ADULT HEALTH FINAL EXAM!
1/851
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
852 Terms
Why is delegation important in nursing?
Your State Board of Nursing Licensure requires it
State Nurse Practice Act
Nurses cannot do everything
Safe and competent patient care is complex
A team approach is needed
Interprofessional collaboration is essential to healthcare
Both the American Nurses Association (ANA) and the National Council for State Boards of Nursing (NCSBN) support nurses in using delegation safely and effectively
Delegation vs. Assigning
Delegation involves transferring authority to perform a task to another qualified individual
The person who delegates the task is still accountable
Assigning involves transferring the authority and the accountability of a task to another qualified individual
In each case, the individual chose must be appropriately trained to take on the task in question
5 Rights of Delegation

Delegation - Factors to Consider
Your role at work
Different facility policies
Your own personal experiences
Public misperceptions
Delegation - Members of the Team
RN
Is a licensed nurse
Program of completion varies but is ~ 120 hrs
Must pass the NCLEX- RN
License governed by State Board of Nursing
LPN
Is a licensed nurse
Program of completion varies but is ~ 60 hrs
Must pass the NCLEX- PN
License governed by State Board of Nursing
UAP
Is unlicensed
Some programs offer a certificate
Facilities can determine and offer required training
Delegation - Score of Practice: RN, LPN, UAP
RN
Initial assessment (admin, post-op)
Assessment of unstable clients
Admin IV push, blood products, TPN, and meds requiring titration/continuous monitoring
Access implanted devices
Interpret and analyze data requiring complex critical thinking
Care plan development
Initial and discharge teaching
LPN
Monitor RN findings and gather data (obtain BP, HR, etc)
Assessment of stable clients (focused and subsequent assessments)
Basic pt care (changing bandages, inserting catheters)
Report client status and concerns to RN/HCP
Care for stable clients with predictable outcomes (chronic, expected findings, ready for discharge, current labs)
Reinforce RN education
UAP
Assist client with ambulation, ROM, hygiene, and activities of daily living (ADLs)
Feeding and oral care for stable clients (not if risk of aspiration)
Record routine vital signs and I&Os (may measure UOP from indwelling catheter bag)
Positioning and linen change
Transfer/transport (to/form bed, chair, commode, stretcher)
Report client status and concerns to RN
Delegation - Facility Specific Training
Facilities can train LPN’s to perform tasks outside their scope of practice
Facilities can train UAPs to perform tasks outside their scope of practice
The RN retains accountability for supervision and safe execution of these tasks
RN CANNOT Delegate
Any task that involves:
Clinical reasoning
Requires nursing judgement
Involves critical decision making
Involves the nursing process
Is above the scope of practice for the LPN or UAP
The nurse is planning care for a group of clients. Which task should the nurse assign to the licensed practical nurse (LPN)?
A. Assisting a client with crutch walking following knee replacement surgery.
B. Analyzing lab data to identify issues for a client who has diabetes mellitus.
C. Performing an admission assessment on a postoperative client.
D. Developing the plan of care for a client following an amputation.
A. Assisting a client with crutch walking following knee replacement surgery.
The nurse is caring for several clients. Which task is most appropriate to delegate to the unlicensed assistive personal (UAP)?
A. Assisting the client with preparation of a sitz bath
B. Walking the post-operative client that just returned from surgery
C. Coaching the client to deep breath during painful procedures
D. Monitoring the client for signs of discomfort while ambulating
A. Assisting the client with preparation of a sitz bath
The RN is caring for a group of clients. Which tasks can be delegated to the LPN? Select all that apply
A. Provide discharge instructions to a client's spouse
B. Obtain vital signs for a client who is 8 hours post-op
C. Administer oral pain medication to a client who is 1 day post-op
D. Initiate a care plan for a client who was admitted last night
E. Administer insulin to a client who is diabetic
B. Obtain vital signs for a client who is 8 hours post-op
C. Administer oral pain medication to a client who is 1 day post-op
E. Administer insulin to a client who is diabetic
A nurse is delegating assignments for a nursing team that includes an unlicensed assistive personnel (UAP). Which tasks should the nurse delegate to the UAP? (Select All That Apply)
A. Bathe a client who had an amputation 2 days ago
B. Assist a client to ambulate using a gait belt
C. Explain a low-sodium diet to a client who has hypertension
D. Review oral hygiene with a client who is receiving chemotherapy
E. Measure and document a client's intake and output
A. Bathe a client who had an amputation 2 days ago
B. Assist a client to ambulate using a gait belt
E. Measure and document a client's intake and output
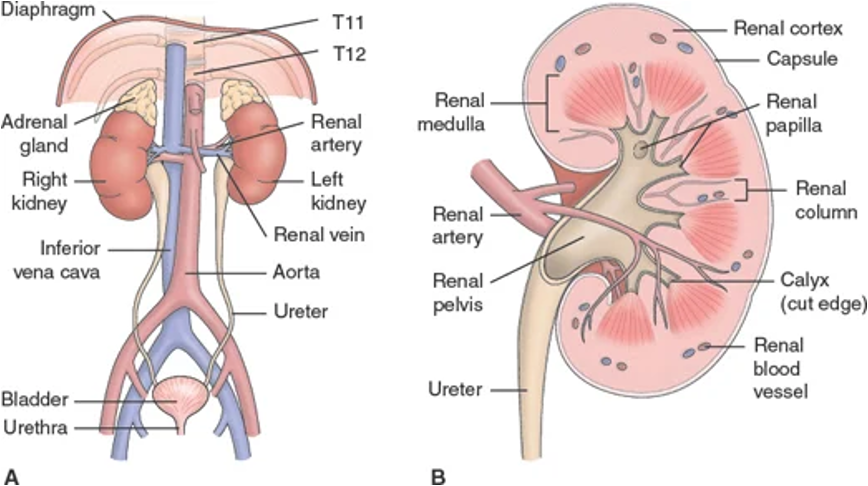
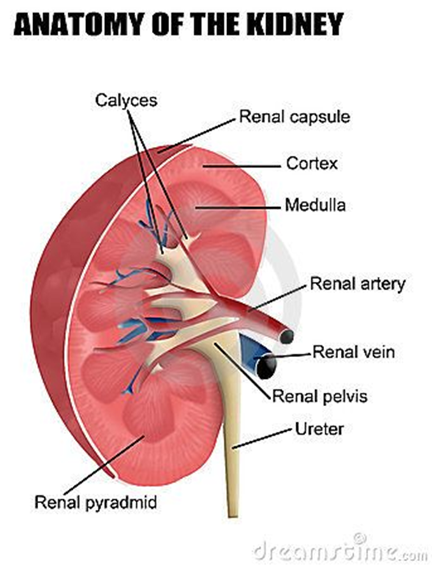
Renal/Urology - System Overview
Structures include kidneys, ureters, bladder, and urethra
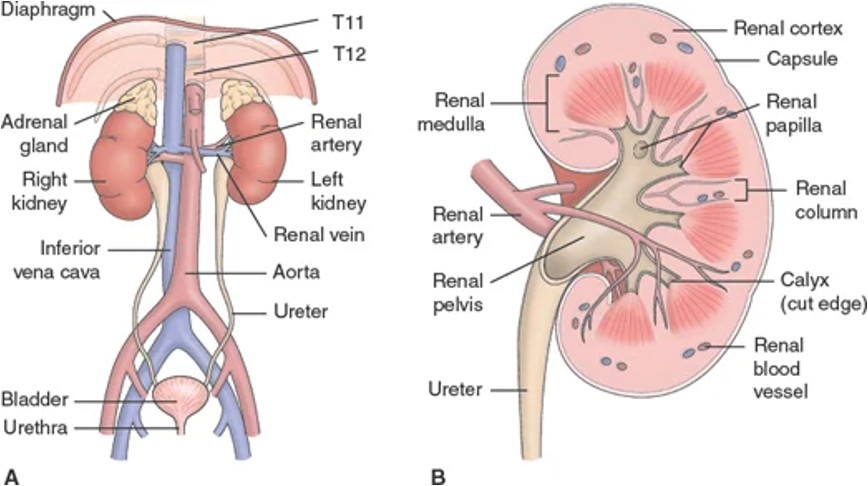
Renal/Urology: Anatomical Components - Nephrons
Cells of the kidneys
Responsible for filtration (urine production)
Consider renal replacement therapy when greater than 85% is damaged
Will autoregulate based on body’s needs
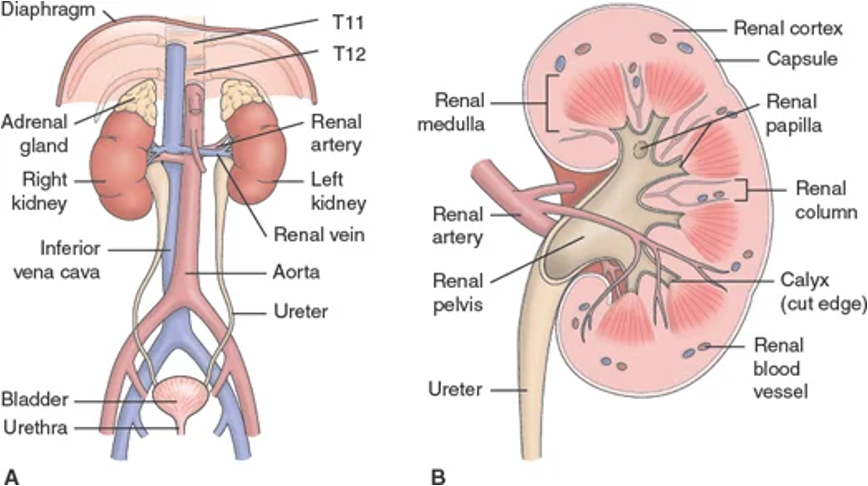
Renal/Urology: Anatomical Components - Ureters
Moves urine to bladder
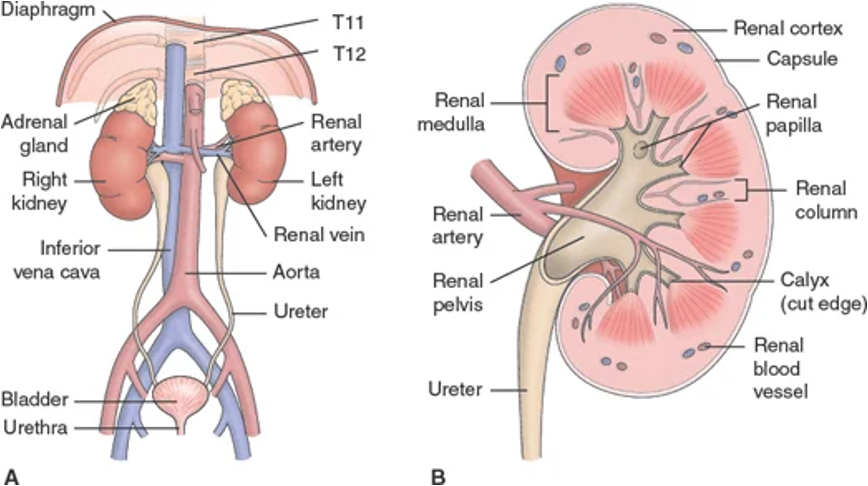
Renal/Urology: Anatomical Components - Bladder
Houses urine to be excreted and prevents urine reflux into kidneys
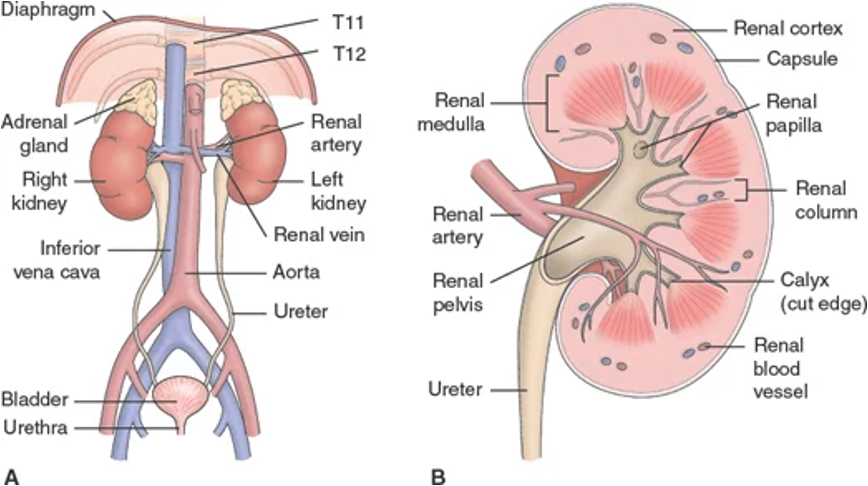
Renal/Urology: Anatomical Components - Urethra
Eliminates urine from bladder
Renal Physiology
Control of blood pressure
Control of water balance
Excretion of waste via urine formation
Regulation of electrolytes
Regulation of acid-base balance
Regulation of red blood cell production
*Production of ADH in the kidneys helps with fluid balance and BP management
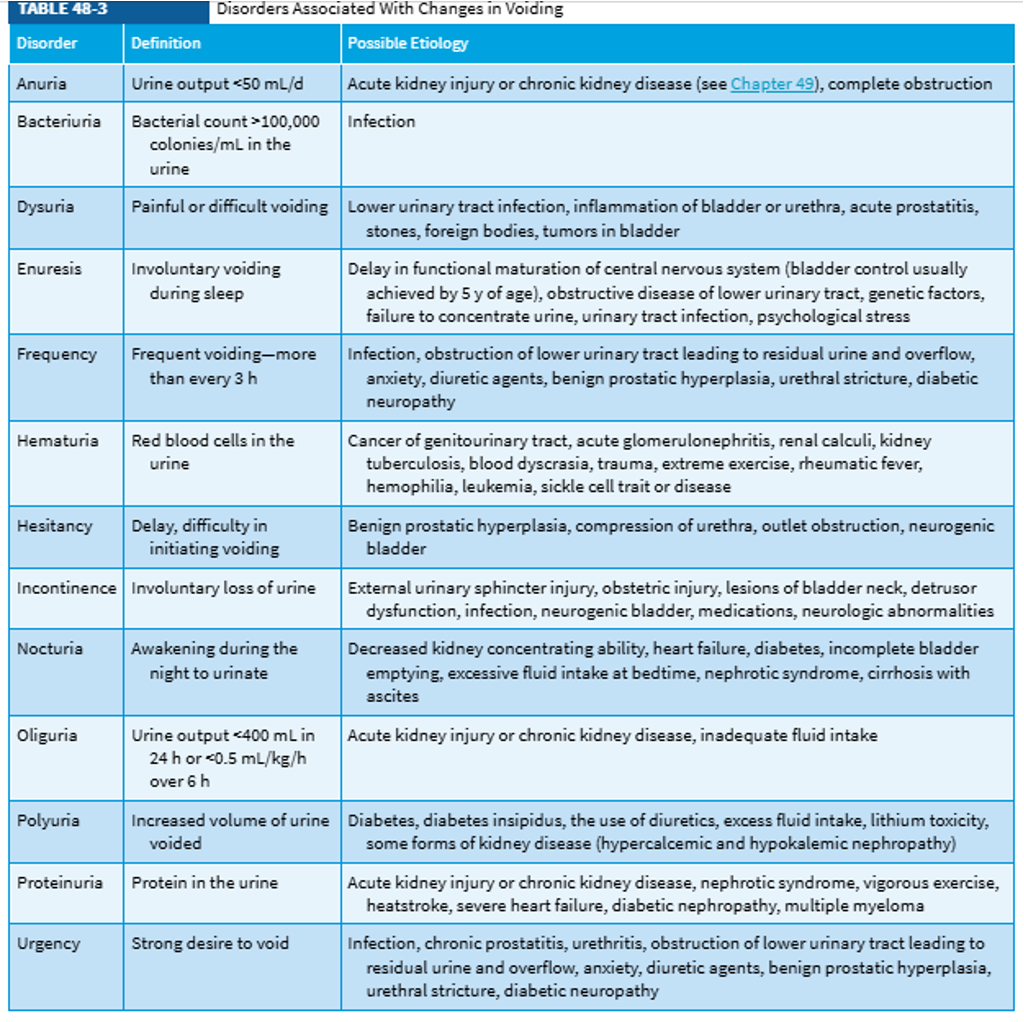
Common Urinary Symptoms
*400 mL of urine per day is the estimated minimum of what is needed to rid the body of waste
Renal/Urology - Nursing Assessment
Head-to-toe focusing on abdomen, suprapubic region, genitalia, low back and lower extremities
Palpation of the kidneys is not usual, this may indicate enlargement
Physical symptoms
Pain characteristics are important for diagnosing
Is it dull or achy? sharp or stabbing? where is it? are you having any other symptoms along with the pain?
Changes in voiding patterns or urine appearance
Are GI symptoms present? N/V, diarrhea, abdominal pain or discomfort
Unexplained anemia
Health history
Ask about risk factors
Previous stones or UTI
Family history
Genetically passed disorders
EXs: polycystic kidney disease (PKD), renal cystic diases, diabetes, CAD, pulmonary HTN
Male inferility or cystic fibrosis
Renal tumors or cancers
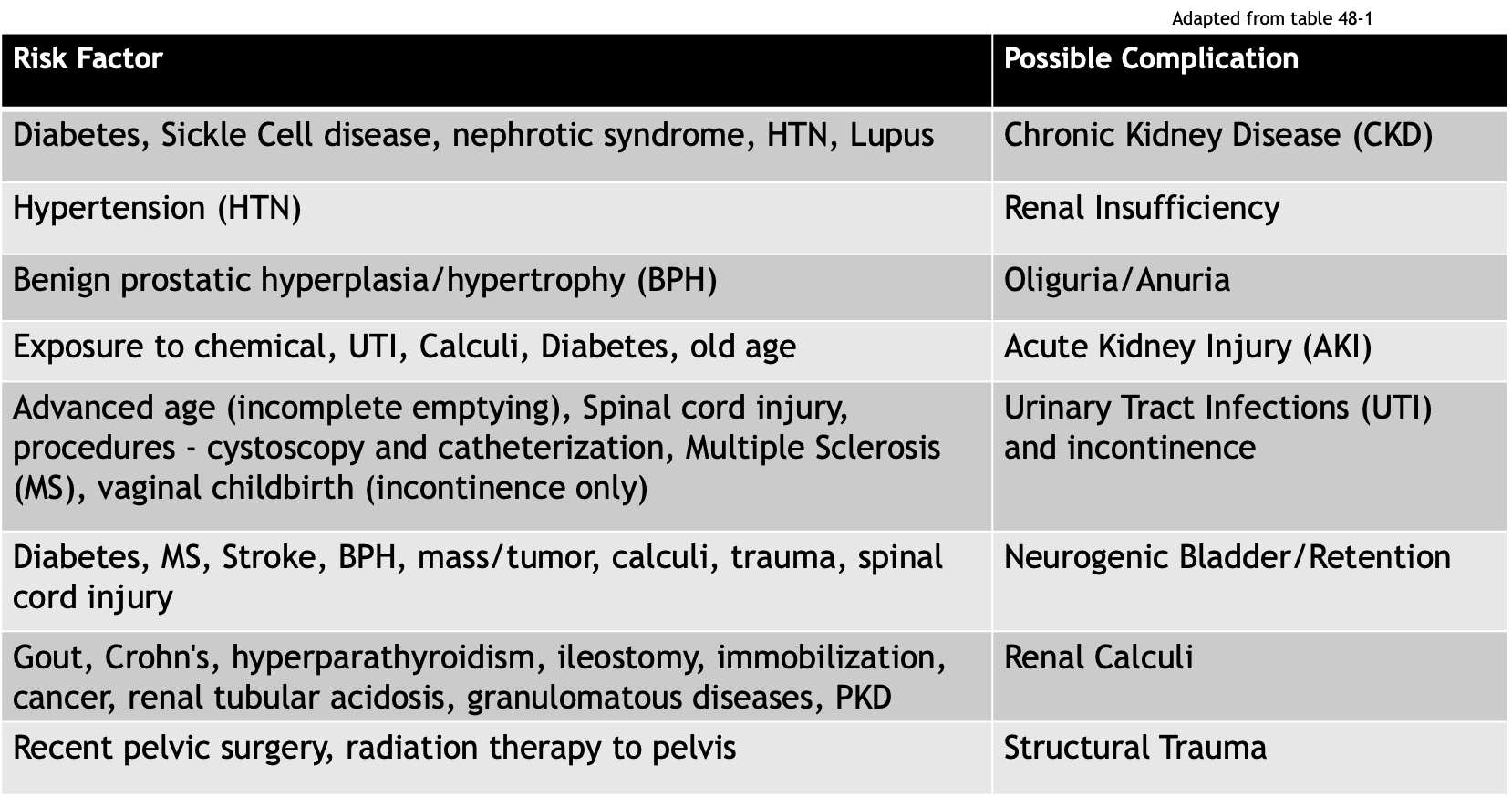
Risk Factors for Renal + Urologic Disorders
Diagnostics for Renal Function - Urine Tests: Urinalysis (US)
Checks color, clarity, pH , specific gravity, and presence of cells/protein/glucose/ketones
Diagnostics for Renal Function - Urine Tests: 24-Hour Urine Collection
24-hour urine collection
Daily urine output (UO) - normal is 1 mL/kg/hr (1-2L/day)
Picture of the kidney’s ability to clear solutes from plasma
Usually measuring creatinine in urine
Diagnostics for Renal Function - Urine Tests: Osmolality
Measures presence of solutes in urine
Normal range: 200-800 (less is best!)
Diagnostics for Renal Function - Urine Tests: Specific Gravity
Measures density compared to water
Normal range is 1.005-1.025
Abnormal low can be from diabetes insipidus, glomerulonephritis, and hyperhydration
Abnoraml highs can be from diabetes mellitus, nephritis, and dehydration
Diagnostics for Renal Function - Blood Tests: BUN
8-20 mg/dL
Blood urea nitrogen (end-product of protein metabolism)
High levels indicate the kidneys are not filtering well
Diagnostics for Renal Function - Blood Tests: Creatinine
Male: 0.6-1.2 mg/dL; female: 0.4-1 mg/dL
Waste product that is not filtered appropriately in presence of renal damage
Diagnostics for Renal Function - Blood Tests: eGFR (Glomerular Filtration Rate)
Used to identify the stage of kidney disease
Decreases naturally with aging changes
Age (years)
Average eGFR
20–29
116
30–39
107
40–49
99
50–59
93
60–69
85
70+
75
Upper and lower urinary tract function changes with age
The GFR decreases, starting between 35-40 years of age, and a yearly decline of about 1 mL/min continues thereafter with a notable decrease in GFR by as much as 30%-50% by age 70
Older adults are more susceptible to AKI and CKD due to structural and functional changes in the kidney
Kidney function results may be within normal limits until the GFR is reduced to less than 50% of normal
GFR Classifications
Stage | Description | eGFR | Kidney Function |
1 | Possible kidney damage (e.g., protein in the urine) with normal kidney function | 90 or above | 90-100% |
2 | Kidney damage with mild loss of kidney function | 60-89 | 60-89% |
3a | Mild to moderate loss of kidney function | 45-59 | 45-59% |
3b | Moderate to severe loss of kidney function | 30-44 | 30-44% |
4 | Severe loss of kidney function | 15-29 | 15-29% |
5 | Kidney failure | Less than 15 | Less than 15 |
Gerontologic Considerations - Renal
GFR begins to decrease 1 point/year starting at age 35-40
Increased risk for AKI due to structural changes of the kidney
Sclerosis of renal tissues, decreased blood flow or perfusion, decreasing GFR, etc
Increased risk for dehydration and hypernatremia with a decreased stimulation of thirst
Gerontologic Considerations - Urology
Decreased bladder muscle tone and decreased vasopressin and ADH levels
Can cause an increase of residual urine
Often have incomplete emptying of the bladder and/or urinary stasis which increase the risk of a UTI and urinary urgency
Increased likelihood of nocturia
Increased likelihood of urinary incontinence
Also maybe related to mobility
May self-limit fluid intake - watch for dehydration
Symptoms may appear as other GI issues making diagnosis difficult
Acute Kidney Injury
Renal damage resulting in a rapid loss of function (impaired filtration/regulatory functions)
Criteria (only one must be present)
Increase in baseline serum Cr by 50% or more
An increase of 0.3 mg/dL within 48 hours
Decreased UO <0.5 mL/kg/h x 6 hours
Can progress to ESKD (end stage kidney disease) if not treated quickly
Changes to BUN, Cr, and GFR
Metabolic complications such as acidosis and/or fluid and electrolyte imbalances
Urine output (UO) may or may not be affected
Patients may appear critically ill showing signs of lethargy, drowsiness, headache, muscle twitching, seizures
Mortality rate can be as high as 80% - prevention is essential
Critical illness symptoms mostly reflect the symptoms of electrolyte imbalance
Phases of AKI - Initiation (1)
Begins at the initial insult to kidney function and ends when the oliguria phase starts
Phases of AKI - Oliguria (2)
Increase of serum concentration of substances usually excreted by kidneys (ex - creatinine, K+, phosphorous, magnesium); UO drops to 400 mL/day or less
Watch for uremic symptoms, life threatening electrolyte imbalances such as hyperkalemia may also develop
Some patients may be non-oliguric and still maintain normal UO of 1-2 L/day, but the substances which should be excreted are not being filtered out
*Do not confuse the “oliguria” phase with the definition of oliguria as a urinary symptom
Phases of AKI - Diuresis (3)
Gradual increase in GFR and UO, stabilization of labs with possible decrease
Continue to monitor for uremic symptoms and for possible dehydration
Phases of AKI - Recovery (4)
Labs return close to patient baseline; permanently decreased GFR will be present (1-3%)
AKI - Causes
Changes to perfusion
Intravascular volume depletion
Impaired cardiac function/decreased CO
Vasodilation
Increased diuresis (physiological or med)
Injury to renal tissue (renal ischemia)
Infections or obstruction in the renal/urologic tract
Transfusion reactions or hemolytic anemia
Trauma/crushing injuries
Rhabdomyolysis
Clinical syndrome characterized by injury to skeletal muscle fibers with disruption and release of their contents into the circulation
Myoglobin, creatine phosphokinase (CK) and lactate dehydrogenase are the most important substances for indicating muscle damage
Rhabdomyolysis-induced acute kidney injury (RIAKI) occurs following damage to the muscular sarcolemma sheath, resulting in the leakage of myoglobin and other metabolites that cause kidney damage
Nephrotic agents (NSAIDS, ACE inhibitors, chemicals, contrasts, etc)
AKI - Treatments
Goal: To restore normal chemical balance and prevent further complications
Identify and eliminate/treat the underlying cause if possible
Provide renal replacement therapy when ordered (KRT - Kidney Replacement Therapy/RRT)
HD; PD -Peritoneal Dialysis; CRRT - Continuous Renal Replacement Therapy
Assess/monitor fluid balance:
Daily weights, CVP - Central Venous Pressure, I/O balance, total UO per 24 hours
Nutrition support: high calorie and high protein, restrict Na, K, phosphorous
Assess physical condition and labs
Turn, cough, deep breathe to prevent atelectasis and pneumonia
Skin care - bathe with cool water and reposition frequently
The skin may be dry or susceptible to breakdown due to edema; therefore, meticulous skin care is important
Excoriation and itching of the skin may result from the deposit or irritating toxins in the patient’s tissues
Strict asepsis
Infection prevent with all catheters and vascular access devices
Treat fevers quickly
Plan + provide individualized education and psychosocial support
Types of Urology Disorders
Urinary tract infections
Adult voiding dysfunction
Urolithiasis and nephrolithiasis
Urinary cancers
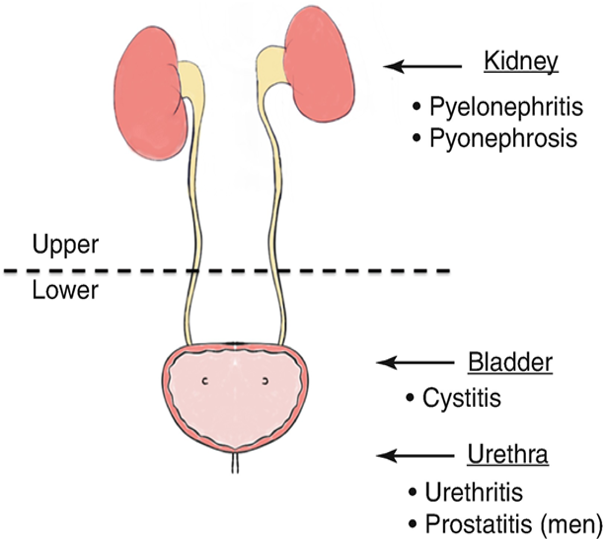
Urinary Tract Infections
Occurs when a pathogen enters the urinary tract, remember this system is sterile above the urethra
Identified by location: upper or lower
Upper UTIs include pyelonephritis, interstitial nephritis, and abscess (renal or perirenal)
Lower UTIs include cystitis (bladder), prostatitis (prostate), and urethritis (urethra)
If not treated, can lead to AKI, CKD, or urosepsis
Accounts for over 8 million healthcare visits/year
More common in females
CAUTI is the most common healthcare-associated infections and cause of secondary bloodstream infections
CAUTI is a UTI associated with indwelling urinary catheters
A UTI that occurs while the pt has an indwelling urinary catheter in place for more than 2 calendar days on the day that the infection was detected
Urinary Tract Infections - Risk Factors
General risk factors
Bacteria in the urinary tract
Female gender - anatomy (shorter), pregnancy, and intercourse
Comorbidities such as DM or gout
Immunosuppression
Urinary stasis and/or backwards flow
Instrumentation of the urinary tract (catheters/procedures)
“HARD TO VOID” acronym (another flashcard)
Age-related (geriatric) risk factors
Cognitive impairment
Frequent use of antimicrobials
Multiple chronic medical conditions
Immunocompromise
Immobility
Incomplete emptying of bladder
Low fluid intake, dehydration
Poor hygiene/stool incontinence
“Hard to Void”
Hormone changes (pregnancy, menopause)
Antibiotics (changes the normal flora)
Renal stones (obstructs flow of urine)
Diabetes (high glucose levels and poor immunity)
Toiletries (powders, perfumes, bubble baths)
Obstruction - BPH (enlarged prostate), masses/tumors
Vesicoureteral reflux (urine returns to the ureters - usually congenital)
Overextended bladder (immobility, spinal cord injury, etc)
Invasive (intercourse, indwelling catheters, procedures)
Disease states (remember the disease related complications)
Urinary Tract Infections - Supporting Data
Physical assessment:
Abnormal abdominal findings, back/suprapubic/pelvic pain
Urinary symptoms
May be asymptomatic (common with an indwelling catheter)
The nurse should inquire about association of symptoms with personal activity (ex - intercourse, hygiene, etc)
Urine characteristics: appearance with UA w/ C&S
Kidney/bladder ultrasound
Urinary Tract Infections - General Nursing Interventions
Treat with providers’ orders
Pain relief - use heat therapy or med if ordered (analgesics and antispasmodics)
Antibiotics or anti-infectives
Increase fluid intake, but avoid irritants like coffee, tea, citrus, alcohol, etc
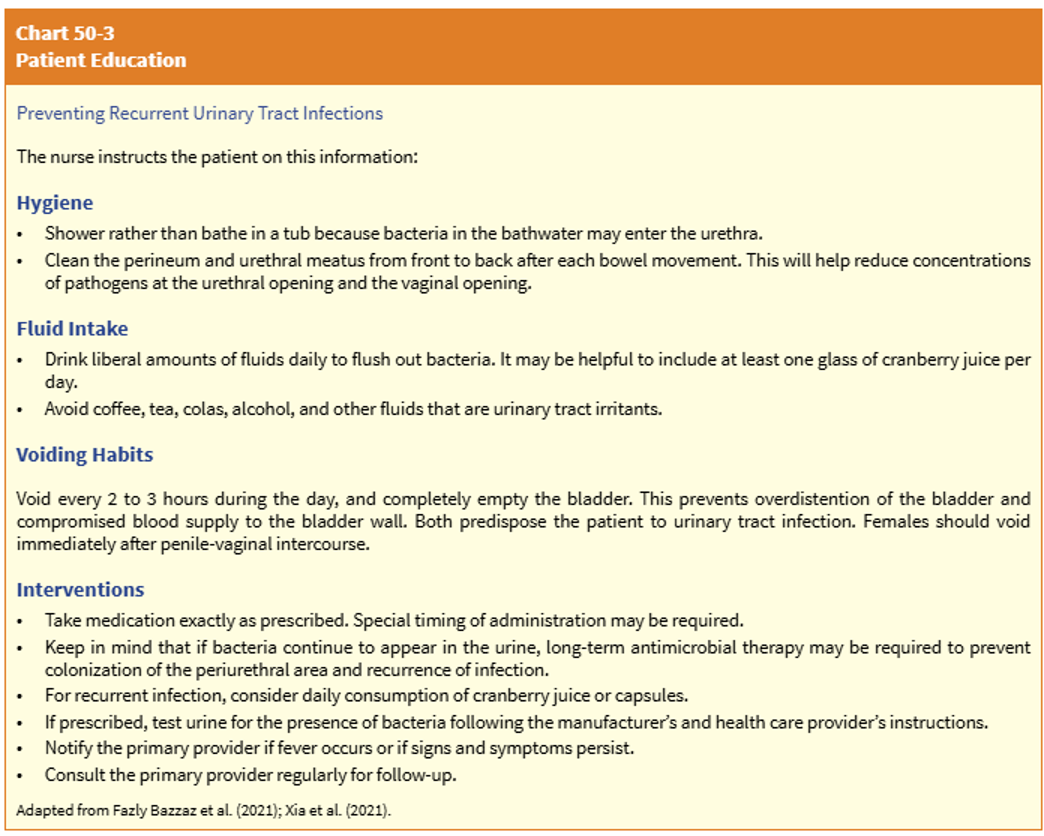
Pt education
Treatment compliance
Prevention of reoccurence by controlling modifiable risk factors
Cranberry juice/supplement for prevention of recurrent UTI
Reduce UTI incidence by 30%
Lower UTI
Bacteria migrates to the bladder and causes an infection
Most commonly, fecal organisms (like E. coli) migrate via the transurethral route
Reflux of urine from the urethra into the bladder (urethrovesical)
Commonly happens when coughing, sneezing, or straining due to an increase of bladder pressure that pushes urine into the urethra, as pressure decreases, the urine flows back to the bladder and can carry bacteria with it
Lower UTI - Nursing Considerations
Additional assessment findings
Elderly - incontinence, delirium, decreased sensation leading to no report of symptoms
Post-menopausal women - malaise, nocturia, incontinence, foul-smelling urine
Confirm with UA or basic labs, no diagnostics needed unless there is concern for spreading infection or complication
Treatment typically involves a pharmacologic agent
Anti-infective/antibiotics and urinary analgesics; 3-5 days
Nursing interventions:
Assess/monitor virals and I&Os
Use external catheters, not indwelling
Monitor for spesis and other complications like pyleonephritis or kidney fialure
Patient education related to treatment and prevention
Upper UTI
Typically caused by bacteria traveling upward from the bladder or from a blood stream infection that reaches the kidneys
AKA: pyelonephritis - bacterial infection of the renal pelvis, tubules, and interstitial tissue of one or both kidneys
Other causes can be interstitial inflammation, abscess, kidney damage, tubular cell necrosis, a bladder infection, urinary stasis, or obstructions (tumors/structures/BPH) that cause reflux from the bladder into either or the ureters (ureterovesical or vesicoureteral reflux)
Less common that lower tract infections, but a more common cause or urosepsis
Upper UTI/Pyelonephritis - Nursing Considerations
Additional assessment findings
Acute - physical assessment may show chills, fever, low back/flank pain, N/V, headache, malaise
The chronic condition happens after several acute episodes that leave scar tissue on the kidneys, resulting in permanent kidney damage
Chronic - asymptomatic unless the patient is experiencing an acute exacerbation and may also show fatigue, poor appetite, polyuria, excessive thirst, and weight loss
CT imaging, ultrasound, or a pyelogram may also be ordered with UA and labs
Treatment typically involves a pharmacologic agent
Anti-infective/antibiotics and urinary analgesics; 2 weeks
Nursing interventions:
Assess/monitor vitals and I&Os
Monitor for complications: ESKD, HTN, and renal calculi
Patient education to prevent further infection
Patient Education for Upper and Lower UTIs
Promote adherence to antibiotic regimen
Don’t stop because symptoms stop
Promote increased water intake - 3-4L per day
Monitor their own I&Os and notify MD of abnormal changes to urine appearance/volume
Encourage/promote frequent voiding (go when you feel the need, and every 2-3 hours)
Maintain good perineal hygiene, especially important for dependent/incontinent patients
Urinate before and after intercourse
Preventive measures for any modifiable tasks
Types of Voiding Dysfunction
Incontinence - “involuntary loss of urine”
Stress - happens with sneezes, laughing, exertion, etc… (no structural changes)
M - after prostatectomy, F - after pregnancy
Overflow - overdistended bladder due to bladder muscle dysfunction or obstructed outflow
Urge - aware of need to void but can’t get to a toilet quickly enough
Functional - physical or cognitive impairment
Latrogenic - external medical factors (ex - meds)
Mixed - combo of factors
Retention - “incomplete emptying”
Voiding Dysfunction - Incontinence
Assessment should include discussion of symptoms
A detailed description of the problem and a history of med use, the patients voiding history, a dairy of fluid intake and output, and any bedside test results (like a residual urine scan)
Skin care!!
Skin breakdown can occur from incontinence-associated dermatitis (IAD), a type of moisture-associated skin damage caused by physical and chemical irritants
Collaborate with the medical plan:
Non-pharmacologic interventions are the first choice of treatment: fluid management, voiding schedule/retraining, pelvic floor exercises
Pharmacologic can be used in conjunction with behavioral changes: first-line meds are anticholinergics (for inhibiting bladder contraction)
Surgery may be indicated when no meds or behavioral methods work
Affects 9-12% of all adults
More common in women (nearly 2x the rate of men)
Up to 90% of elderly patients in institutions
Often goes undiagnosed
Pts are embarrassed to seek help and may not want to discuss symptoms
Patient Education for Incontinence
The nurse should educate the patient on: avoid bladder irritants (caffeine + alcohol) and artificial sweeteners such as aspartame
Increase awareness of the amount and timing of all fluid intake and avoid taking diuretics after 4 pm
Take steps to avoid constipation: drink adequate fluids, eat a well-balanced diet high in fiber, exercise regularly, and take stool softeners if recommended
Void regularly 5-8x/day (about every 2-3 hours)
First thing in the morning; before each meal, before retiring to bed, once during the night if necessary
Perform all pelvic floor muscle exercises as prescribed every day
Stop smoking (if applicable)
Financial or community resources, discuss barriers to compliance
Voiding Dysfunction - Retention
Nursing Considerations:
Changes with elderly: older adults may retain 50-100 mL due to changes in bladder tonicity
Assessment/diagnosis can be challenging since symptoms can be vague
Ask the patient lots of questions to understand their voiding patterns:
What was the time of the last voiding, and how much urine was voided?
Is the patient voiding small amounts of urine frequently?
Is the patient dribbling urine?
Does the patient report pain or discomfort in the lower abdomen? (Discomfort may be relatively mild if the bladder distends slowly)
Is the pelvic area rounded and swollen (could indicate urine retention and a distended bladder)?
Does percussion of the suprapubic region elicit dullness (possibly indicating urine retention and a distended bladder)?
Are other indicators of urinary retention present, such as restlessness and agitation?
Palpate for bladder distention and lower abdominal pain
Postvoid bladder ultrasound
When untreated, this can lead to a UTI, calculi formation, pyelonephritis, and sepsis
Nursing interventions:
Promote good body position for elimination
Apply warmth to perineum
Reduce caffeine
Request MD order for bladder ultrasound if needed
Straight cath if indicated, try to avoid indwelling catheters
Neurogenic Bladder
A nervous system disorder that impacts voiding, by causing either incontinence or retention
Incontinence (functional): spastic muscle tone, empties with no controlling influence/regulation
Retention:
Flaccid muscle tone - no bladder contraction so the bladder becomes overdistended; must be straight cath’d to empty
May eventually lead to overflow incontinence when it is too full
Complications include infection, impaired skin integrity, and renal calcili
Treated with meds or with a voiding schedule; may need to straight cath on a schedule if the patient has retention
Urinary Catheters
Types: indwelling/straight, indwelling, suprapubic
Only use when absolutely necessary:
Retention/neurogenic bladder
Post-op following urological procedures
Stage 3-4 skin injuries of the perineum
Urinary tract obstruction
End-of-life care/critical illness care
Nursing considerations:
CAUTI prevention
Catheter care “bundle”
Below the bladder, not of the floor, perineal care 2x/day and prn, secured to leg, no kinks in tubing
Identify true patient need
Advocate for external device and removal asap
Skin care (stat-lock and moisture)
Asepsis of catheter bag/ports, do not disconnect tubing for samples
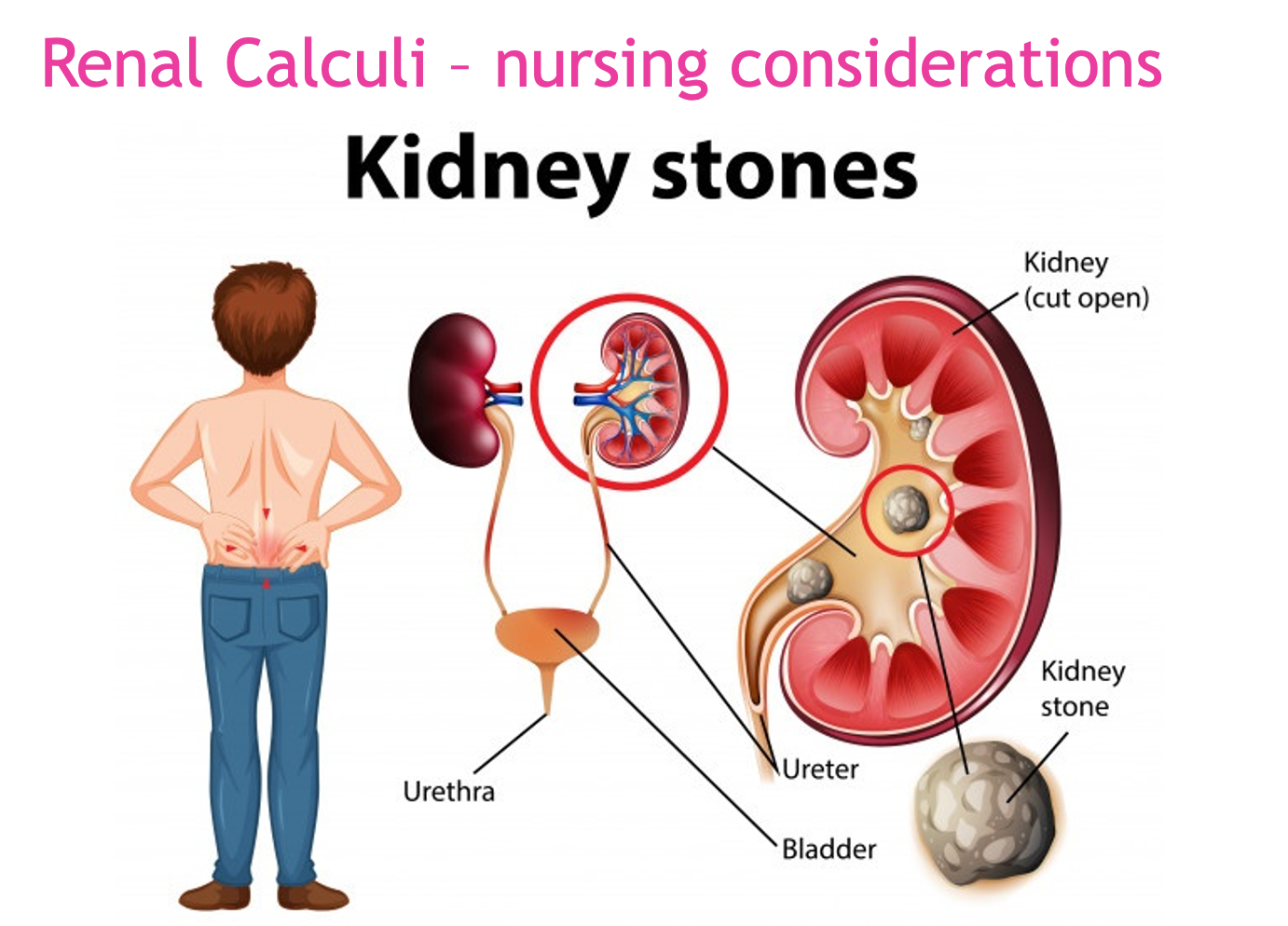
Urolithiasis + Nephrolithiasis
Causative substances
Increased serum calcium levels (most common type)
Calcium rich foods like dairy
Calcium oxalate foods - peanuts, dark leafy greens, beets, chocolate, sweet potatoes
Struvite
Starts from bacteria exposure
Most common type in women
Excess uric acid (acidic urine, pH < 5.5)
Common for people with large amounts of dietary protein (and gout)
Only about 10% of stones are this type
Generally more common in men than women
X-ray or non-contrast CT may be needed in addition to standard blood and urine tests
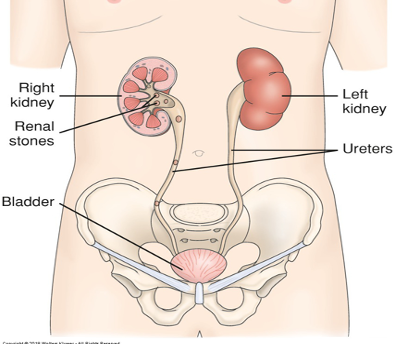
Renal Calculi - Nursing Considerations
Assessment
Pain
Signs of obstruction - dysuria, hematuria, frequency/oliguria
Fever and chills
N/V
Diaphoresis + pallor
Elevated HR, RR, and BP
Nursing Interventions
Provide analgesic therapy: opioids, NSAIDS, heat therapy to low back/flank area
Increase fluid intake, unless contraindicated; avoid activities that may cause sweating
Monitor for S/S of UTI and for blood/stones in urine (save stones for lab analysis)
Stones in the renal pelvis may be associated with an intense, deep ache in the costovertebral region
Stones lodges in the ureter (ureteral obstruction) cause acute, excruciating, colicky, wavelike pain that radiates down the thigh and to the genitalia
Monitor I&O for oliguria/anuria
Draw + monitor ordered labs
Blood chemistries and a 24-hour urine test for measurement of calcium, uric acid, creatinine, sodium, pH, and total volume may be part of the diagnostic workup
Dietary restrictions: foods high in protein, sodium, or oxalate
Sodium competes with calcium for reabsorption in the kidneys
Maintain daily recommendation of calcium, don’t restrict since it can lead to osteoporosis
Medical procedures may be ureteroscopy, lithotripsy, or nephrolithotomy
Urinary Tract Cancers
Cancers can be in any urinary organ: kidney, bladder, ureters, prostate, and surrounding structures
Diagnostics include urinary imaging, CT, MRI, ultrasound, manual exam, and biopsy
Bladder Cancer
Account for 16,000+ deaths/year
90% of cases are in age 55+
More common in men than women
Smoking is a leading risk factor
Surgical treatment is radical cystectomy with urinary diversion
Transurethral resection or cauterization may be done for benign tumors
Prostate Cancers
Over 70% of cases are in men 65+
The second most common cancer in men (skin CA is #1)
2nd highest cancer-related death rate in men (lung CA is #1)
If detcted early there is a high cure rate
Common lab - PSA; no true normal, the ideal is < 4 ng/mL
Common surgery for treatment - TURP (transurethral resection of prostate)
Urinary Tract Cancers - Assessment
Bladder CA: focus on urine characteristics mostly; UTIs, painless hematuria, and changes to voiding patterns are commonly seen
Back and pelvic pain typically is associated with metastasis
Prostate CA: may include signs of obstruction, blood in urine or semen, and painful ejaculation
Sexual dysfunction is a common early sign
Urinary Tract Cancers - Nursing Interventions
Admin of chemo/radiation
Post-surgical care for incisions, drains, and/or stomas
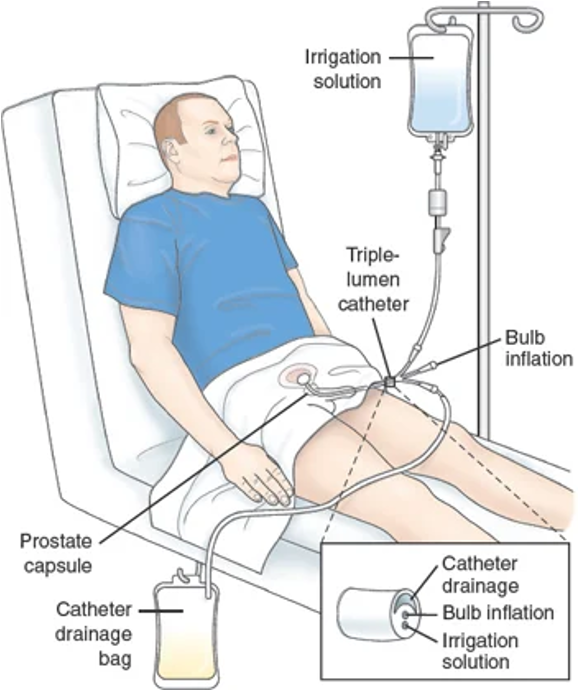
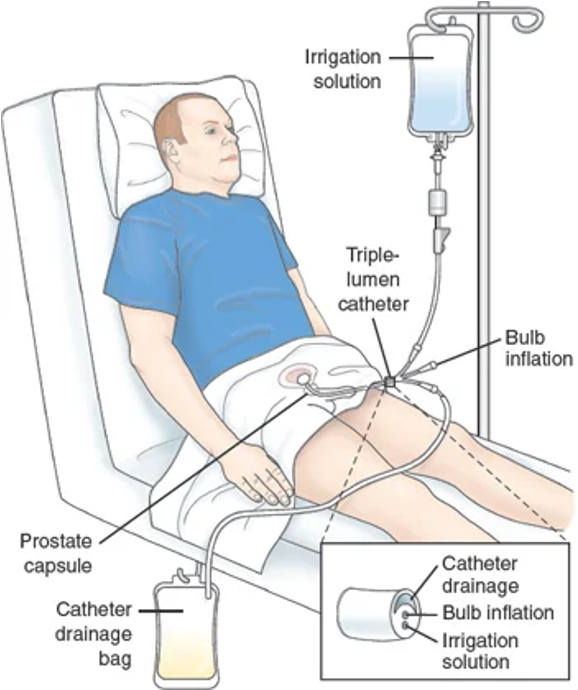
Maintain continuous bladder irrigation if order (hospitalized pt)
Skin care
Monitor urine
Encourage fluid intake
Pt education and emotional support
Nursing Diagnoses for Renal/Urological Disorders
Acute pain
Deficient knowledge
Infection, risk for
Eliminations, impaired urinary
Retention, urinary (acute or chronic)
Incontinence (be specific to which one)
Electrolyte imbalance, risk for
Fluid volume, risk for imbalanced
Injury, risk for urinary tract
*Just a sample, there are more
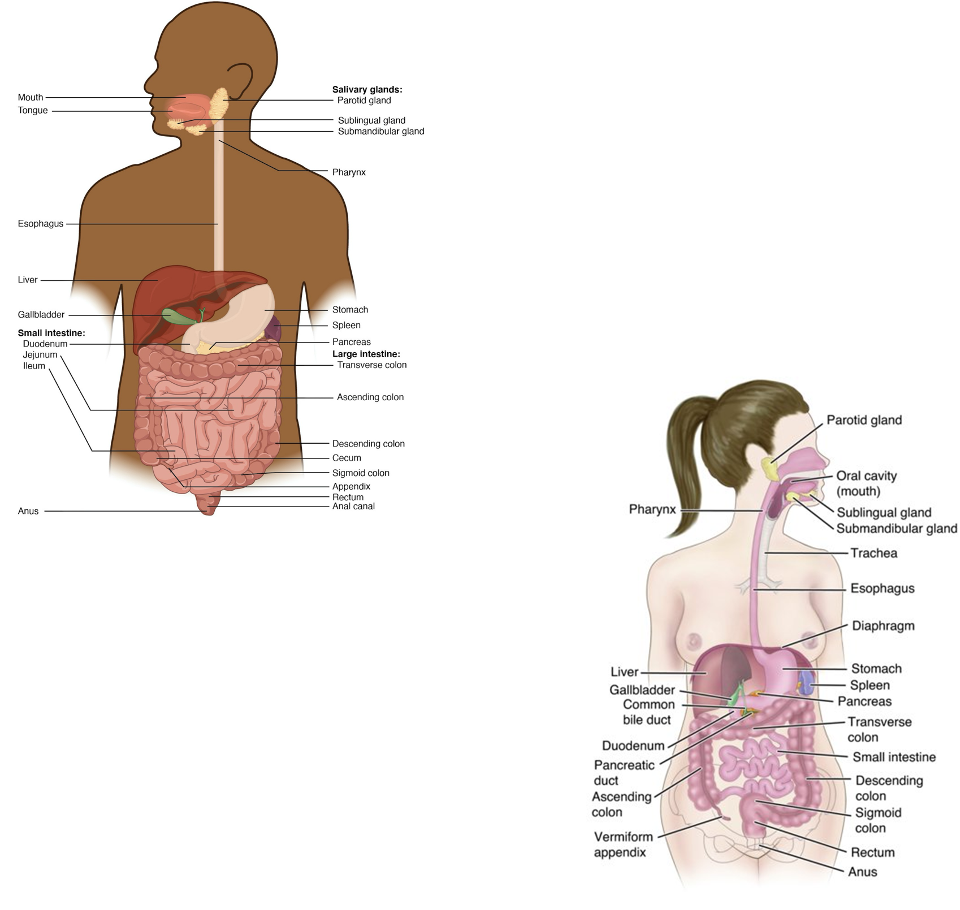
GI Anatomy - Overview
Break down food → absorb nutrients → eliminate waste
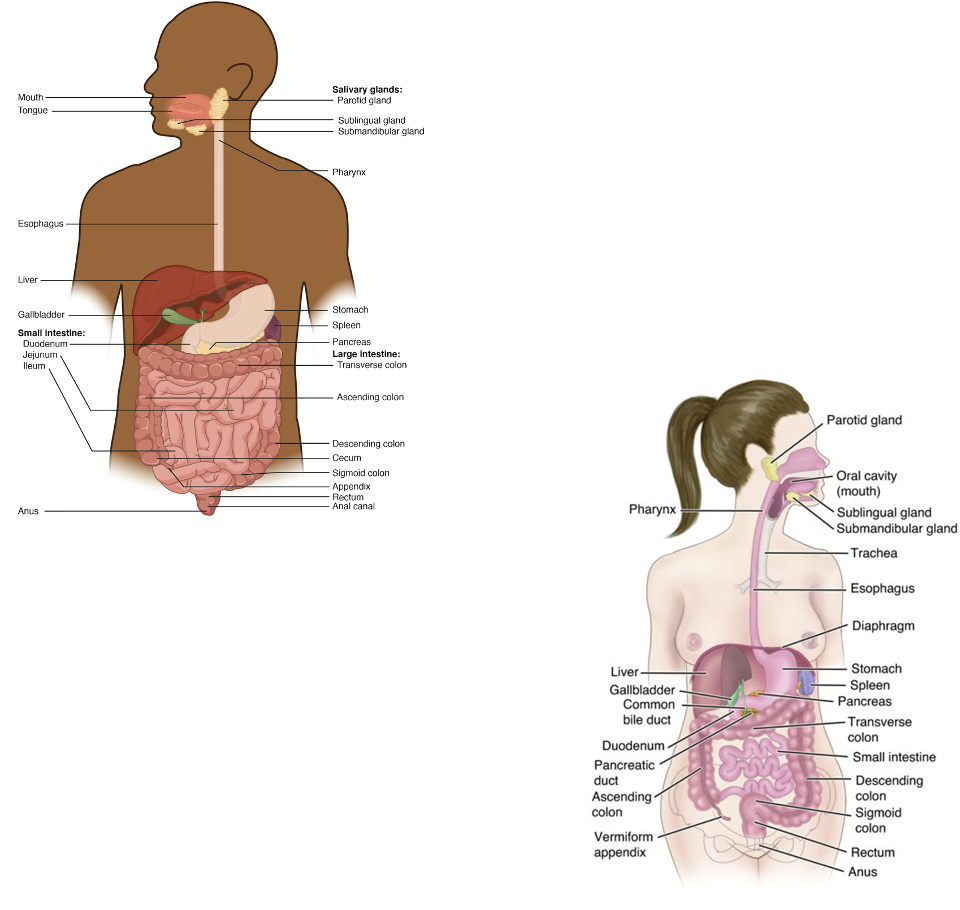
GI Anatomy - Mouth
Mechanical digestion (chewing)
Saliva
Amylase: starch → sugars
Lipase: fats
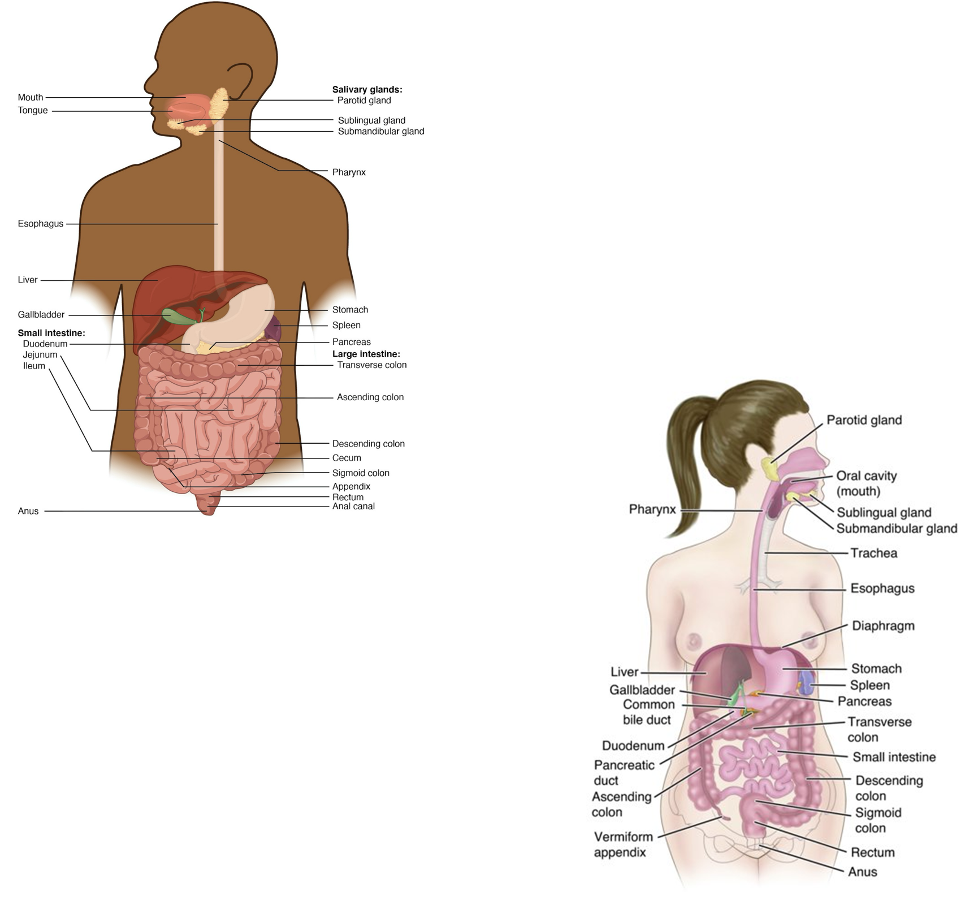
GI Anatomy - Esophagus
Stores and mixes food → chyme
Secretions
HCl: protein breakdown, bacteria destruction
Pepsin: protein digestion
Intrinsic factor: vitamin B12 absorption
Hormones
Gastrin: increases acid + motility
CCK: stimulates gallbladder + pancreas, decreases appetite
Secretin: increases bicarbonate release
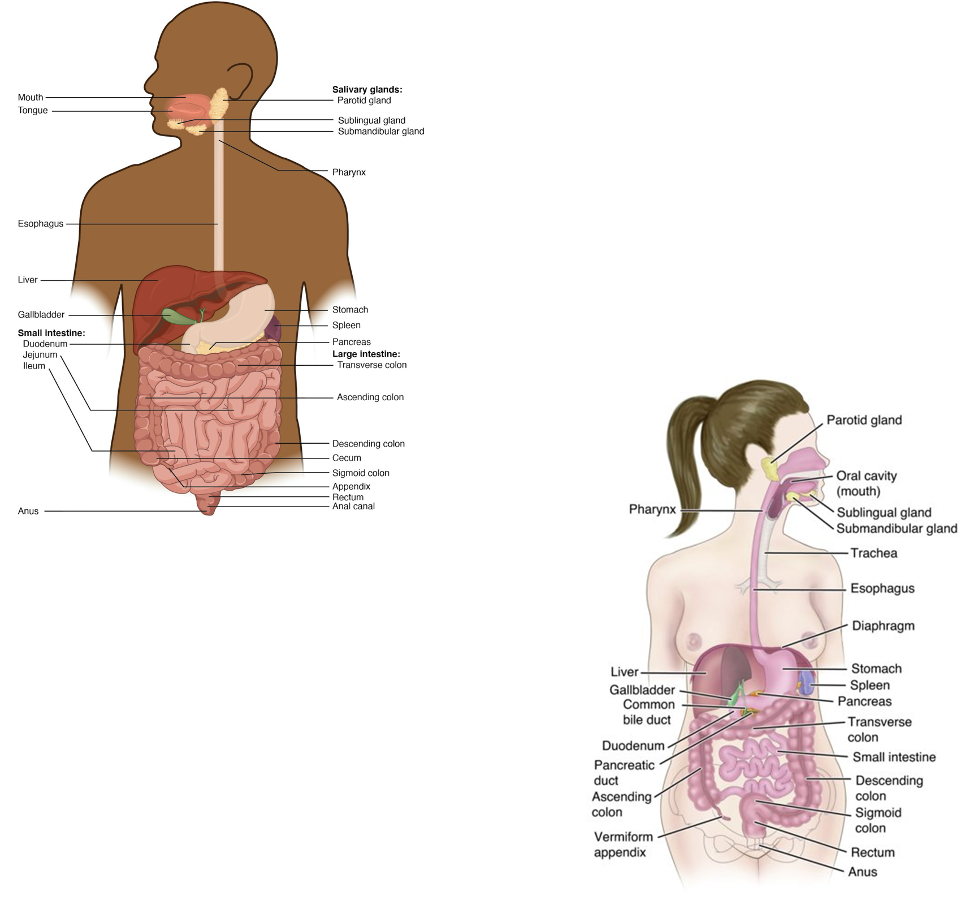
GI Anatomy - Small Intestine
Doudenum → jejunum → ileum
Primary site of digestion and absorption
Enzymes
Pancrease: trypsin, amylase, lipase
Liver/gallbladder: bile → fat emulsification
Motility
Peristalsis: propulsion
Segmentation: mixing for absorption
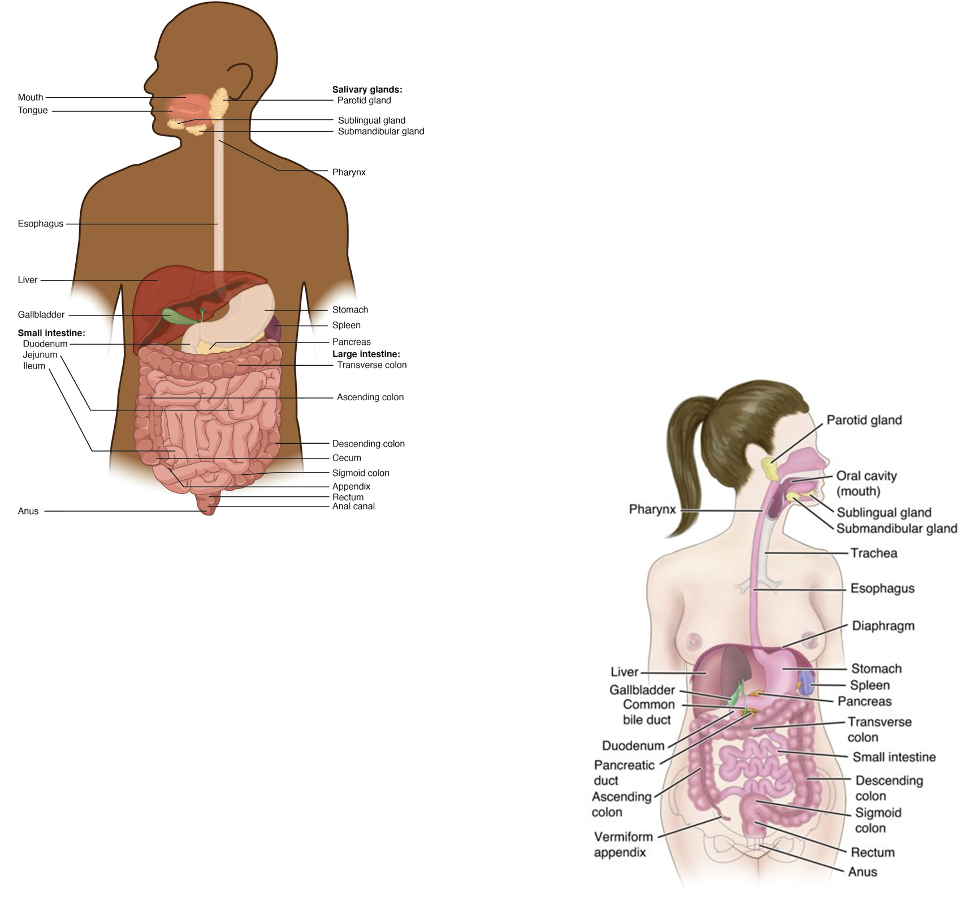
GI Anatomy - Large Intestine (Colon)
Ascending → transverse → descending
Absorbs water and electrolytes
Gut bacteria
Break down leftovers
Produce vitamins
Protect against pathogens
Secretions
Bicarbonate: neutralizes acids
Mucous: protects lining, stool movement
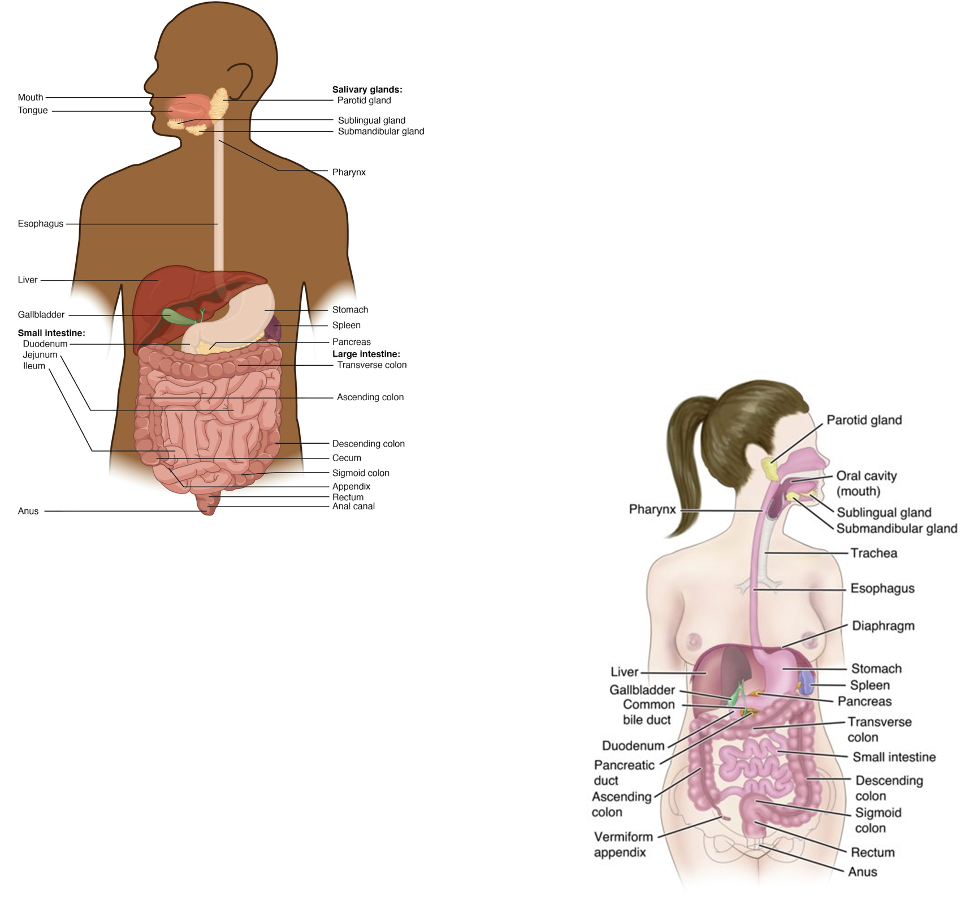
GI Anatomy - Rectum + Anus
Rectum: stores stool
External anal sphincter: voluntary control of defecation
Functions of the Digestive System
Breakdown of food for digestion
Ingestion - taking food into the mouth
Mechanical digestion - chewing and stomach-churning break food into smaller pieces
Absorption into the bloodstream of small nutrient molecules produced by digestion
Absorption - nutrients move from the small intestine into the bloodstream
Water reabsorption - the large intestine absorbs water and electrolytes
Elimination of undigested unabsorbed foodstuffs and other waste products
Elimination - waste is expelled through the rectum and anus
Gut microbiome support - beneficial bacteria aid vitamin production, immunity, and waste breakdown
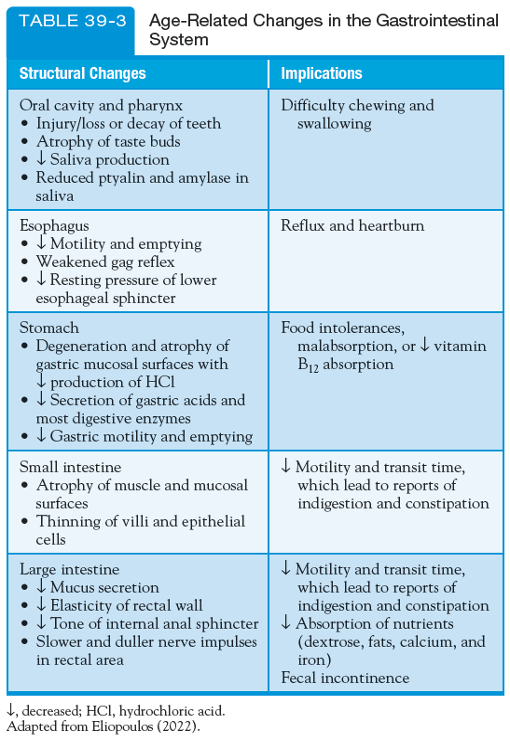
GI - Gerontologic Considerations
Normal physiologic changes of the GI system that occur with aging. Careful assessment and monitoring of S/S related to these changes are necessary. Older adult pts frequently report dysphagia, anorexia, dyspepsia, and disorders of colonic function.
Assessment of the GI System
Healthy history
A focus GI assessment is info about abdominal pain, dyspepsia, gas, N/V/D, constipation, fecal incontinence, jaundice, and previous GI disease
Physical assessment
Past health, family, social history
Pain
Presenting symptoms, character, duration, pattern, frequency, location, distribution or referred abdominal pain, and time of the pain vary greatly depending on the underlying cause
Assessment of the GI System - Health History
Ask about:
Dental hygiene, dentures, mouth sores
Usual food and fluid intake
Current and past medications
Previous GI tests or procedures
Alcohol and tobacco use
Appetite or weight changes in the past year
Assessment of the GI System - Physical Assessment
Inspection and palpation of:
Oral cavity, Lips: moisture, color, texture, symmetry, ulcers, fissures
Gums: inflammation, bleeding, recession, discoloration
Tongue: color, texture, lesions
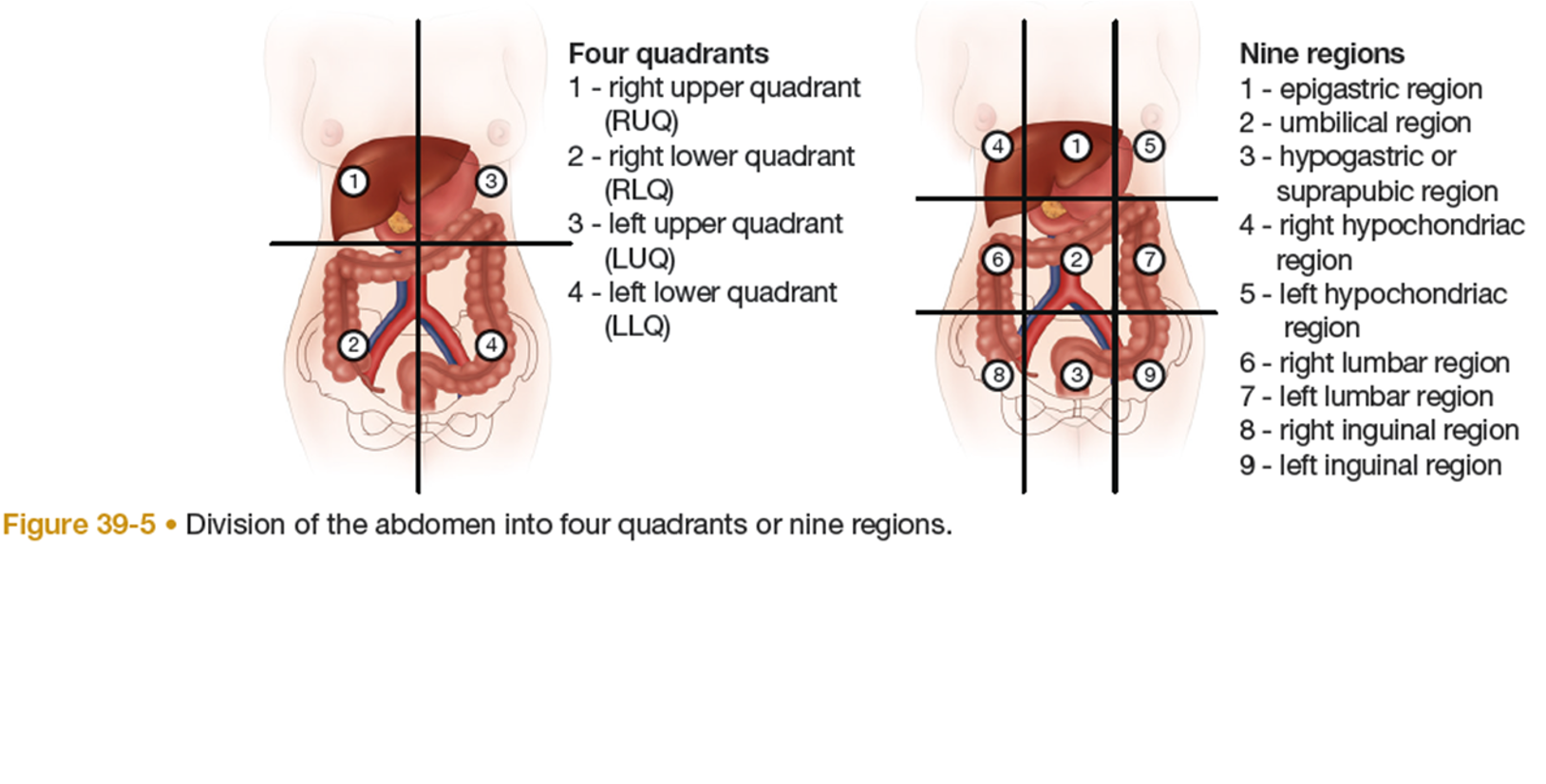
Abdominal Assessment
Use the four‑quadrant method:
Inspection
Look for skin changes, scars, lesions, discoloration, bruising, or visible masses.
Auscultation
Assess bowel sounds—normal, hyperactive, hypoactive, or absent—and note their location and frequency.
GI Pain Assessment
Evaluate: Pain
Character: sharp, dull, cramping
Duration: how long it lasts
Pattern/Frequency: when it occurs, what triggers it
Location: where the pain is felt
Radiation: whether it spreads to the back, shoulder, or other areas
Pain Assessment (GI Focus) - Abdominal Assessment (4-Quadrant Method)
1. Inspection
Look for skin changes, scars, lesions, discoloration, bruising, striae, or visible masses.
2. Auscultation
Listen for bowel sounds—normal, hyperactive, hypoactive, or absent—and note their location and frequency.
3. Percussion
Helps identify organ size and detect air, fluid, or solid masses.
Tympany: air‑filled areas (stomach, small intestine)
Dullness: organs or solid masses
4. Palpation
Light palpation: tenderness, guarding, muscle tension
Deep palpation: masses or deeper abnormalities
Rectal Assessment
May be uncomfortable; use appropriate positioning (knee‑chest, left lateral, or standing with hips flexed).
Inspect for lumps, rashes, tears, scars, hemorrhoids, fistulas, fissures, or prolapse.
Ask the patient to bear down to reveal hidden abnormalities such as internal hemorrhoids or polyps.
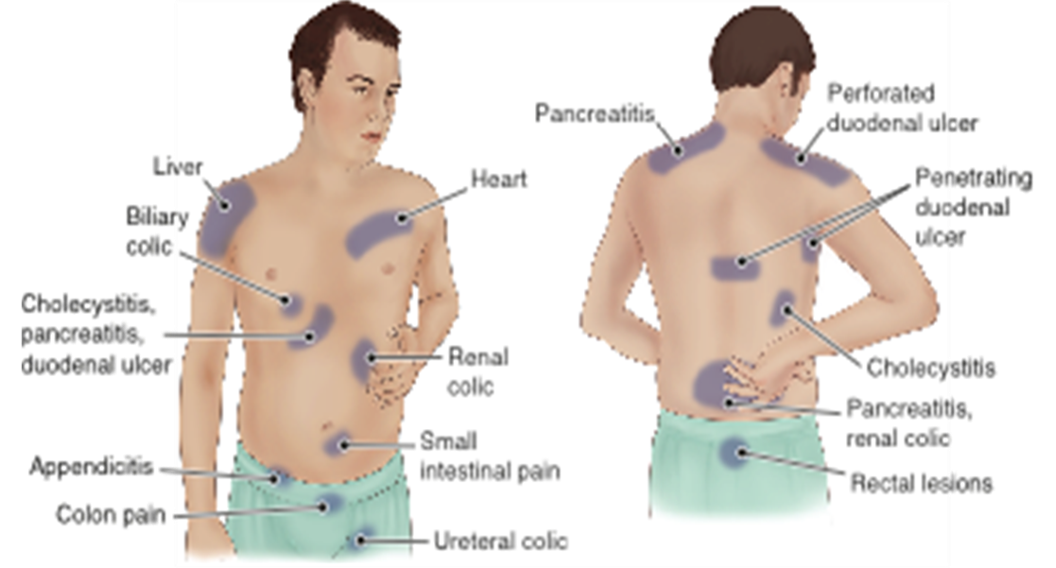
GI - Common Sites of Referred Abdominal Pain
GI - Lab Studies
CBC: Anemia or infection
CMP: Electrolytes, kidney function, liver enzymes
AST, ALT, bilirubin: Liver injury or disease
PT/PTT: Clotting ability
Amylase + Lipase: Pancreatic inflammation
Triglycerides: High levels can stress the pancreas
Cancer-specific labs
Stool tests
Breath test
Genetic testing: Identifies risk for - gastric cancer, lactose intolerance, inflammatory bowel disease, colon cancer
GI: Lab Studies - Cancer-Specific Labs
Cancer antigen (CA): Various GI cancers
Carcinoembryonic antigen (CEA): Colorectal cancer
Aplha-fetoprotein (AFP): Liver cancer (hepatocellular carcinoma)
GI: Lab Studies - Stool Tests
Identify infection, inflammation, or malabsorption
Fecal urobilinogen: High or low levels suggest liver or bile duct issues
Fecal leukocytes: WBCs in stool → inflammation or infection
Parasites: Detects worms, eggs, protozoa (Giardia, Entamoeba, helminths)
Fecal fat: High levels indicate malabsorption (celiac, pancreatic insufficiency)
C. difficile: Detects bacteria causing severe diarrhea/colitis, often after antibiotics
Fecal Occult Blood Test (Guaiac): Detects hidden blood in stool, used for early cancer screening
Avoid red meat, aspirin, NSAIDS for 72 hours (prevents false positives)
Not used if hemorrhoids are actively bleeding
GI: Lab Studies - Breath Tests
Hydrogen breath test: Carbs absorption and bacterial overgrowth
Urea breath test: Detects H. pylori (peptic ulcer disease)
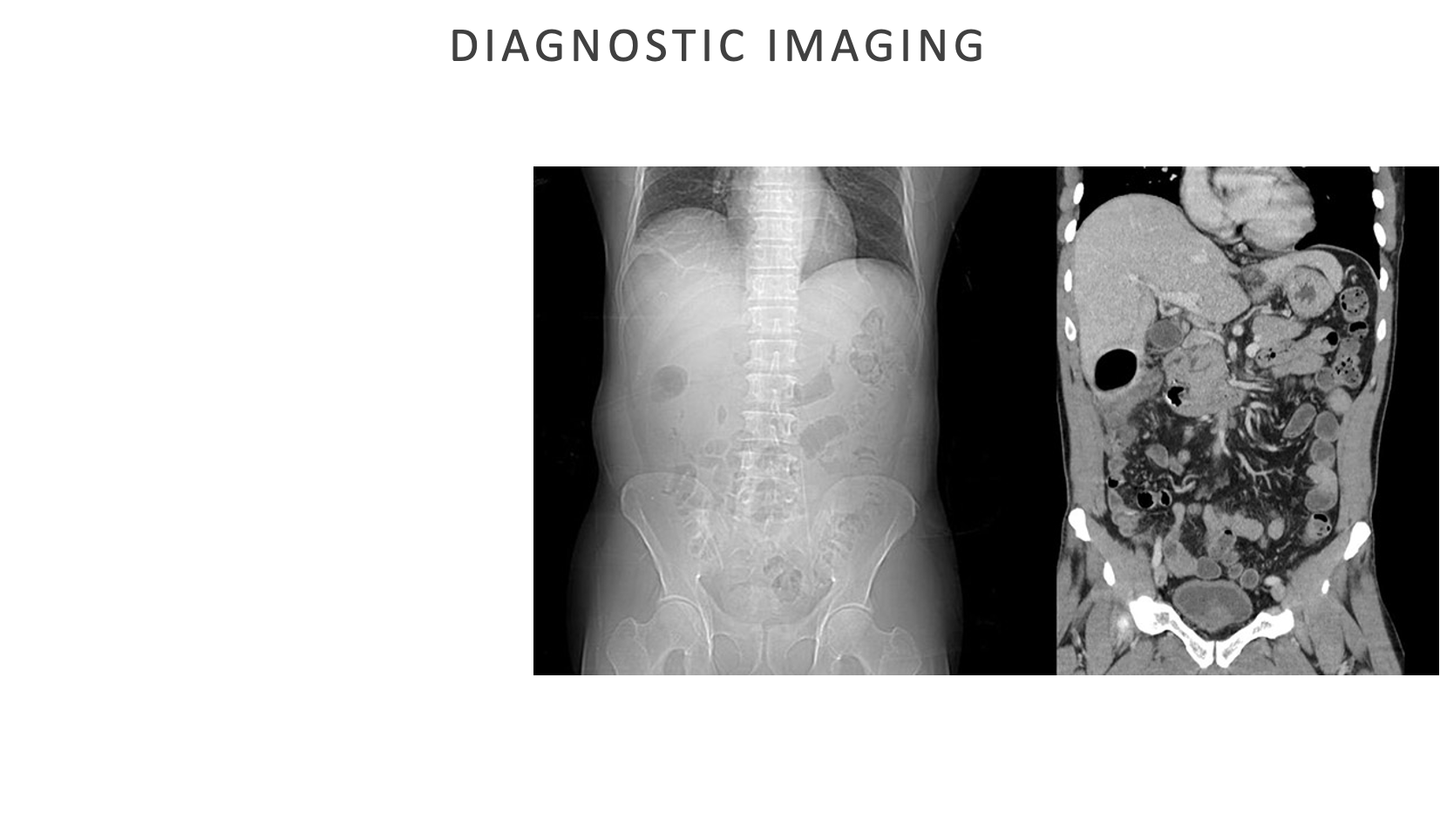
Diagnostic Imaging
Abdominal imaging tests help identify structural problems, inflammation, infections, or cancer
Diagnostic Imaging - Abdominal Ultrasonography
Uses high-frequency sound waves to visualize organs
Finds: enlarged gallbladder/pancreas, gallstones, enlarged ovary, ectopic pregnancy, appendicitis
Nursing: fast 8-12 hours to reduce bowel gas; if gallbladder is a concern (fat-free meal before fasting)
Do ultrasound before any barium studies (since it interferes with imaging)
Diagnostic Imaging - X-Ray
Shows the abdominal cavity and detects: masses, bowel obstruction, foreign objects, solid structures appear whiter on the image
Diagnostic Imaging - CT Scan (w/ or w/o Contrast)
Provides detailed cross-section images of abdominal organs and structures
Finds: appendicitis, diverticulitis, crohn’s/ulcerative colitis, liver/spleen/kidney/pancreas issues, pelvic organ problems, abdominal wall disease
Nursing: screen for contrast risks (kidney issues, allergies, pregnancy)
Some pts need premed for contrast allergy
Encourage hydration afterward to flush contrast
Diagnostic Imaging - MRI Scan (w/ or w/o Contrast)
Detailed imaging of soft tissues and blood vessels
Finds: abscesses, fistulas, tumors, bleeding sources
Nursing: NPO 6-8 hours if possible
Remove all metal/jewelry
Screen for claustrophobia
Test lasts 60-90 mins
Check for contrast contraindications
Sedation may not be required, pt will lie flat for 15-25 mins
Diagnostic Imaging - PET Scan (Nuclear Imaging)
Uses IV radioactive isotopes to detect abnormal metabolic activity, cells using more energy often for cancer evaluation
Nursing: requires a working IV
Isotopes clear through urine and stool
Radiation exposure is low because isotopes decay quickly
Diagnostic Imaging - Barium Swallow (Upper GI Series)
Barium sulfate (a radioplaque liquid contrast) is swallowed to detect disorders of esophagus, stomach, duodenum, and small intestine
Pt drinks liquid barium, coats upper GI tract
Multiple x-rays are obtained to create a continuous x-ray image
Shows shape, movement, and structural abnormalities
Detects swallowing problems, esophageal strictures or tumors, hiatal hernia, ulcers, GERD-related changes
Possible diagnoses: ulcers, varices, tumors, enteritis, and malabsorption syndromes
Nursing points:
Low‑residue diet before the test
Clear liquids + PEG laxative the evening before (if ordered)
NPO after midnight; no smoking or gum chewing because they increase secretions
Hold morning medications unless the provider gives different instructions
Insulin may need adjustment when the patient is NPO (provider decides)
Post‑procedure: Encourage hydration to help pass the barium
Expect white or light‑colored stool for 1–3 days
Diagnostic Imaging - Barium Enema (Lower GI Series)
Rectal instillation of barium that allows for visualization of the lower GI tract via x-ray
Barium is inserted into the rectum through a small tube; x-ray shows colon structure + movement
Possible diagnoses: polyps, tumors, and lesions
Diverticula, inflammatory changes, structural issues (twisting, narrowing)
Contraindications: active inflammatory disease, fistulas, perforation or obstruction of colon; active GI bleeding may prohibit use of laxatives and enemas
Nursing points:
Low‑residue diet 1-2 before the test
Clear liquids + laxative the evening before
Morning enema may be needed until returns are clear
NPO after midnight
Post‑procedure: Encourage hydration and a high‑fiber diet to prevent constipation
Stool may appear white or light for 1–3 days
Patient may feel cramping or fullness during the test
Monitor bowel movements afterward
Endoscopic Procedures - Esophagogastroduodenoscopy (EGD)
Direct visualization of esopahgeal, gastric (motility), and dudoneal mucosa
Collect secretions and tissue specimens
Topical anesthetics and moderate sedation
Diagnostic and/or therapeutic
Pt may get atropine to reduce secretions and/or glucagon to relax smooth muscle
Pt usually wares mouth gaurd to prevent biting the endoscope
Nursing care:
NPO 8 hours before procedures
Priority during procedures: airway + oxygenation
Assess for signs of perforation
Relieve minor throat discomfort
Post-procedure education
Therapeutic endoscopy
Remove common bile duct stones
Dilate strictures
Treat gastric bleeding and esophageal varices

Endoscopic Procedures - Colonoscopy
Direct visualization of the large intestine (anus, rectum, sigmoid, transcending, and ascending colon)
Moderate sedation
Diagnostic and/or therapeutic
Pt lies on left side with legs drawn up towards chest
Nursing care:
Colon cleanse education and med admin
Clear liquid or low residue diet
Moderate sedation
Priority during procedure: ABCs
Assess for perforation and hemorrhage
Therapeutic colonscopy
Removal of visible polyps, treat bleeding or area of stricture, bowel decompensation, biopsies
Contraindications
Suspected or confirmed colon perforation, acute severe diverticulitis, acute colitis
GI Intubation: Types and Rationale
Tube feedings have several advantages over parenteral nutrition: they are lower in cost, safer, usually well tolerated by the patient, and easier to use in extended care facilities and in the patient’s home. When possible, the physiological-based preference is the feed the gut
GI Intubation: Rationale - Decompression
Removes gas or fluid from the stomach or intestines to relieve pressure and distention
GI Intubation: Rationale - Levage
Flushes the stomach to remove toxins, blood, or irritants
GI Intubation: Rationale - Med Admin
Delivery of meds directly into the stomach or small intestine when PO isn’t possible
GI Intubation: Rationale - Nutritional Support
Provides enteral feeding when a pt cannot meet nutritional needs by mouth
GI Intubation: Types - Nasogastric (NG) Tube
Inserted through the nose into the stomach for short-term decompression, feeding, or med delivery
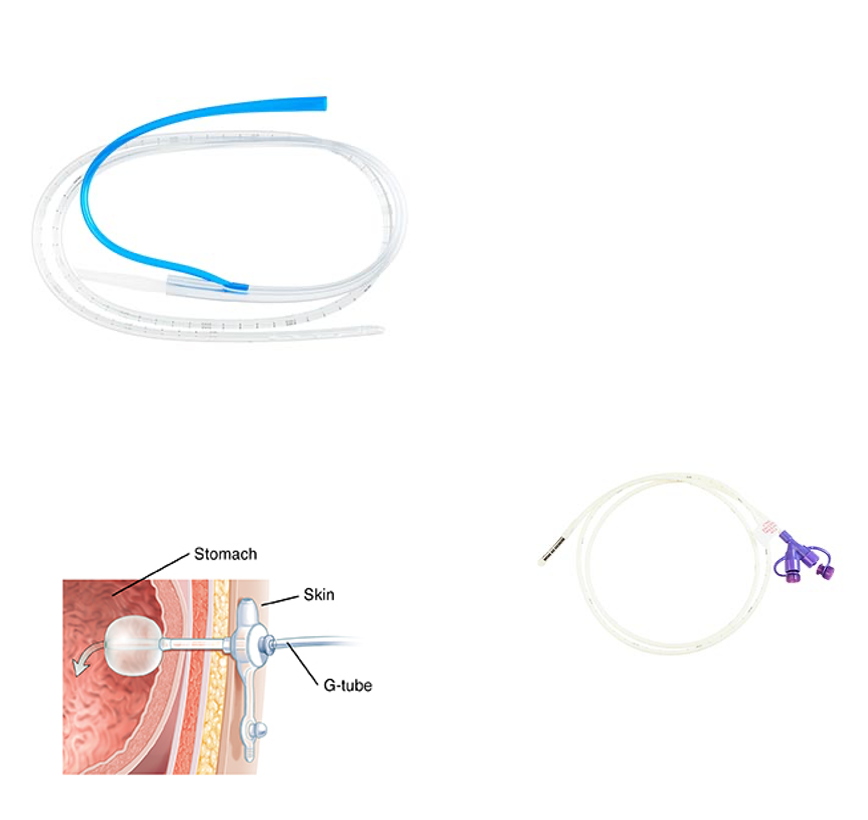
GI Intubation: Types - Nasojejunal (NJ) Tube
Inserted through the nose into the duodenum or jejunum for feeding when gastric assess is not safe or tolerated
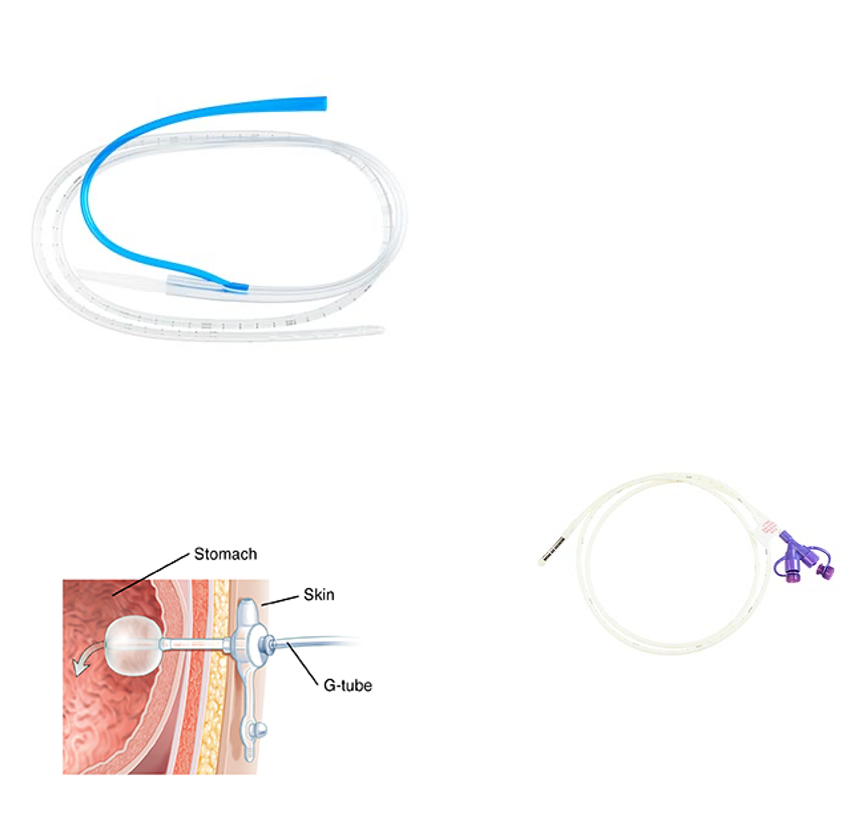
GI Intubation: Types - Gastrostomy (G Tube or PEG Tube)
Surgically placed into the stomach for long-term feeding or med admin
Done in endoscopy lab
Feedings can be started within several hours of insertion
Stoma takes 30-90 days to mature so original tube should not be replaced for at least 30 days following insertion
Replacement of tube is done per manufacturer guidelines or PRN for ruptured balloon, fistula formation, stomal tract disruption, or deterioration of tube
Tube is changed every 3-6 months
Preferred for med and nutrition admin (lasts longer than 4 weeks)
GI Intubation: Types - Jejunostomy (J Tube)
Surgically placed into the jejunum for long-term feeding when gastric feeding is not appropriate or to decrease aspiration risk when the stomach is not functioning adequately
Place in surgery, endoscopically, or radiologically
Indications: gastric route is not
Lasts 6-9 months
Preferred for med and nutrition admin (lasts longer than 4 weeks)
GI Intubation: Types - Single-Lumen Tube (Levin or Dobhoff)
Used primarily for med admin and enteral feedings because it has one simple channel
Preferred method for med admin and tube feedings