Sleep Disorders
1/86
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
87 Terms
What is the restorative function theory of sleep?
The theory that the body repairs and rests during the sleep state
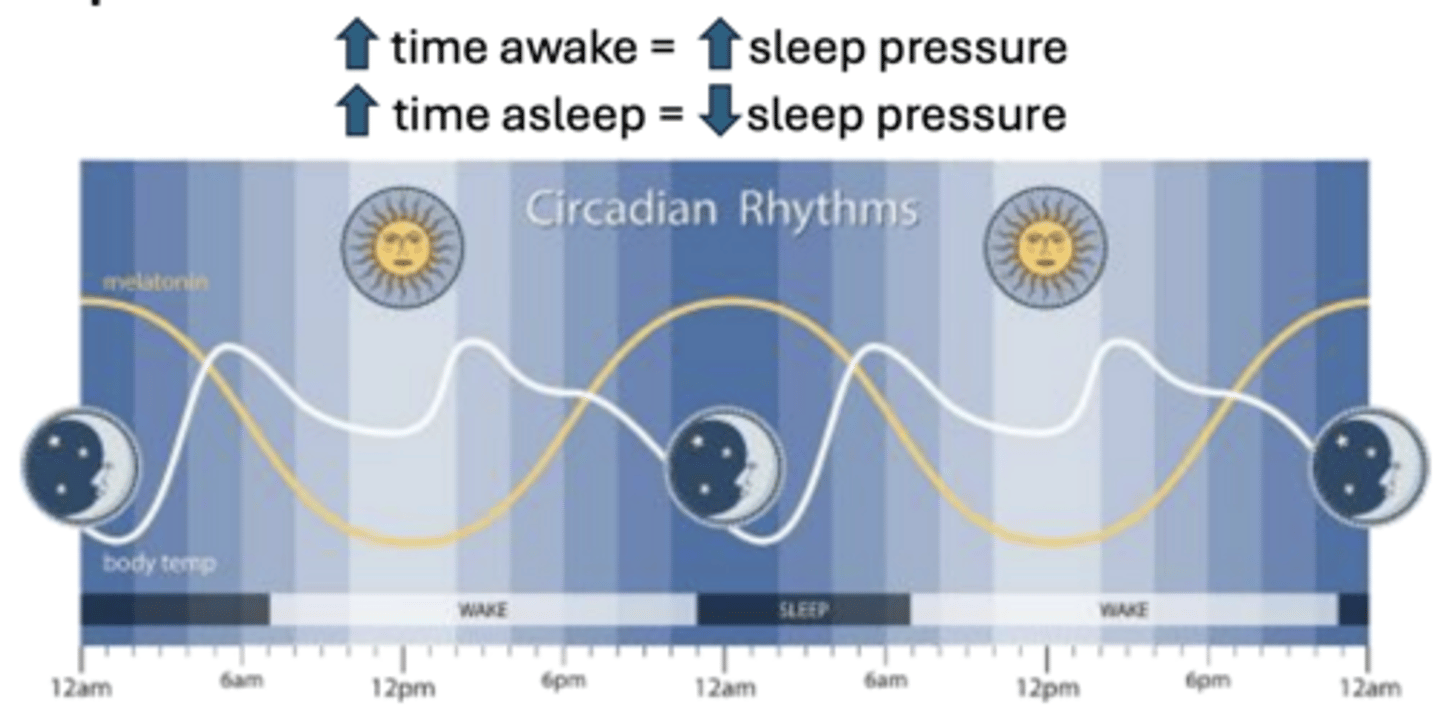
What is the relationship between time awake and sleep pressure?
Sleep pressure increases as time awake increases and decreases as time asleep increases.
What is the glymphatic system in the context of sleep?
A brain waste removal pathway that clears substances like adenosine, associated with an increase in interstitial space during sleep.
What is the function of the suprachiasmatic nucleus (SCN)?
It receives light exposure information from the eyes to control behavioral rhythms.
Which neuropeptide is synthesized in the lateral hypothalamus?
Orexin (hypocretin).
Which brain structure is responsible for directing muscle paralysis during REM sleep?
The brainstem.
What is the role of the pineal gland in sleep regulation?
It receives signals from the SCN to increase melatonin production.
Which neurotransmitters promote sleep?
GABA, Galanin, and Adenosine.
Which neurotransmitters promote wakefulness?
Histamine, Norepinephrine, Serotonin, Acetylcholine, and Orexin.
How long is a typical sleep cycle in a healthy adult?
90 to 120 minutes.
What are the different stages of normal sleep architectute?
W- wake
N1/N2- light sleep
N3- deep sleep
R- REM sleep stage
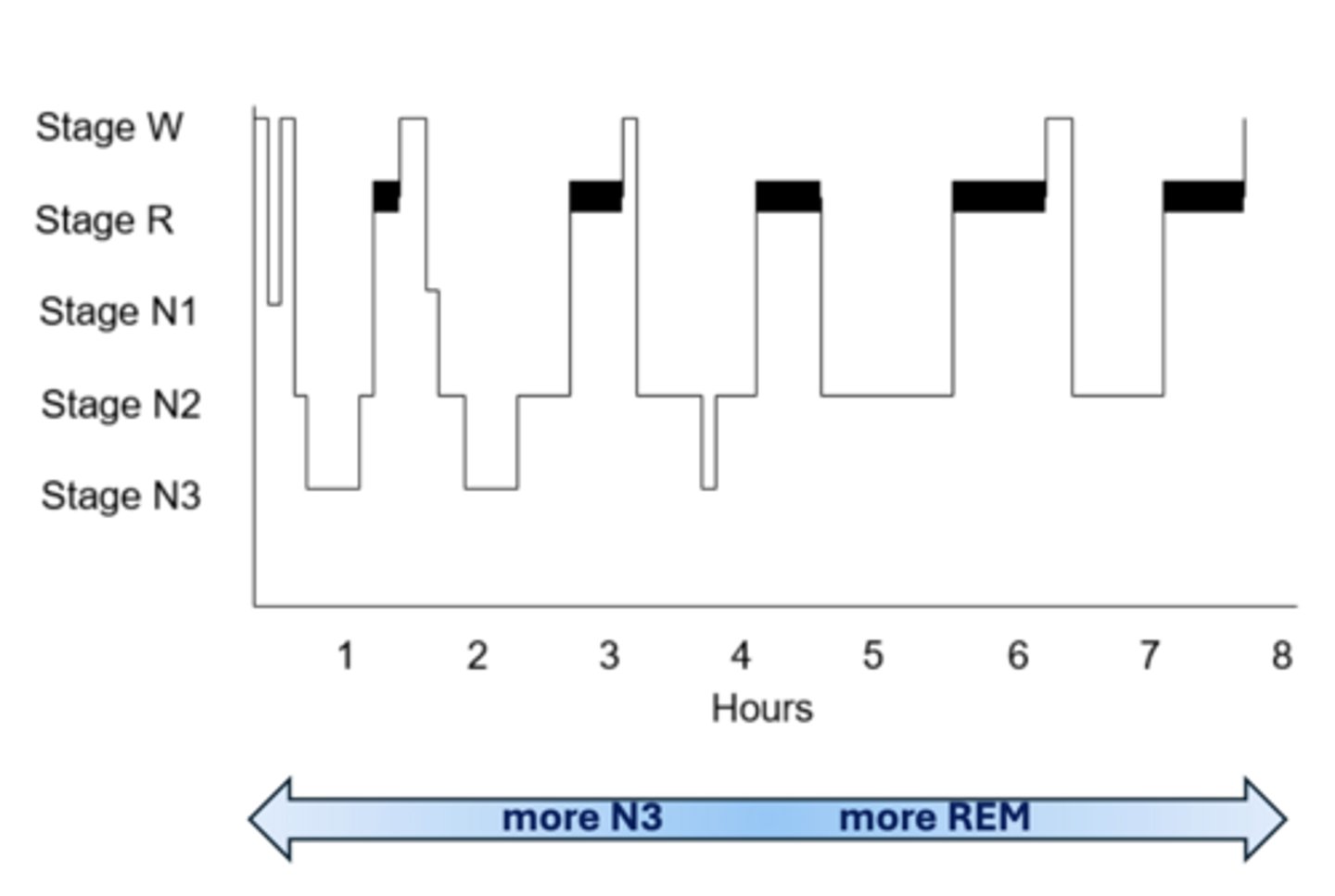
What is NREM sleep?
- N1 feels like space between awake and asleep
- N2 highest portion of our night, considered "light" sleep
- N3 is slow wave sleep
What occurs physiologically during REM sleep regarding skeletal muscles?
Skeletal muscle paralysis occurs, with the exception of eye motion control and accessory breathing muscles. Vivid dreams occur here as well
How do blood pressure and heart rate change during REM sleep compared to NREM?
They decrease during NREM but exhibit large variations during REM
What is the effect of urine flow during dsleep?
reduced and more concentrated with decreased excretion of Na, K, Cl and Ca
What happens to Growth Hormone (GH) secretion during sleep?
GH secretion increases overnight during sleep.
What are common causes of early REM onset (prior to 60 minutes)?
Sleep deprivation, depression, hypersomnia of central origin, circadian rhythm disorders, or substance/medication withdrawal.
Which substances are known to cause REM suppression?
SSRIs, stimulants, anti-epileptics, beta agonists, and alcohol.
What are examples of NREM parasomnias?
Night terrors, sleepwalking, sleep talking, confusional arousals, sleep-related eating disorder, sexsomnia, and PLM
What is REM behavior disorder?
A condition characterized by the loss of muscle atonia during REM sleep, leading to dream enactment.
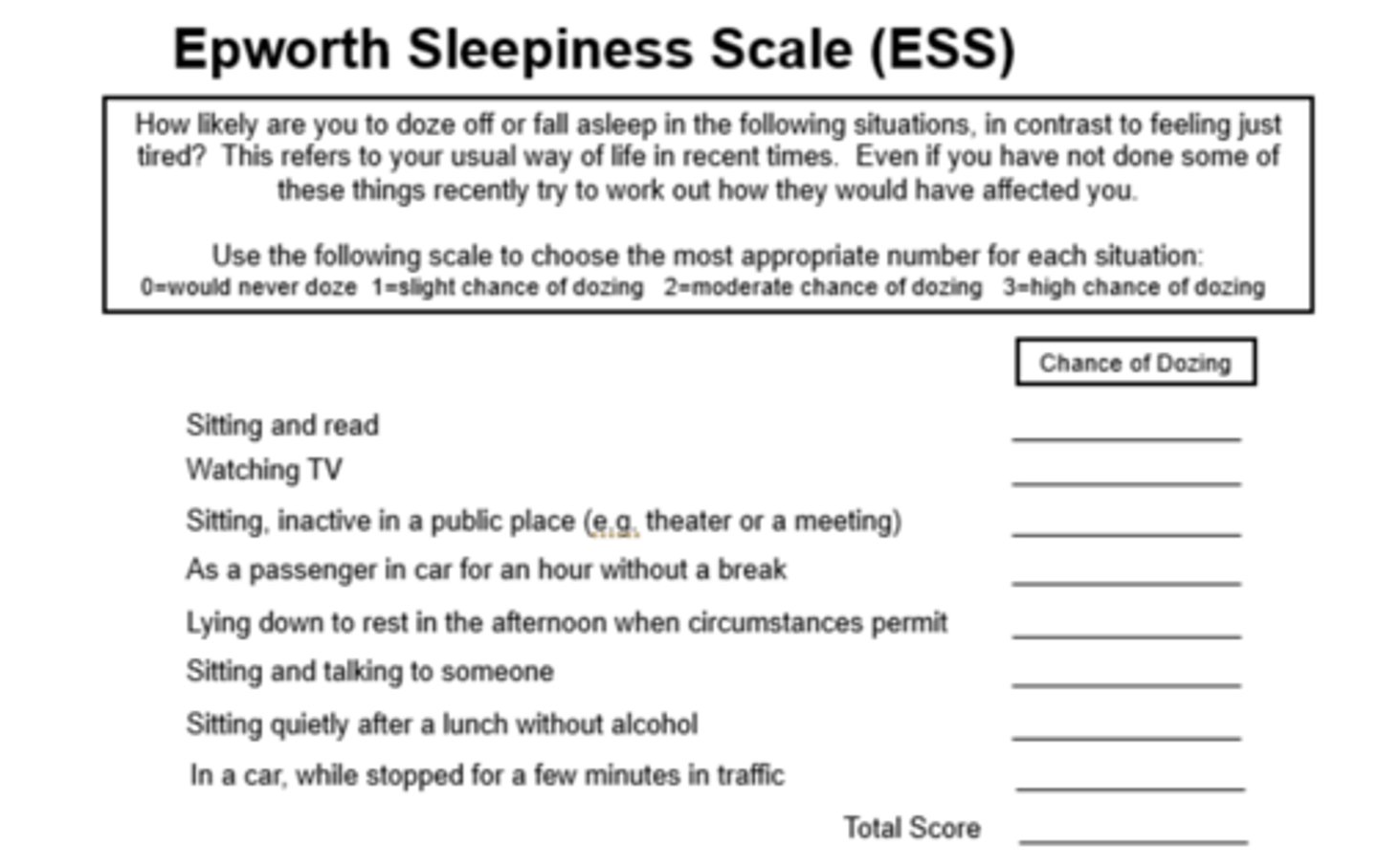
What is the Epworth Sleepiness Scale used for?
To assess daytime sleepiness in patients suspected of having a sleep disorder.
Why is it important to ask about sleep schedule?
bedtime, rise time, awakenings during night/estimated duration, consistency
Why is it important to ask about naps during a sleep history?
frequency, duration, timing, and whether they are refreshing
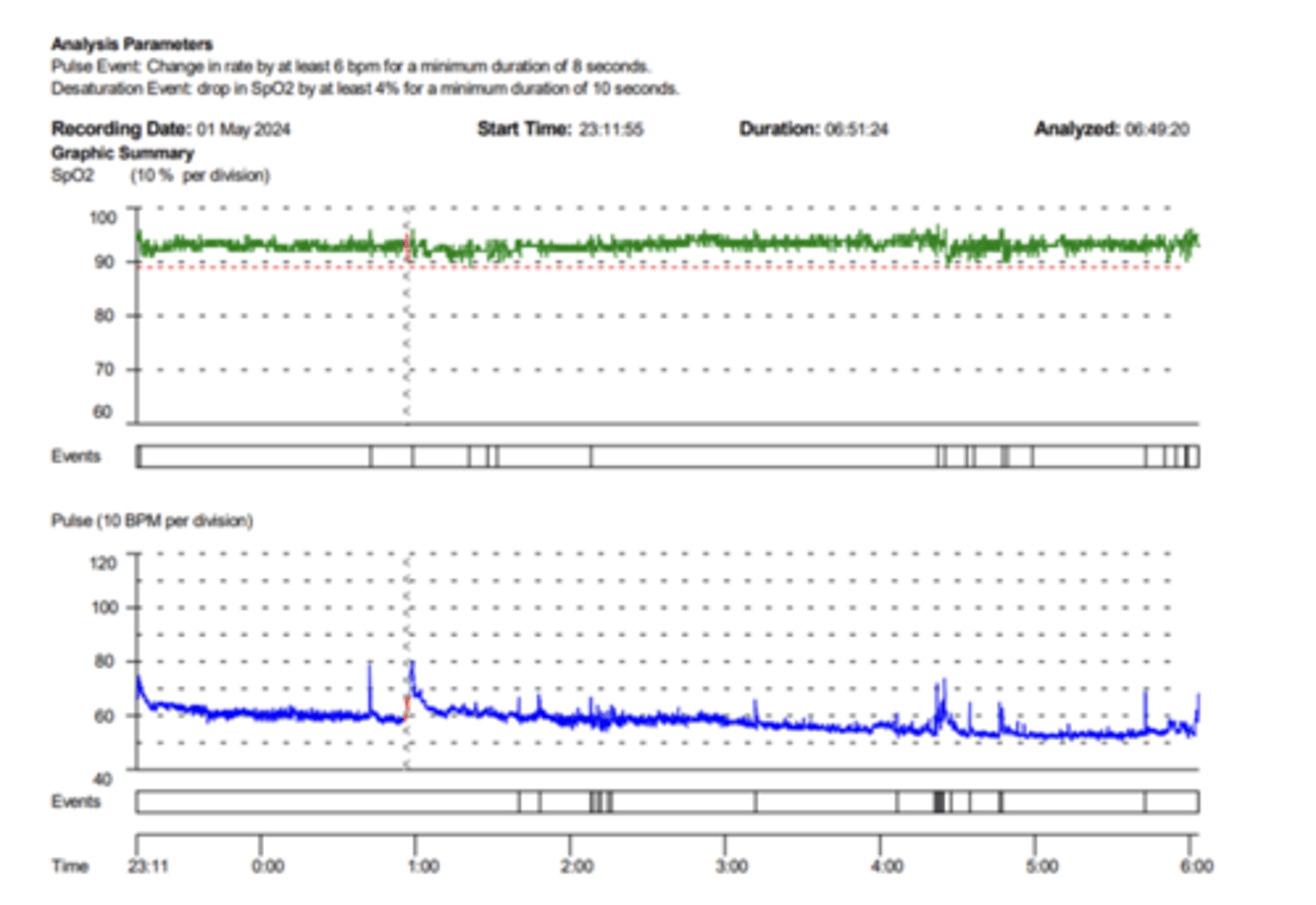
What is the primary diagnostic threshold for sleep apnea using overnight oximetry?
An oxygen desaturation index (ODI) of greater than 5 events per hour.
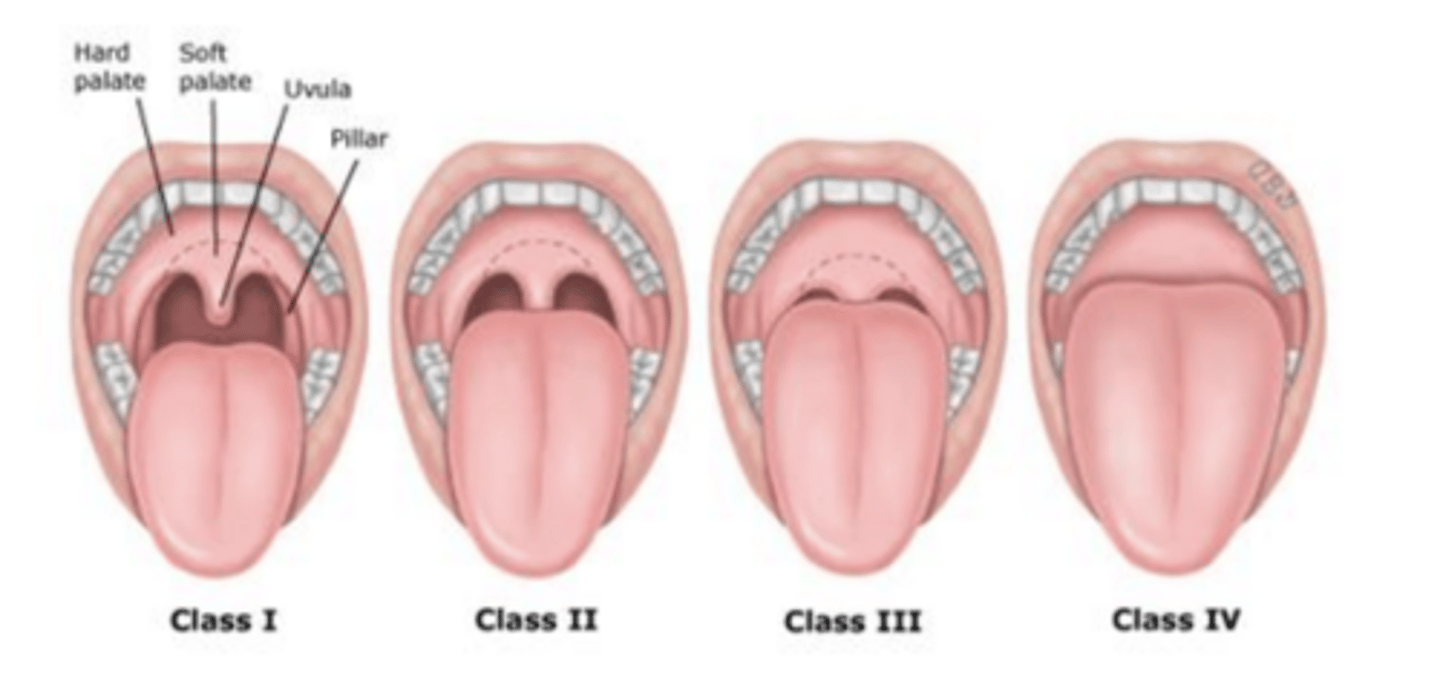
What is included in the head and neck PE?
Mallampati airway score (tongue size, presence of tonsils), neck circumference, surgical changes, and nasal patency
What is micrognathia and retrognathia?
Small chin and no room for tongue

What are the most common sleep diagnostics used?
overnight oximetry, home sleep apnea testing, and polysomnography
What diagnostics are used for hypersomnia?
Mean sleep latency testing (MSLT) and Maintenance of wakefulness testing (MWT)
What is the oxygen desaturation index (ODI)?
number of desaturation events per hour (> 5 suggestive of sleep apnea)
What are the indications and requirements for home sleep apnea testing (HSAT)?
Nearly always specific for sleep apnea and requires patient ability to apply and correctly execute the testing procedure

What are the indications for the in-lab polysomnography (PSG)?
Preferred test for parasomnia, hypoventilation, suspicion for very mild or very severe sleep apnea, movement disorders
What are the pros of PSG?
Ideal for patients unable to successfully complete home sleep study
What are the cons of PSG?
Unusual environment, often lacks personal comfort preferences
What is Multiple Sleep Latency Test (MSLT)?
Assessment of daytime sleepiness / testing required for diagnosis of narcolepsy type I or II. Consists of 4-5 strictly timed naps over course of 1 day
What MSLT result is suggestive of central hypersomnia?
A mean sleep latency of less than 8 minutes.
What MSLT finding is suggestive of narcolepsy type I or II?
Presence of REM sleep on 2 or more naps.
What is the primary goal of the Maintenance of Wakefulness Testing (MWT)?
To assess a patient's ability to remain awake during 4 sessions of intentional wakefulness (sitting up for 40 mins in a bed/recliner)
What are the risk factors of Obstructive Sleep Apnea (OSA)?
older age, obesity, narrowed airway, testosterone-based HRT, menopause, smoking, and nasal congestions
What are the three classic symptoms of OSA?
Excessive daytime sleepiness, insomnia, and snoring (or witnessed apnea/choking).
What are the comorbidities of OSA?
Resistant HTN, CAD, A-fib, CHF, CVA/TIA, Pulmonary HTN
What are the consequences of OSA?
intermittent hypoxemia w/wo hypercapnia, intrathoracic pressure, changes recurrent microarousals
What is a significant risk of untreated OSA?
Increased risk of acute CV events, arrhythmias, hypertension, CVA, sudden cardiac death (moderate to severe)
What is the Apnea hypopnea index (AHI) threshold for mild, moderate, and severe OSA?
Mild: 5-14 events/hr
Moderate: 15-29 events/hr
Severe: 30+ events/hr.
What severity of OSA is treated?
mild with symptoms and always moderated to severe (AHI 15+)
What distinguishes Upper Airway Resistance Syndrome (UARS) from OSA?
UARS involves airflow limitation due to increased respiratory effort without significant oxygen desaturation.
What is central sleep apnea?
Airflow reduces/stops along with stoppage of effort of breathing
What are the risk factors for central sleep apnea?
heart failure, CVA, A-fib, ERSD, sedating meds
What is the first-line treatment for most cases of sleep apnea?
Positive Airway Pressure (PAP) therapy.

What is Hypoglossal Nerve Stimulation?
used for moderate to severe OSA only (AHI 15+) only if PAP fails. Other criteria must be met (BMI range, favorable anatomy)
What is the only FDA-approved medication for OSA in patients with obesity?
Tirzepatide (Zepbound) indicated for moderate to severe OSA in patients with obesity
What are sleep terrors?
sudden arousal, sit up, intense fear, scream, intense autonomic activation; confusion, inconsolable, no recollection
What is sleepwalking and talking?
slow quiet walking with eyes open, often goal oriented; patient may wake spontaneously or return to bed
What are confusional arousals?
interval of excessive sleep inertia involving confusion and disorientation after waking from N3 / slow wave sleep
What is a sleep-related eating disorder (SRED)?
recurrent involuntary eating, not linked to daytime eating disturbances, often inappropriate/inedible/toxic selections
What is sleep-related abnormal sexual behavior (sexsomnia)?
abnormal sexual behaviors with lack of awareness and intention, followed by morning amnesia (partial or complete)
During which part of the night do NREM parasomnias most commonly occur?
The first third of the night (when N3 sleep is predominant).
What are the predisposing factors of parasomnias?
primarily genetic
What are the priming factors of parasomnias?
sleep deprivation, stress, medications (hypnotic drugs)
What are the precipitating factors of parasomnias?
noise, touch from bed partner, sleep disordered breathing, periodic limb movements of sleep, sleep apnea, medication (zolpidem)
What is the management for parasomnias?
manage triggers, preventative/safety strategies, educate family, consider anticipatory awakenings, CBT, and pharmacotherapy rarely needed
What is REM Behavior DIsorder (RBD)?
Loss of REM atonia often resulting in dream enactment that is "purposeful" most commonly in second half of the sleep
RBD is considered a prodromal syndrome for which class of neuropathology?
Alpha-synuclein neuropathology (e.g., Parkinson’s, Multiple System Atrophy, Lewy Body Dementia).
What are the risk factors for RBD?
Antidepressant medication, narcolepsy, PTSD, Parkinson disease, dementia w/ Lewy bodies
What is the diagnostic criteria for RBD?
repeated episodes of sleep vocalization/complex motor behavior, REM without atonia
What is the recommended pharmacological treatment for RBD?
1) Melatonin (3 mg+ at bedtime)
2) Clonazepam (0.25mg at bedtime)
What is exploding head syndrome?
Loud noise/explosive sensation in head NOT associated with significant pain occurring during transition to sleep or transition to wake during night
What is the pathophysiology of Narcolepsy Type I?
Loss of orexin neurons in the dorsolateral hypothalamus, leading to low CSF orexin-A levels.
What are the four diagnostic criteria for Narcolepsy Type I?
Excessive daytime sleepiness, presence of cataplexy, positive MSLT, and low CSF orexin-A concentration.
What is the differentiating factor of Narcolepsy Type II?
No cataplexy
What is cataplexy?
sudden onset of muscle weakness usually caused by intense emotional episodes
What constitutes a positive MSLT?
mean sleep latency of < 8 minutes AND 2+ naps containing REM sleep
What is the pharmacotherapy treatment for Narcolepsy sleepiness?
Modafinil, armodafinil, Solriamfetol, and amphetamines
What is the pharmacotherapy treatment for Narcolepsy cataplexy?
Oxyates (Xyrem) taken at bedtime and in the middle of the night, antidepressants, and Pitolisant (selective H3 receptor antagonist)
What is Idiopathic Hypersomnia (IH)?
Daily episodes of irrepressible need for sleep for at least 3 months. At least 11 hours total sleep time in 24 hour period
What is the treatment for Idiopathic Hypersomnia (IH)?
Modafinil/armodafinil, Methylphenidate, Clarithromycin • Methylphenidate, Pitolisant, Sodium oxybate
What are the risk factors of insomnia?
older age, female, family history, "light sleeper", chronic pain, substance use, psyche disorders
What is the diagnostic criteria for symptoms?
symptoms 3 times a week including problems with initiation/maintenance, daytime consequences, and deficient opportunity to sleep
What is Psychophysiological insomnia?
heightened arousal and learned sleep-preventing associations that result in complaint of insomnia
What is Idiopathic insomnia?
longstanding sleep difficulty, insidious onset during early childhood w/o discernible cause
What is Paradoxical insomnia?
complaint of severe sleep disturbance despite objective evidence of relatively normal sleep initiation and maintenance and duration
What is the first-line treatment for chronic insomnia?
Cognitive Behavioral Therapy for Insomnia (CBT-I).
What are the three core components of the 3P model of insomnia?
Predisposing factors, Precipitating factors, and Perpetuating factors.
What is 'sleep restriction therapy' in CBT-I?
Improve ratio of opportunity time versus sleep time to reduce awake time during the night. Really restricting time in bed, not sleep time
What is 'stimulus control therapy' in CBT-I?
Strengthening the bed as a cue for sleep by avoiding napping, setting a regular rise time, and exiting the bed if unable to sleep.
What is 'sleep hygiene' in CBT-I?
Avoiding naps, exercise routine and timing, avoid liquids/snack, avoid caffeine 6+ hours prior to bedtime, avoid alcohol & nicotine, ear plugs, light mask, environmental disruptors (pets)
What are the cognitive therapy aspects?
Identify and reduce thoughts and worries about sleep that interfere; shift from "trying to sleep" to "allowing sleep"
What pharmacotherapy is used for insomnia?
Non-benzo receptor agonists, benzodiazepines, melatonin receptor agonists, dual orexin receptor antagonists, antidepressants (trazodone), antihistamines, supplements