is symptomatic and remains supportive
risk factors for dementia and cognitive decline
low educational attainment
midlife hypertension
midlife obesity
hearing loss
late life depression
diabetes
physical inactivity
smoking
social isolation
global deterioration scale for assessment of primary degenerative dementia
thinking
stage 1: no dementia, no cognitive decline: normal function, no memory loss, people w/no dementia are considered in stage 1
stage 2: very mild cognitive decline, no dementia: forgets names, familiar objects, symptoms not evident to loved ones or doctors; expected duration of stage unknown
stage 3: mild cognitive decline, no dementia: increased forgetfulness, slight difficulty concentrating, decreased work performance, gets lost more frequently, difficulty finding right words, loved ones begin to notice; average duration of this stage is btwn 2 and 7 yrs
stage 4: moderate cognitive decline, early stage dementia: difficulty concentrating, forgets recent events, cannot manage finances, cannot travel alone to new places, difficulty completing tasks, in denial about symptoms, socialization problems: withdraw from fam and friends, physician can detect cognitive problems; average duration is 2 yrs
stage 5: moderately severe cognitive decline, mid stage dementia: major memory deficiencies, need assistance w/ADLs, forgets details like address and phone #, doesnt know time or date, doesnt know where they are; average duration 1.5 years in this stage
stage 6: severe cognitive decline (middle dementia), mid stage: cannot carry out ADLs without help, forgets familys names, forgets recent events, forgets major events in past, difficulty counting from 10, incontinence, difficulty speaking, personality and emotional changes, delusions, compulsions, anxiety; average duration is 2.5 yrs
stage 7: very severe cognitive decline (late dementia), late stage: cannot speak or communicate, req help w/most activities, loss of motor skills, cannot walk, average duration of this stage is 1.5-2.5 yrs
functional assessment staging test
function
clinical dementia rating
thinking and function
goal for dementia treatment?
to preserve function and autonomy for as long as possible and to maintain quality of life for both patient AND caregivers
cholinesterase inhibitors
main stay treatment for alzheimer disease
does NOT prevent the progression to AD
40-50% pt show improvement
diet and dietary supplements for dementia
mediterranean diet (high in fruits, veggies, whole grains, nuts, seeds, fish, healthy oils) currently the most promising diet for brain health
antioxidant w/a plausible mech of action (evidence is inconsistent)
vitamin E/gingko biloba
vitamin B, coconut oil, fish oil
better to eat antioxidants (fresh fruit and veg)
and healthy fats (omega 3 fatty acids - salmon, flax seeds, walnuts
nursing care of people with dementia
appropriate use of medications
cholinesterase inhibitors
atypical antipsychotics and mood stabilizers (agitation and behavioral disturbances)
antidepressants and anxiolytics for depression and anxiety
advanced dementia
feed and nutrition (oral versus tube feed)
infections and fever (resp and urinary tract)
interventions for communication challenges with dementia
stroke → stroke rehabilitation
finding the right word? → supply the word
don’t know what they mean? → ask them to describe it or point to it
lost in the middle of what they are saying? → repeat their first word, this may help them to get started again
trouble expressing an idea? → guess what they are trying to say and confirm
appear relaxed → create a calm environment
behavioral challenges in dementia
potential precipitators
strange situations
confusion
groups of ppl
noises
being asked to do something they find difficult
needing to think about several things at once
being cared for by someone who is rushed or upset
not wanting to appear inadequate
not understanding what they saw or heard
being tired/not feeling well
not being able to express thoughts, etc
being treated like a child
combativeness can often be prevented by being alert to the person’s stress level
care giver impact
30% caregivers are age 65 or older
2/3 are women, 1/3 daughters
most caregivers (66%) live w/person w dementia
1 quarter third of dementia caregivers are “sandwich generation” caregivers → aging parent and at least one child
devastating role on caregivers. compared w/caregivers of ppl w/o dementia 2x as many cg of those w/dementia indicate substantial emotional, financial, and physical difficulties
of total lifetime cost of caring for someone w/dementia, 70% is borne by families either through out of pocket health and long term care expenses or from the value of unpaid care
interventions for behavior challenges with dementia
(for nursing and family)
if person w/dementia becoming upset w/something being done, STOP THE OFFENDING BEHAVIOR and allow time to rest
adjusting environmental factors when possible
addressing loneliness
structured activities
appropriate use of medication
the best way to manage behavioral disturbances in dementia depends on the severity of the symptoms
montreal cognitive assessment (MoCA)
most sensitive and validated cognitive screening tool used widely internationally (many languages/versions)
18-25= mild cognitive impairment
10-17= moderate cognitive impairment
less than 10= severe cognitive impairment
delirium
a clinical syndrome caused by a medical condition, substance intoxication or withdrawal or medication side effect that is characterized by disturbance of consciousness w/reduced ability to focus, sustain or shift attention
disturbance in attention (dev over short period of time)
an additional disturbance in cognition
disturbances are not better explained by another preexisting, evolving, or established neurocognitive disorder
disturbance is caused by a medical condition, substance intoxication, or withdrawal, or medication side effect
delirium presentation
loss of mental clarity
distractibility (patients flow of thought)
may appear drowsy, lethargic, semicomatose - more advanced cases
OR
hypervigilance seen more in cases of alc or sedative drug withdrawal
change in cognition - memory loss, disorientation, difficulty w/language and speech
hallucinations - visual, auditory, somatosensory
language difficulties ex: lose ability to write or to speak a second language
evaluation for delirium
confusion assessment method - identifies and recognizes delirium quickly and accurately in both clinical and research settings
investigate medical causes
fluid/electrolyte imbalances
infections
drugs or alcohol toxicity
withdrawal from alcohol
withdrawal from barbiturates, benzos, and selective serotonin reuptake inhibitors
metabolic disorder (hypoglycemia, hypercalcemia, uremia, liver failure, thyrotoxicosis)
low perfusion states (shock, HF)
postop states especially in older adults (pain)
prevention and nursing care: delirium
SAFETY KEY!
orientation protocols - clock, calendar, windows, verbally reorienting pt
cognitive stimulation - provide activities such as regular visits dont overstimulate especially at night
sleep - avoid procedure during sleeping; reduce night time noise
early mobilization and minimal use of physical restraints
delirium (medical emergency)
causes: “I WATCH DEATH”
I: infections
W: withdrawal
A: acute metabolic
T: trauma
C: CNS disease
H: hypoxia
D: deficiencies
E: environmental
A: acute vascular
T: toxins/drugs
H: heavy metals (LEAD AND MERCURY)
alcohol withdrawal delirium
“delirium tremens or DTs”
rapid onset fluctuating disturbance of attention and cognition sometimes w/hallucinations in the presence of alcohol withdrawal
withdrawal delirium typically begins within 72-96 hrs after pt last drink
in most severe manifestations its accompanied by agitation, severe tachycardia, hypertension, drenching sweats, and fever (extreme autonomic hyperactivity)
mod-sev withdrawal symptom of alcohol withdrawal include hallucination, seziures, or DTs - latter two can be life threatening!
communication interventions in persons w/delirium
keep conversations basic and one topic at a time
talk in calm soothing voice
give time to respond
remind where they are and what is happening
avoid asking too many questions
if having a hallucination, DO NOT ARGUE W/THEM OR TRY TO CORRECT THEM, INSTEAD ACKNOWLEDGE THEIR FEELINGS AND CALMLY REASSURE THEM
behavior interventions in persons w/delirium
have someone stay in room w/patient
have regular and night routine
keep room calm and quiet
make sure theyre comfortable
well nourished and hydrated
sensory items available
re-orient!
delirium vs dementia
delirium
rapid onset (hrs to day or two)
ability to stay focused is impaired
symptoms can come and go several times in a day
dementia
onset of minor symptoms that progress over years
remains alert in early stages
memory and thinking skills stay at a constant level
communication challenges in dementia
expressing themselves
difficulty in finding words
difficulty remembering names of people or objects
substitute words w/similar sounds (wrong for ring)
substitute words w/related meaning (wedding for ring; music thing for piano)
describe the object they cannot name
difficulty communicating the whole thought, but can com words within the thought (bus-home for “im concern about missing the bus that takes me home” or rambling thoughts, use of curse words…