Written exam
1/152
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
153 Terms
What is the purpose of a subjective examination?
Obtain sufficient information about a persons symptoms, goals and medical history to be able to plan efficient, effective and safe physical examination and treatment
What are questions you might ask in a subjective examination?
what are they seeking help for from you?
what are their goals?
can you help them?
What are the main components of a subjective assessment?
patient information
body chart
behaviour of symptoms
history of presenting complaints
special/ screening questions
social history
family history
interests
patient perspective
previous experiences with physiotherapy
flags
Patient information
age, gender, occupation
Body chart
Where are the main areas of symptoms (if more than 1 area, marks P1, P2, P3. Tick areas that are pain free)
Other symptoms related to the main area of symptoms (p&n, numbness, referred pain. Note presence or absence of it)
Severity and superficial or deep
Constant/intermittent/variable
Nature of symptoms (sharp/dull/throbbing/pulling)
Other areas of body with symptoms
Relationship of all symptom areas
Behaviour of symptoms
aggravating factors
easing factors
24-hour pattern
irritability
status
Special/screening questions
General health (GHx)
Loss of weight (LOW) and/or history of cancer (Hx Ca)
Night pain
Major illness/injuries/surgeries
Current medications
Corticosteroid use
Anticoagulants
Body mass index
Physical activity (PA) levels
Imaging (X-ray, CT, MRI, bone scan)
Blood tests
Flags
Orange - mental health factors
Yellow - psychological factors
Blue - social factors
Black - litigation and threats to financial security
When does manual handling occur?
When any person, animal or object is:
lifted or lowered
pushed or pulled
carried
moved
held
restrained
What is hazardous manual handling?
repetitive or sustained application of force, awkward posture or movement
Application of high force
exposure to sustained vibration
Manual handling of live persons or animals
manual handling of loads which are unstable, unbalance or difficult to grasp or hold
What is the aim of manual handling techniques?
Protect ourselves from injury and protect person/object you are handling from injury/damage
How to minimise risk of manual handling?
identify the hazard
assess the risk
use hierarchy of control strategies
monitor and review the control measures
What is masssage?
Is a mechanical stimulation of tissues by means of rhythmically applied pressure and stretching
Why is massage used?
increase flexibility, coordination, venous return and blood flow
to reduce muscle spasm
to promote relaxation
to decrease neuromuscular excitability and pain
to stimulate circulation
to facilitate healing and restore joint mobility
to remove lactic acid and oedema
When is massage indicated?
increase range of motion
stretch scar tissue/ ahdesions
alleviate muscle cramps
decrease pain
remove edema
increase blood flow
When is massage contraindicated?
acute contusions
acute inflammatory conditions
severe varicose veins
open wounds/ abscesses
failed or incomplete fracture healing
thrombophlebitis and embolisms
What are the massage techniques?
Stroking
effleurage
petrissage
kneading
tapotement
friction
trigger point
What are the components of an objective assessment?
Observation
Palpation
Functional movements
Active range of movement
Passive range of movement
Muscular system
Nervous system
Special tests
Clearing tests
What are functional movements?
Asking patient to do activities that reproduce the pain or symptoms e.g. walking, running, jumping or hopping
Active range of motion (AROM)
assessing the patients ability to actively move limb themselves
Passive range of motion (PROM)
movement produced by the therapist while the patient remains relaxed
Isotonic
Muscle changes length during contraction. Movement occurs.
Isometric
Muscle contracts without movement. Position held against resistance.
What are the clinical indication of cold therapy?
Acute injuries
Post surgery
pain
Pain due to muscle spasm
spasticity
Change muscle responsiveness
Inflammation
What are the contraindications of cold therapy?
Cardiovascular diseases
High blood pressure
Cold hyposensitivity
What are the benefits of cold therapy?
Reduce inflammation
Accelerate muscle recovery
Ease the soreness of the muscle
What are the risk factors of cold therpay?
Rapid increase in heart rate and blood pressure
What are the contraindication of heat therapy?
Sensation issues
Cardiovascular conditions
Open wounds
What are the benefits of heat therapy?
Relieve pain
Reduce pain tension
Improve muscle flexibility
What are the risks of heat therapy?
Burns
What is clinical reasoning?
Is the process of deciding which factors are relevant to a patients presenting problem, then deciding what to do about them
Why is clinical reasoning important?
each person we assess/treat is unique
clinical guidelines and results can only provide general guidelines to strategies of assessment and treatment
clinicians must then use their own clinical reasoning skills to determine how best to proceed with each patient
What are the 3 models of clinical reasoning?
WHO ICF
Intervention Process Model
Collaborative reasoning model (hypothesis categories)
Hypothesis categories
Activity & participation capability & restriction
Patients’ perspectives on their experiences & social influences (psychosocial status
Pain type
Sources of symptoms
Pathology
Impairments in body function or structure
Contributing factors to the development & maintenance of the problem
Pre-cautions & contraindications to physical examination and treatment
Management/treatment selection and progression
Prognosis
Pain types
nociceptive
neuropathic
nociplastic
Nociceptive pain
pain that is associated with actual or threatened damage to non-neural tissue and involves the activation of peripheral nociceptors e.g. inflammatory and mechanical pattern, clear aggravating and easing factors
Neuropathic pain
pain associated with a lesion or disease of the somatosensory nervous system e.g. sharp, burning sensation, pins and needles and numbness
Nociplastic pain
Nociplastic pain is pain that continues even when there is no clear tissue damage and no obvious nerve injury.
What is a problem list?
It is a list of problems that may require treatment, management or re-assessment
What does a problem list help with?
It helps to plan and guide your patients management plan and prognosis
How to develop a problem list?
Subjective examination findings: activity restrictions, participation restriction
Physical examination findings: physical impairments
How to make goals SMART?
Specific: Well defined, clear, and unambiguous
Measurable: specific criteria that measure progress towards the accomplishment of the goal
Achievable: Attainable and not impossible to achieve
Realistic: Within reach, realistic, and relevant to your life
Timely: With a clearly defined timeline, including a target date
SMART goals need to be written in one sentence
What are outcome measures?
An outcome measure is a measure or tool, to assess a person’s current or future health status and demonstrate the effectiveness of an intervention or treatment
What are the stages of healing?
Days 0-5: inflammatory period
Days 0-2: vascular phase (new capillaries, re-innervation)
Days 3-5: Cellular phase (lymphocytes, macrophages)
Days 6-21: proliferation period
Fibroblasts start to form new collagen
Takes 21 days to reach full repair of collagen
22 days onwards: organisation period and maturation phase
What are the stages of tissue healing?
homeostasis and inflammation - days 2-3
proliferation (fibroblastic) - days 3-5 lasts 2-4/52
remodelling (maturation) - days 21 to 12 months
Factors that affect healing
severity of injury
vasculation of tissue and circulation
age
drugs
surgical repair
infection
nutrition
immobilisation
general health
treatment
Factors affecting how we prescribe exercises
How severe was the injury/surgery?
Stage of healing
What are the current pain levels?
Patient goals e.g. return to sport/ work
What factors do you want to work on? E.g. neuromuscular/motor control, range of motion, strength, endurance, power, muscle length, combination of these factors
Muscles involved e.g. fast twitch/phasic or slow twitch/tonic
What is the function of the muscle within the body?
Baseline activity levels
What is irritability?
the measure of how easily a patient's symptoms are aggravated, the intensity of those symptoms, and how long they take to subside
What is a hazard?
any agent, condition, or situation with the potential to cause harm, damage, or adverse health effects to humans, property, or the environment
What is a risk?
risk is the likelihood and severity of the hazard actually occurring
Types of hip pain
hip oesteoarthritis
extra articular hip tendinopathies
hip related pain (non-OA)
What is hip osteoarthritis (OA)?
Osteoarthritis (OA) is a clinical syndrome characterised by joint pain, varying degrees of functional limitation, and reduced quality of life. It develops as a response to joint injury, which may result from repeated microtrauma over time or a significant single insult. Physiologically, OA involves the progressive loss of articular cartilage, remodelling of the underlying bone, and varying levels of joint inflammation.
What is the subjective assessment for hip OA?
Groin pain with mechanical and inflammatory behaviours (pain on loading, pain and morning stiffness)
Problems putting shoes and socks on
Loss of mobility of hip joint (bony changes, capsular irritation and thickening, muscle tightness, especially IR +/- F ROM)
NICE Guidelines Diagnostic Criteria
can diagnosis a person with OA with imaging/ investigation if:
Age > 45 years
has activity related joint pain
has either no morning joint stiffness or morning stiffness that lasts no longer than 30 mins
Altman diagnostic criteria
can diagnose a person with OA if:
hip pain and hip internal rotation < 15 deg and hip flexion < 115deg
hip internal rotation > 15 deg and pain on hip internal rotation and morning stiffness that lasts < 60 mins and age > 50 years
Hip OA objective examination
functional movements (activity): sit to stand, stairs, gait - walking, stairs
30 sec sit to stand
timed up and go
6 minute walk test
observation of gait
PROM and AROM
muscle tightness
muscle atrophy/weakness in quads and glutes
Hip OA diagnostic takeaways
morning stiffness 30-60 mins
trouble putting shoes and socks on in the morning
deep hip pain that is activity related
impairments - restricted hip internal rotation +/- restricted hip flexion
Hip OA conservative management
treatment and management is guided by goals ad finding on assessment
education (exercise benefits, encourage behaviour change)
local muscle strengthening (increase muscle strength all around hip, glutes, quads and back)
heat/cold therapy for pain relief
manual handling and stretching (increase or maintain joint ROM)
gait aids
refer to GP for pain relief or if pain doesn’t improve with physiotherapy for surgical options
Types of surgical management
Hip resurfacing
Partial hip replacement
Total hip replacement
Lateral hip pain - Greater Trochanteric Pain Syndrome
Greater trochanteric pain syndrome (GTPS) is a common condition causing chronic, persistent pain on the outer (lateral) side of the hip and thigh. It occurs when the tendons and bursa that wrap over the hip bone's bony prominence (the greater trochanter) become irritated, overloaded, or damaged.
Risk factors of lateral hip pain
female
over the age of 40
lower back pain
high weight/BMI
Lateral hip pain subjective examination
pain on outside of the hip
Aggravating activities - lying on side at night, walking, climbing up/down stairs, walking up stairs and hill, sitting
24 hour pattern - disturbs sleep
History - gradual onset or a change in training load or physical activity
imagining - thickening/thinning/tears of gluteus medius/gluteus minimus tendons
Lateral hip pain objective examination
observation - gait (may have trendelenburg sign)
palpation (pain on palpation greater trochanter and common gluteal tendon)
functional tests - single leg stance, single leg squats, step up, hop
special test: resisted hip abduction, resisted hip ER de-rotation, FABER, obers, single leg stance (all will have pain provocation)
education: reduce compression at greater trochanter, avoid - standing with weight on one leg, sitting with legs crossed, sleeping on side with top leg/hip forward in a flexed and adducted position. Sleep on back with pillow under knees. Strengthen gluteus medius/minimus - sit to stand, ½ squat, bridging, stepping
Lateral hip pain treatment
need to slowly progress exercise
manual therapy - soft tissue work at muscle belly (don’t irritate the tendon)
mechanical - single point stick in same hand as painful hip
Refer to GP for pain relief
don’t stretch gluteus medius as it causes compression at greater trochanter
What is motion in arthrokinematics?
motion - motion of a joint is the result of movement of one joint surface in relation to another
Movements that occur at joint surfaces = slides (glides), rolls and spins
What is a slide movement is arthrokinematics?
sliding of one joint surface over another - translatory movement
What is a spin movement is arthrokinematics?
All points of a joint on the moving joint rotate on a fixed axis of motion - rotary motion
What is a roll movement in arthrokinematics?
a forward and backward rolling motion similar to that of a bottom of a rocking chair - rotary motion
What are the planes of movement
sagittal (divides the body into left and right - flexion and extension)
frontal (divided the body into anterior and posterior - abduction and adduction)
transverse (divides the body into upper and lower sections - rotation)
What is end feel?
sensation that is transmitted to the examiners hands at the extreme end of PROM and that indicated the structure that is limiting joint movement
What is normal end feel?
when there is full PROM and normal anatomy limits/stops the movement
What is abnormal end feel?
occurs when there is an increased or decreased PROM (outside the normal range), or when there is normal PROÂ, but the structures other then the normal anatomy limit the movement
Soft end feel
When 2 surfaces come together and there is a soft spongy feel e.g. elbow flexion
Firm end feel
firm or spongy sensation that has a little give when muscle is stretched or firm stop to movement when capsule or ligaments are stretched e.g. ankle DF
Hard end feel
Abrupt hard stop to movement when bone contacts bone e.g. elbow extension
How to measure ROM
Axis of the goniometer is placed at either the axis of movement of the joint or a landmark that can represent the axis of movement
Stationary arm is placed parallel to the longitudinal axis of the fixed proximal joint or segment, or points to the distal bony prominence
Moveable arm is placed parallel to the longitudinal axis of the distal joint or segment, or points to the distal bony prominence
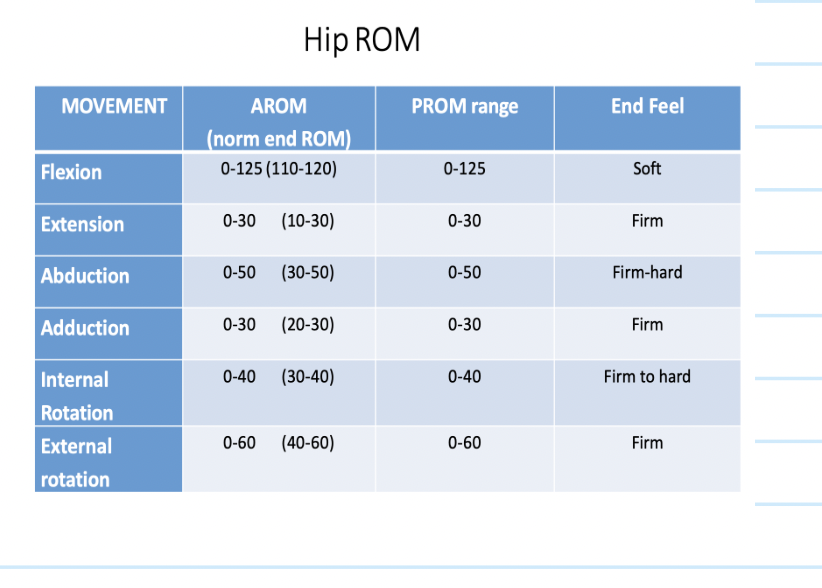
Hip ROM
What is palpation?
Is a method of feeling with the fingers or hands during a physical examination to evaluate the structures beneath
Prior to palpation what do you need to do?
ensure the client is comfortable
the therapists body positioning
expose the area that we need to assess
When palpating you need to be …
deliberate, purposeful and systematic
consider irritability/pain
use pads of fingers
compare to other side
palpate superficial to deep
During palpation the following should be noted …
temperature chnages of the area
localised increased skin mosture
presence of oedema/effusion
mobility and feel of superfical tissues
muscle spasm, guarding, knots, tenderness
Common hip and groin conditions
Femoroacetabular impingement syndrome (FAI)
Acetabular dysplasia and/or hip instability
other conditions: labral tears, chondral lesions, ligamentum teres tears
Acetabular dysplasia
Misalignment between the femoral head and acetabulum secondary to changes in shape/size/orientation. Instability and overload of the acetabular rim
FAI syndrome
Is a motion related clinical disorder of the hip with a triad of symptom, clinical sings and imaging findings. It represents symptomatic premature contact between the proximal femur and the acetabulum
FAI subjective examination
motion or position related pain in hip or groin
pain may be felt in back, buttock or thigh
patient may describe clicking, catching, locking, stiffness, restricted ROM, giving way
Deep groin pain worse in FADIR functional positions
often presents with generalised groin pain
may complain of chronic back/gluteal pain
kicking sports, martial arts
FAI objective examination findings
pain on hip impingement test (FADIR)
limited ROM - restricted internal rotation in hip flexion
imaging - x-ray confirmation of cam/pincer morphology
FAI objective examination
functional movements: DL squat - reduced squat depth, single leg balance - poor balance
AROM and PROM - IR may be restricted or imbalance between affected and non affected hip
Muscle strength - reduced strength in hip adduction, abduction, flexion, internal rotation, external rotation
imbalance between affected and non-affected hips
Special tests - pain on anterior impingement test (FADIR), IR at 90 deg hip F less than 20 deg = FAI, pain and reproducible clunk/catch on hip quadrant test
FAI standardised outcome measures
patient reported outcome measures
hip and groin out come score (HAGOS)
international hip outcome tool (iHOT)
FAI treatment/managment
strengthen around the hips
manual therapy to soft tissues
stretching
Risk factors of groin pain
previous injury
pain and reduced strength on adductor squeeze test prior to onset of symptoms
reduced hip internal rotation/bent knee fallout
Groin pain subjective examination
pain in the groin area
aggravating factors include kicking and change of direction, pain during and after exercise, tight/stiff during or after activity
24 hour pattern - pain/stiffness in morning, especially after training/playing
History: loss of acceleration, max speed, distance with kick. Previous groin injury. Increase in training load
Groin pain objective examination
functional movements: single leg stance, single leg squat, kicking motion
AROM/PROM: Hip IR and ER ROM at 90deg hip F and in neutral
muscle strength: squeeze test and pain rating at 60deg hip F
Isometric strength around hip in all directions - will have weakness and asymmetries between abduction and adduction and between affected and unaffected leg
special tests: FADIR and FABER
Palpation
Groin pain standardised outcome measures
hip and groin outcome score (HAGOS)
hip outcome score (HOS)
international hip outcome score (iHOT)
Groin pain diagnosis
pain in affected region that worsens on exercise
pain on palpation, resistance testing and stretching
pain resistance testing should be felt in the affected area structures and reproduce the patients familiar/recognisable pain
Adductor related groin pain
adductor tenderness on palpation and pain on resisted adduction testing
Illiopsoas related groin pain
iliopsoas tenderness
pain on resisted hip flexion
pain in stretching the hip flexors
Inguinal related groin pain
pain at location of the inguinal canal
tenderness of the inguinal canal
no palpable inguinal hernia
pain on reisted testing of the abdominal muscles
Pubic related groin pain
local tenderness on palpation of the pubic symphysis and immediately adjacent bone
no particular resistance test will provoke pubic-related groin pain
Hip related groin pain
FAI syndrome can refer to the groin
common cause of groin pain
Groin pain treatment/management
education
Physiotherapy specific: address stability, increase ROM - manual therapy and stretching, address strength deficits
address overtraining