Neural Vision & Action - Lecture 5
1/64
Earn XP
Description and Tags
Cerebral Cortex
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
65 Terms
gordon et al. - overview
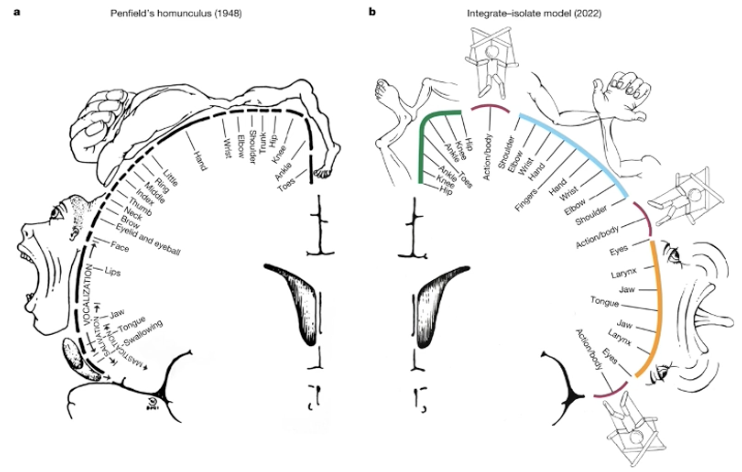
The researchers identified a previously unrecognised system in the human primary motor cortex (M1) called the Somato-Cognitive Action Network (SCAN).
This network challenges the traditional view of the motor homunculus as a continuous map of the body, revealing an integrate-isolate organisational pattern.
gordon et al. - key findings
Interrupted Homunculus: The classic foot, hand, and mouth motor areas are interrupted by three "inter-effector" regions.
While effector-specific areas are responsible for fine motor control (fingers, toes, tongue), the SCAN integrates whole-body action planning and physiology.
Connectivity and Structure: SCAN regions are strongly interconnected and exhibit high functional connectivity to the cingulo-opercular network (CON), which is critical for executive action control, arousal, and pain processing.
Structurally, these regions have lower cortical thickness than effector-specific areas.
Functional Role: Unlike the specific motor regions, SCAN areas lack movement specificity.
They co-activate during action planning and the coordination of large muscle groups (axial body movements like the abdomen or eyebrows) rather than the execution of fine limb movements.
gordon et al. - development and evolution
Development: The SCAN motif is not evident in newborns but is detectable in 11-month-old infants and becomes nearly adult-like by age nine.
Cross-Species Homologues: Precision fMRI in macaques identified similar inter-effector regions connected to the CON, suggesting a conserved evolutionary system for whole-body coordination.
gordon et al. - clinical implications
Stroke and Recovery: The SCAN was found to be preserved even in an individual with extensive perinatal stroke that destroyed large portions of M1, suggesting its vital role in maintaining basic motor function.
Movement Disorders: Due to its connections with thalamic motor nuclei and internal organs, the SCAN may be relevant to symptoms of Parkinson’s disease (e.g., postural instability and autonomic dysfunction) and targets for deep brain stimulation.
primary motor cortex: location
Found within the precentral gyrus, the strip of cortex directly anterior to the central sulcus.
primary motor cortex: function
It contains a "motor map" where specific areas correspond to the movement of different body parts.
primary motor cortex: neural pathways
Signals travel through the corticospinal tract (for body movement) or the corticobulbar tract(for head, neck, and face movement).
non-primary motor cortex: 2 mai regions
Supplementary Motor Cortex: Believed to be involved in executing sequences of movement, acquiring motor skills, and selecting movements based on sensory input.
Premotor Cortex: While it contributes roughly 30% of neurons to the corticospinal tract, it is most active during the planning phase rather than the actual execution of movements.
three primary areas of the motor cortex
Primary Motor Cortex (M1): Located in the precentral gyrus (Brodmann’s area 4).
It initiates voluntary movement and requires the least amount of electrical current to elicit a response.
Premotor Cortex: Located just anterior to M1, it handles movement planning and selection, especially in response to external cues.
Supplementary Motor Area (SMA): Involved in complex action sequences, bimanual coordination, and internally generated movements
motor cortex - organisational principles
Somatotopic Map: The primary motor cortex is organised such that specific areas control different parts of the body, often visualised as a motor homunculus.
Disproportionate Representation: Body parts requiring fine, delicate control (like the hands and face) occupy significantly more cortical space than larger areas with coarse movement (like the trunk).
Agranular Cortex: Unlike sensory regions, the primary motor cortex lacks a distinct granular layer (Layer 4) but contains prominent pyramidal neurons in Layer 5 that send output to the spinal cord.
motor cortex - descending pathways
Corticospinal Tract: The primary direct pathway carrying commands to alpha motor neurons in the spinal cord.
Corticobulbar Tract: Carries motor information to the brainstem to control the head, neck, and face.
Side Loops: The cortex influences "side loops" by projecting to the basal ganglia (corticostriate) and the cerebellum (corticopontine and cortico-olivary) to refine motor performance.
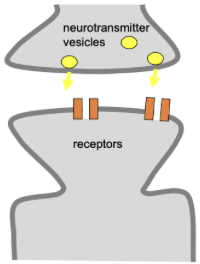
the mechanism of LTP
involves the NDMA receptor
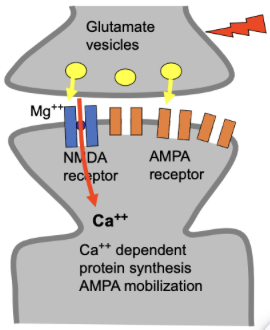
Initial Activation: Glutamate is released and first activates AMPA receptors.
Removing the Block: NMDA receptors are initially blocked by a magnesium ion.
High-frequency stimulation depolarises the neuron, which forces the magnesium out of the NMDA receptor.
Calcium Influx: Once unblocked, calcium ions flow into the neuron through the NMDA receptor.
Strengthening the Synapse: This calcium influx triggers the insertion of more AMPA receptors into the membrane and makes them more responsive to glutamate.
long-term effects of LTP
Sensitivity: The postsynaptic cell becomes more sensitive to glutamate because it has more receptors to respond to the signal.
Retrograde Signalling: Signals may travel back across the synapse to stimulate higher levels of glutamate release from the sending neuron.
Structural Changes: LTP is associated with changes in gene transcription, leading to the production of new receptors or structural modifications that make these synaptic changes long-lasting.
hierarchical sensory-motor organisation
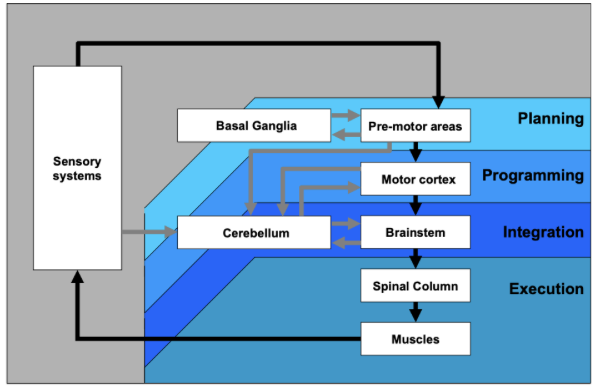
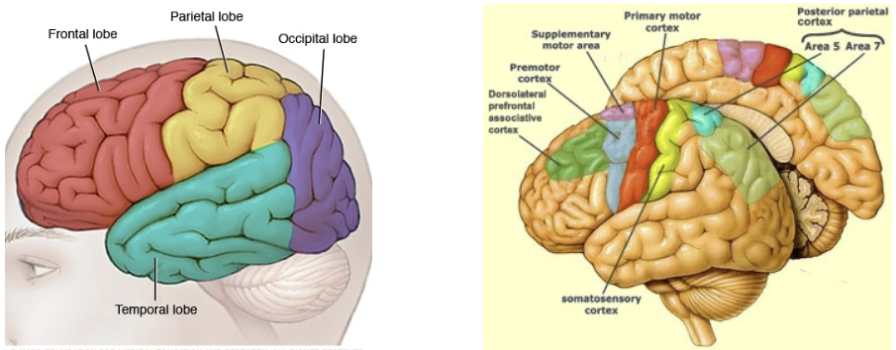
organisation of the cerebral cortex (diagram)
left - very broad subdivision, four different lobes
right - more details of the cortical components of the motor system
primary motor cortex - main output region, sends directly to the muscles
somatosensory cortex - receives signals sent to the brain from the muscles
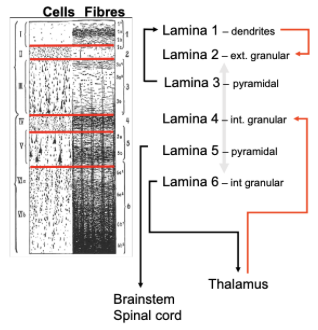
organisation of the cerebral cortex (description)
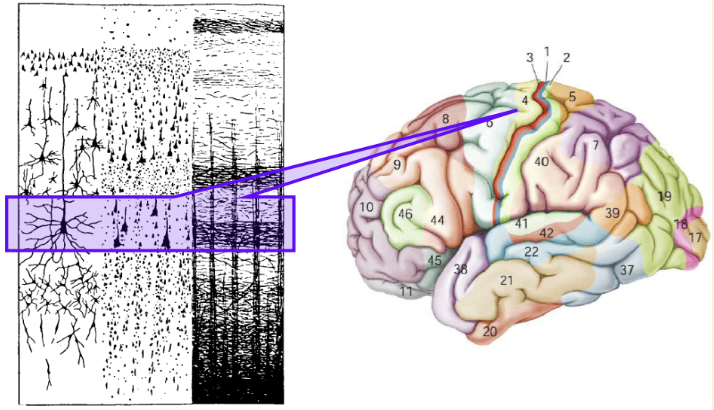
Cortex forms the outer surface of the forebrain (grey matter)
6 distinct layers (‘laminae’). →
Different cell types that receive specific inputs and send specific outputs
Layer 4 is the main input site
Layers 5 and 6 are the main output structures
Cortex covers the other “subcortical” forebrain structures.
Inputs and outputs are layer-specific
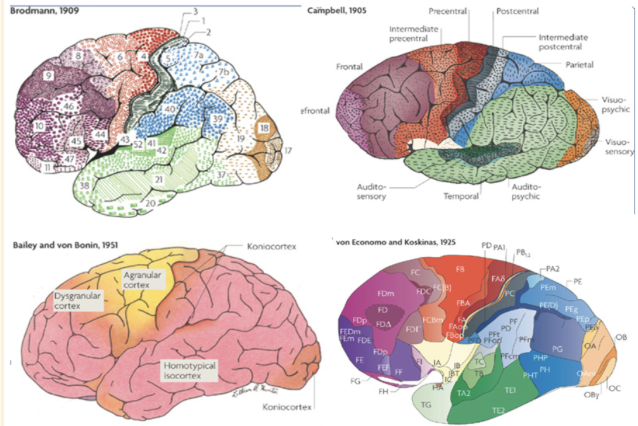
Cytoarchitectural differences (cytoarchitectonics) define different areas
brodmann - described ~ 52 areas
aimed to identify subdivisons
did careful anatomical work looking through brains and looking at transitions between different brain cells
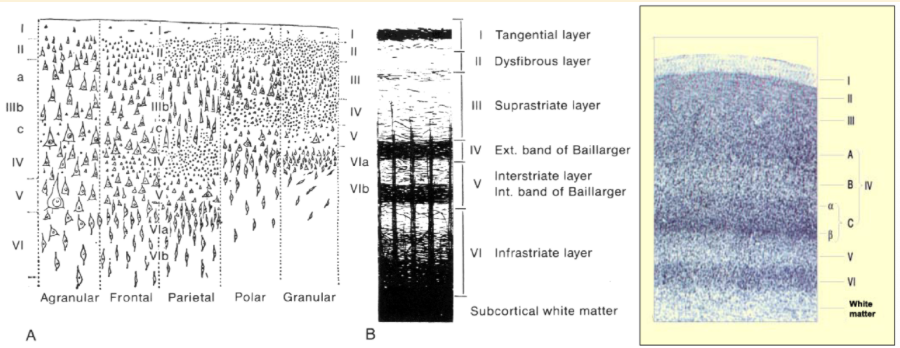
anatomical distinction (brodmann) is functionally relevant
captures regional differences in brain function
gives us a scale of brain function
isolation can be done in various ways and different spatial scales
4: primary motor cortex, and just behind is the somatosensory
function is constrained by the input from other brain regions, and the termination of different outputs
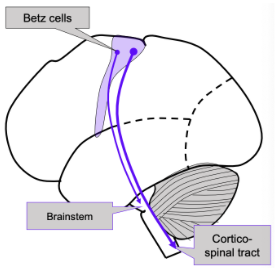
M1 (BA4) contains Betz cells in layer 5 (one of 2 output layers)
project directly to the spinal cord and brain stem
have direct connection to muscles
betz cells - cortical projections
Betz cells – large pyramidal cells
Project from the motor cortex to the spinal tract (cortical tract neurons)
Only 5% project to motor neurons; the rest reach spinal interneurons
Betz cells also project to the brain stem
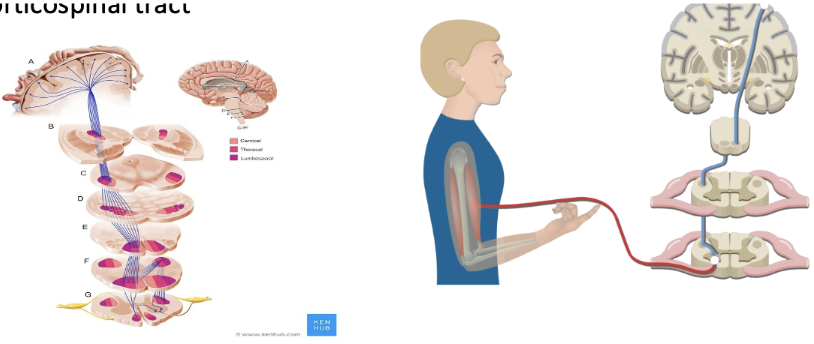
corticospinal tract
Betz cells from the motor cortex initiate, regulate and control voluntary skilled movements by innervating alpha and gamma motor neurons in the spinal cord.
Provides conscious voluntary control of skeletal muscles.
Tract crosses at the medulla (located at the base of your skull), so limb movements are controlled by the contralateral motor cortex.
There is no obvious advantage to this; it is just important to know
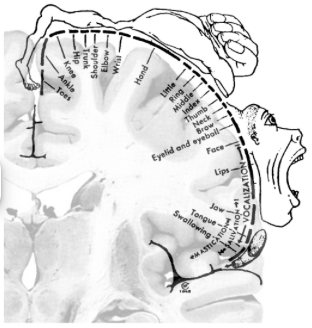
mapping the motor cortex - topography
dedicated regions in the motor region control dedicated regions in your body
At the very top, the motor cortex represents the legs, and as you move down different body parts
fritsch & hitzig - mapping the motor cortex
electrical stimulation in a dog, mapping of the somatotopic motor representation
penfield - mapping the motor cortex
stimulated during surgery on epileptic patients
Discovered that electrical stimulation causes simple movements
Map established (and cartooned ever after)
Cartoon has been called into question (incomplete, general description)
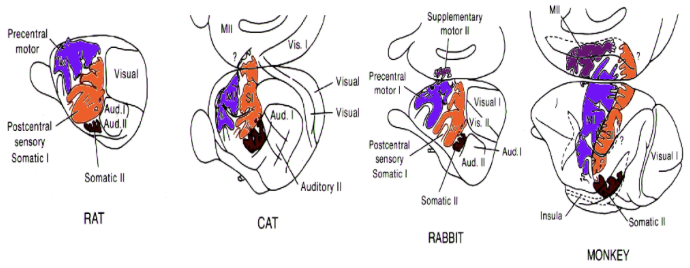
cortical motor maps
Close mirror relationship between sensory & motor maps
Multiple maps: maps reflect sensory-motor specialisation
Rats and cats - a large representation of the whiskers
Monkeys and humans - large representation in the hands - reaching for things
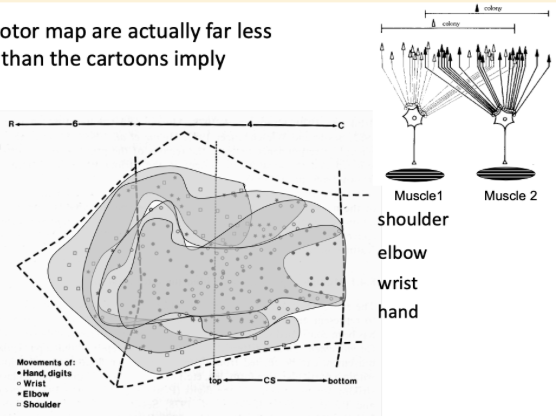
Cortical motor maps are actually far less "realistic" than the cartoons imply
there are parts of the motor cortex that do not obey these rules of specialisation
some parts are not completely separated - overlap
study uses electrical stimulation in the motor cortex, where contractions are caused
areas where stimulation predominantly activates different body parts, but not as clear-cut as the cartoon implies
overlap - possible relates to how much each muscle group works together
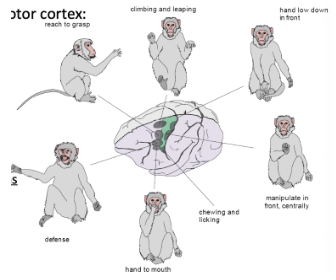
what is represented in the motor cortex: muscles or movements (electrical stimulation)
Brief micro-stimulation (50ms):
Simple movements/contractions of contralateral muscles
Prolonged stimulation:
Complex goal-directed actions
E.g. reaching, climbing, etc.
Previously thought, stimulation of one particular group of neurons would cause contraction in one specific muscle group
However, this was not found in studies; different muscle activity has been observed with different stimulation
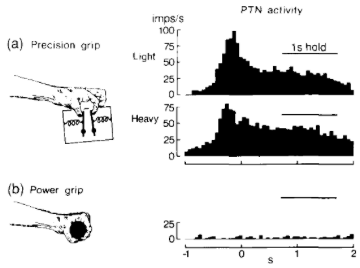
what is represented in the motor cortex: precision grip & skilled use of fingers?
Motor lesions result in a loss of individual finger use
The study was recording activity in the motor cortex of monkeys trained to produce two different types of grip (precision - more difficult, power = simpler, but more force)
Recorded muscle activity with an EMG
Result - activity in the motor cortex is greater for the precision grip than the power grip
primary motor cortex
The primary motor cortex, or M1, is one of the principal brain areas involved in motor function.
M1 is located in the frontal lobe of the brain.
The primary motor cortex is defined anatomically as the region of cortex that contains large neurons known as Betz cells.
Betz cells send long axons down the spinal cord to synapse directly onto the alpha motor neurons in the spinal cord, which connect to the muscles.
Somatotopic contralateral representation is, although far more integrated.
Size is based on precision/fine motor control rather than the size of the body part.
Unclear specifically what the M1 codes, but individual muscles and complex actions can be ‘stimulated’.
In effect, it sends the signals required for movement.
Motor cortical stroke: permanent loss of fine motor control.
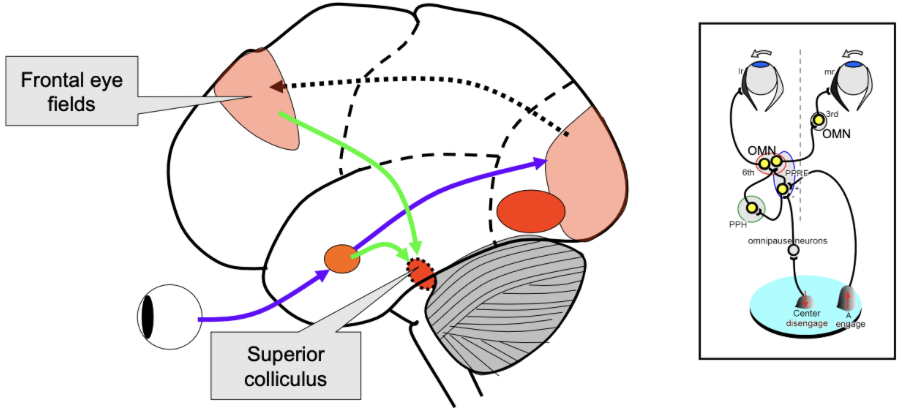
frontal eye fields
region part of the frontal cortex (slightly more towards the front of your head)
proposed to play a key role in the control of eye movement
play an important role in visual attention
receives a lot of input, but also can influence activity in the visual cortex
connected to the prefrontal cortex (involved in decision making)
also have topography- neighbouring regions represent neighbouring regions in visual space
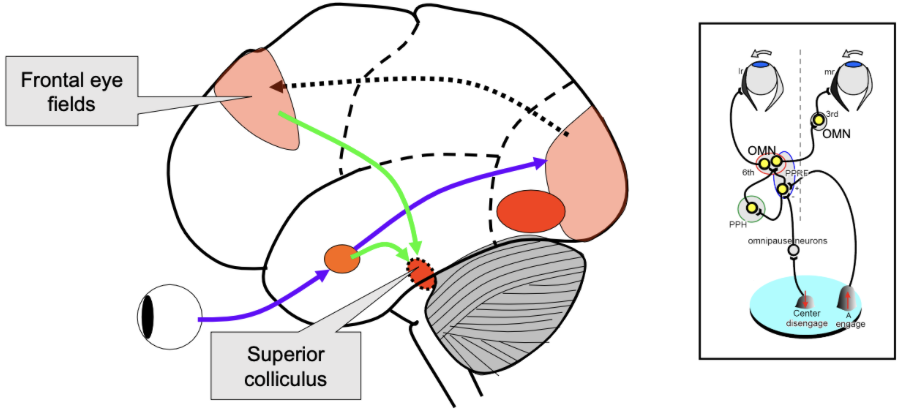
frontal eye fields - superior colliculus
the region that triggers the execution of an eye movement
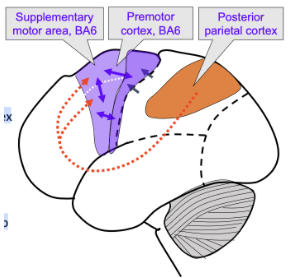
name secondary motor/association areas
Supplementary motor area (SMA)
Pre-motor (PMC)
Dorsal PM (PMd)
Ventral PM (PMv)
Posterior parietal cortex
Typically send input/involved in planning
secondary areas
Very dense connections between secondary motor areas
Heavily connected to the primary cortex, leading to the execution of actions
SMA & PMC are more involved in planning movements
Brain imaging shows activation when imagining or planning a sequence of movements, even if no action is performed
Are active before the movement is executed
posterior parietal cortex (ppc)
Links the frontal cortex (decision-making) with the premotor (planning) areas.
Receives information from sensory regions (visual cortex, sensorimotor cortex etc).
Important for determining potential actions/goals given the environment (pick up coffee, pick up a sandwich, continue working).
The frontal cortex is more critical in decision-making about which action to perform, and secondary areas develop a plan for that action.
Association area - both sensory and motor processes
supplementary motor area (sma)
The very top and the middle of your brain
SMA is now considered to be two areas
SMA proper (learning)
Pre-SMA (execution)
Postural stability
Planning & executing complex sequential movements
Initiation of internally generated movements (rather than stimulus-driven).
dorsal premotor (PMd)
Important in the preparation of movement
Learning conditional actions (response to external cues)
Red traffic light: foot on the brake
Green traffic light: foot on accelerator
Set related activity – (‘get ready, get set, go’)
ventral premotor (PMv)
Important for sensory guidance of movement: responsive to tactile, visual and auditory stimuli
Visuomotor control during grasping
Mirror neurons
PMv and mirror neursons (MNs)
First reported in the ventral premotor cortex (PMv)
MNs show similar activity when a monkey makes a goal-directed action and when the same action is observed (visual), or heard (ripping paper)
Thought to be important for learning through observation.
Also, for understanding other people’s intentions.
Study - observed in other regions of the brain, seem to respond similarly to execution and observation of actions
Maybe it's our motor system that simulates what someone else is doing

mirror neurons and food/object-related responses
MNs only responded to meaningful goal reactions
When monkeys are repeatedly exposed to those types of actions, they complete the same actions, and plasticity in the systems
MNs have only been tested in invasive studies on animals
Only suggested evidence in humans in possible responses
Could be an evolutionary design or a low-level learning function
Human action towards food – strong response
Human action, no food – weak response
Action towards food using pliers – initially, Gallese reported no responses, but monkeys eventually “understood” these actions, and MNs responded

neuroplasticity
The ability of the brain to form and reorganise synaptic connections, especially in response to learning or experience or following injury.
This can occur in all areas of the brain, but there are very clear examples for the somatotopic maps in S1 and M1…
Very pronounced in childhood and early development and decreases as you get older.
Varies very substantially across the lifespan
sensory remapping
Rapid changes in somatosensory (or motor maps) are evident after a change in inputs: training ++ (pianist) & denervation – (amputation)
changes in the somatotopic maps
Training could increase the cortical representation of different factors
After amputation, the part of your motor cortex that is used to represent your limbs may be reassigned to a different body part
Fusion - frequent coactivation of different limbs, like using different fingers together, the cortical maps may become increasingly similar
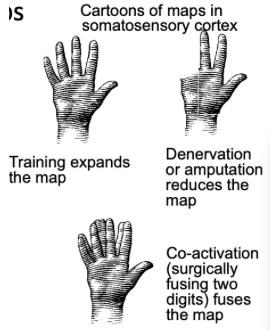
changes in somatosensory maps - an example from co-activation
fusion of motor nerves
fmri with a motor learning task to study neuroplasticity
task: lots of individual finger movements, analyse the cortical activity patterns that happen when moving an individual finger
neat separation of sections of the cortex for different fingers on the same hand
can see how the maps change after extensive training
fuses two of the fingers (index and middle), glued together for 24 hours
uses a repeated measures design to look at the reorganisation of the somatosensory maps
found changes in the somatosensory in the somatotopic maps
changes occurred primarily in the fingers that were not manipulated (fused fingers become less similar to the fingers not glued together)
changes in somatosensory maps - an example from amputation (methods)
neuroplasticity after limb amputation
prediction that amputation might lead to neighbouring regions in somatotopic maps taking over the previously occupied territory
examined patients that has amputations
no longer receiving input would change the cortical representation
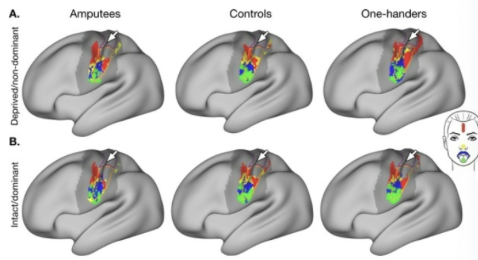
changes in somatosensory maps - an example from amputation (results)
clear separation between the different areas
a group where a hand was amputated later in life, and a group where they never had a hand (grew up without a hand)
found the amputees have a similar somatoptic map to the control
the "one-handers" had other areas taking over those previously occupied areas of the brain
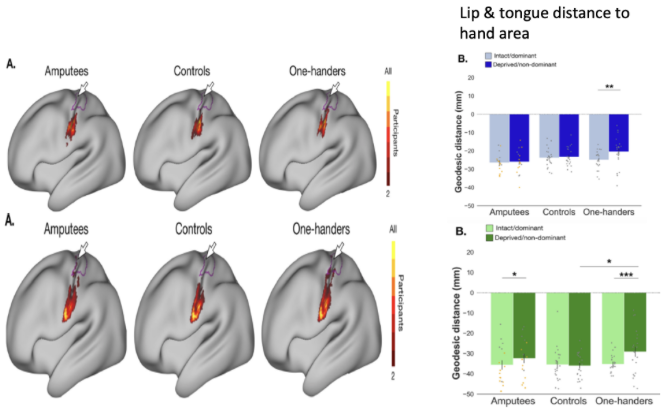
the distances are selectively shorter in amputees on the side that is missing
the effect is consistently stronger in the group of "one-handers"
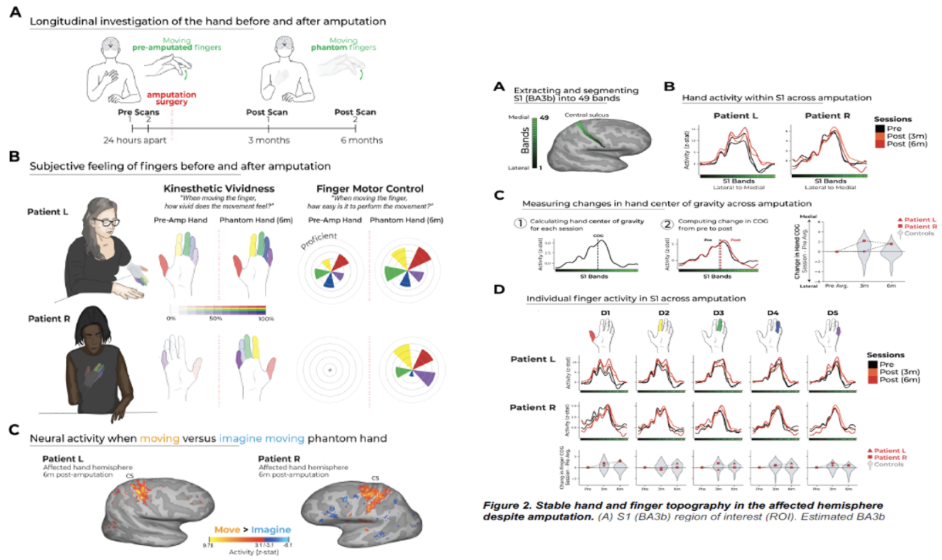
changes in somatosensory maps - patients before & after amptutation surgery
Scanning two patients before and after surgery, where they underwent amputation surgery
Pre-scans 24 hours apart, 3 months after and 6 months after
Collected: how they experienced the movement, how they could control different movements, and “phantom pain”
Looked into reorganisation in the somatotopic maps, e.g. fingers becoming fused, taking over body parts no longer occupied
In both patients, there is convincing evidence that there are no changes in the somatotopic maps
changes in maps reflect neuroplasticity
Long-term changes in functional connectivity, e.g. growth of neurons.
Branching (or pruning) of dendritic connections.
Neurons appear to “compete” for space in the cortex – unused cortex gets taken over by other inputs.
Imaging of the living mouse brain shows changes (growth & pruning) in dendritic branches in the mouse within hours or days of a new task.
However, in humans, some forms of plasticity are very constrained and do not change on a short or even long scale
learning-based neural changes: synapse efficacy
Neuroplasticity can affect all parts of a synapse and even create new synapses
Pre-synaptic
Increase vesicle volume
Increase the availability of vesicles
Increase release probability
Neuroplasticity - increased efficacy
Synaptic cleft
Reduce reuptake mechanisms
Reduce gap dimensions
Post-synaptic
Increase receptor density/area
Growth - new synapses
Make new synapses
long-term synaptic plasticity
Specific timed patterns of neuronal activity (or artificial stimulation) can lead to long-term synaptic changes:
Long-term potentiation (LTP) is an activity-dependent persistent strengthening of synapses.
These produce a long-lasting increase in signal transmission between two neurons.
Long-term depression (LTD) is an activity-dependent reduction in the efficacy of neuronal synapses.
These produce a long-lasting decrease in signal transmission between two neurons.
associative LTP induction
The NMDA channel is normally blocked by Mg ++
Concurrent voltage change to drive out Mg ++ (action potentials or electrical stimulation)
Achieved by glutamate binding to nearby AMPA receptors
Equivalent to stimulation with high-frequency electrical pulses
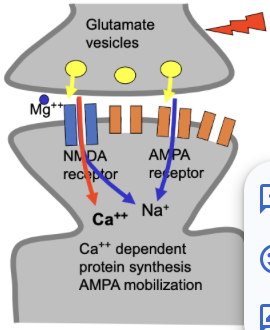
Glutamate binds to NMDA & AMPA receptors
A temporary change in the shape of the channel opens up the channel
Calcium can enter through the open, unblocked NMDA channel
Ca++ entry triggers an intracellular signalling cascade, which results in:
Migration of AMPA receptors from intracellular stores to the cell membrane
Synthesis of more AMPA receptors
key principles of LTP
Cooperatively: LTP requires simultaneous activation of a large number of axons (due to large depolarisation).
Associative: When weak synaptic input is paired with strong, then large depolarisation can propagate and cause LTP at the synapse with weak input. (strong can activate weak)
Synapse-specific: If a particular synapse is not activated, then LTP will not occur even with strong post-synaptic depolarisation.
importance of learning and memory
Cooperatively: ensures that only events of a high degree of significance (that have sufficient active inputs) will result in memory storage.
Associative: allows an event with little significance (CS) to be endowed with a higher degree of meaning if associated with a significant event (US).
Synapse-specific: Inputs that convey info not related to a particular event will not be strengthened to participate in a given memory.
Long-Term Depression (LTD)
First identified in the hippocampus, thought to be a major component of motor learning in the cerebellum.
Decrease in neural communication
Cerebellar LTD involves a decrease in AMPA receptors.
However, this is not NMDA-dependent.
Does not require magnesium
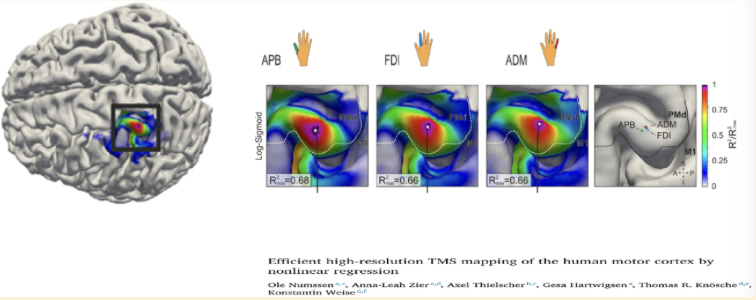
numssen et al. - measuring in humans (TMS) - overview
used to externally stimulate the brain
magnetic field is delivered to a coil
initially used in clinical practice, but is becoming a prominent tool in neuroscience research
Transcranial Magnetic Stimulation (TMS) is a non-invasive procedure that uses magnetic fields to stimulate nerve cells in the brain.
It is most commonly used to treat depression when other treatments haven’t been effective, but it is also a vital tool in cognitive neuroscience research.
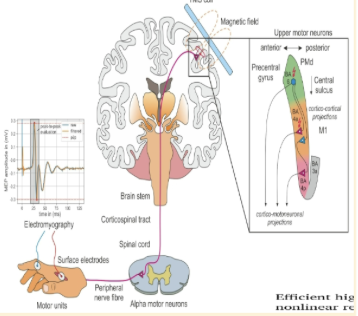
numssen et al. - measuring in humans (TMS) - electromagnetic induction
A handheld treatment coil is placed against the scalp.
When a high-intensity electrical current passes through this copper coil, it creates a powerful, rapidly pulsing magnetic field that lasts for only microseconds.
numssen et al. - measuring in humans (TMS) - passing the barrier
Unlike direct electrical stimulation, magnetic fields can pass through the skin and skull completely painlessly and without interference.
The magnetic field typically penetrates the cortex to a depth of about 2–3 centimetres.
numssen et al. - measuring in humans (TMS) - inducing electrical activity
Once the magnetic field reaches the brain tissue, it induces a secondary electrical current in the neurons.
If the pulse is strong enough, it causes the neurons to "fire" (depolarise).
Single Pulse: Used to see how the brain controls muscles (e.g., making a finger twitch).
Repetitive TMS (rTMS): Involves thousands of pulses in a session.
Over time, this repetitive firing can strengthen or weaken specific neural pathways—a process known as neuroplasticity.
numssen et al. - measuring in humans (TMS) - targeting specific regions
For clinical treatments like depression, the coil is usually placed over the Dorsolateral Prefrontal Cortex (DLPFC).
This area is often underactive in people with depression; by "exercising" these circuits with TMS, the brain can eventually regain more normal activity levels.
measuring the somatotopic map with TMS
maps out individual fingers
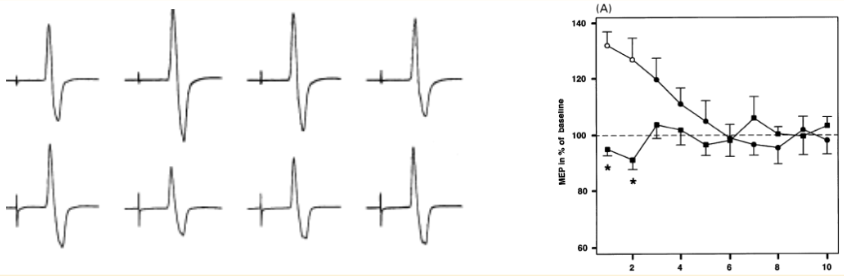
measuring LTP-like and LTD-like mechanisms with TMS
MEPs are sensitive to learning and neuroplasticity
amplitude of MEPs is enhanced in the group learning the motor skill for a period of time (~5 minutes)
can measure broad markers of neuroplasticity in humans using TMS
not as good as invasive tools, but it is an ethical window into understanding
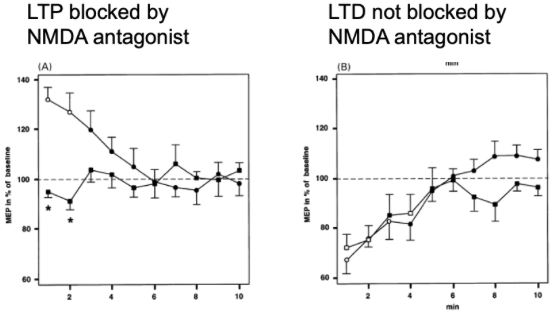
LTP-like and LTD-like mechanisms in humans
Pharmacological approach to the mechanisms of transcranial DC-stimulation- induced after-effects of human motor cortex excitability.
One group is undergoing learning, and the other group is not
No difference in LTD between the different groups
gordon et al. - Effector maps might not be the only organisational principle within the motor cortex
Effector-specific regions are interdigitated with regions showing different connectivity, structure, and function
Inter-effector regions that show high connectivity to each other and to the cingulo-opercular network
Replicated in various data sets (including infants, newborns, and non-human animals)
Inter-effector regions become active during planning (rather than execution) and lack effector specificity
Interpreted as Somato-Cognitive Action Network (SCAN)
results were very reliable across many different ppts, also had a high test-retest reliability
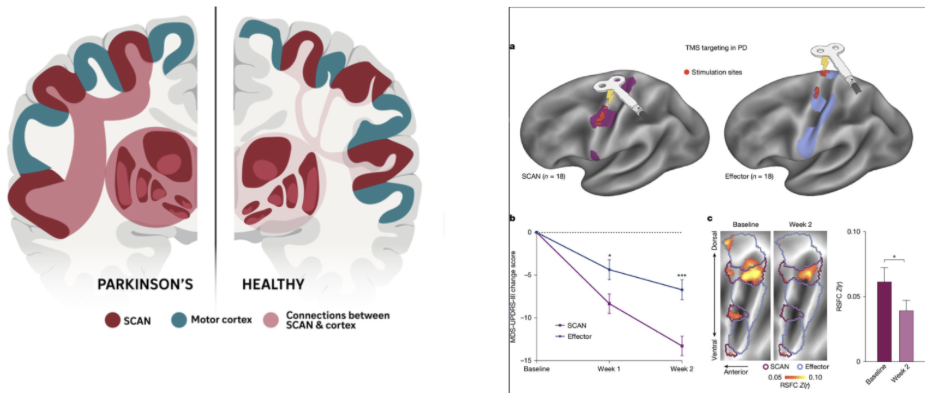
ren et al. - Effector maps might not be the only organisational principle within the motor cortex
Somatotopic Cognitive Action Network seems to be implicated in Parkinson’s disease
Hyperconnectivity between inter-effector regions in PD and subcortical regions that are common targets of deep-brain stimulation treatments
Targeting inter-effector regions (instead of effector-specific regions) improves clinical outcomes of brain stimulation treatments
Mirror neurons are thought to contribute to Theory of Mind (our ability to infer another person’s mental state). They were first observed in…
…the ventral premotor cortex (PMv)
Which of these statements about the Somato-Cognitive Action Network is false?
It is located in the premotor cortex