LE Peripheral Arterial (A&P & Fluid Dynamics)
1/83
Earn XP
Description and Tags
CVT Vascular 1
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
84 Terms
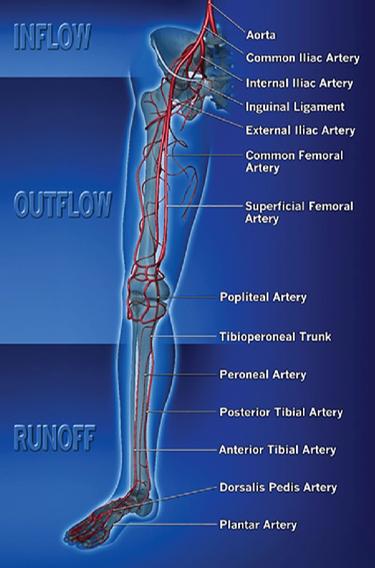
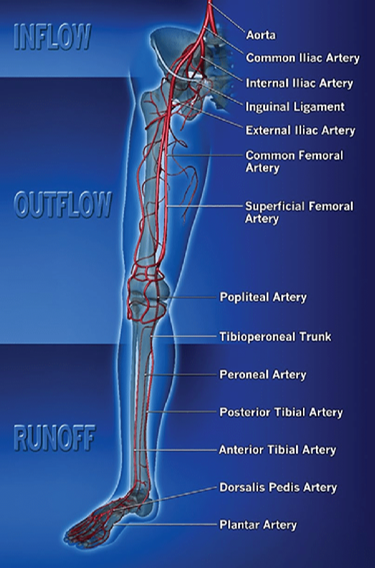
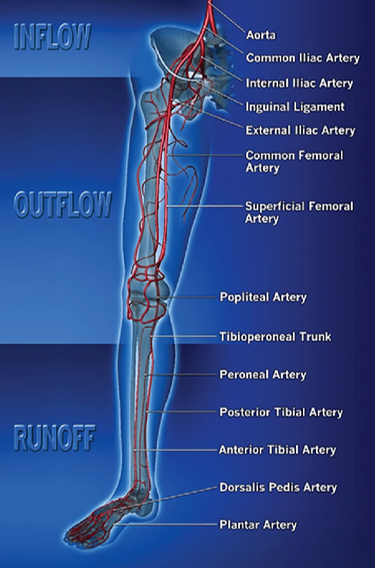
What are inflow vessels?
the more proximal (aorta-iliac) in the body
Which anatomical location is used to differentiate location of inflow & outflow?
inguinal ligament
What are outflow vessels?
vessels at the inguinal crease & below
Which vessels are considered inflow vessels?
abdominal / distal aorta
common iliac arteries
external iliac arteries
What does the abdominal aorta bifurcate into & where at?
right & left common iliac arteries
level of the umbilicus (belly button)
What does the common iliac arteries bifurcate into & where at?
internal & external iliac artery
lumbosacral junction
Which vessel descends into the pelvis & provides arterial flow to the pelvic wall, gluteal muscle, pelvic viscera, thigh & perineum?
internal iliac arteries (hypogastric)
Which vessel is a continuation of the common iliac artery that then continues to the inguinal ligament in the groin?
external iliac arteries
What branches arise off the external iliac artery?
inferior epigastric artery
deep circumflex artery
What does the inferior epigastric artery supply blood to?
abdominal muscle & skin
What does the deep circumflex artery supply blood flow to?
abdominal muscles
Which inflow vessels can anastomose (connect) to other branches as collaterals?
internal iliac arteries (hypogastric)
deep circumflex artery
Which vessels are considered outflow vessels?
common femoral artery
deep femoral (profunda femoris) artery
superficial femoral artery
popliteal artery
tibioperoneal trunk
When does the distal external iliac become the common femoral?
as it passes underneath the inguinal ligament in the groin
What does the common femoral artery bifurcate into?
superficial femoral artery & deep femoral artery
Which outflow vessel tends to develop into a collateral pathway for the lower extremity in situations of significant stenosis or occlusion?
deep femoral / profunda femoris
What is the hunters / adductors canal?
the location for where the SFA transitions into the popliteal in the distal thigh
also a common area for stenosis
Which branches supply flow to the muscles, knee joint & skin?
genicular (knee area) branches off the popliteal artery
Which vessels are considered runoff vessels?
anterior tibial artery
dorsalis pedis artery
posterior tibial artery
peroneal artery
What is the first branch off the distal popliteal artery?
anterior tibial artery
When does the anterior tibial turn into the dorsalis pedis?
in the distal segment at the level of the ankle
What branches off the dorsalis pedis artery?
first dorsal metatarsal
deep plantar artery
What vessel does the deep plantar artery connect to to complete the plantar arch of the foot?
lateral plantar artery
What does the posterior tibial artery supply?
sole of the foot
What does the peroneal artery supply?
structures in the lateral aspect of the leg
Which vessel extends down the medial side of the fibula bone?
peroneal artery
What is the most significant factor in peripheral resistance?
vessel diameter
What is the primary site peripheral resistance occurs at?
the arterioles
What is hydrostatic pressure?
force of gravity on a column of fluid
What is the atmospheric pressure considered to be at in the right atrium?
zero
When standing, where is pressure the highest?
in the lower portion of the body (ankle)
What does the peripheral arterial system use to categorize blood flow?
the phasicity of the waveform
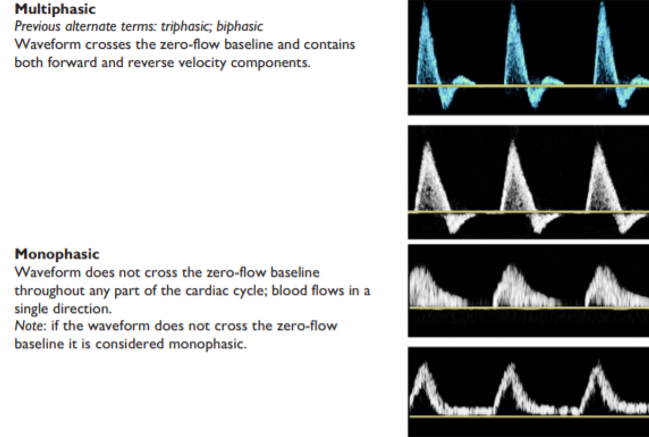
What type of waveform is seen when a normal to mild disease is present?
multiphasic
What type of waveform is seen when a significant disease is present?
monophasic
In a normal state, what resistance type should all the arteries in the peripherals be?
high resistance
What type of doppler is used for physiologic testing?
CW doppler
What type of doppler is used for duplex images?
PW doppler
How does the evolution of PAD present in the lower extremities?
claudication
ischemic rest pain
tissue loss
What are some risk factors of peripheral arterial disease (PAD)?
diabetes
hypertension
hyperlipidemia
smoking
family history
age
male gender
Which vessels are more likely to have an occlusive disease for a diabetic patient?
distal popliteal artery & tibial vessels
this is due to medial wall calcification developing in the arterial wall
Why are ulcerations, gangrenous tissue & amputations more prevalent in the diabetic population?
due to neuropathy that causes poor sensation leading to unknowing trauma of lower leg & foot
Why can hypertension be a risk factor for PAD?
exacerbates the formation of atherosclerotic plaque due to increased force of the shearing of blood at points of bifurcations
Why can hyperlipidemia be a risk factor for PAD?
elevated plasma lipids that are insoluble in water accumulate & contribute to the formation of plaque
What is claudication?
pain that occurs in the muscle while walking / exercising that subsides with rest due to inadequate blood supply to the exercising muscle
Which vessels would be suspected to be involved with buttock disease?
aorta-iliac
Which vessels would be suspected to be involved with thigh claudication?
distal external iliac
common femoral
Which vessels would be suspected to be involved with calf claudication?
femoral-popliteal
Where do symptoms typically occur with ischemic rest pain?
forefoot
heal
toes
NOT calf region
What are the acute arterial signs & symptoms?
pain (severe)
pallor (pale)
pulselessness
paresthesia
paralysis
poikilothermia (coolness)
What are some manifestations of disease?
atherosclerosis (embolism)
aneurysm
dissection (dissecting aneurysm)
pseudoaneurysm
arteritis (buerger’s)
coarctation of aorta
vasospastic disorder
entrapment
Where are aneurysms most likely in the lower extremities?
common femoral & popliteal (on slide 19)
infrarenal (below kidneys) abdominal aorta (on slide 20)
(im not sure which is the more correct one)
What is an aneurysm?
weakening of the arterial walls causing bulging or dilation
What is the difference between a true & false aneurysm?
true involves all 3 walls
false doesn’t
What is a fusiform aneurysm?
circumferential dilation of the arterial wall
What is a saccular aneurysm?
localized out-patching of the arterial wall
What is a dissecting aneurysm?
a tear in the intimal wall along with weakening of the arterial wall causing an aneurysmal dilation
Where does a dissecting aneurysm commonly occur in?
thoracic aorta
What is a pseudoaneurysm?
focal “pouch or sac” outside of the artery with high pressure blood flow due to a hole in the arterial wall
What is a pseudoaneurysm fed by?
a tract coursing directly from the main artery
What are pseudoaneurysms typically caused by?
an iatrogenic (by medical treatment) injury while trying to gain arterial access
What is a hematoma?
blood leaking into the surrounding tissue, doesn’t have a tract due to inactive flow
What is an arterial-venous connection?
abnormal connection between the vein & artery due to injury (likely from attempted access with a needle)
What is buerger’s disease also known as?
thrombongiitis obliterans
What is buerger’s disease?
a form of arteritis where the patient presents with occlusion of the distal arteries
often in males & heavy smokers
What is coarctation of the aorta?
a congenital anomaly where there is narrowing of the thoracic aorta, can result in hypertension, lower extremity ischemia, decreased pulses & pressures
What are vasospastic disorders?
occurs when the vessels in the hands & feet vasoconstrict reducing the blood flow in the giner & toes
What are some symptoms of vasospastic disorders?
skin color changes (pallor, cyanosis, & rubor)
paresthesia
What is raynaud’s phenomenon?
intermittent ischemia of the fingers & toes due to cold exposure or stress
What is the difference between primary (idiopathic) & secondary raynaud’s?
primary : ischemia due to arterial spasm in digits, may be hereditary
secondary : vasoconstriction of arterioles superimposed on fixed arterial obstruction
Which entrapment syndrome is most common?
popliteal entrapment
Why does popliteal entrapment occur?
there is compression of the popliteal artery by the medial head of the gastrocnemius muscle or fibrous bands
Why might someone’s skin turn pallor?
lack of blood supply
Why might someone’s skin turn rubor?
infection or hyperemia causing vessels to dilate or be damaged
Why might someone’s skin turn cyanotic?
concertation of deoxygenated hemoglobin
What is livedo reticularis?
purple patches (like bruises) at dorsum of foot due to dilated capillary & venule filling
How do arterial ulcers tend to present?
deep with regular borders & often located over the tibial (shin) area (bony areas)
What are trophic changes?
loss of hair, shiny skin, or a scaly appearance due to lack of blood flow
How can you use capillary filling to detect decreased arterial perfusion?
apply manual pressure to skin, upon release the skin should quickly turn from white to its original color — if the refill time is delayed it suggests an abnormality
What is dependent rubor?
blood only seems to flow to the lower extremities when lowered appearing red, instead of white when raised & lacking blood flow
What does each number on the palpation scale represent?
0 = no pulse
1+ = weak pulse
2+ = good pulse
3+ = strong pulse
4= + bounding pulse
What kind of pulse can aneurysms present with?
bounding
What are bruits?
abnormal sounds heard on auscultation
What does each number on the bruit scale represent?
1+ = mild
2+ = moderate
3+ = severe
What are bruits graded off of?
their strength & duration