CHAPTER 1: INTRODUCTION TO PRELIMINARY DIAGNOSIS OF ORAL LESIONS
1/99
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
100 Terms
After arriving at a differential diagnosis, information from which one of the following categories will best establish a final or definitive diagnosis?
a. Clinical
b. Historical
c. Microscopic
d. Radiographic
c. Microscopic
The descriptive term that would best be used for a freckle is a:
a. Bulla
b. Vesicle
c. Lobule
d. Macule
d. Macule
Which one of the following terms describes the base of a lesion that is stalklike?
a. Sessile
b. Lobule
c. Pedunculated
d. Macule
c. Pedunculated
Bulla (adjective, bullous; plural, bullae)
A circumscribed, elevated lesion that is more than 5 mm in diameter, usually contains serous (serous meaning; resembling or producing serum) fluid, and looks like a blister.
Lobule (adjective, lobulated)
A segment or lobe that is a part of the whole; these lobes sometimes appear fused together.
Exampled: Lobulated torus palatinus
Papule
A small, CIRCUMSCRIBED lesion usually LESS than 1 cm in diameter that is ELEVATED or PROTRUDES ABOVE the surface of normal surrounding tissue.
Vesicle
A small, elevated lesion LESS than 1 cm in diameter that contains SEROUS FLUID.
Nodule
A palpable SOLID lesion up to 1 cm in diameter found in soft tissue; it can occur ABOVE, LEVEL WITH, or BENEATH the skin surface.
Palpation
The evaluation of a lesion by feeling it with the fingers to determine the texture of the area; the descriptive terms for palpation are SOFT, FIRM, SEMIFIRM, & FLUID FILLED; These terms also describe the consistency of a lesion.
Colors
Red, pink, salmon, white, blue-black, gray, brown, and black are the words used most frequently to describe the colors of oral lesions; they can be used to identify specific lesions and may also be incorporated into general descriptions.
Erythema
an abnormal REDNESS of the mucosa or gingiva.
Erythroplakia
A clinical term used to describe an oral mucosal lesion that appears as a SMOOTH RED PATCH or GRANULAR RED & VELVETY PATCH.
Leukoplakia
A clinical term for a WHITE PLAQUELIKE LESION on the ORAL MUCOSA that CANNOT be RUBBED OFF or DIAGNOSES as a specific disease.
Pallor
Paleness of the SKIN or MUCOSAL tissues.
Pedunculated
Attached by a STEMLIKE or STALKLIKE BASE similar to that of a MUSHROOM.
Exampled: Fibroma with a pedunculated based
Sessile
describing the sized circumscribed elevations containing PUS.
Exampled: Fibroma with sessile base
Pustules
Variously sized circumscribed elevations containing PUS.
Clinical diagnosis can be used to determine the final or definitive diagnosis of all of the following EXCEPT:
a. Fordyce granules
b. Underupted supernumerary teeth
c. Mandibular tori
d. Erythema migrans
b. Underupted supernumerary teeth
Radiographic diagnosis would contribute to the definitive diagnosis of all of he following EXCEPT:
a. Internal resorption
b. Periapical cemento-osseous dysplasia
c. Odontomas
d. A retained deciduous tooth
d. A retained deciduous tooth
To determine the presence of blood DYSCRASIAS, which one of the following would provide the most definitive information?
a. Laboratory blood tests
b. Bleeding during probing
c. Pallor of the gingiva and mucosa
d. Patient complaint of weakness
a. Laboratory blood tests (check answer for verification in the textbook)
When an antifungal ointment or cream is used to treat angular cheilitis, which one of the following diagnostic categories is being used?
a. Clinical
b. Therapeutic
c. Laboratory
d. Differential
b. Therapeutic (Confirm answer with textbook)
Yellow clusters of ectopic SEBACEOUS GLANDS commonly observed on the buccal mucosa & evaluated through clinical diagnosis are most likely:
a. Lipomas
b. Fibromas
c. Fordyce granules
d. Linea alba
c. Fordyce granules
A slow-growing, bony, hard, exophytic growth on the midline of the hard palate is developmental & hereditary in origin. The diagnosis is determined through clinical evaluation. You suspect:
a. Torus palatinus
b. Mixed tumor
c. Palatal cyst
d. Nasopalatine cyst
a. Torus palatinus
The "white line" observed clinically on the buccal mucosa that extends from anterior to posterior along the occlusal plane is:
a. Leukoedema
b. Leukoplakia
c. Linea alba
d. Lichen planus
c. Linea alba
Which one of the following occurs as an erythematous area, is devoid if filiform papillae, is oval to rectangular in shape, does not change its characteristics, and is located on the midline of the dorsal surface of the tongue?
a. Median rhomboid glossitis
b. Erythema migrans
c. Fissured tongue
d. Lingual thyroid
a. Median rhomboid glossitis
Which one of the following diagnostic categories would the dental hygienist most easily apply to the preliminary evaluation of oral lesions?
a. Microscopic
b. Clinical
c. Therapeutic
d. Differential
b. Clinical
These examples of EXOTOSES are found on the lingual aspect of the mandible in the area of the premolars. They are benign, bony, hard, and require no treatment. Radiographically they appear as radiopaque areas and are often bilateral. You suspect:
a. Retrocuspid papilla
b. Lingual mandibular bone concavity
c. Genial tubercles
d. Mandibular tori
d. Mandibular tori
Which one of the following terms is most often used when describing mandibular tori?
a. Bullous
b. Lobulated
c. Sessile
d. Pedunculated
b. Lobulated (check answer in textbook)
Which of the following conditions is a BENIGN ANOMALY, has a diffuse GRAY-TO WHITE OPAQUE appearance on the BUCCAL MUCOSA, and is most commonly seen in adult black individuals?
a. Leukoedema
b. Linea alba
c. Erythema migrans
d. Leukoplakia
a. Leukoedema
A patient has the clinical signs of NECROTIZING ULCERATIVE GINGIVITIS. The hygienist has the patient begin HYDROGEN PEROXIDE RINSES without culturing the bacterial flora. This action applies to which one of the following diagnostic categories?
a. Therapeutic
b. Microscopic
c. Clinical
d. Final or definitive
a. Therapeutic
A small circumscribed lesion usually LESS THAN 1 cm in diameter that is elevated and PROTRUDES above the surface of normal surrounding tissue is called a:
a. Bulla
b. Macule
c. Vesicle
d. Papule
d. Papule
The base of a SESSILE lesion is:
a. Broad and flat
b. Stemlike
c. Corrugated
d. Lobulated
a. Broad and flat
The identification of which one of the following is NOT determined by clinical diagnosis?
a. Fordyce granules
b. Tori
c. Compound odontoma
d. Retrocuspid papilla
c. Compound odontoma
Another term for ERYTHEMA MIGRANS is:
a. Allergic tongue
b. Median rhomboid glossitis
c. Geographic tongue
d. White hairy tongue
c. Geographic tongue
The cause of supernumerary teeth is most likely:
a. Genetic
b. Traumatic
c. Cystic
d. Systemic
a. Genetic
Historical diagnosis can include the patient's:
a. Age and sex
b. Family history
c. Medical history
d. All of the above
d. All of the above
Which condition is most often seen on the buccal mucosa?
a. Melanin pigmentation
b. Fordyce granules
c. Nicotine stomatitis
d. Angular cheilitis
b. Fordyce granules
Which one of the following is NOT considered a variant of normal?
a. Migratory glossitis
b. White hairy tongue
c. Fissured tongue
d. Hairy Leukoplakia
d. Hairy Leukoplakia
Side Note:
Which CYST is often described as a RADIOLUCENCY that SCALLOPS around the ROOTS of the teeth involved?
a. Stafne bone
b. Traumatic bone
c. Radicular
d. Residual
b. Traumatic bone
What percentage of erythroplakias is diagnosed as SEVERE EPITHELIAL DYSPLASIA or SQUAMOUS CELL CARCINOMA?
a. 10%
b. 25%
c. 60%
d. 90%
d. 90% (Pg.67)
Side Note:
Which of the following best describes the NUMBER of types of HPV? More than:
a. 35
b. 75
c. 100
d. 130
d. 130 (Pg. 67)
Which one of the following terms best defines LEUKOPLAKIA?
a. Clinical
b. Histologic
c. Historical
d. Microscopic
a. Clinical
Gingival enlargement is caused by which of the following groups of drugs?
a. Antiviral
b. Calcium channel blockers
c. Antibiotics
d. Hypersensitivity medications
b. Calcium channel blockers
Because it is associated with candidiasis, an ANTIFUNGAL medication is used sometimes to help in the diagnosis or treatment of:
a. Lingual thyroid
b. Erythema migrans
c. Central papillary atrophy
d. Black hairy tongue
c. Central papillary atrophy
The best way to determine whether LINGUAL THYROID contains the patient's FUNCTIONING THYROID tissue is:
a. Thyroid scan
b. Blood test
c. Biopsy
d. Medication
a. Thyroid scan
RETROCUSPID PAPILLAE are found on the:
a. Lingual gingiva between maxillary centrals
b. Buccal mucosa
c. Lingual aspects of mandibular canines
d. Lateral border of the posterior tongue
c. Lingual aspects of the mandibular canines
The BENIGN STRATIFIED SQUAMOUS CELL PAPILLOMA is considered LOW RISK & is associated with which types of HPV?
a. 16 and 18
b. 2 and 3
c. 6 and 11
d. 1 and 9
c. 6 and 11
The most common location for lingual thyroid is:
a. Ventral tongue
b. Dorsal of anterior third of tongue
c. In the neck
d. Between the foramen cecum and epiglottis
d. Between the foramen cecum and epiglottis
Which of the following is characterized by symptoms including DYSPHAGIA, DYSPHONIA, & DYSPNEA?
a. Median rhomboid glossitis
b. Erythema migrans
c. Lingual thyroid
d. Fissured tongue
c. Lingual thyroid
All of the following are characteristics of PERIAPICAL CEMENTOOSSEOUS DYSPLASIA except one. Which one is the exception?
a. Black women
b. Vital teeth
c. Mid thirties
d. Elevated serum alkaline phosphatase
d. Elevated serum alkaline phosphatase
All of the following are diagnosed without biopsy except one. Which one is the exception?
a. Fissured tongue
b. Erythroplakia
c. Central papillary atrophy
d. Erythema migran
b. Erythroplakia
A lesion is measured at 6cm. What is the approximate size of the lesion?
a. 6 inches
b. 3 inches
c. 100 mm
d. 10 mm
b. 3 inches
Side Note: Centimeter (cm) One-hundredth of a meter; EQUIVALENT to a LITTLE LESS THAN ONE-HALF INCH (0.393) (Fig. 1.4). If a lesion is described as being 3 cm in size, it is really about ONE & ONE-HALF INCHES.
Centimeter (cm)
One-hundredth of a meter; EQUIVALENT to a LITTLE LESS THAN ONE-HALF INCH (0.393) (Fig. 1.4). If a lesion is described as being 3 cm in size, it is really about ONE & ONE HALF INCHES.
Side Note: A meter has 100 CENTIMETERS. 10 MILLIMETERS make ONE CENTIMETER. The CENTIMETER can be WRITTEN as "cm".
Millimeter (mm)
ONE-THOUSANDTH OF A METER (a METER is EQUIVALENT to 39.3 INCHES); the PERIODONTAL PROBE is of great assistance in documenting the size or diameter of a LESION that can be measured in MILLIMETERS (general terms such as SMALL, MEDIUM, or LARGED sometimes used, but these terms are NOT as specific) (Fig. 1.5)
Corrugated
Wrinkled (ridged)
Fissure
A CLEFT or GROOVE, normal or otherwise, showing PROMINENT DEPTH.
Papillary
Resembling SMALL, NIPPLE-SHAPED projections or elevations found in CLUSTERS.
Smooth, rough, folded
terms used to describe the SURFACE TEXTURE of a LESION.
Radiographic Terms used to describe Lesions in Bone
- Coalescence
- Diffuse
- Multiocular
- Radiolucent
- Radiopaque
- Radiolucent and Radiopaque
- Root resorption
- Scalloping around the root
- Uniocular
- Well circumscribed
Coalescence
The process by which PARTS of a WHOLE JOIN TOGETHER, or FUSE, to make ONE.
Diffuse
Describes a lesion with BORDERS that are NOT WELL DEFINED, making it IMPOSSIBLE to DETECT the EXACT PARAMETERS of the LESIO; this may make treatment MORE DIFFICULT and, depending on the BIOPSY RESULTS, more RADICAL (Fig. 1.6)
Multilocular
Describes a LESION that EXTENDS BEYOND the CONFINES of ONE DISTINCT area & is DEFINED as many LOBES or PARTS that are SOMEWHAT FUSED TOGETHER, making up the ENTIRE LESION; a MULTILOCULAR RADIOLUCENCY is SOMETIMES described as RESEMBLING SOAP BUBBLES; an ODONTOGENIC KERATOCYST often presents as a MULTILOCULAR, RADIOLUCENT LESION.
Radiolucent
describes the BLACK or DARK areas on a radiograph; RADIANT ENERGY can pass through these structures; LESS DENSE TISSUE such as the PULP is seen as a RADIOLUCENT STRUCTURE. (Fig. 1.8)
Radiolucent and Radiopaque
Terms used to describe a MIXTURE of LIGHT & DARK areas within a LESION, usually DENOTING a STAGE in PERIAPICAL CEMENTO-OSSEOUS DYSPLASIA (CEMENTOMA) (Fig. 1.9A), the LESION is RADIOLUCENT; in STAGE II it is RADIOLUCENT & RADIOPAQUE (Fig. 1.9B).

Radiopaque
Describes the LIGHT or WHITE area on a radiograph that results from the inability or RADIANT ENERGY to pass through the structure; the DENSER the structure, the LIGHTER or WHITER it appears on the radiograph; this is illustrated in Fig. 1.10.
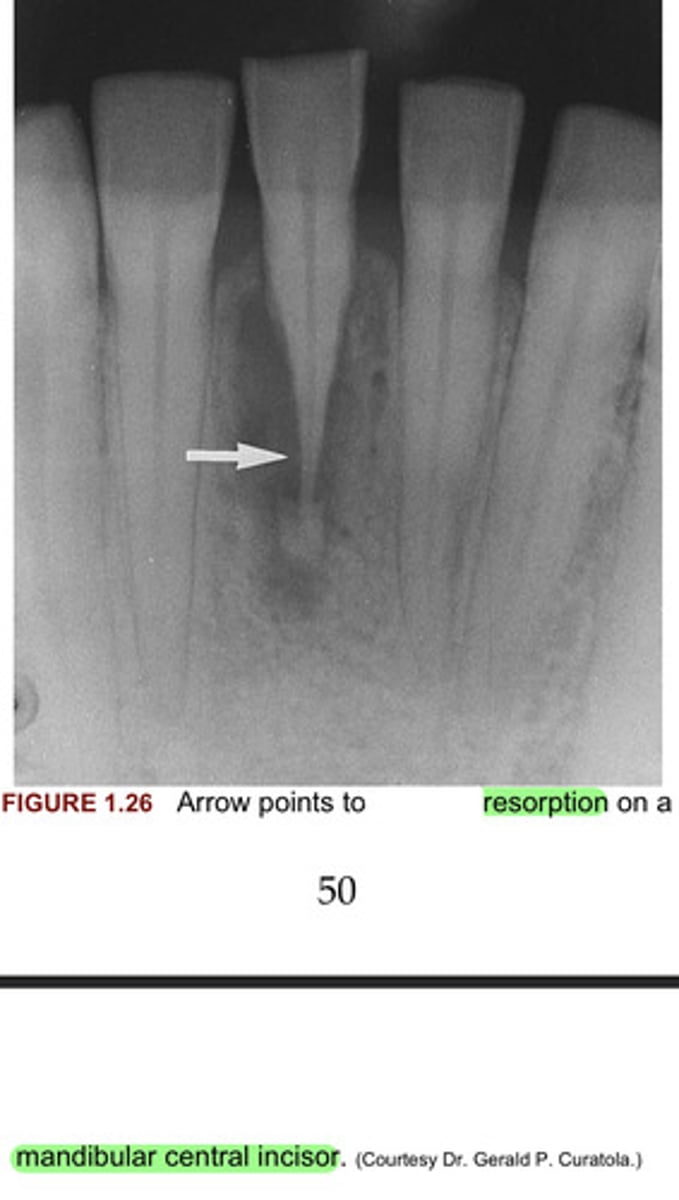
Root Resoprtion
Observed radiographically when the APEX of the tooth appears SHORTENED or BLUNTED & IRREGULARLY SHAPED; occurs as a response to STIMULI, which can include a CYST, TUMOR, or TRAUMA; Fig. 1.11 illustrates RESORPTION of the ROOTS as a result of a RAPID ORTHODONTIC PROCEDURE (see Fig. 1.26); EXTERNAL RESORPTION ARISES from tissue OUTSIDE the tooth such as the PERIODONTAL LIGAMENT, whereas INTERNAL RESORPTION is TRIGGERED by PULPAL TISSUE REACTION from within the tooth; in the LATTER the PUPAL area can be seen as a DIFFUSE RADIOLUCENCY BEYOND the confines of the NORMAL PULP area.
Scalloping around the root
A RADIOLUCENT LESION that extends between the ROOTS, as seen in TRAUMATIC BONE CYST; this lesion appears to extend up the PERIODONTAL LIGAMENT (Fig. 1.12).
Unilocular
Having one COMPARTMENT or UNIT that is WELL DEFINED or OUTLINED, as in a simple RADICULAR CYST (Fig. 1.13).
Well Circumscribed
term used to describe a LESION with BORDERS that are SPECIFICALLY defined and in which ONE CAN CLEARLY see the EXACT MARGINS & extent (Fig. 1.14)
Anomaly
Something that DEVIATES from what is STANDARD or NORMAL.
Dysphagia
Difficulty SWALLOWING
Dysphonia
Difficulty SPEAKING
Dyspnea
Difficulty BREATHING
The 8 categories that contribute segments of information leading to the DEFINITIVE or FINAL DIAGNOSIS are:
1. Clinical
2. Radiographic
3. Historical
4. Laboratory
5. Microscopic
6. Surgical
7. Therapeutic
8. Differential findings
Side Note: It is important to note that usually one area ALONE does NOT provide sufficient information to make a DIAGNOSIS; the STRENGTH of the DIAGNOSIS is OFTEN derived from ONE, TWO, or even THREE areas. As the dental hygienist becomes more aware of the DISEASES and CONDITIONS discussed in this text, it will be MOST HELPFUL to use the DIAGNOSTIC CATEGORIES as a GUIDE to EVALUATING LESIONS.
Clinical diagnosis suggests that the strength of the diagnosis comes from the clinical ______________________ of the _____________.
appearance, lesion
By ___________________________ the area in a well-illuminated clinical setting and palpating it if necessary, the clinician can establish a diagnosis for some lesions on the basis of color, shape, location, and history of the lesion.
observation
Side Note: When a diagnosis can be made on the basis of these unique clinical features, biopsy or surgical intervention is NOT NECESSARY.
What are some examples of lesions in which lesions can be clinically diagnosed?
- Fordyce granules
- Torus palatinus
- Mandibular tori
- Melanin pigmentation
- Retrocuspid papillae
- Lingual varicosities
Other benign conditions of unknown cause that are recognized by their distinct clinical appearance include:
- Fissured tongue
- Median rhomboid glossitis (central papillary atrophy)
- Erythema migrans (aka geographic tongue)
- Hairy tongue
Erythema migrans have areas of _________________________________.
depapillation
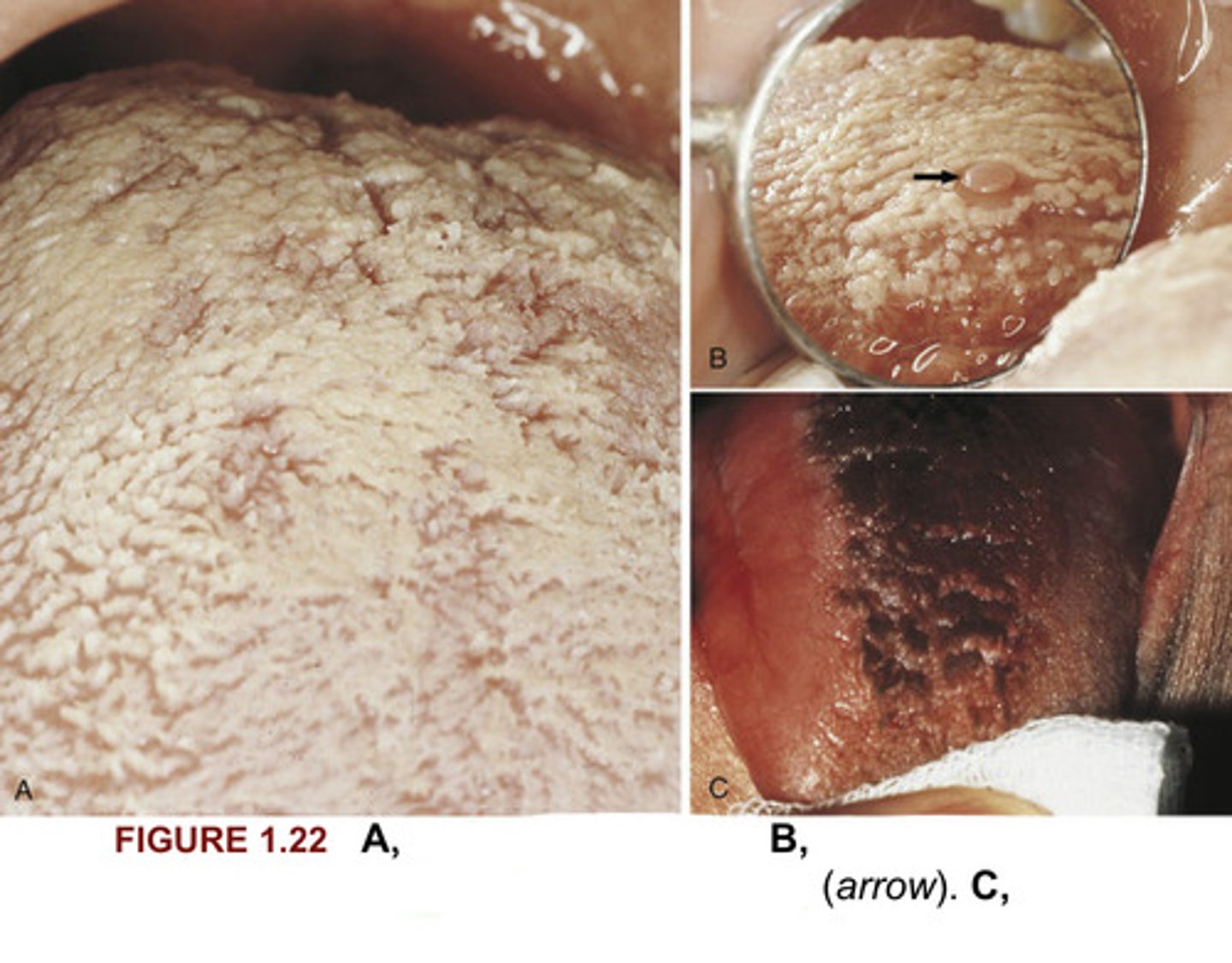
A. White hairy tongue
B. White hairy tongue showing a CIRCUMVALLATE PAPILLA (ARROW)
C. Black hairy tongue
Please identify what you see in Figure 1.22.
In radiographic diagnosis the radiograph provides ______________________ information to establish the diagnosis.
sufficient
Side Note: Although additional clinical & historical information may contribute, the diagnosis is obtained from the radiograph.
Conditions for which the radiograph provides the MOST SIGNIFICANT INFORMATION include:
- Periapical pathosis
- Internal resorption
- External resorption
- Heavy interproximal calculus
- Dental caries
- Compound odontoma
- Complex odontoma
- Supernumerary teeth
- Impacted pr unerupted teeth
- Calcified pulp
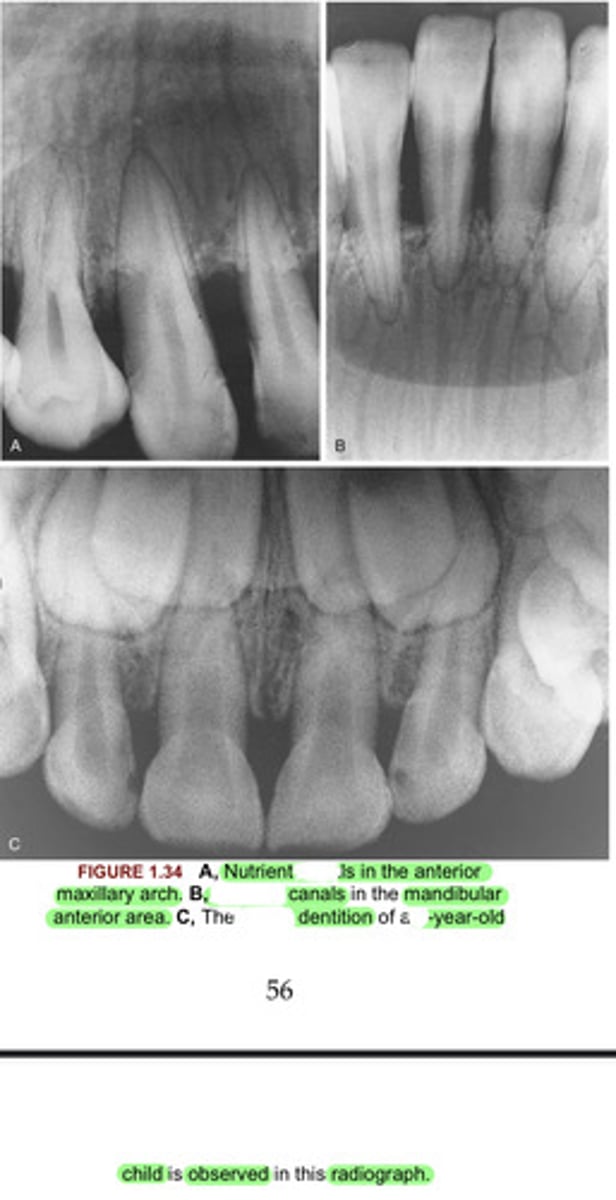
Normal anatomic landmarks are also _______________ observed radiographically. In some cases the radiographic image may show very DISTINCT and WELL-DEFINED STRUCTURES such as the NUTRIENT CANALS seen in Figure 1.34A-B and the MIXED DENTITION seen in Figure 1.34C.
easily
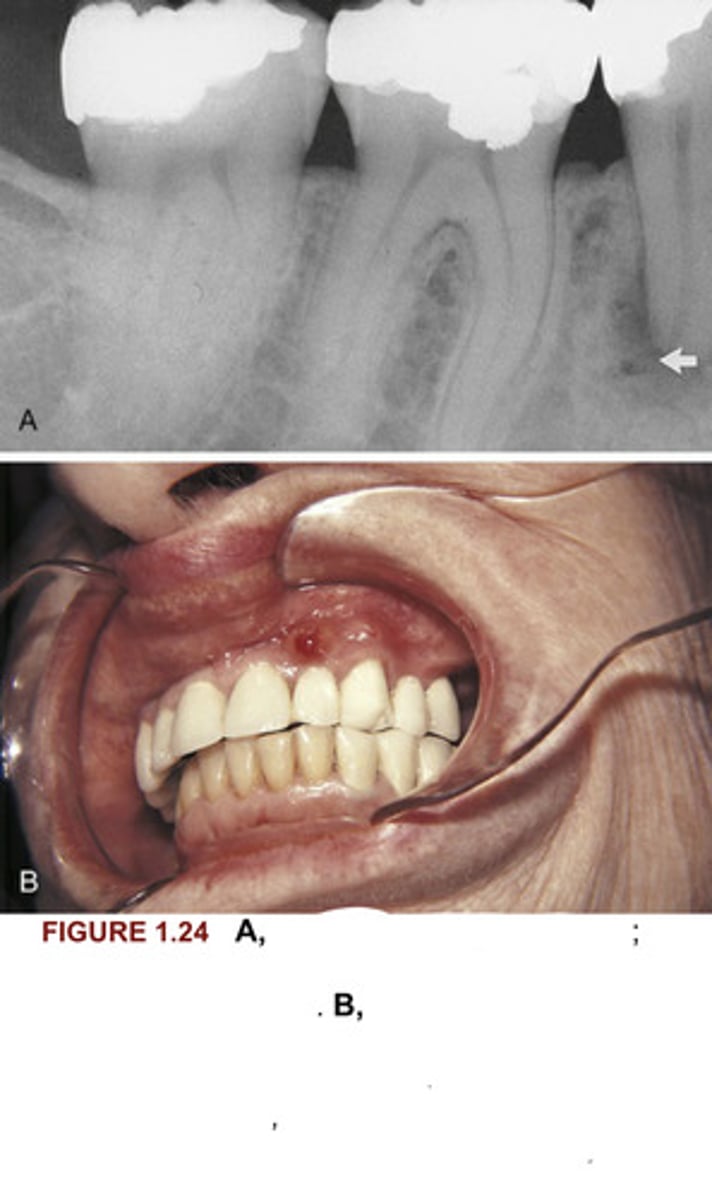
A. Periapical pathosis (PAP); a radiolucency is seen at the APEX of the mandibular second premolar (arrow).
B. In another patient a FISTULA is seen on the maxillary lateral incisor. A FISTULA is usually an indication of PAP. When a FISTULA is OBSERVED CLINICALLY, a radiograph is NECESSARY for DIAGNOSTIC & TREATMENT purposes.
Identify the diagnosis of images A & B in figure 1.24
resorption
The arrow in Figure 1.25 points to the area of internal what on the maxillary first molar?
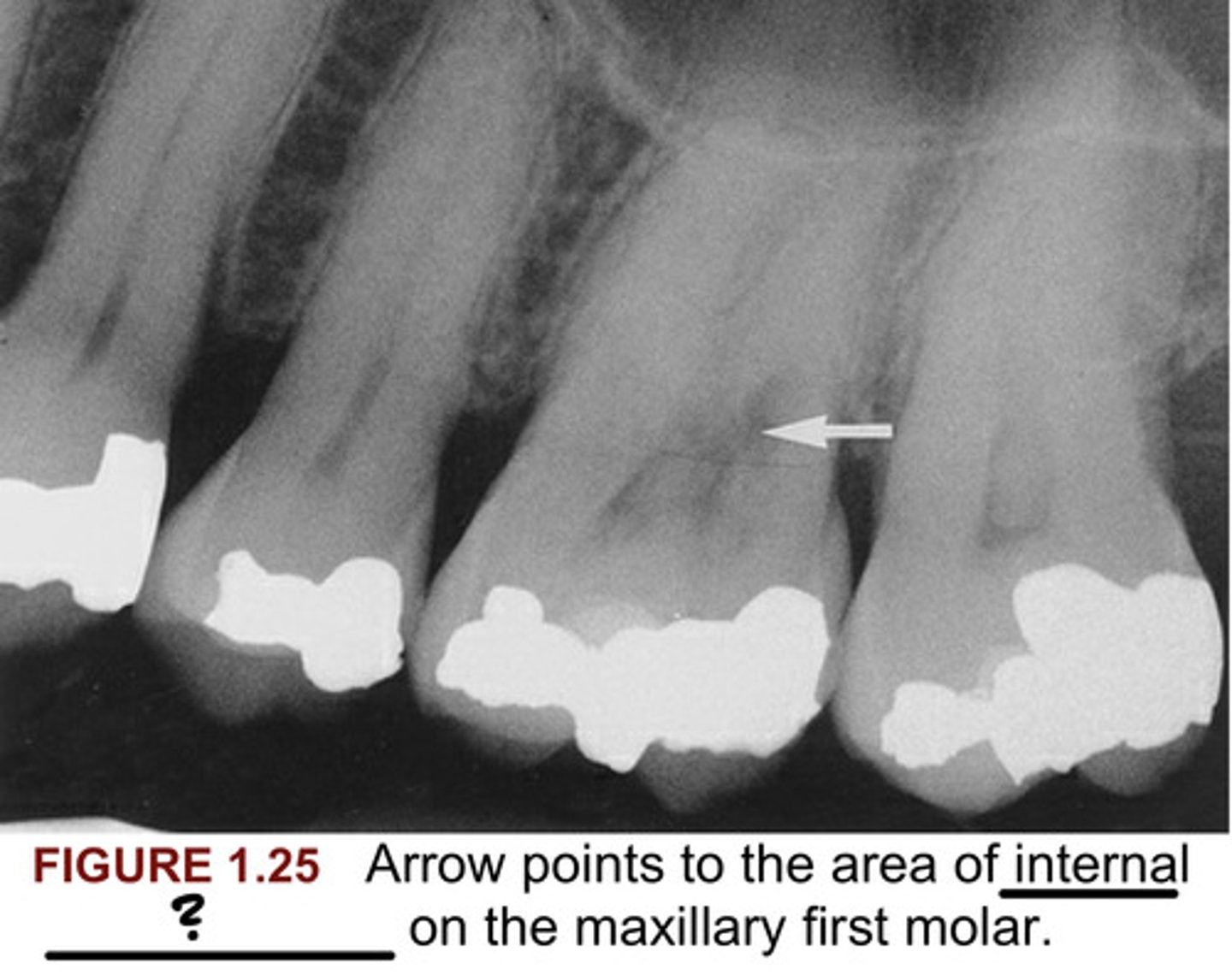
external
In figure 1.26 the arrow points to what resorption on a mandibular central incisor?
heavy interproximal calculus
In figure 1.27, arrows point to what?
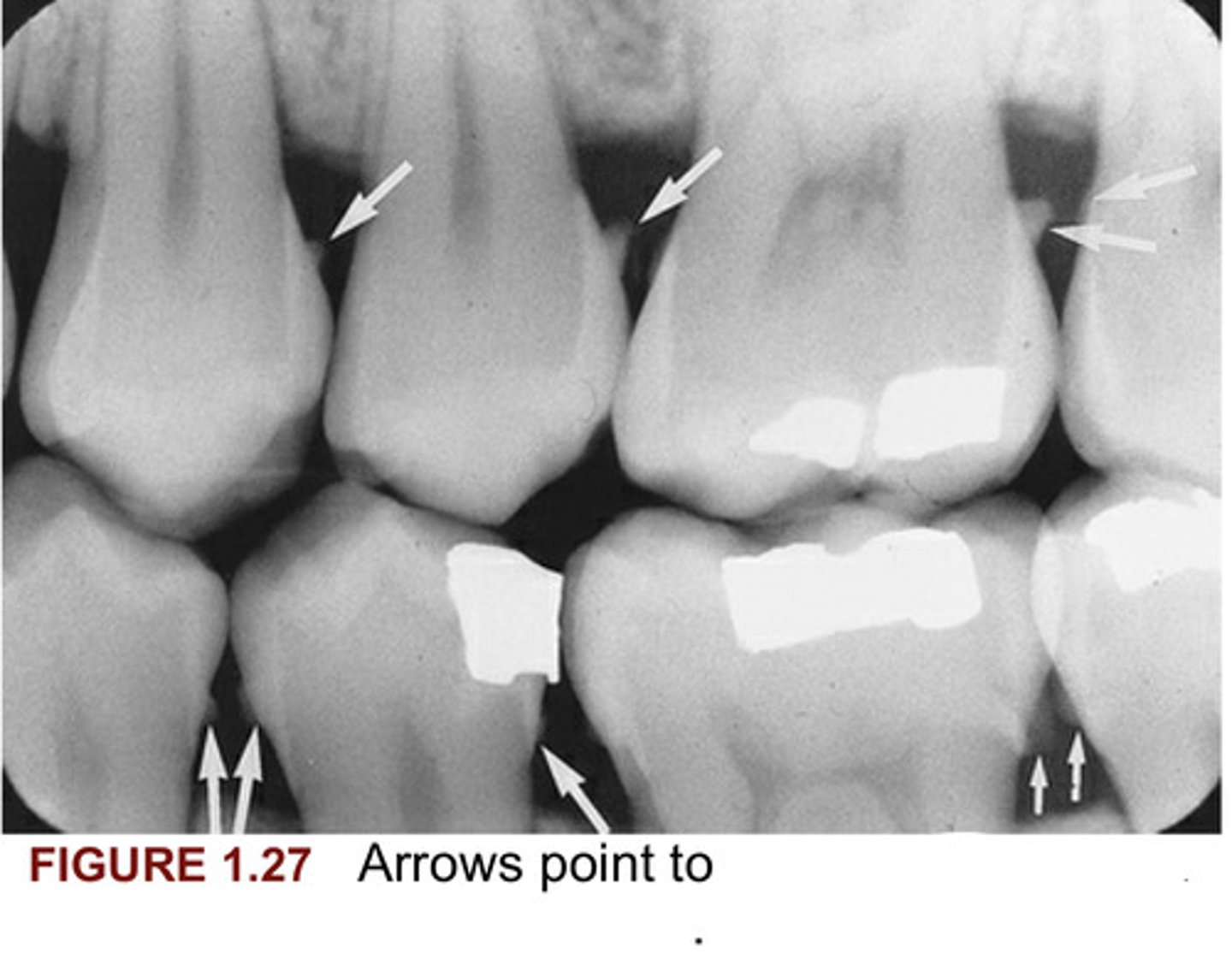
caries, necessary, clinical, radiographic
In Figure 1.28, please fill in the blanks for A, and C.
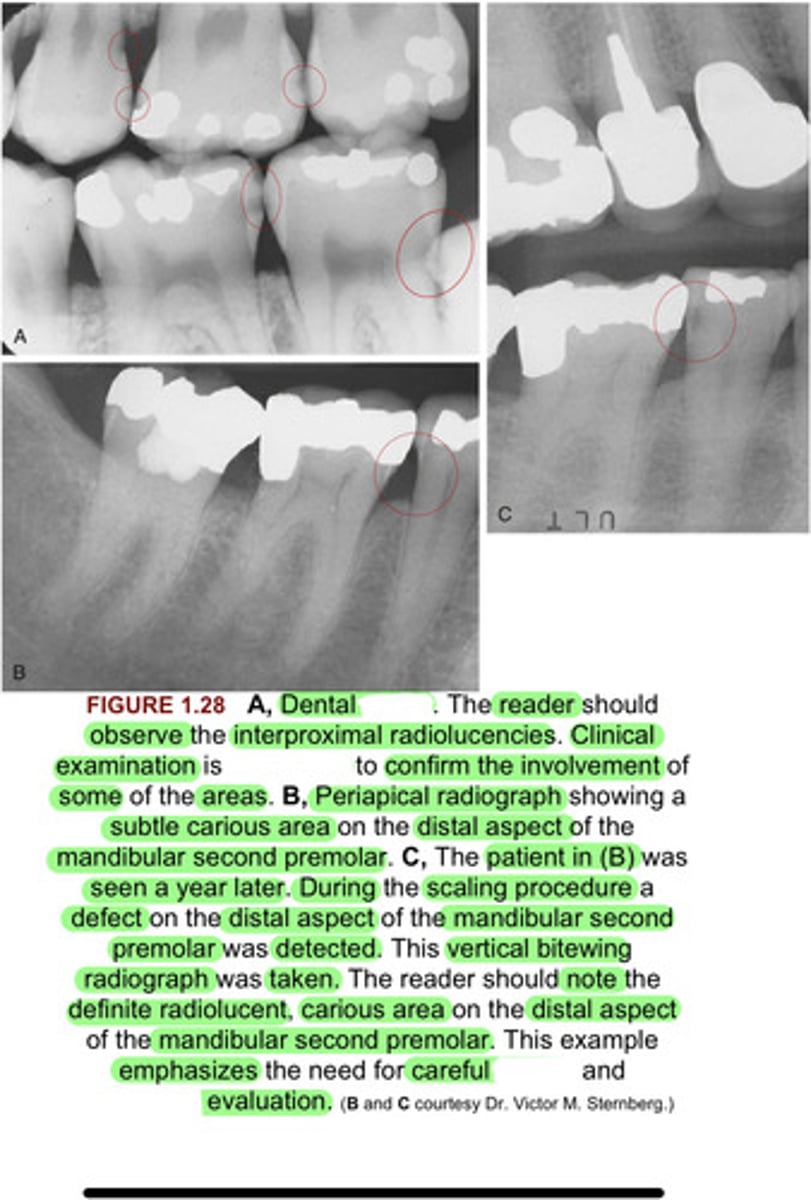
Compound odontoma
Figure 1.29, Arrow points to what?
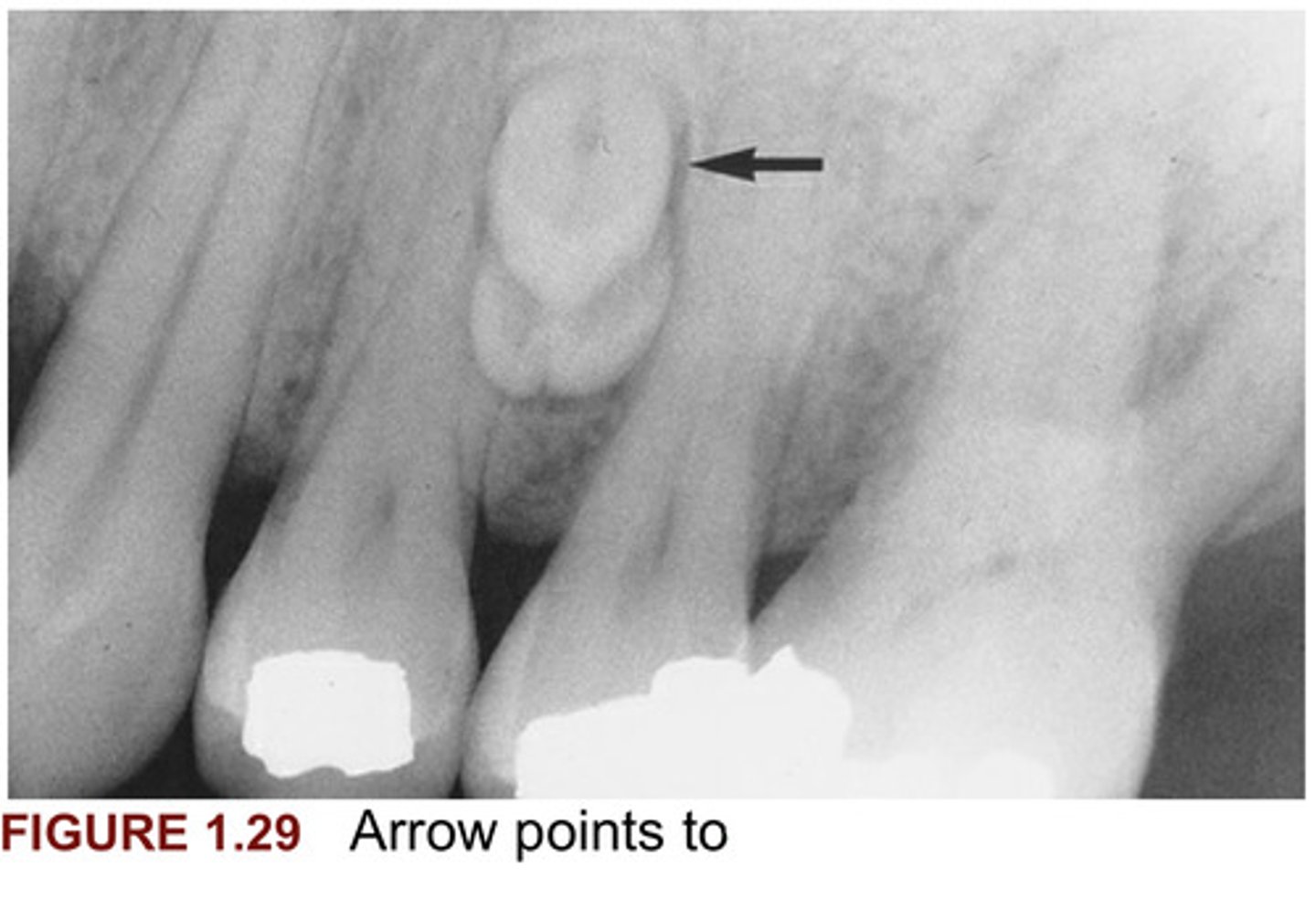
A. Compound odontoma
B. Complex odontoma, histopathologic
For Figure 1.30, please fill in the blanks for A & B.
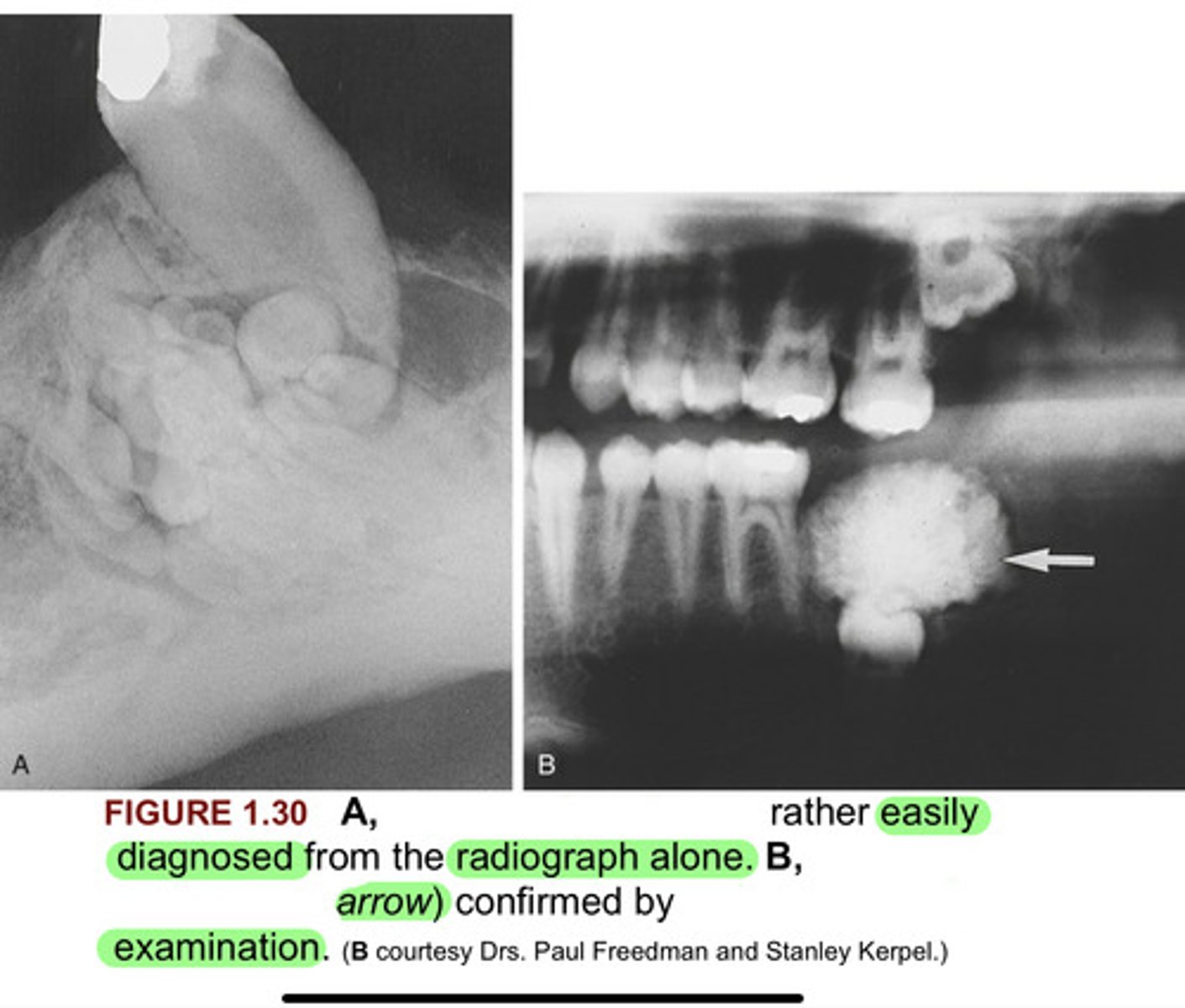
A. Mesiodens
B. Supernumerary, dentigerous cyst, clinically
For figure 1.31 A & B, please fill in the blanks.
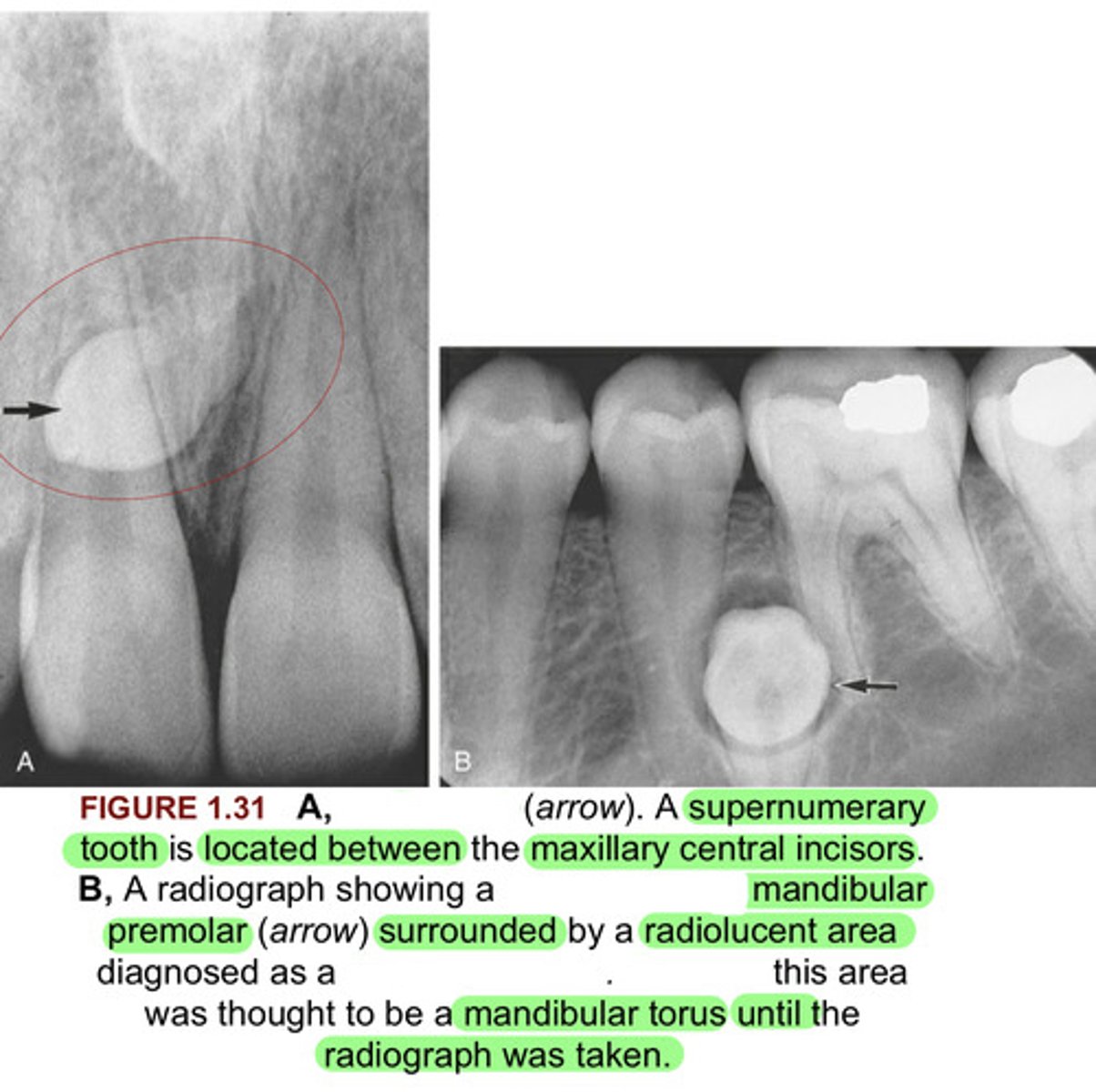
A. Cuspid
B. Cuspid
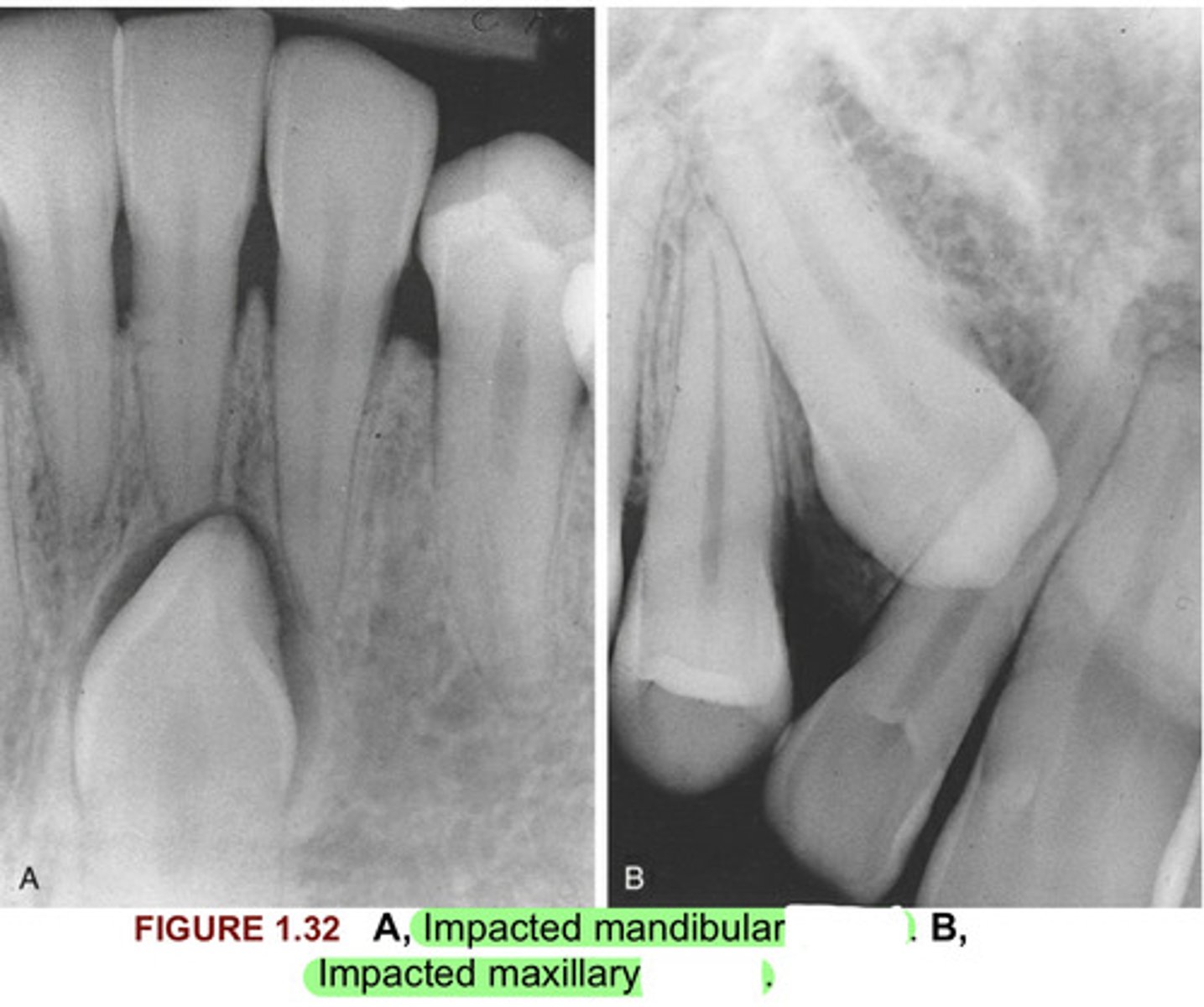
In Figure 1.32, please fill in the blanks for both A & B.
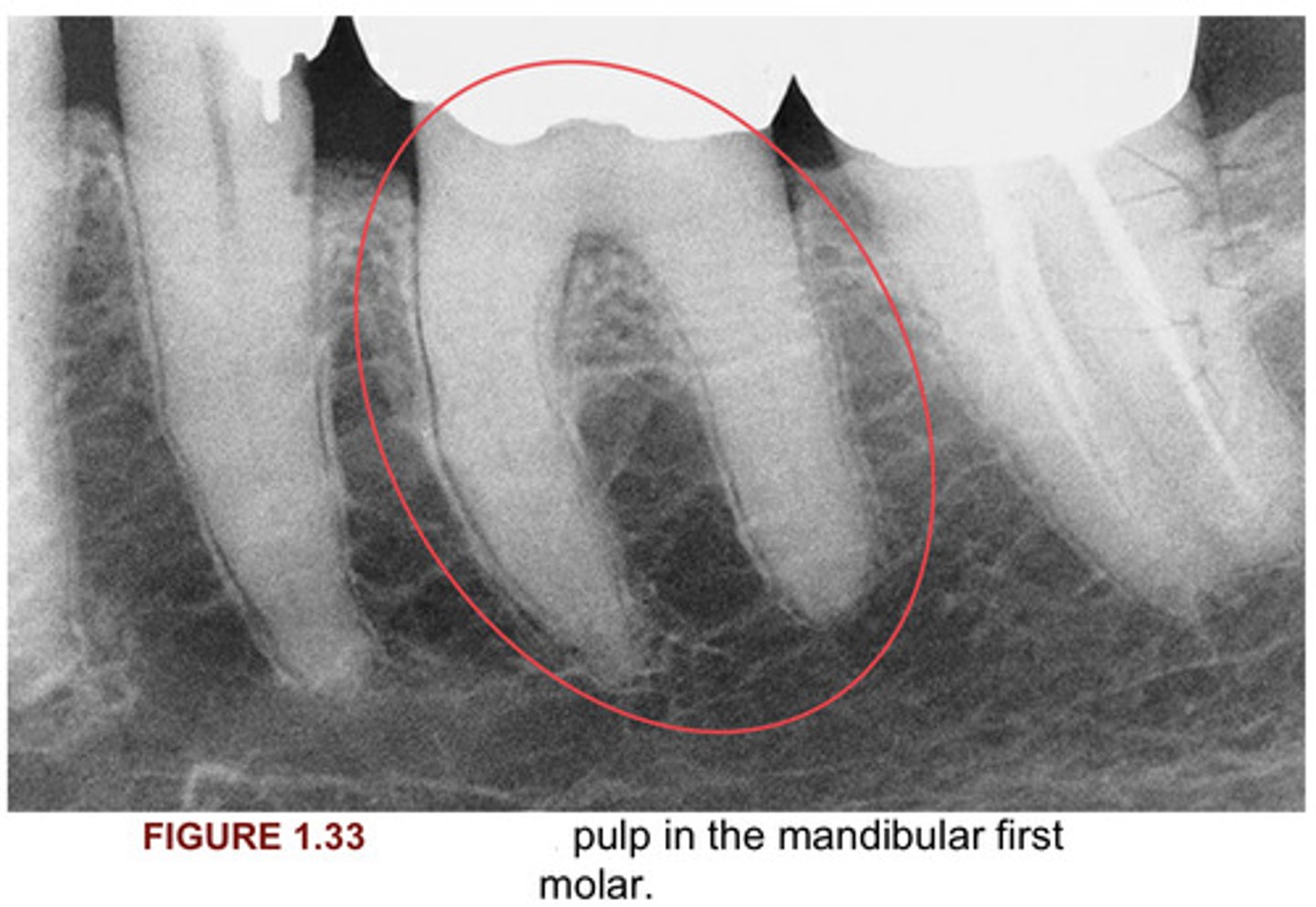
Calcified
In figure 1.33, please fill in the blank.
A. canals
B. Nutrient
C. mixed, 5
In figure 1.34 please fill in the blanks for A, B, & C.
T/F?
Historical data constitute an important component in every diagnosis; occasionally when historical data are COMBINED with OBSERVATION of the clinical appearance of the lesion, the historical information constitutes the MOST important CONTRIBUTION to the DIAGNOSTIC PROCESS.
True
PERSONAL HISTORY, FAMILY HISTORY, PAST & PRESENT MEDICAL & DENTAL HISTORIES, HISTORY OF DRUG INGESTION, & HISTORY OF THE PRESENTING DISEASE OR LESION can provide information necessary for the ___________ diagnosis.
final
Thorough ______________________ & ____________ histories MUST be a part of every patient's permanent record.
medical, dental
Side Note: The clinician should review these documents carefully & update them with the patient at each visit.
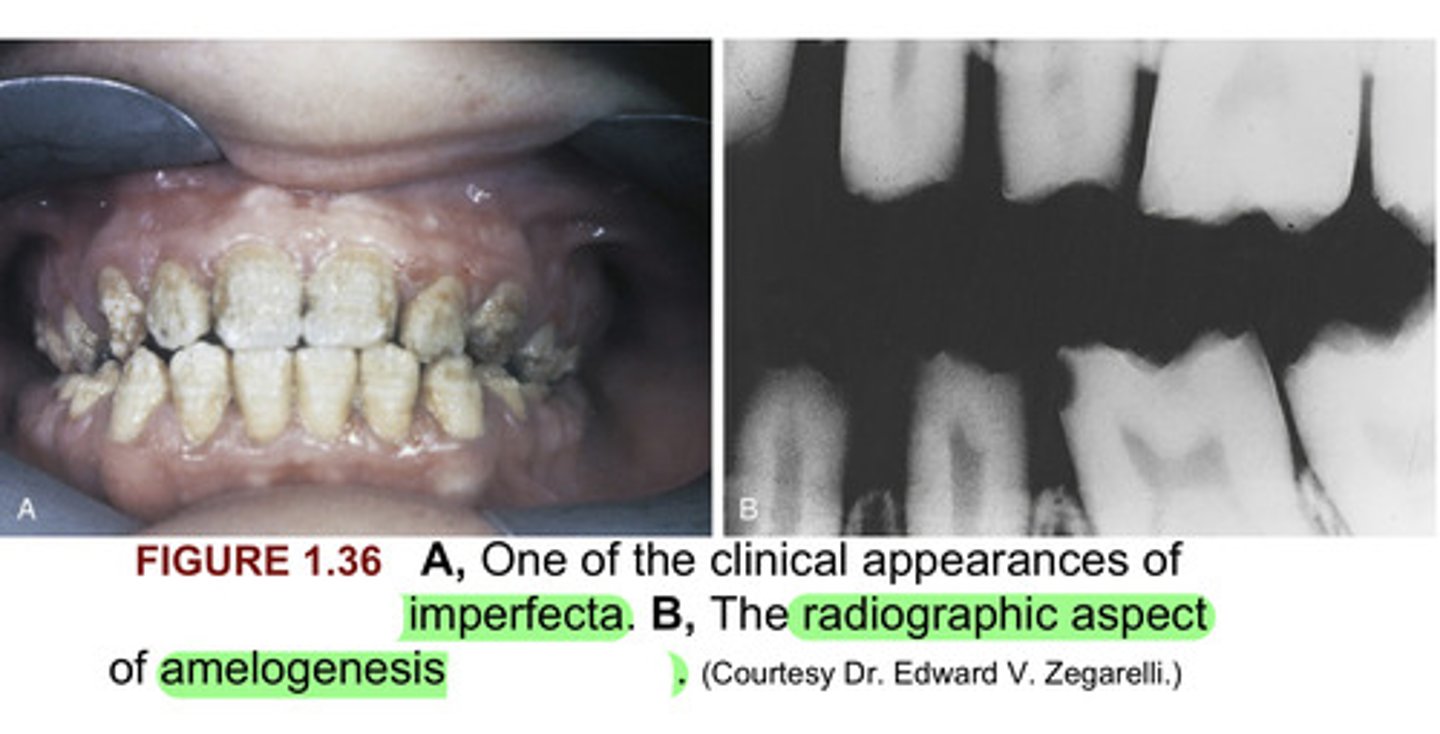
__________________________ conditions in which the FAMILY HISTORY contributes a SIGNIFICANT ROLE in the diagnosis include:
Pathologic
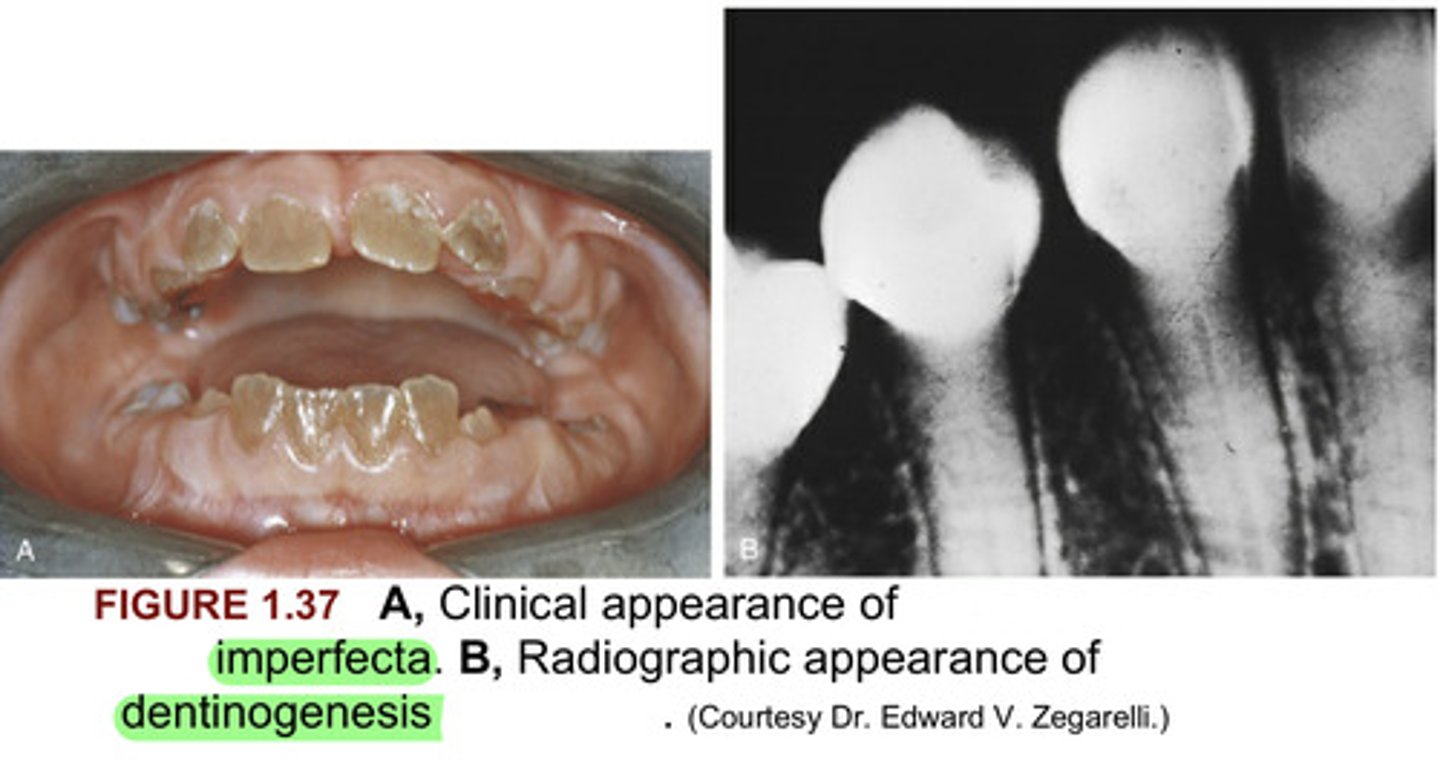
- Amelogenesis imperfecta
- Dentinogenesis imperfecta
& many other genetic disorders.
Side Note: In addition, clinical findings & radiographs provide significant assistance to the diagnostic process of these conditions.
A. Amelogenesis
B. imperfecta
In figure 1.36, please fill in the blanks for both A & B.
A. Dentinogenesis
B. imperfecta
In figure 1.37 please fill in the blanks for both A & B.