applanation tonometry
1/24
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
25 Terms
what is the Imbert Fick principle (3)
When a flat surface (tonometer probe) with a defined area is pressed against the surface of a sphere (cornea)(applanation)
with a given internal pressure (IOP)
equilibrium is reached when the force exerted is balanced by the internal pressure. (= to IOP) - if force exceeded would be applanating
what is the Imbert Fick formula
W = P x A
the force required to flatten the surface of a sphere (W) is equal to the product of the pressure inside the sphere (P) and the area applanated (A)
what assumptions does the formula take into account
above formula is only true assuming that:
the cornea is dry, thin, perfectly elastic and flexible
and that the only force acting on the surface should be the pressure of the applanating surface
what considerations does GAT (Goldmann applanation tonometry) take into account (4)
–Surface tension (S) of the tear film which attracts the tonometer prism towards the cornea.
–Corneal rigidity (B) which resists applanation
--also need to take into account central corneal thickness (CCT)
--and corneal biomechanics
what does GAT determine the value of the area being applanated as (3)
if the area being applanated was 3.06mm2, then these two forces cancelled each other out
Therefore: W + S = (P x A) - B — so formula goes back to W = P x A
Will never be larger than 3.06mm2 due to cancelling out effects of B and S
explain how to give consent to patients (4)
Explain the test to the px beforehand - fully - reasoning why - pressure is a bit high this will allow me to do so - if we need to refer you hospital will need this information
Obtain informed consent
Ask about sensitivity to anesthetic drops - if they have had previous sensitivity for instance can refer them to being measured in hospital as they would be better equipped to do so
anesthetic drops lasts around 20 mins – advised not to go into any windy environments or rub eyes
what do you need to inform the patient about in regards to the anesthetic drops (4)
Inform px drops will sting at first -this should dissipate quickly - make sure to inform of the sting to gain trust especially with children
Add a drop to each eye
After a minute add a second drop to each eye
They should not feel the second drop if you have correctly inserted the first drop correctly.
how do we set up the GAT on the slit lamp (3)
Need to place GAT on stage
Stage and GAT need to be secure - should hear a click sound - that’s when you know its secure
ensure it is seen by the dominant eye as this is a monocular test and probe will be seen by one eye

how do we align the tonometer probe (6)
Insert and align 0 with white line on the carrier. – only if corneal astigmatism is less than 3.00D – (this reading is found via keratometry)
If corneal astigmatism is greater than 3.00 D (rare but may be in px with kerataconus)
Then an error of 1 mmHg is produced for every 4.00 D of corneal astigmatism
If astigmatism is WTR or ATR than you can move to the red line on carrier
If oblique than it needs to be 43 degrees from the flattest meridian
remember to disinfect the probe in between px

describe slit lamp set up for GAT (5)
•Mag 10-16x
•Angle 45-60 degrees
•Widest beam
•Cobalt Blue Filter (+Wratten if available)
-High Illumination

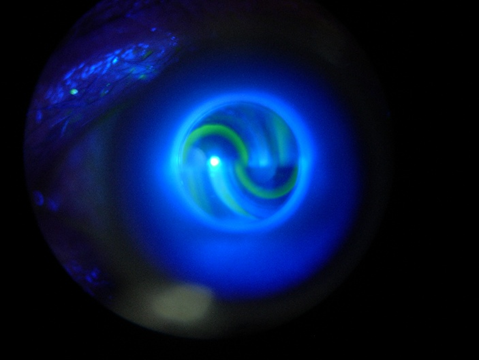
explain instillation of fluorescein (5)
Fl needs to be instilled safely
Makes mires easier to see
Aim not to put in too much as this will affect the quality of the mires – if too big inaccurate result
at this point we can say the eye has been applanated
note the bi-prism in the probe - line division - bi-prism probe touches the cornea
how do we instruct the px to ensure accurate readings (4)
Ask patient to keep as still as possible during the procedure - need to keep their head right up against the forehead rest
Ensure Slit Lamp is at right height for px prior to GAT
Ask them to look straight ahead and encourage them not to blink
Be aware that readings can be higher in an anxious patient - so do your best to reassure
explain how we actually get to the point of applanation after set up (5)
Set the tonometer to the expected result from before - usually from non-contact tonometry - so only need fine tuning to get to accurate result - makes it easier
Gently move the slit lamp forward
You should be looking around the side of the slit lamp until applanation has occurred
You will see the tonometer probe head move back - this is point of applanation
will see fl lighting up as it touches the eye - atp do not go any further and remind px not to move

what is the ideal GAT appearance and what is not ideal
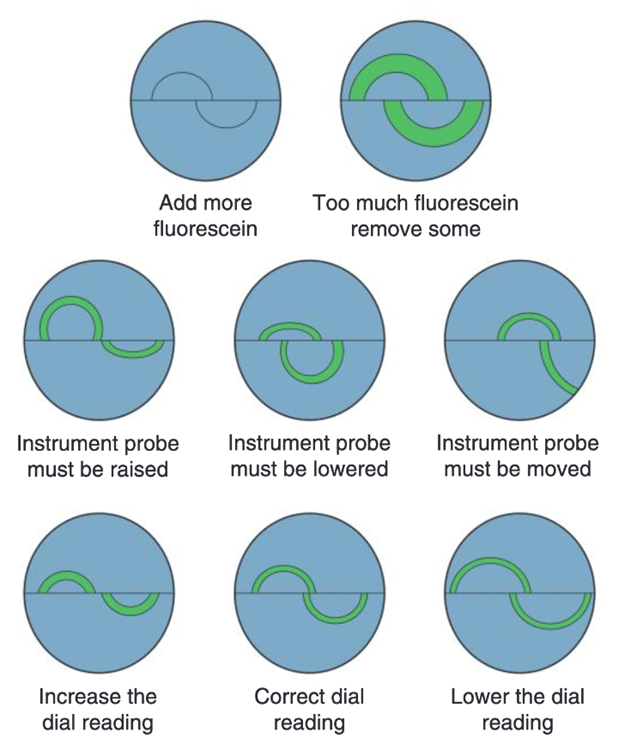
CANNOT use reading at all if too much Fl has been used
for no.5 we would move the probe towards the bottom image to get closer
ideal - is when the inside of mires barely touching eachother
what is essential to do post GP (2)
•Check the corneal integrity after GAT
•Ensure any staining is not affecting the stroma - check via optic section
what do we need to record for GAT (4)
Techniques used
IOP Measures (each eye) - get the average of the movement measures
Time of day – in case of doing repeat measures – tends to be higher in AM and reduces onwards
E.g. GAT R 21 L 22 @ 3:00pm
how do we calibrate the GAT (3)
calibrate at least once a month to ensure accurate readings or taking into account any inaccuracies
insert calibration rod at 0, 20 and 60 - will start to wobble/move around
for example at 60 if it starts to move around at 58 and at 20 if it starts to move around at 18 - this tells us its off by 2 - so if we get a value of 26 we know the actual value would be 24 as it is off by 2
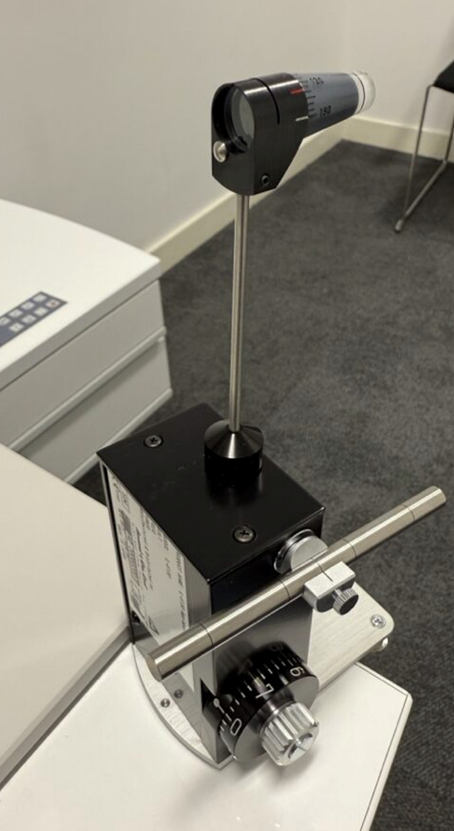
explain what a Perkins is and its use (3)
Similar to GAT but with a different setup - rest forehead circle against their head and take reading
also uses cobalt blue light
portable but useful for patients that are unable to use a slit lamp - domiciliary patients etc.

define pachymetry
measure is the term used for the measurement of corneal thickness
when would we perform pachymetry - for what patients ()
Patients with ocular hypertension - not glaucomatous at the moment but need to be aware as more likely/risk of developing
When IOP is measured
Refractive Surgery - can determine what type of surgery is most suitable for a patient
Screening and monitoring of: Corneal oedema / Keratotconus / Corneal dystrophies
what is the average pachymetry reading
around 550
what is the average CCT measurement with tonometry (4)
•Corneal Centre Thickness (CCT) is assumed to be 520 µm with the Goldmann tonometer
•Most other tonometers assume either 545 or 550 µm for the CCT - so make sure to take into account the average of the machine YOU are using
•If the CCT is higher than that assumed by the tonometer, then the device will OVER ESTIMATE the patients IOP
• If the CCT is lower than that assumed by the tonometer, then the device will UNDER ESTIMATE the patients IOP
what are the different types of tonometry (5) need to read up on these
•Ultrasound Pachymetry
•Ultrasound Biomicroscopy
•Optical Pachymetry
•OCT
•Scheimpflug imaging
explain the use of Tonovue-P (2)
•Uses Scheimpflug Camera
•Calculates a compensated IOP measure
what do we record for pachymetry (3)
–Techniques used
–CCT Measures (each eye)
–Time (time of day can affect CCT)