P2
1/29
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
30 Terms
How is the aerosol formed by the propellant?
Formed as a gas is compressed
Pressure coverts the gas to a liquid
Then converted to a gas when the pressure is released, and liquid boils quickly to gas.
In the propellant; what converts the gas to a liquid and then to a gas
Pressure
And then the release of this pressure.
In a pmdi, the drug is in the device starts as what and what does it turn into?
Gas to liquid by pressure
Drug formulated in the liquid
When pressure is release, the liquid propellant rapidly boils to form a gas.
Gas→liquid→gas.
The gas leaves behind an aerosol of drug particles.
What are HFA pMDI’s?
Why are CFC’s no longer used?
Current pMDI propellants are hydrofluroalkanes
CFC’s = chlorofluoroalkanes we’re once used. Are now banned as they deplete the ozone layer.
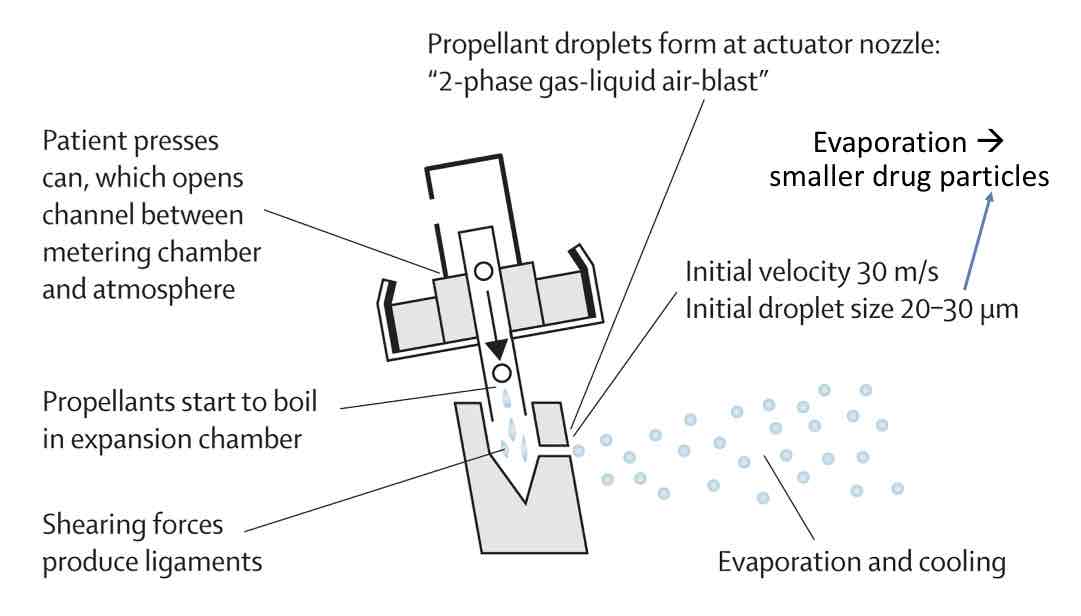
How is the spray formed?
Drug formulations for pMDIs?
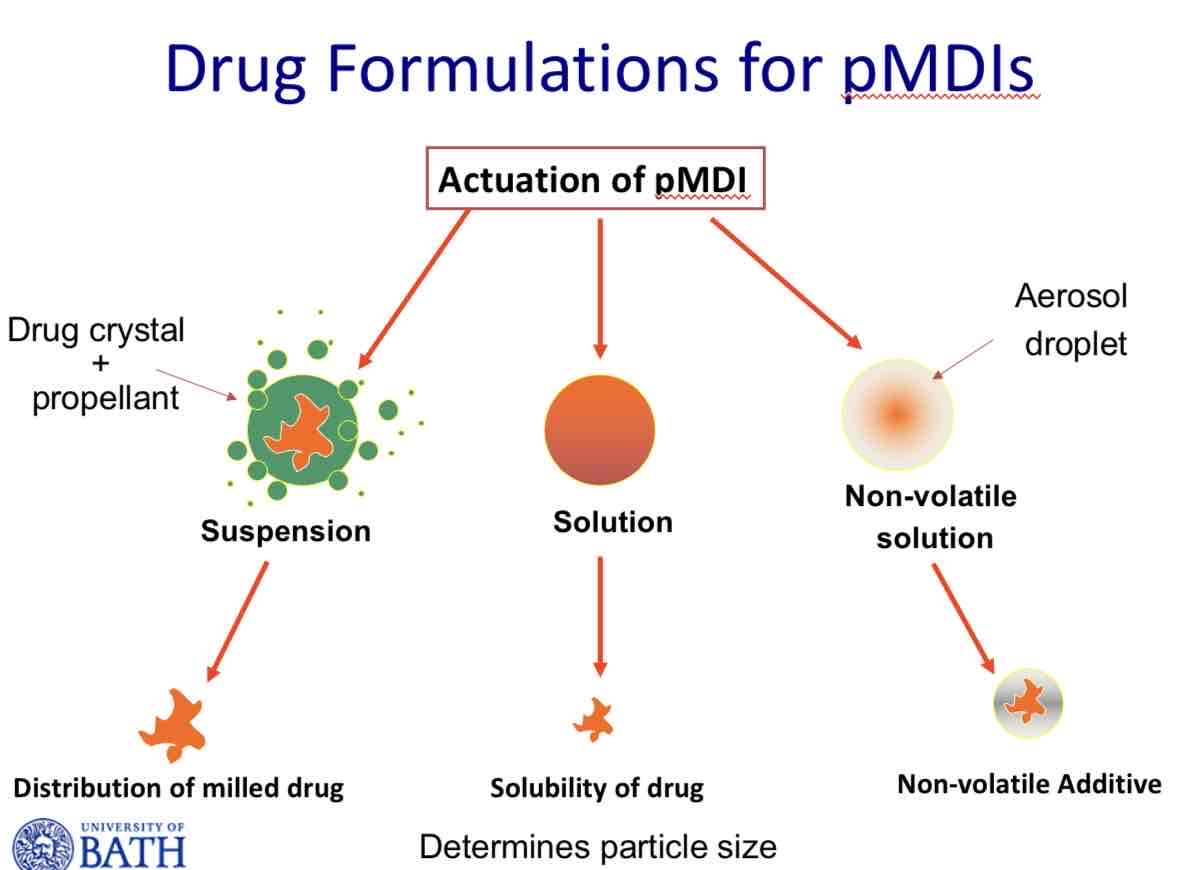
For most drugs, what formulations are generally preferred?
Suspensions
Why are suspensions generally preferred?
Capable of delivering high powder loads
What are the requirements for having suspensions as formulation, for pmdi?
Needs drugs to be milled/ micronised
Needs drug to be practically insoluble in propellant
Drug needs to be freely dispersed in the propellant.
So need to shake to ensure re-dispersion and formulation is homogenous.
Physical instability:
Rapid Flocculation
Loose Agglomerates (Interparticulate Forces)
Physical instability:
Bulk separation
Creaming or sedimentation (density, particle size)
Physical instability:
Irreversible aggregation
Crystal growth and caking (solubility)
Physical instability:
Crystal structure instability
Polymorphic inter conversion.
Flocculated system vs deflocculated system

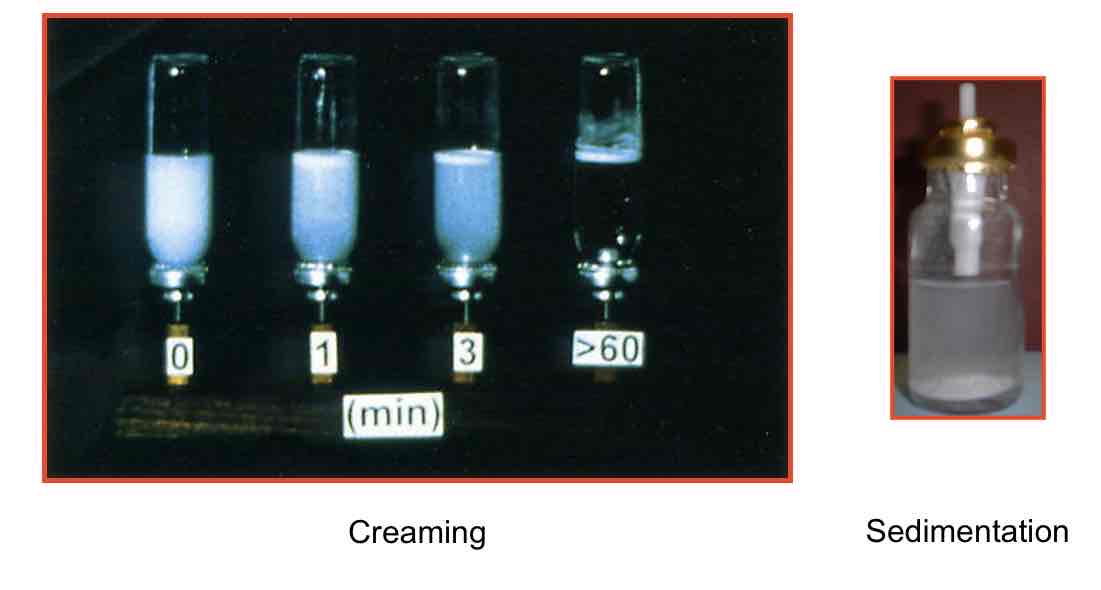
What does creaming and sedimentation look like?
What is the role of excipients?
Ensure physical stability of suspension
Capable of dispersing and re-dispersing drug in suspension
Allows homogenous distribution of drug within suspension.
Minimal segregation during period prior to administration.
What are commonly used surfactants in HFA propellants
Oldie acid, PEG, PVP, magnesium stearate
What are typical suspension formulations?
Micronised drug
Surfactant - like oleic acid
Propellant - HFA 134a (e.g).
Testing the pMDI formulation:
Testing for:
sedimentation rates
Particle size changes
Dose uniformity measurements
Ultimate test - uniformity in the aerosol dose (Consistent dose and particle size distribution needs to be consistent also)
Solution based formulations:
What are the requirements and when can they be used?
Can only be used if solubility and stability of drug in propellant with co-solvent are adequate.
Need to check the chemical stability of drug in the solution.
The amount of dose emitted is directly related to solubility
Usually needs a co-solvent (like ethanol)
Name a co solvent that is usually used with solution based formulations for inhalers?
Ethanol.
Do solution based formulations have the potential to crystallise out during their shelf-life?
Yes.
Solution based formulations with cosolvents have potential to crystallise out.
What is the typical solution based formulation?
Drug (not micronised)
Ethanol (co-solvent)
Saccharine (for taste)
Menthol (for flavour)
Ascorbic acid (antioxidant)
Propellant (vapour pressure)
What are the problems associated with solution based formulations?
Co solvents can erode aluminium canisters
Drugs can be relatively unstable
There needs to be modification of drug chemical structure.
What are the advantages of pMDI’s?
+ many doses
+ Compact
+ Consistent delivery
+ Relatively cheap
+ Sealed container protects the drug
+ Lower capital costs for market entry.
What are the disadvantages of pMDI’s?
- Patient co-ordination and force is needed to actuate the drug
- Cold freon effect
- Tail off at the end of a can
- Force of aerosol spray
- Varying deposition pattern in airways
What devices can you use to train a patient to use their inhaler?
Vitalograph AIM
In-Check Dial

Spacers
pMDI actuated into a chamber with a valve to prevent aerosol escaping
Patient can then inhale aerosol from spacer
Gives space for particles to slow down
Propellant evaporates smaller particles
No “cold Freon effect”
No need to coordinate
actuation & inhalation
Washing spacers
Electrostatic charge can cause drug to adhere to spacer
Regularly clean spacer with water with a drop of washing up liquid
Allow to air dry – do not rub with a cloth
Summary
pMDIs are a convenient dosage form
Requires a pressurised propellant
Both solutions and suspensions possible
Many patients have difficulties using them, which can lead to poor disease control
Patients need your support with pMDIs
Important to reduce pMDIs where clinically appropriate