Di Imaging I - Exam 3 (Spinal RA, Seropositive, Systemic Diseases)
1/109
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
110 Terms
RA in the Cervical spine will impact about 50% of RA patients within ______ of diagnosis
10 years
RA of the Cervical spine findings
atlantoaxial subluxations (AADI >3 mm, PADI <14 mm)
atlantoaxial impaction
odontoid erosions (whittled dens)
subaxial subluxations (canal <14 mm)
apophyseal joint disease
spinous process erosions
osteopenia
Which of the findings of cervical RA is the MC to cause neurological symptoms
atlantoaxial impaction
Odontoid erosions can occur in what three different synovial joints
btw dens and anterior arch (AADI)
btw dens and transverse ligament
tip of dens

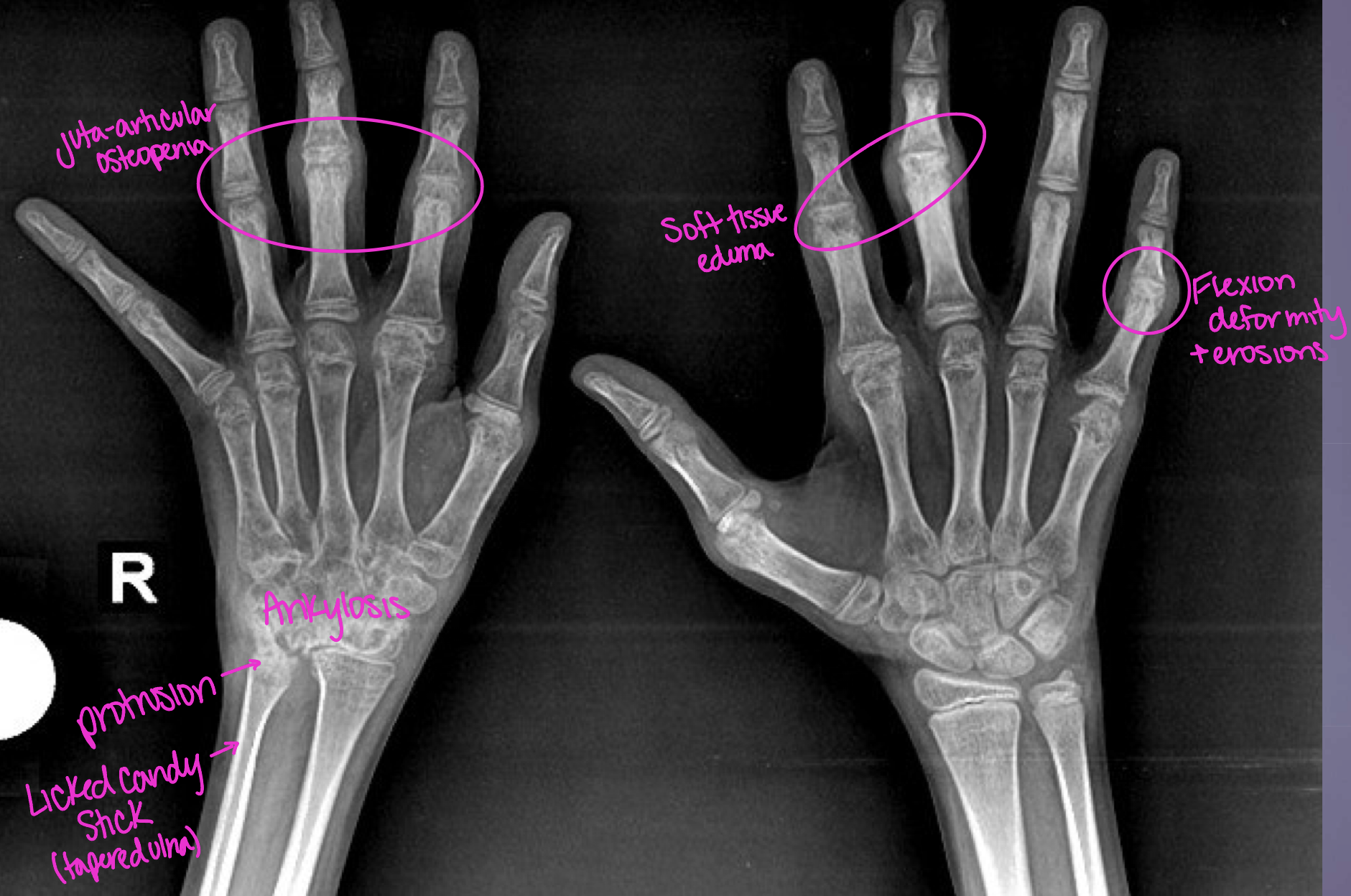
What two diseases does this pt have
OA + RA
What two image studies should be perfomed to evaluate the AADI movement
flexion and extension
The AADI should not exceed ____ in an adult
3mm
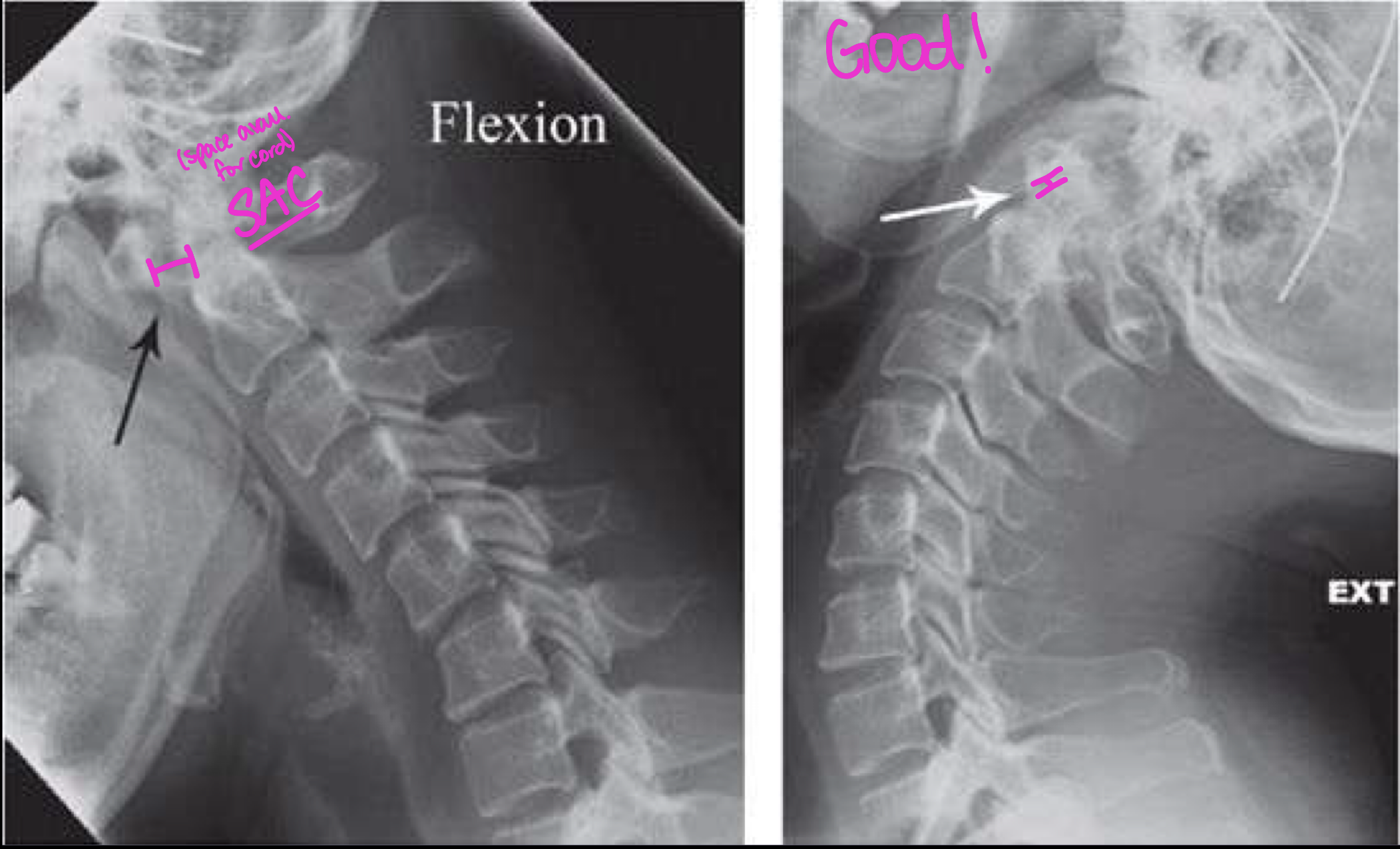
A wider AADI (due to erosions caused by pannus) is bad b/c
space available for cord (SAC) is decreased → posterior cord compression
If erosions of bone is seen, it has already gotten through
ligaments and soft tissues

What finding of cervical RA is in this image
Occ-C1 and C1-2 facet erosions

What finding of cervical RA is in this image
basilar invagination
What are four other reasons why a pt could have a wider AADI
congenital anomaly
narrowing PADI
fracture of C1 (at least 2 in ring)
inflammation or degenerative
Juvenile Chronic Arthritis (juvenile idiopathic arthritis) onset
before 16 yo
Which type of JCA is most common
seronegative - polyarticular in females
JCA (Juvenile Chronic Arthritis) is a _____ disease (lymph, spleen, liver, heart)
systemic
Polyarticular form of JCA
bilateral and symmetrical involvement
mild fever
lymphadenopathy
rash
JCA (Juvenile Chronic Arthritis) radiolgy findings
soft tissue swelling (bare areas)
osteopenia (pannus dec bone density)
JSN
articular erosions
malalignments/subluxations (growth disruptions, periostitis (mouse ears), ankylosis)
JCA locations
hands - periostitis and shortening
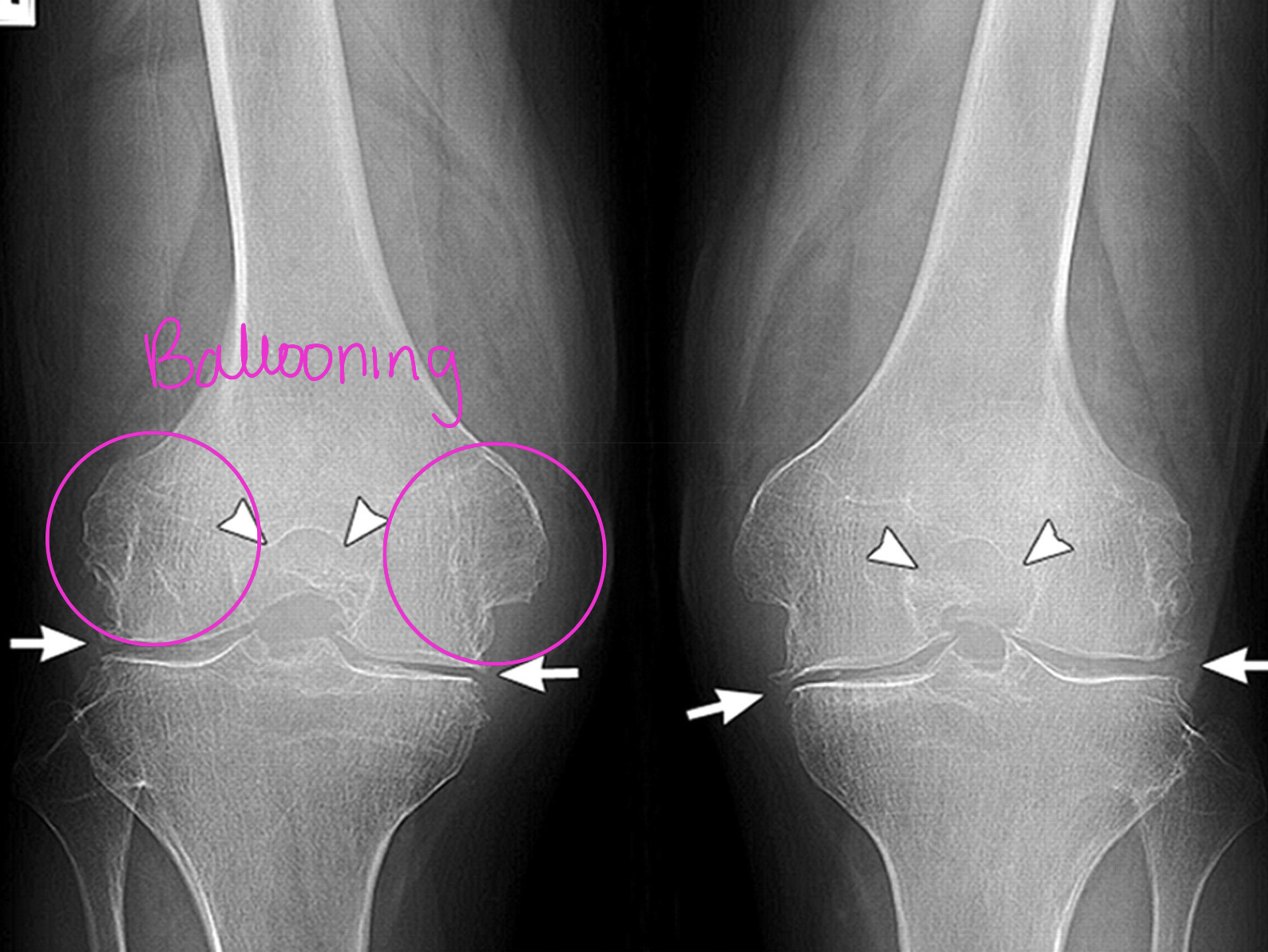
knee - ballooning of metaphysis
hip - acetabular protrusion
cervical spine - erosions, posterior joint ankylosis
Balooning represents large epiphysis with a constricted appearance of the
metaphysis and diaphysis

What finding of JCA is found in this image
periostitis
children have loosley attached periosteum
This young female presented with stiffness and pain in both wrists, limitation of movement in both wrists (esp. right side), what diagnosis would you give her
JCA
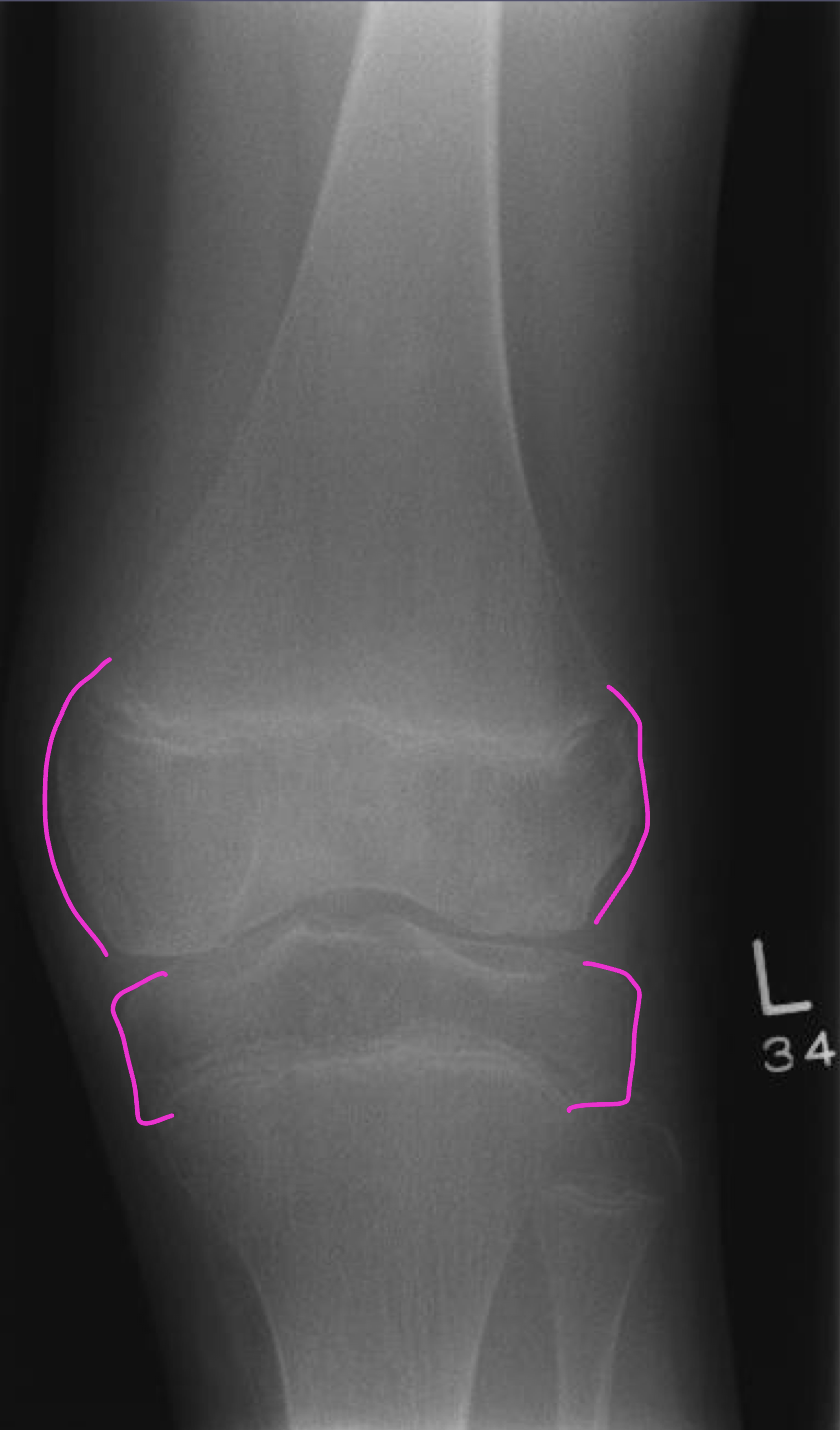
What JCA two radiological findings are in this image
osteopenia
ballooning - enlargement of distal femoral epiphysis

This adult patient who had JCA presents what findings
hypoplastic bodies (didn’t fully develop)
ankylosed facets
This pt has what two diseases
OA + JCA (more clinically significant)
Systematic lupus erythematosus (SLE)
generalized connective tissue disorder involving multiple organs
seropositive
20-40 yo females
ANA positive
90% of SLE pt have articular symptoms regardless of
radiographic evidence (symp well before radiographic findings)
The MC and serious consequences of SLE involve the
kidneys - nephropathy and renal failure
raynaud phenomenon
SLE findings
hands, wrists, shoulders, knees, feet
bilateral and symmetrical
widened AADI
joint swelling and pain
soft tissue calcifications
non-erosive
subluxed joint can be temporarily manually reduced
SLE is commonly treated with
corticosteroids (on/off to reduced risk of avascular necrosis/osteonecrosis)
Fibrinoid necrosis in tissues due to SLE cause
synovitis, vasculitis, pleuritis, pericarditis, nephritis

SLE in hands
MCP and PIP joints
ligament laxity → ulnar and fibular deviation
swan neck deformity (unopposed flexion)
boutonneire deformity (unopposed extension)
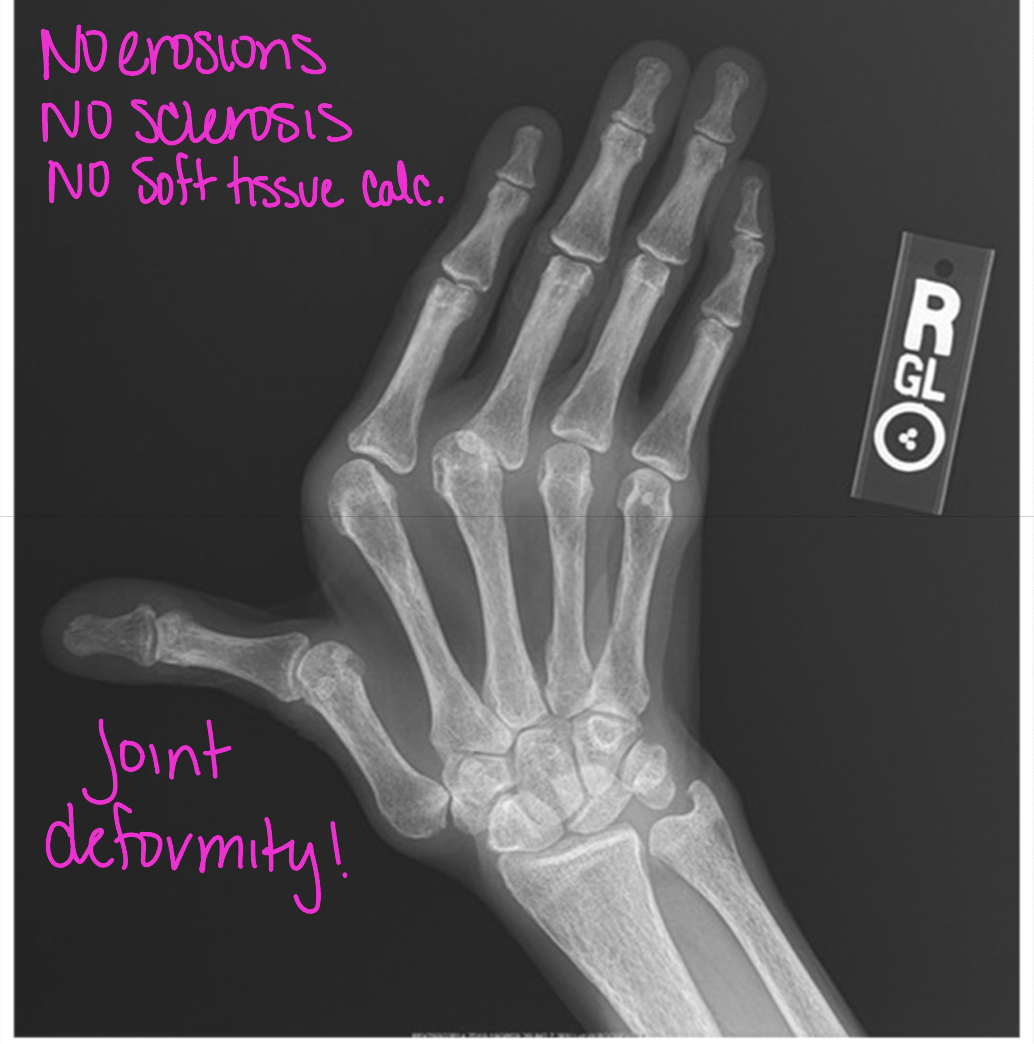
What disease does this pt have
SLE
What findings of SLE does this x-ray show
ulnar deviation (NO erosions)
osteopenia
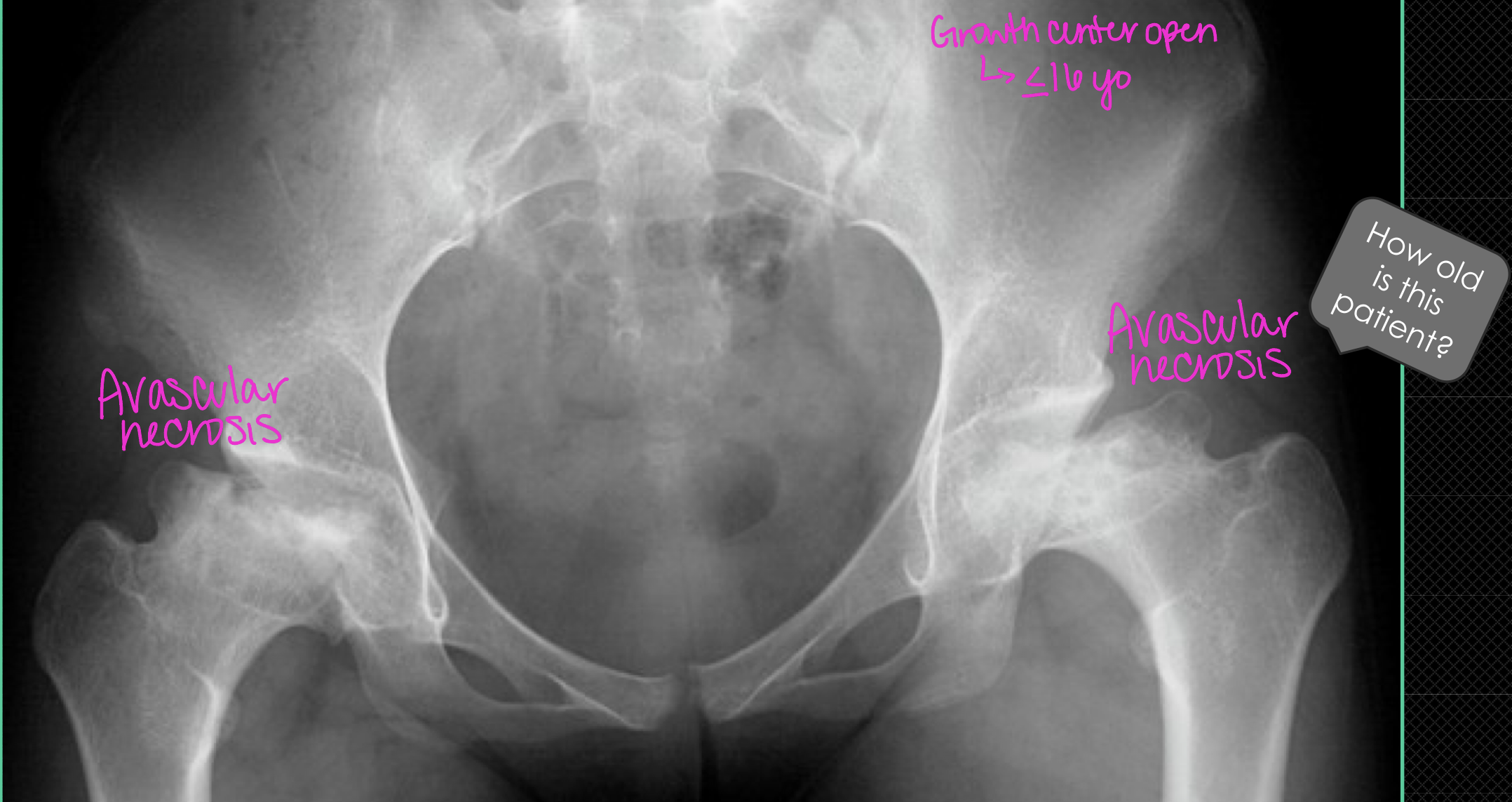
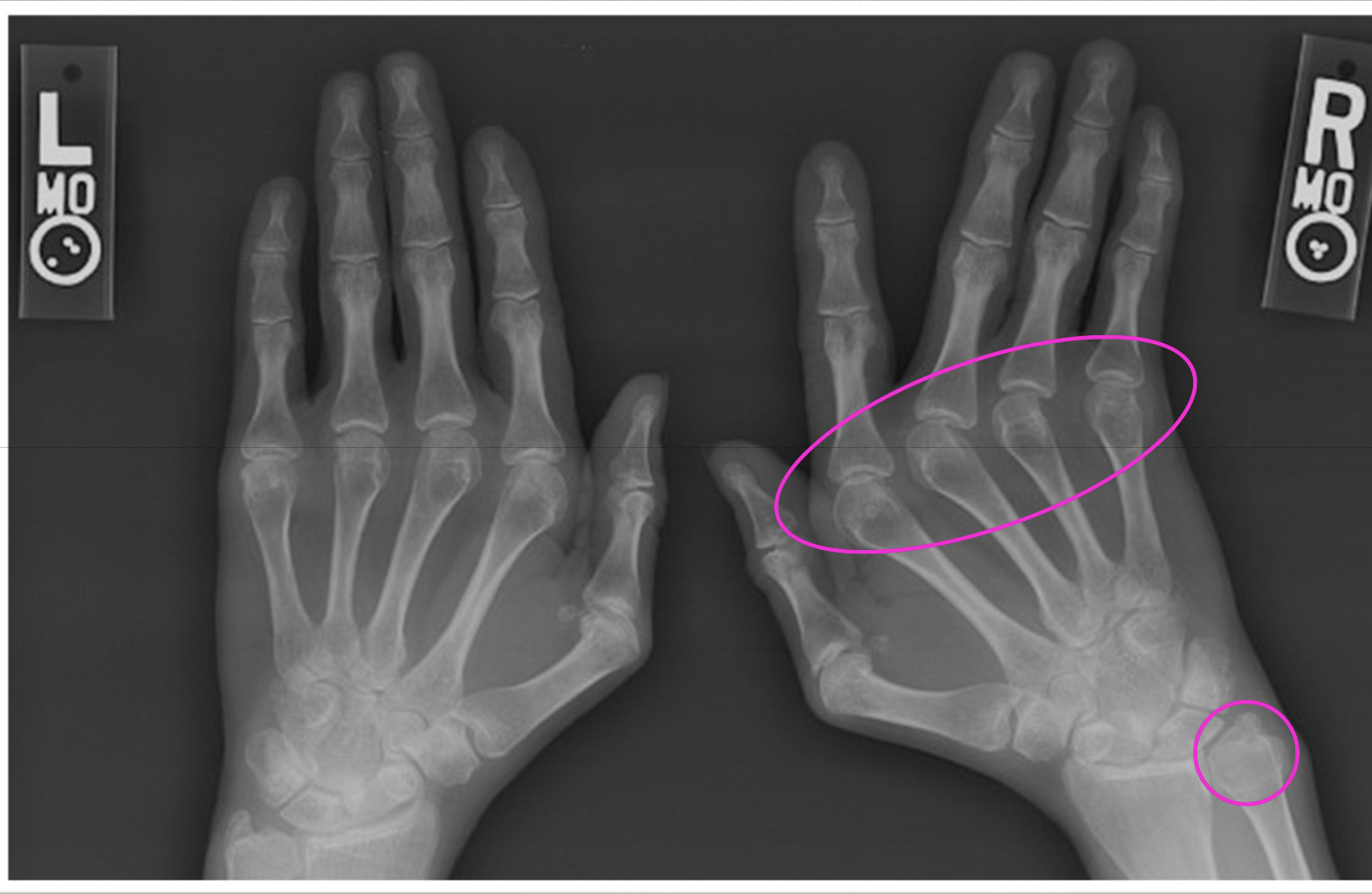
SLE + increased risk of clots + Tx of corticosteroids =
increased risk of avascular necrosis
Jaccoud Arthropathy
follows rheumatic fever (hx of strep)
associated with multiple connective tissue disorders
Jaccoud arthropathy is a radiographic mimic of
SLE (non-erosive, ulnar deviation, fibular deviation, swan neck, boutonniere)
How to differentiate SLE from Jaccoud
SLE first thought from findings…but Jaccound will have a hx of cardiac issues
Scleroderma (progressive systemic sclerosis - PSS)
generalized systemic inflammatory connective tissue disorder of skin, lungs, GI, kidneys, MSK system
seropositive
What is the MC finding of scleroderma (PSS)
small vessel calcifications

Scleroderma (PSS) skin findings progression
1) edema
2) induration/hardening (Hidebound)
3) atrophy
sometimes raynaud pheomenon too
MC organ involvement of scleroderma besides the skin
esophagus dilate and reduced mobility (dysphagia and heartburn)
bowels slow down (constipation and impaction)
CREST syndrome fo scleroderma
Calcinosis (of soft tissues)
Raynaud phenomenon
Esophageal dysmobility
Sclerodactyly (contracture)
Telangiectasia (dilated subdermal blood vessels)
Scleroderma (PSS) in hands
osseous resorption of distal tufts/ungual tufts (acral osteolysis)
flexion contractures
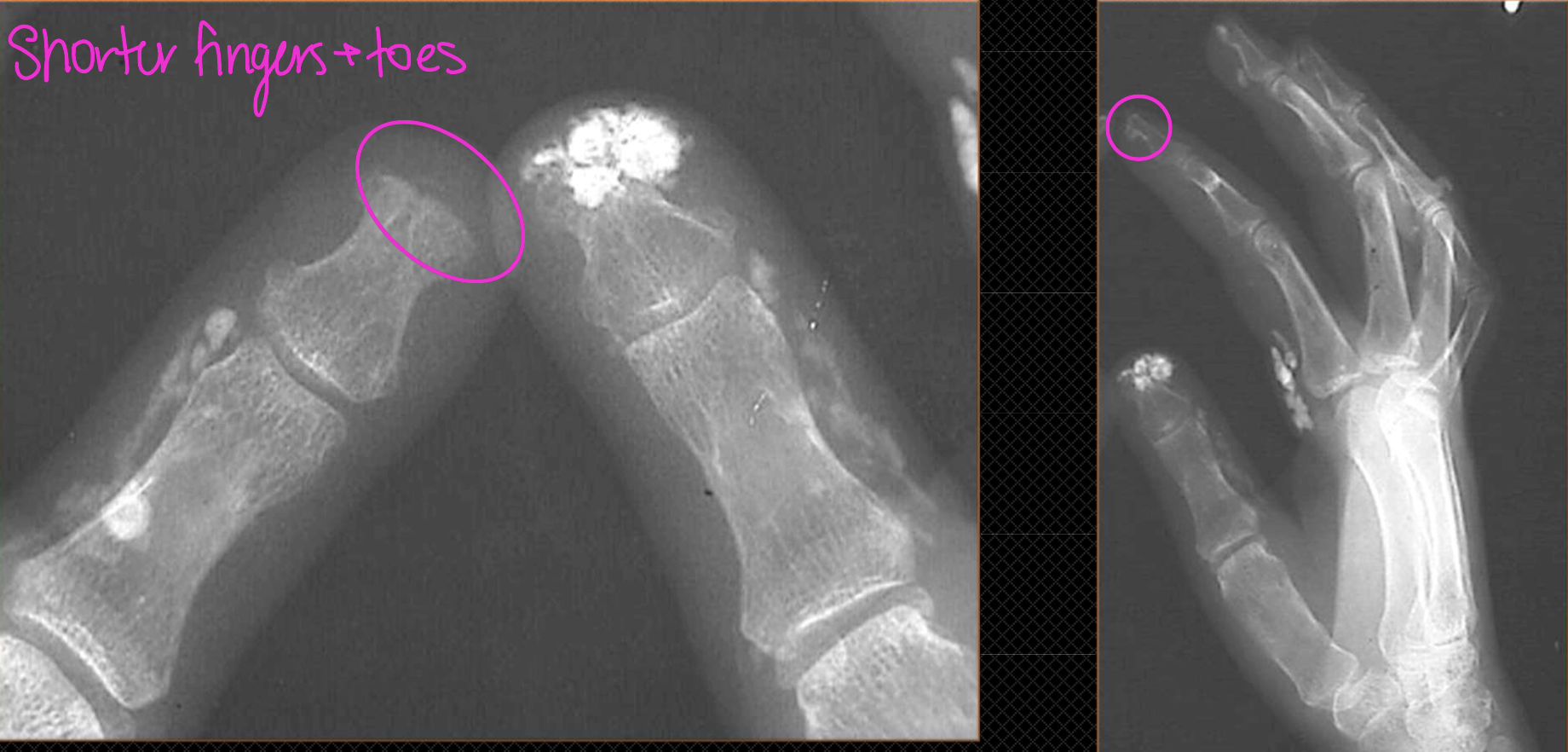
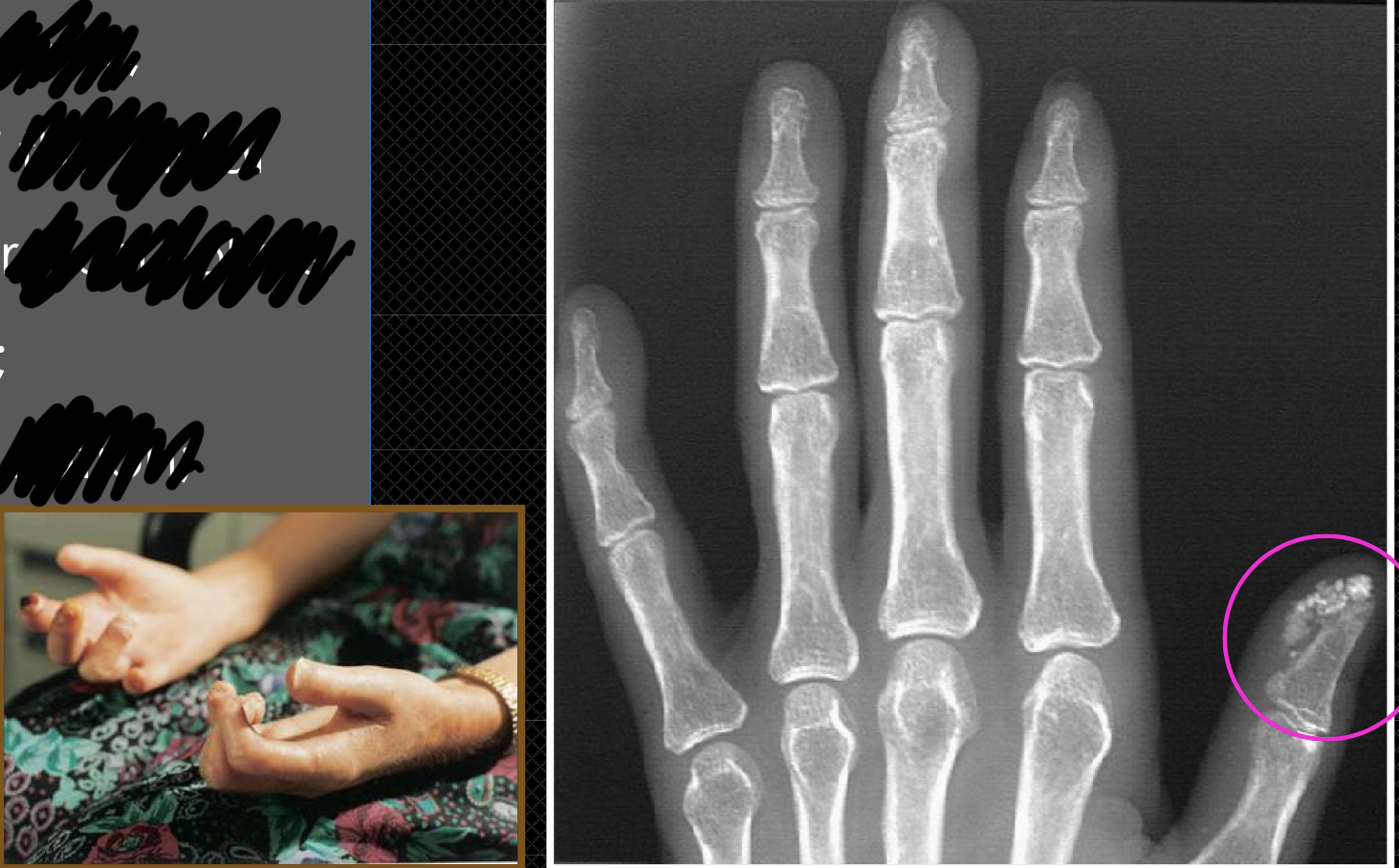
What x-ray finding is present in this pt with Scleroderma (PSS)
acral osteolysis
soft tissue calcifications (calcinosis)
Other causes of acro-osteolysis
burns, frostbite, electric shock, syringomyelia, diabetes
raynaud, sarcoidosis, hyperparathyroidism, leprosy, lesch-nyhan

How to differentiate scleroderma from other causes
just acral osteolysis = think of other causes
soft tissue calcification + acral osteolysis = scleroderma
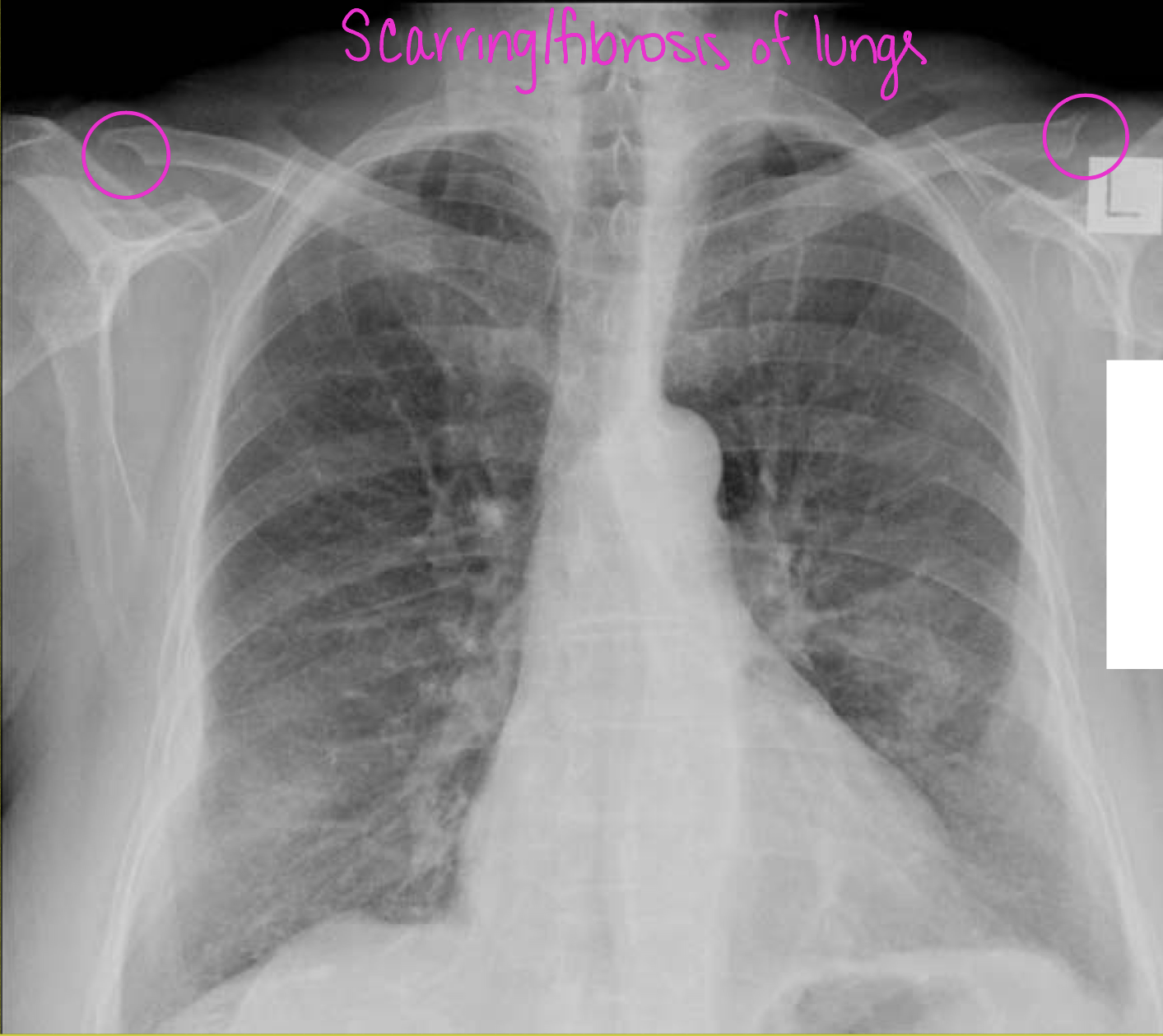
What are some ddx for clavicle erosions
hyperparathyroidism
RA
post-traumatic osteolysis
scleroderma
ankylosing spondylitis
Osteopenia
broad, all-encompassing term describing increased radiolucency of bone
generalized loss
a FINDING (not dx)
If the cause of bone density loss is osteoporosis, use the term
osteoporosis (radiolucency)
generalized loss of bone quantity
regional loss of bone quantity
localized loss of bone quantity
If the cause of bone density loss is NOT osteoporosis, use the term
osteopenia
Hormones and nutrients inhibiting bone production
parathyroid hormone (PTH) *Primary bone absorption*
cortisol
Max bone density in males vs females
Males = 40-50
Females = 35
Non-modifiable osteoporosis risks
>70
asian and caucasian
early onset of menopause
thin build frames
Chances of hip fractures (femoral neck) in women ____ every 5 years after 60yo
double
Primary osteoporosis
Age related (senile) osteoporosis
Post-menopausal osteoporosis (dec estrogen)
Transient or regional osteoporosis (cast/immobilized)
Secondary osteoporosis
coricosteroids
malignancy
infection
Complex regional pain syndrome (CRPS)
You wouldn’t take an ___ if you want to confirm a diagnosis of osteopenia
x-ray (require 30-50% loss before able to see)
Bone scan
evaluate degree the tissues absorb the radiotracer
technetium is absorbed by cells immediately, soft tissues, bone (3hrs)
increased uptake in areas more metabolically active (ANYWHERE)
The Bone scan is a sensitive exam for bone activity, but not a
specific exam
DEXA T scores
T score: amount of bone you have compared w/young adult of same gender with peak bone mass
-1.1 to -2.4 = osteopenia
< -2.5 = osteoporosis
DEXA Z scores
Z score: amount of bone you have compared w/other people your age of same size and gender
abnormally high or low require further tests
T score predicts fracture risk by saying for every -1 SD, the fracture risk
doubles
Orientation of trabeculae
1* = weight bearing (vertical)
2* = stability (horizontal)
3* = tertiary (crisscross)
Bone resorption ordered 3→2→1 (vertical only left)
Osteopenia radiographic findings
cortical thinning (pencil thin)
vertical trabeculae/struts
altered VB shape
There is a normal less dense area within the femoral neck known as
Wards triangle
A compression fracture occurs in a pt with
non-altered bone density
A pathological fracture occurs in a pt with
altered bone density
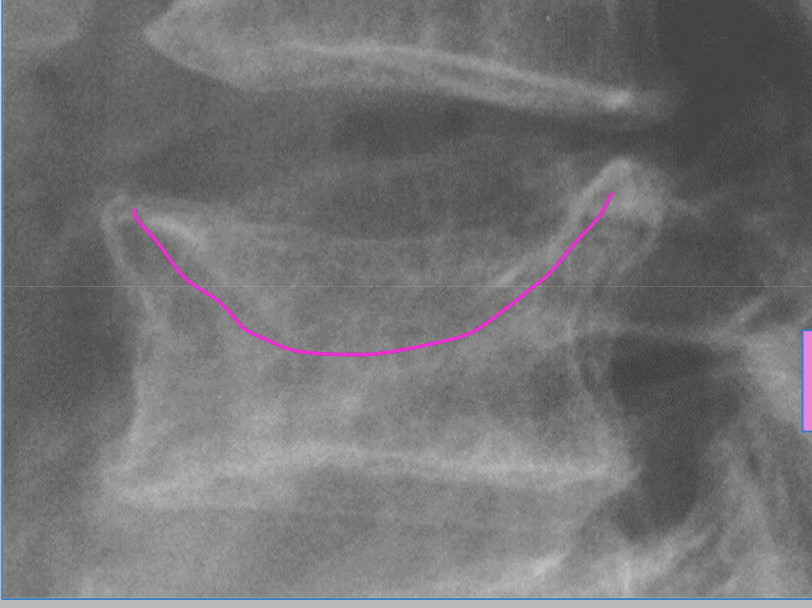
Fracture shapes of osteoporosis
wedge-shaped
endplate concavity
codfish vertebra deformity (biconcave compression fx)
schmorl nodes

What type of fracture due to osteoporosis is shown in the image
codfish vertebra deformity (biconcave compression fx)
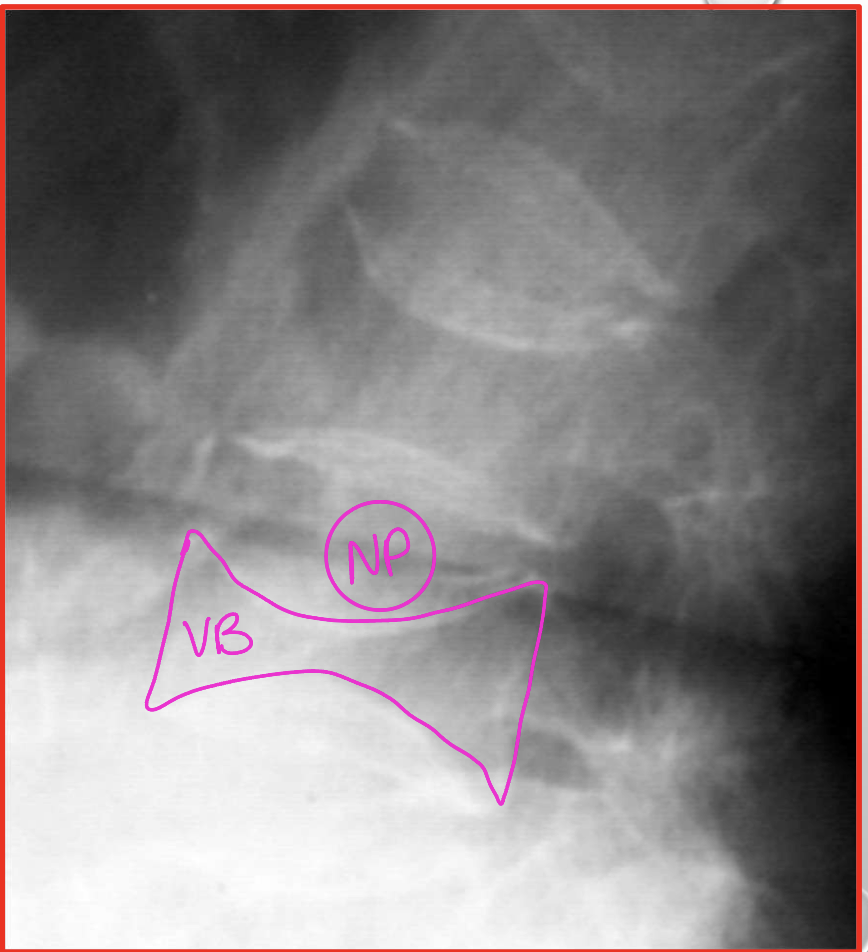
What is a DDX of codfish vertebra deformity
nuclear impressions (nucleus pulposus of IVD)

This patient has hyperparathyroidism which has caused ______ and fractures that made the VB to be smaller than the IVDs
osteopenia
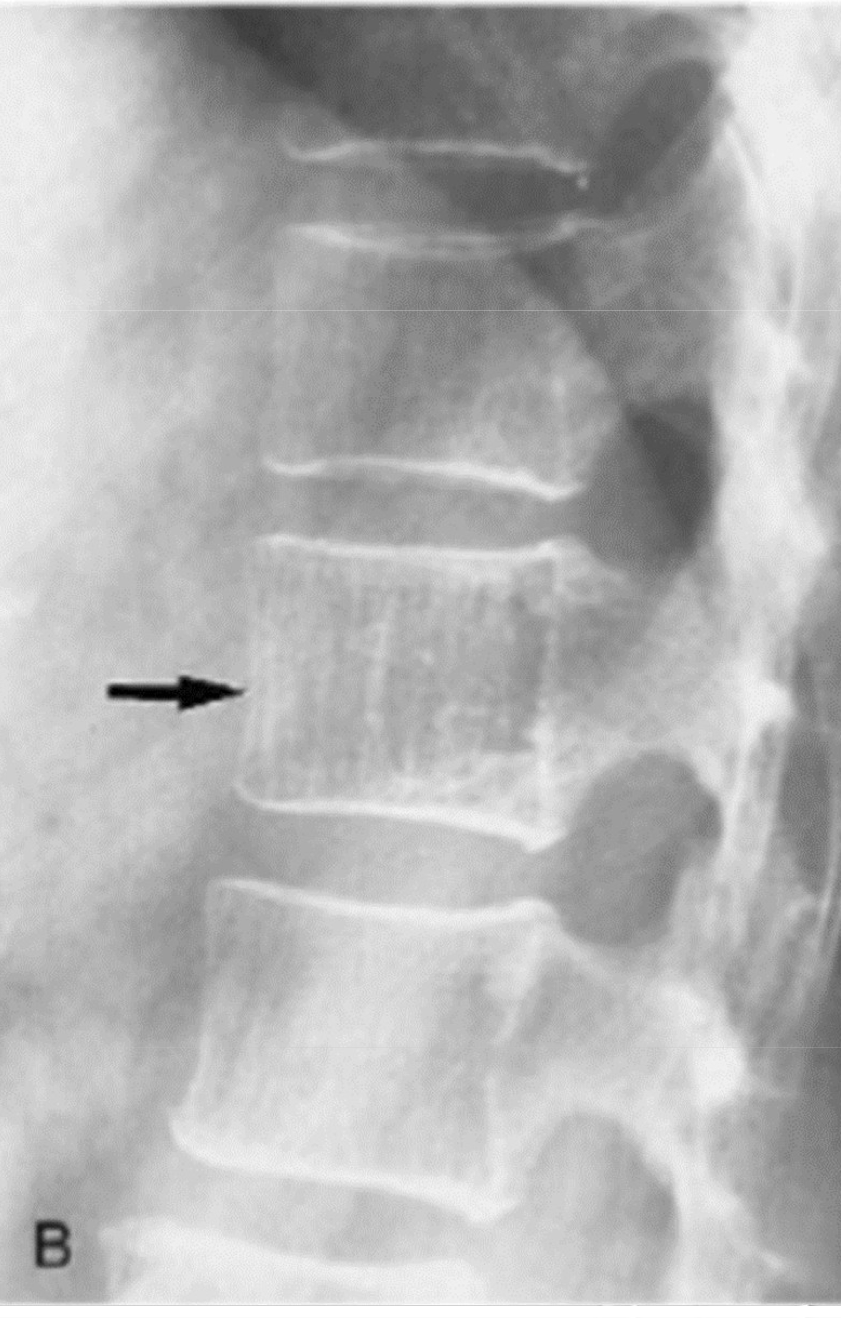
A single vertebra with accentuated vertical trabeculae is a characteristic finding of a benign tumor-like condition of dilated capillaries
hemangioma
Pathological fractures
metastasis (lytic)
multiple myeloma
osteoporosis
eosinophilic granuloma (pediatrics)
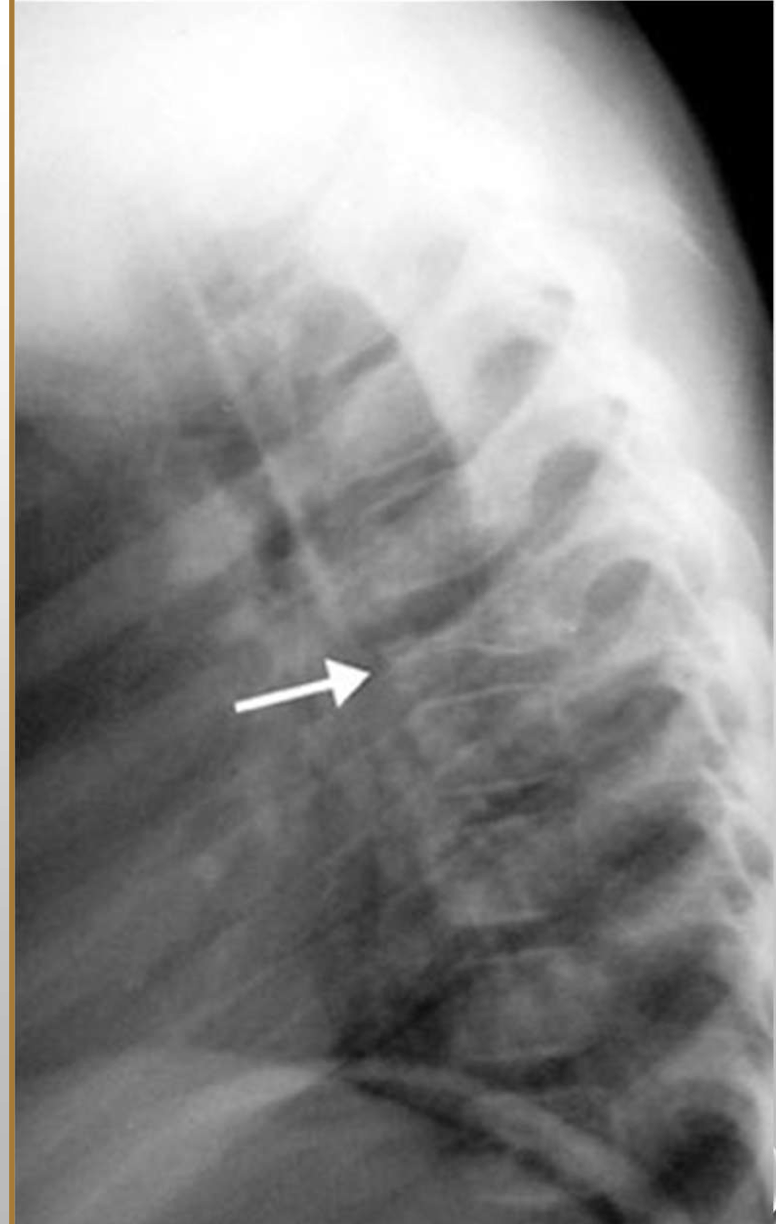
What diagnosis does this pediatric patient have
Eosinophilic granuloma
Disuse osteoporosis findings
diffuse osteopenia of that region
lucent bands of osteopenia proximal to physeal line
subchondral lucency
uniform/spotty demineralization (spotty carpals)
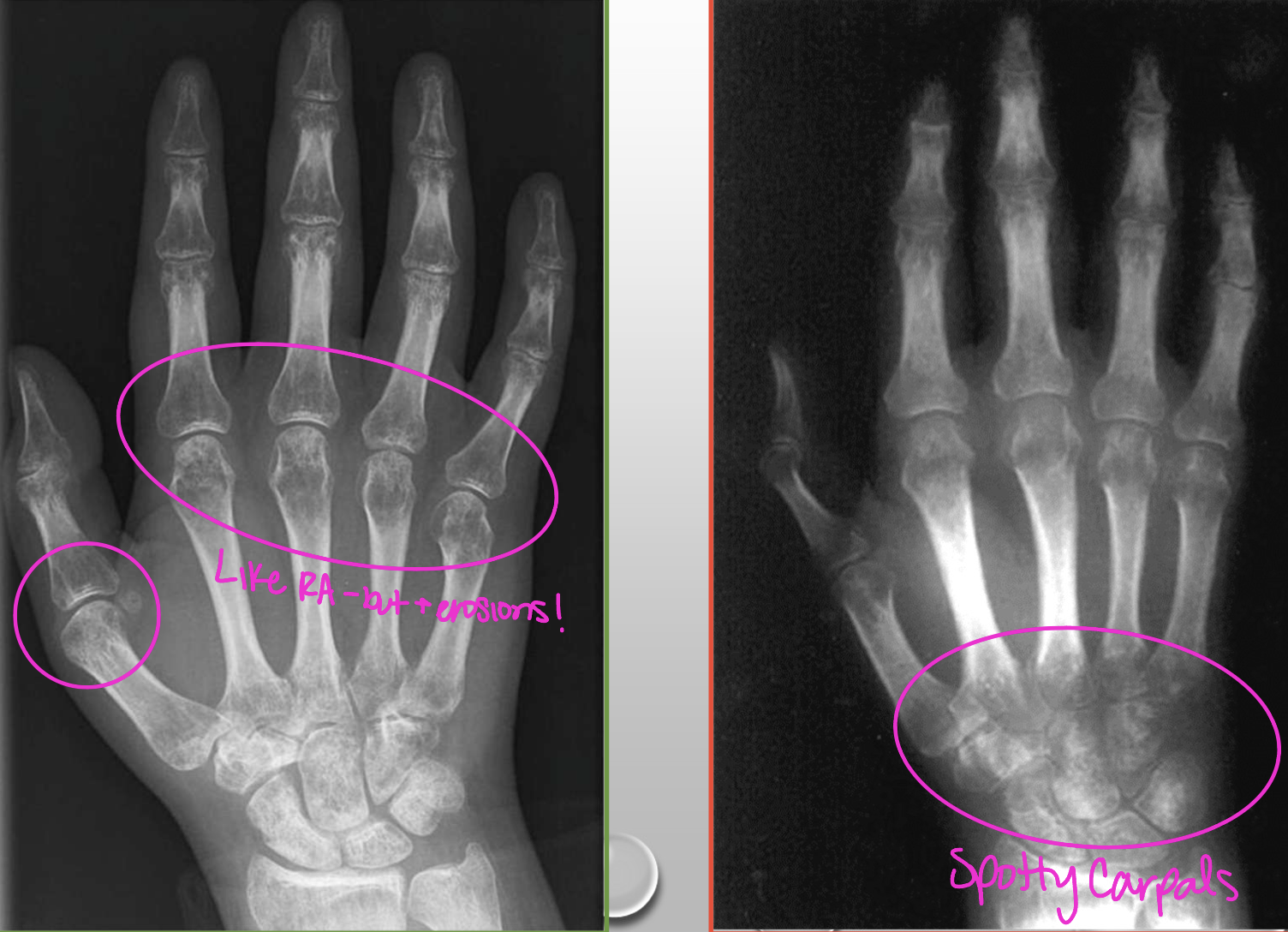
What radiographic findings of Disuse osteoporosis are found in this image
diffuse osteopenia
uniform/spotty demineralization (spotty carpals)
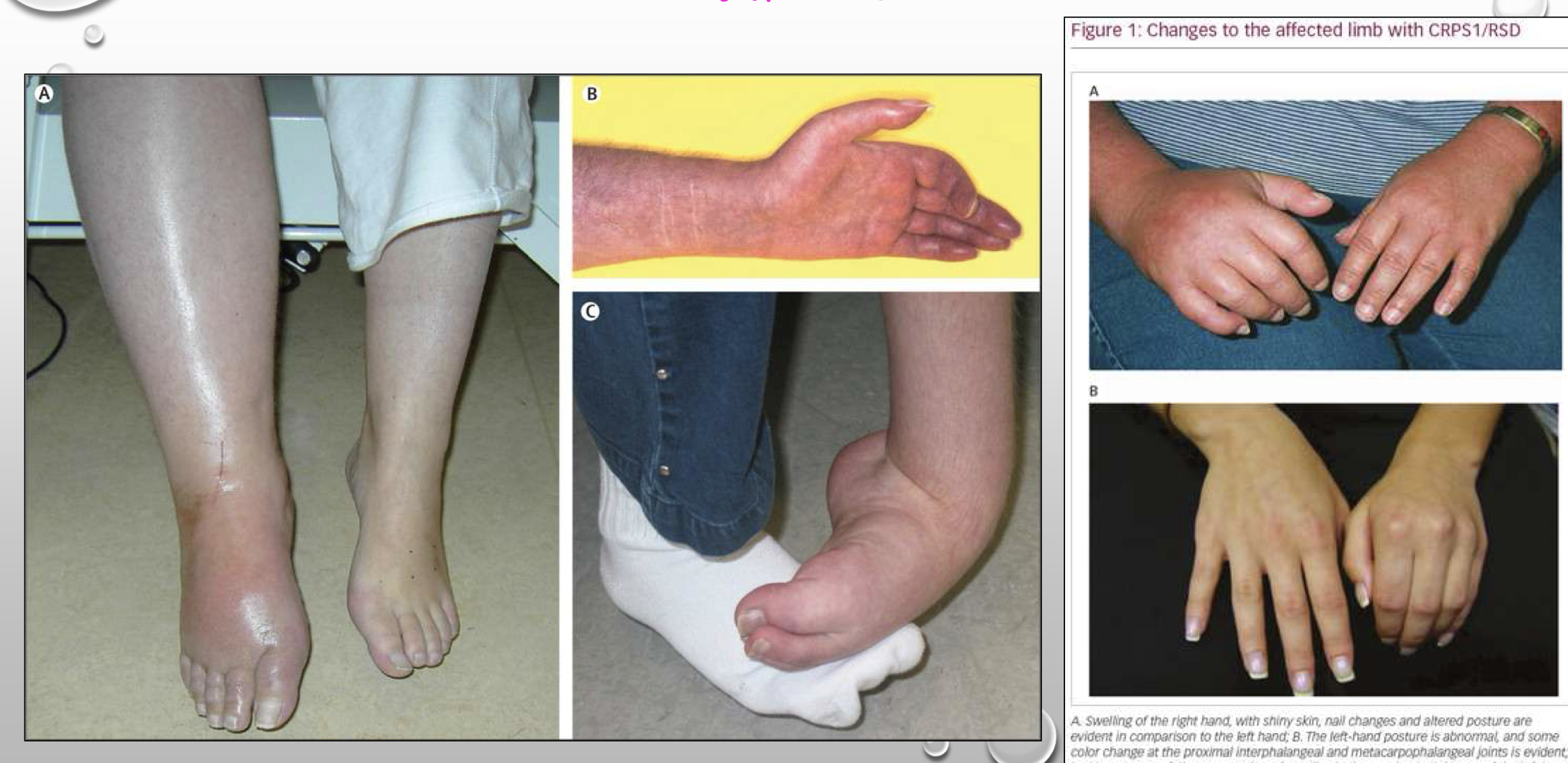
Complex regional pain syndrome (CRPS) osteoporosis
neuropathic pain disorder
allodynia (nerve related pain), hyperalgesia (sensitive to stimuli), sudomotor and vasomotor abnormalities, trophic changes
soft tissue swelling
regional osteoporosis
Complex regional pain syndrome (CRPS) osteoporosis types
Type 1 - absence of nerve trauma
Type 2 - occurs in the setting of known nerve trauma
**Follows a regional distribution

What type of secondary osteoporosis does this pt have
CRPS osteoporosis
Transient Osteoporosis of the hip (TOH)
MC in young adults 20-40 and pregnancy (3rd tri)
MC in men bilaterally
MC in left hip in women
self-limiting over 3-12 months
Transient Osteoporosis of the hip (TOH) findings
periarticular osteopenia w/preserved joint spaces
bone scan - increased uptake of radiotracer (hot spots)
MRI (T2) - diffuse bone marrow edema
An accurate diagnosis of Transient Osteoporosis of the hip (TOH) requires what imaging type
MRI
**sensitive to fluid accumulation
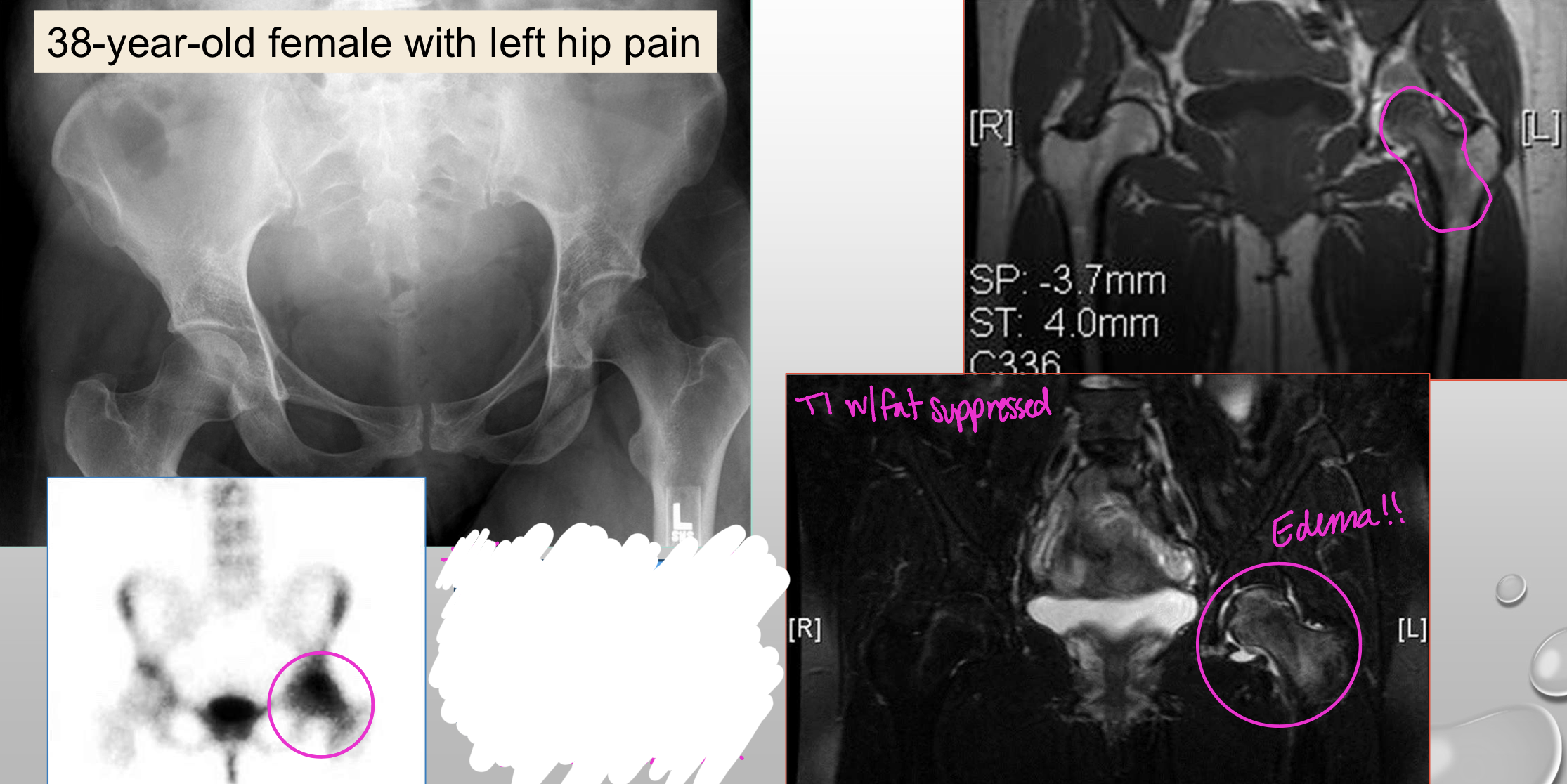
What type of secondary osteoporosis does this pt have
Transient Osteoporosis of the hip (TOH)
Osteomalacia (malacia = softening)
diminished bone QUALITY due to lack of calcium salt deposits
abnormal ratio of osteoid to mineralized bone
Osteomalacia findings
osteopenia
coarsened trabeculae
medial looser zones (pseudofractures) *late sign*
horizontal osteoid lines
basilar invagination
acetabular protrusion
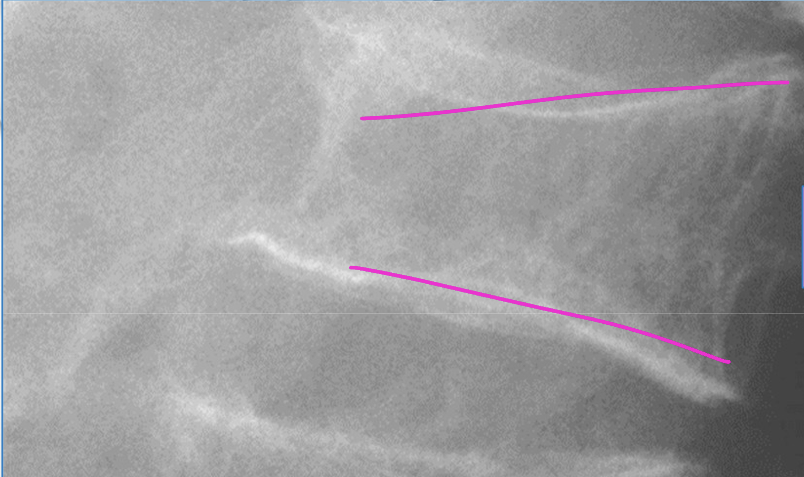
What is required in order to definitively diagnose osteomalacia
bone biopsy

What finding is seen in this image of a pt with Osteomalacia
medial looser lines/zones at most weight bearing part of femoral neck
**Note: we don’t get fractures ½ into bone!!
What radiographic finding of Osteomalacia can be found in RA too
acetabular protrusion (BUT with erosions in RA!!)
Rickets (pediatric osteomalacia)
decreased quantity of calcified osteoid
delayed skeletal maturation (small stature)
soft tissue edema near open ossification centers
Rickets findings
physeal/growth plate appearance
“fraying”
reduced mineralization of cartilage
cartilage overgrowth
bowing deformities
widening/splaying at physes
rachitic rosary in ribs
Rickets findings are common in which type of bones
long bones!
ribs
femur, humerus, tibia, ulna, radius
What radiographic finding is in this image of Rickets
Rachitic rosary
What radiographic finding is in this image of Rickets
Widening/splaying at physes (splayed and frayed)
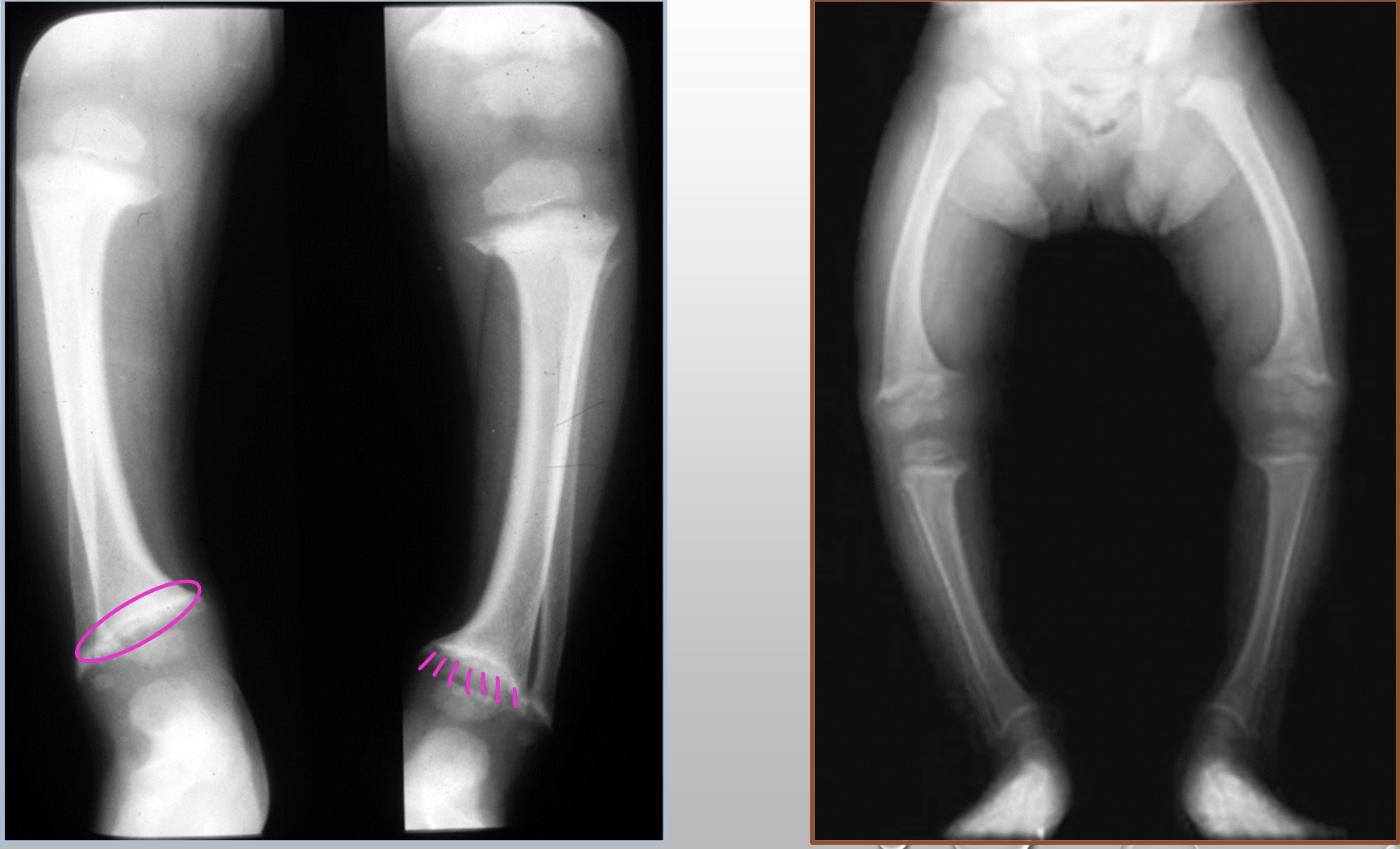
What two radiographic findings are in this image of Rickets
splayed metaphyses (fraying and sclerosis)
bowing deformities (genu varus)
Osteomalacia and Rickets are caused by what deficiencies
vitamin D, calcium, and/or phosphate deficiencies
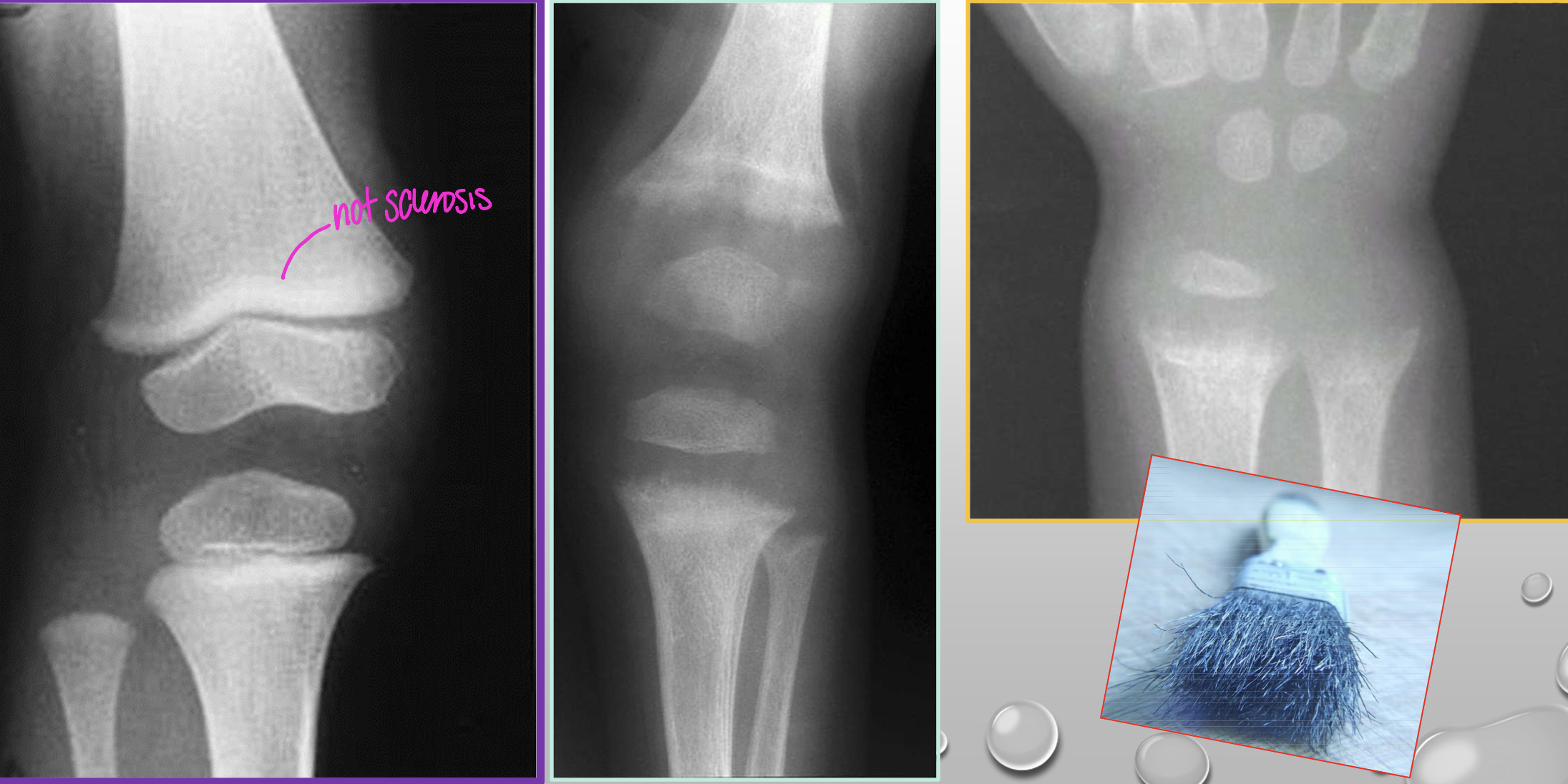
Scurvy (Barlow disease)
vitamin C deficiency
infants that were fed pasteurized/boiled milk (infantile scurvy)
Scurvy (Barlow disease) findings
petechiae, bleeding gums, hematuria
joint edema and pain (frog leg position relieves pain)
mimics non-accidental trauma (abuse)
cartilage is slow to grow BUT mineralizes
osteopenia
Scurvy (Barlow disease) radiographic findings
widened metaphyses (splaying and fraying)
sclerotic/dense zones of provisional calcification (ZPC)
white line of frankel
radiolucent band adjacent to ZPC
scorbutic zone/trummerfeld zone
beak-like metaphyseal outgrowths at right angles to diaphyseal shafts
pelken spurs
dense sclerosis around epiphyses w/lucent centers
wimberger ring sign
irregular metaphyseal margins
corner sign
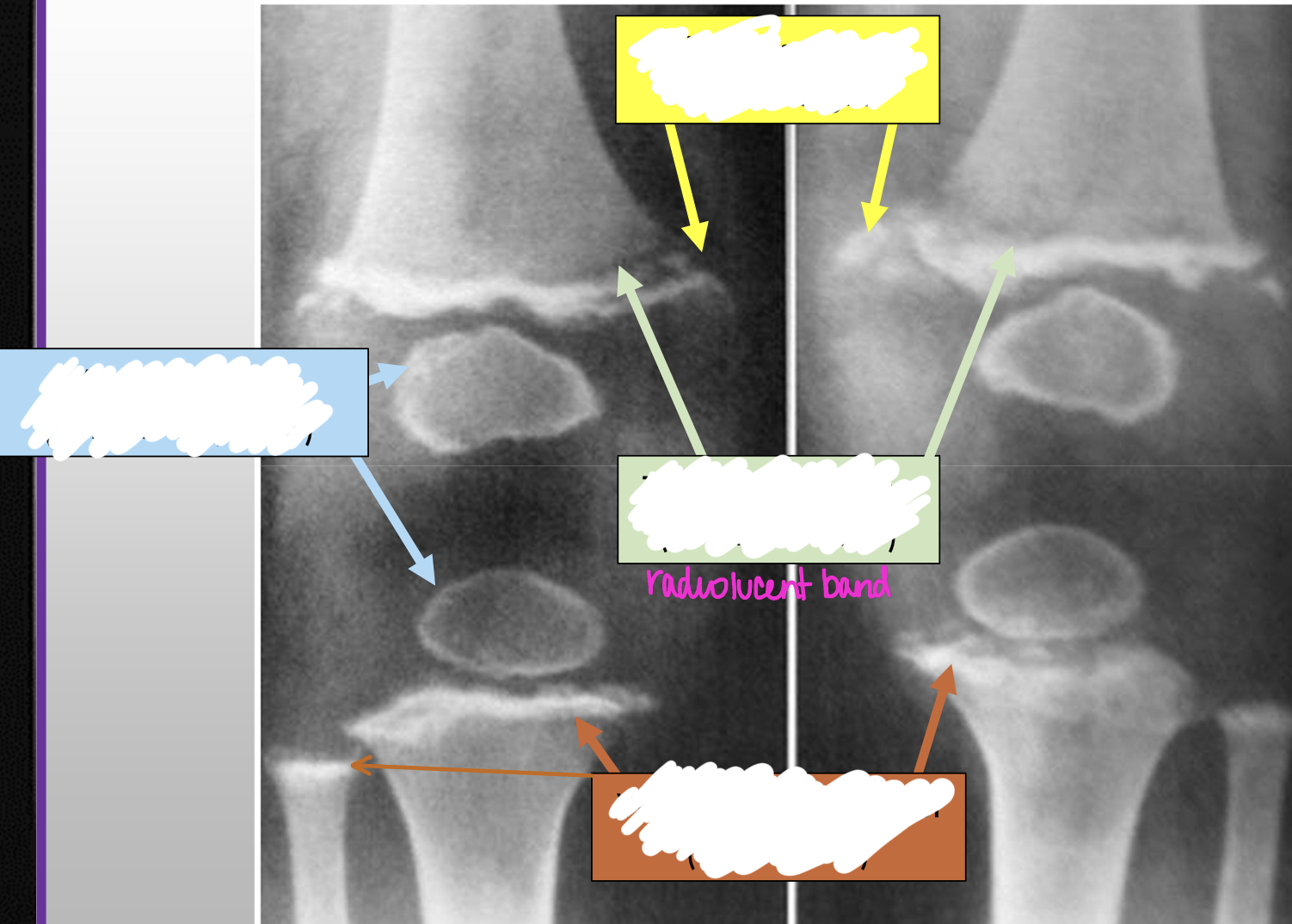
What radiographic finding of Scurvy is in the blue box
wimberger sign (ringed epiphysis)
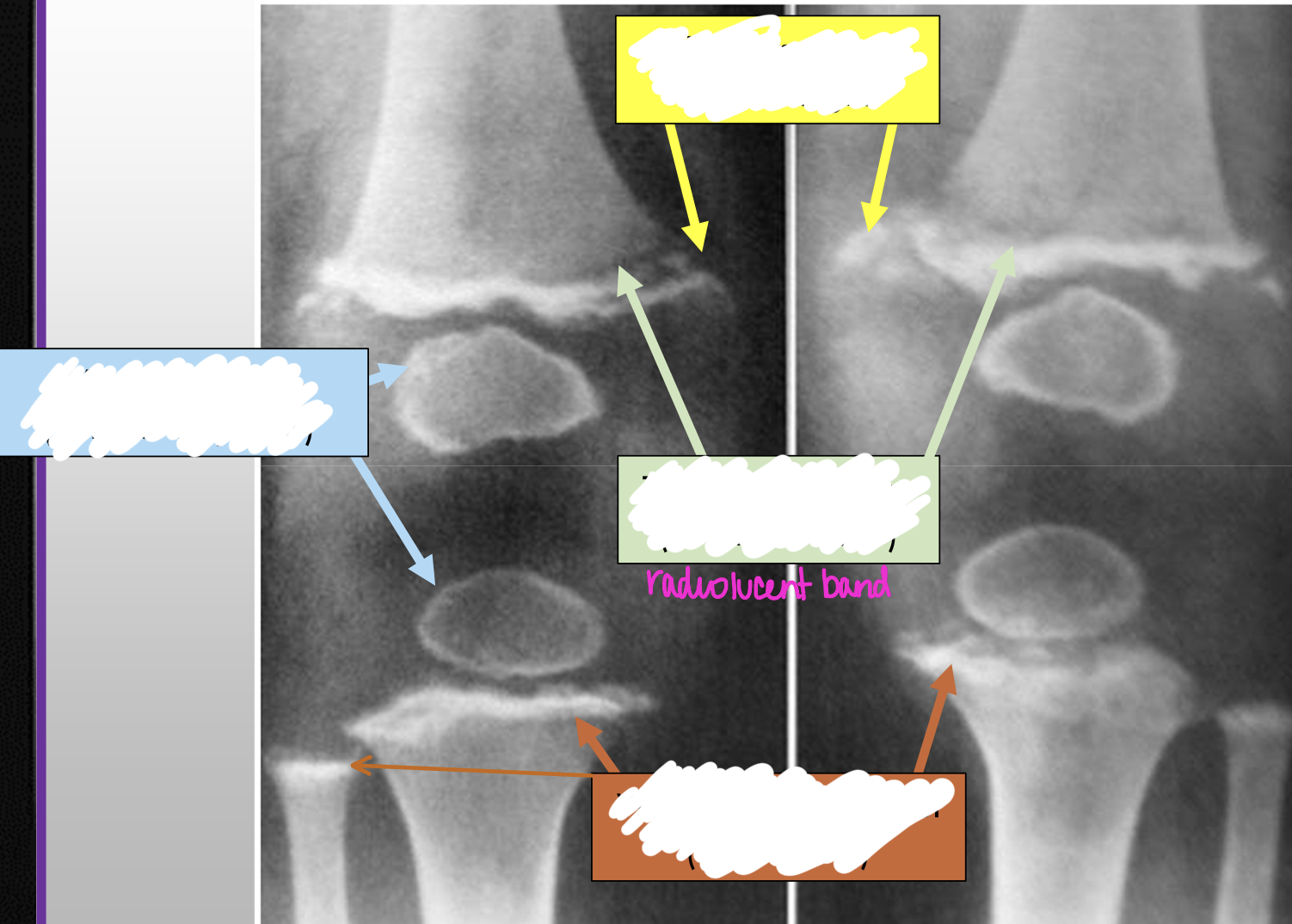
What two radiographic findings of Scurvy are in the yellow box
pelkin spurs
corner signs