Equine: Hemic + Lymphatic IVCA Diseases
1/42
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
43 Terms
Acute Blood loss
Increased cardiac output
Anaplasmosis (Anaplasma Phagoctophilum):C.S
The clinical presentation of equine anaplasmosis can vary in severity, ranging from mild to life-threatening. The incubation period following the tick bite is typically 10 to 14 days. Common clinical signs include:
Fever: Horses often present with a high fever (>102.5°F or 39.2°C), which may be the first indication of the disease.
Lethargy and Depression: Profound lethargy is a hallmark of the disease, with affected horses appearing listless and reluctant to move.
Anorexia: Reduced or absent appetite is a common sign.
Limb Edema: Swelling in the limbs, particularly the lower extremities, may be observed. This is often linked to vasculitis and poor circulation.
Ataxia and Weakness: Some horses exhibit signs of incoordination and general muscle weakness, making ambulation difficult.
Petechiae and Ecchymosis: Due to thrombocytopenia, horses may develop pinpoint hemorrhages (petechiae) or larger areas of bruising (ecchymosis) on mucous membranes.
Icterus: A mild form of icterus or jaundice can develop due to hemolysis and hepatocellular dysfunction.
Anaplasmosis (Anaplasma Phagoctophilum):D.X
The diagnosis of equine anaplasmosis relies on a combination of clinical suspicion, hematological changes, and confirmatory testing. Key diagnostic steps include:
Blood Smear Examination: Peripheral blood smears can reveal morulae within neutrophils, which is pathognomonic for anaplasmosis. However, morulae may not be seen in every case, especially if the infection is in its early stages.
Complete Blood Count (CBC):
Thrombocytopenia: A marked decrease in platelets is a consistent finding, often resulting in clinical hemorrhage (e.g., petechiae).
Neutropenia: Low neutrophil counts are common, despite the presence of neutrophil inclusions.
Anemia: Mild, non-regenerative anemia may be seen, likely secondary to immune-mediated destruction or inflammation.
PCR (Polymerase Chain Reaction): PCR testing can identify Anaplasma phagocytophilum DNA in whole blood, providing a highly specific and sensitive method for diagnosis, especially in the acute phase of the disease.
Serology: Serological testing (e.g., indirect fluorescent antibody [IFA] test) can detect antibodies against A. phagocytophilum. However, this method is more useful in confirming chronic infection, as antibodies take 1–2 weeks to develop.
Immunohistochemistry: In some cases, immunohistochemistry of tissue samples, such as spleen or liver, may confirm the presence of A. phagocytophilum.
![<p>The diagnosis of equine anaplasmosis relies on a combination of clinical suspicion, hematological changes, and confirmatory testing. Key diagnostic steps include:</p><ol><li><p class="preFade fadeIn"><strong>Blood Smear Examination:</strong> Peripheral blood smears can reveal morulae within neutrophils, which is pathognomonic for anaplasmosis. However, morulae may not be seen in every case, especially if the infection is in its early stages.</p></li><li><p class="preFade fadeIn"><strong>Complete Blood Count (CBC):</strong></p><ul><li><p class="preFade fadeIn"><strong>Thrombocytopenia:</strong> A marked decrease in platelets is a consistent finding, often resulting in clinical hemorrhage (e.g., petechiae).</p></li><li><p class="preFade fadeIn"><strong>Neutropenia:</strong> Low neutrophil counts are common, despite the presence of neutrophil inclusions.</p></li><li><p class="preFade fadeIn"><strong>Anemia:</strong> Mild, non-regenerative anemia may be seen, likely secondary to immune-mediated destruction or inflammation.</p></li></ul></li><li><p class="preFade fadeIn"><strong>PCR (Polymerase Chain Reaction):</strong> PCR testing can identify <em>Anaplasma phagocytophilum</em> DNA in whole blood, providing a highly specific and sensitive method for diagnosis, especially in the acute phase of the disease.</p></li><li><p class="preFade fadeIn"><strong>Serology:</strong> Serological testing (e.g., indirect fluorescent antibody [IFA] test) can detect antibodies against <em>A. phagocytophilum</em>. However, this method is more useful in confirming chronic infection, as antibodies take 1–2 weeks to develop.</p></li><li><p class="preFade fadeIn"><strong>Immunohistochemistry:</strong> In some cases, immunohistochemistry of tissue samples, such as spleen or liver, may confirm the presence of <em>A. phagocytophilum</em>.</p></li></ol><p></p>](https://assets.knowt.com/user-attachments/3a161169-d244-4027-8aa0-3f606feb9d62.jpg)
Anaplasmosis (Anaplasma Phagoctophilum):T.X
Prompt treatment is crucial to prevent progression to severe disease, especially in horses with intense fever or signs of hemorrhage. The cornerstone of therapy is antibiotic administration:
Tetracyclines:
Oxytetracycline: Administered intravenously at 6.6 mg/kg every 24 hours for 5–7 days, this is the first-line treatment for equine anaplasmosis.
Doxycycline: If intravenous administration is not feasible, doxycycline can be given orally at 10 mg/kg twice daily for 10–14 days. This is often used as a follow-up to IV oxytetracycline or as the primary treatment for milder cases.
Supportive Care:
Non-Steroidal Anti-Inflammatory Drugs (NSAIDs): NSAIDs such as flunixin meglumine (Banamine®) or phenylbutazone can help reduce fever and inflammation.
Fluid Therapy: Horses with severe dehydration or shock may require IV fluid therapy to maintain electrolyte balance and hydration.
Monitoring: Horses should be closely monitored for worsening thrombocytopenia, coagulopathies, or secondary infections.
Prognosis: The prognosis for equine anaplasmosis is generally excellent when treatment is initiated early. Most horses respond within 24–48 hours after starting tetracycline therapy. In more severe cases involving complications such as ataxia, the recovery may be slower, but long-term outcomes are favorable if treatment is prompt.
Hallmark Clinical Signs and Diagnosis
The hallmark signs of equine anaplasmosis include fever, thrombocytopenia, and the presence of morulae in neutrophils on a blood smear. Rapid diagnosis using blood smear evaluation or PCR is critical in ensuring a timely intervention, as delayed treatment may lead to complications like disseminated intravascular coagulation (DIC) or prolonged recovery due to hematological abnormalities.
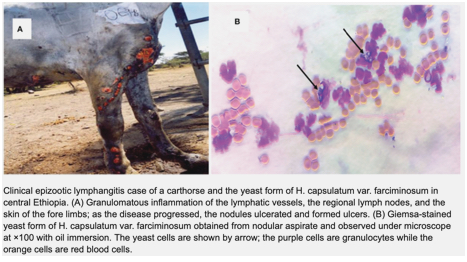
Epizootic Lymphangitis (Histoplasma Farciminosum):C.S
Clinical Signs The hallmark clinical sign of epizootic lymphangitis is the development of firm, painful nodules along the lymphatic vessels, typically progressing to ulceration and purulent discharge. The most commonly affected regions are the limbs, neck, chest, and head, although the disease can involve any part of the body where the lymphatic vessels are prominent.
Classic clinical signs include:
Nodular lesions along lymphatic vessels
Ulceration of nodules, with thick, creamy pus
Swelling of affected limbs, leading to lameness
Regional lymphadenitis
Weight loss and progressive weakness in chronic cases
Fever may occur during acute exacerbations
The disease often presents in a chronic, relapsing manner, with periods of exacerbation followed by partial remission.
Epizootic Lymphangitis (Histoplasma Farciminosum):D.X
Diagnosis Diagnosing epizootic lymphangitis involves a combination of clinical, cytological, and microbiological approaches:
Clinical examination: Based on the characteristic nodular lesions and ulcerative lymphangitis, a presumptive diagnosis can often be made. The chronicity and geographic location also aid in clinical suspicion.
Cytology and histopathology: Aspiration of the nodules or exudate typically reveals yeast forms of Histoplasma capsulatum var. farciminosum within macrophages. The organism appears as small, oval yeast cells surrounded by a clear halo (the fungal capsule). Special stains such as Periodic Acid-Schiff (PAS) or Gomori methenamine silver (GMS) can enhance visibility of the fungal organisms.
Fungal culture: Isolation of Histoplasma capsulatum var. farciminosum from the exudate or tissue samples can confirm the diagnosis. The organism grows as a mold at 25°C and converts to the yeast form at body temperature (37°C). Fungal culture is definitive but can take several weeks.
Serology: Several serological tests, such as agar gel immunodiffusion (AGID) or enzyme-linked immunosorbent assays (ELISA), may aid in diagnosis, particularly in endemic areas.
PCR testing: Molecular diagnostics, such as polymerase chain reaction (PCR), can detect the fungal DNA and provide a more rapid diagnosis, though availability may be limited.
Differential Diagnosis Given the similarities in clinical presentation, the following conditions should be considered in the differential diagnosis:
Glanders: Caused by Burkholderia mallei, glanders presents with nodular lymphangitis but has a bacterial etiology.
Sporotrichosis: A fungal infection caused by Sporothrix schenckii, which also causes nodular lesions along lymphatics.
Ulcerative lymphangitis: Other bacterial infections, such as Corynebacterium pseudotuberculosis, can cause ulcerative lymphangitis with similar clinical signs.
Sarcoidosis: Though less common, sarcoidosis can present with nodular skin lesions.
Cutaneous leishmaniasis: This parasitic infection can cause nodular skin lesions in endemic areas.
Epizootic Lymphangitis (Histoplasma Farciminosum):T.X
Treatment Treatment of epizootic lymphangitis is challenging, particularly in chronic cases, and often requires long-term therapy:
Antifungal therapy:
Itraconazole (3-5 mg/kg/day PO) is the treatment of choice for systemic fungal infections in horses. Treatment is often prolonged (several months), and relapses can occur if therapy is discontinued prematurely.
Sodium iodide IV can be used as an adjunct treatment, administered weekly for several weeks. It has shown some efficacy in reducing clinical signs, though the mechanism is unclear.
Surgical intervention: In some cases, surgical excision or curettage of the nodules may be necessary to reduce the fungal load. Surgical drainage of large abscesses can provide symptomatic relief.
Supportive care: This may include anti-inflammatory drugs, nutritional support, and care of ulcerated lesions to prevent secondary bacterial infection.
Environmental control: Reducing environmental contamination, improving hygiene, and controlling insect vectors are crucial to prevent further spread of the disease.
Isolation: Infected horses should be isolated from healthy animals to prevent direct transmission.
Equine Infectious Anemia:C.S
Lifelong infection
Clinical Signs: EIA presents with three clinical stages: acute, chronic, and inapparent carriers.
Acute stage: Fever, depression, and weakness are the hallmark signs. The horse may exhibit petechiation on mucous membranes, edema, and thrombocytopenia.
Chronic stage: Horses may suffer recurring bouts of fever, weight loss, edema (ventral), anemia, and lethargy. These horses are often called “swampers” due to their persistent but fluctuating clinical signs. The term "swampers" likely arose because these horses appear to be chronically unwell and can look run-down or in poor condition, similar to someone struggling through a swamp—persistently sluggish and worn down. Their signs may not be as acute or severe as in the initial stages of the disease, but they suffer from chronic, low-grade illness that can flare up intermittently.
Inapparent carrier stage: Horses show no outward clinical signs but still harbor the virus and pose a risk of transmission.
Other signs may include tachycardia, icterus, and occasional hematuria, particularly in severe cases. The disease often fluctuates in its presentation, leading to varying degrees of illness over time.
Equine Infectious Anemia:D.X
Diagnostics: The gold standard diagnostic test for EIA is the Coggins test, an agar gel immunodiffusion (AGID) assay that detects antibodies to EIAV. This test is widely used and mandated by law in many countries for horses crossing state or country borders or participating in events.
Other diagnostic methods include:
ELISA (Enzyme-Linked Immunosorbent Assay): This test is faster than the Coggins test and can provide results within a few hours, but it is generally used as a screening tool. Positive ELISA results must be confirmed by a Coggins test.
Polymerase Chain Reaction (PCR): This can detect viral RNA in the blood and is particularly useful in detecting acute infections before the horse mounts an antibody response. However, PCR is less commonly used due to its higher cost and complexity.
Hallmark Clinical Signs and Diagnosis:
Fever and anemia: Recurrent fever spikes and progressive anemia are classic signs of EIA. Horses may display pallor of the mucous membranes, weakness, and exercise intolerance.
Thrombocytopenia: This is one of the earliest detectable hematologic abnormalities, often seen in the acute stage. Petechiae on the mucous membranes may be present.
Chronic weight loss: Chronic infection leads to wasting, edema, and intermittent fever, especially in horses that progress to the chronic stage.
Definitive diagnosis is made via the Coggins test, which remains the legal and practical standard for EIA diagnosis.
Equine Infectious Anemia:T.X
Treatment: Unfortunately, there is no cure for EIA. Horses that test positive must be permanently quarantined at least 200 yards away from other equids or euthanized. Supportive care, including anti-inflammatory medications and management of clinical signs such as fever or anemia, may be provided, but these treatments do not affect the underlying viral infection. Prevention is key in managing the spread of EIA.
Equine Infectious Anemia: Prevention
Prevention and Control: Preventing EIA requires a multifaceted approach:
Regular testing: Routine Coggins testing is essential, particularly for horses that travel or are introduced into new herds. Testing should be conducted annually, or as required by local regulations.
Vector control: Reducing the population of biting insects, particularly in areas with high horse populations, is crucial. This includes using fly repellents, maintaining clean, dry pastures, and reducing standing water where flies breed.
Isolation of positive horses: Horses that test positive should be immediately isolated to prevent transmission to other horses. Many countries have strict laws regarding the quarantine or euthanasia of positive animals.
Sterile equipment: Ensuring all veterinary equipment, particularly needles and syringes, is used only once per animal and properly sterilized can reduce the risk of iatrogenic transmission.
Equine Viral Arteritis:C.S
The clinical presentation of EVA is highly variable, ranging from asymptomatic cases to severe systemic illness. Common clinical signs of EVA include:
Fever: One of the earliest and most consistent signs, with body temperatures often exceeding 39.5°C (103°F).
Edema: This commonly affects the limbs, ventral abdomen, prepuce, and scrotum in stallions. Edema results from increased vascular permeability due to vasculitis.
Conjunctivitis: A hallmark sign of EVA, often referred to as “pink eye,” presenting with ocular discharge.
Nasal discharge: Initially serous but can become mucopurulent as the disease progresses.
Respiratory distress: Coughing, dyspnea, and nasal discharge are more prevalent in severe cases.
Urticaria: Raised patches of skin can occur as part of a hypersensitivity reaction secondary to vasculitis.
Abortion: Pregnant mares infected with EVA may abort, usually between 3 to 10 months of gestation. Abortions may occur without prior clinical signs of illness in the mare.
Stallion infertility: Persistent infection in the reproductive tract of stallions can lead to reduced fertility or subfertility.
Weak foals: Foals born to infected mares may be weak, underweight, or stillborn.
Equine Viral Arteritis:D.X
Virus Isolation: The gold standard for diagnosing EVA involves isolating EAV from respiratory secretions (nasal swabs), semen, or fetal tissues in abortion cases. The virus can be grown in cell culture.
PCR (Polymerase Chain Reaction): PCR is commonly used to detect EAV genetic material in nasal secretions, semen, blood, or tissue samples. This method is highly sensitive and allows for rapid identification of the virus, even in cases with low viral loads.
Serology: Paired serum samples collected two to four weeks apart can be used to detect a rising antibody titer, indicating recent infection. The most common serologic tests are the virus neutralization test (VNT) and enzyme-linked immunosorbent assay (ELISA). A single positive titer may indicate prior infection, vaccination, or persistent infection in stallions.
Histopathology: Examination of tissues from aborted fetuses can reveal the typical lesions associated with EVA, including necrotizing arteritis and lymphocytic infiltration of blood vessels.
Testicular Biopsy: In persistently infected stallions, biopsy of the reproductive tract can help identify viral localization in accessory sex glands.
Equine Viral Arteritis:T.X
Supportive Care: Treatment of EVA is largely supportive, as there are no specific antiviral therapies available for this disease. Non-steroidal anti-inflammatory drugs (NSAIDs) can help reduce fever and alleviate pain. Horses with respiratory distress may require oxygen supplementation and bronchodilators.
Antibiotics: Although EVA is viral, antibiotics may be administered to manage or prevent secondary bacterial infections, particularly in cases of respiratory involvement.
Edema Management: Diuretics such as furosemide can be considered to help reduce severe edema, although their efficacy is limited in cases of profound vasculitis.
Breeding Stallions: Stallions that are persistently infected with EAV should not be used for breeding unless their semen is treated to inactivate the virus. It is important to note that castration of infected stallions can stop viral shedding, as the virus localizes in the reproductive tissues.
Abortion Management: For pregnant mares that abort due to EVA, supportive care and uterine treatment may be necessary to prevent secondary uterine infections.
Prevention: Vaccination
Failure of Passive Transfer: C.S
Failure of Passive Transfer (FPT) in horses occurs when a foal does not receive an adequate amount of immunoglobulins (IgG) from the mare's colostrum within the first 12-24 hours of life
FPT itself is not immediately associated with clinical signs but predisposes the foal to a variety of secondary infections and complications. These may manifest as:
Septicemia: This is the most common and life-threatening complication. Foals may exhibit lethargy, fever, or hypothermia, decreased suckling, tachycardia, and tachypnea. Petechiation or mucous membrane abnormalities are often seen with sepsis.
Pneumonia: Foals with FPT are at higher risk for bacterial infections such as pneumonia, which presents with increased respiratory rate, nasal discharge, or coughing.
Diarrhea (Enteritis): Foals may develop enteritis due to opportunistic pathogens, presenting with watery feces, dehydration, and lethargy.
Omphalophlebitis: Inflammation of the umbilical stump, often leading to infection and abscessation.
Septic Arthritis (Joint Ill): Joint infections can occur in foals with FPT, leading to lameness, heat, and swelling in the affected joints.
Failure of Passive Transfer:D.X
The diagnosis of FPT is primarily based on measuring IgG levels in the foal's serum. The following diagnostic approaches are commonly used:
Serum IgG Levels:
ELISA-based Snap Tests: A semi-quantitative test performed stall-side, giving a rapid assessment of IgG levels. Foals with levels <400 mg/dL are considered to have complete FPT, while levels between 400-800 mg/dL indicate partial FPT.
Radial Immunodiffusion (RID): This is the gold standard for measuring serum IgG, but results take longer (24-48 hours) compared to snap tests. It provides a more accurate and quantitative measurement.
Refractometry: Total protein refractometers can give an indirect estimate of IgG levels, although it’s less reliable compared to direct IgG measurement.
Complete Blood Count (CBC) and Fibrinogen: Signs of infection (elevated white blood cell count, fibrinogen, or neutrophilia) can indicate secondary complications like sepsis.
Blood Culture: In cases where septicemia is suspected, a blood culture is useful to identify bacterial pathogens and guide antibiotic therapy.
Physical Exam: A thorough examination, including assessment of the umbilicus, joints, respiratory, and gastrointestinal systems, should be conducted in foals with suspected FPT to rule out complications.
A colostrometer is a tool used to measure the quality of colostrum, the first milk produced by a mare after foaling. It measures the specific gravity (density) of colostrum, which correlates with the concentration of antibodies (immunoglobulins) critical for passive transfer of immunity to the foal. If the colostrum has a low antibody concentration (indicated by a low specific gravity on the colostrometer), the foal is at risk for failure of passive transfer (FPT), which can lead to increased susceptibility to infections.
Good quality colostrum: Specific gravity >1.060, indicating a high antibody concentration.
Moderate quality colostrum: Specific gravity between 1.050 and 1.060.
Poor quality colostrum: Specific gravity <1.050, indicating low antibody levels and a risk for failure of passive transfer (FPT).
Failure of Passive Transfer:T.X
Treatment for FPT depends on the age of the foal and the degree of passive transfer failure.
Oral Colostrum (if <12 hours old): For foals less than 12 hours of age that have not yet absorbed colostrum, fresh or frozen colostrum can still be administered orally. If good-quality colostrum is not available, commercial colostrum substitutes may be used.
Plasma Transfusion: Once the foal is older than 12-24 hours, intestinal absorption of IgG is no longer effective. In such cases, intravenous plasma transfusion is the primary treatment:
Fresh or Frozen Plasma: Commercially available equine plasma with high IgG concentrations can be administered intravenously. One to two liters of plasma are typically required, depending on the IgG deficiency severity.
Monitoring: Foals receiving plasma should be monitored for transfusion reactions, including fever, tachycardia, and urticaria.
Antibiotic Therapy: Given the high risk of infection, broad-spectrum antibiotics (e.g., ampicillin and gentamicin) are commonly administered to prevent or treat septicemia, particularly in foals with severe FPT (<400 mg/dL IgG).
Supportive Care: Foals with FPT and concurrent infections may require intensive supportive care, including IV fluids, nutritional support (e.g., tube feeding or parenteral nutrition), and non-steroidal anti-inflammatory drugs (NSAIDs) to manage fever and inflammation.
Immune Deficiency Syndrome: Types
SCID (severe combined immunodeficiency) is the most well-known immune deficiency syndrome in horses, particularly in Arabians. It is caused by a genetic defect in the DNA-dependent protein kinase (DNA-PK) enzyme, which is crucial for V(D)J recombination, a process necessary for the development of functional B and T lymphocytes. Individuals with SCID have defects in both the T cells and B cells, which are critical components of the adaptive immune system. As a result, foals with SCID lack functional adaptive immunity.
It is characterized by recurrent infections beginning at around 2-3 months of age due to the lack of functional B and T cells, leading to profound lymphopenia and hypogammaglobulinemia. The hallmark feature is the mutation in the DNA-PK gene, crucial for V(D)J recombination, which is pathognomonic for SCID.
CVID (common variable immunodeficiency) in horses, a condition more commonly diagnosed in mature adults, is marked by a gradual loss of B cells and plasma cells, leading to an inability to produce sufficient antibodies. This disorder is characterized by low levels of antibodies (immunoglobulins) and an impaired ability to produce antibodies. This leads to a weakened immune system
IgM Deficiency is another immunodeficiency condition seen in horses, characterized by low or absent levels of IgM, one of the major classes of immunoglobulins, making the horse vulnerable to infection.
Immune Deficiency Syndrome:C.S
Clinical signs of immune deficiency syndromes in horses often relate to the chronic and recurrent infections caused by a compromised immune system. Key signs include:
SCID (Severe Combined Immunodeficiency):
Foals appear normal at birth but show recurrent infections, including pneumonia, diarrhea, and sepsis, as maternal antibodies wane around 2-3 months of age. Without a functional adaptive immune system, these foals typically succumb to infection by 4 to 6 months of age. Common pathogens include Rhodococcus equi, Pseudomonas spp., and Streptococcus spp.CVID (Common Variable Immunodeficiency):
Older horses develop persistent or recurrent respiratory tract infections, chronic weight loss, and poor growth. These horses may show signs of chronic bronchitis, pneumonia, or sinusitis. Infections of the gastrointestinal system, particularly bacterial enteritis, are also common. Unlike SCID, CVID develops later in life, often in middle-aged or older horses.IgM Deficiency:
Foals and young horses with IgM deficiency are prone to recurrent respiratory infections, arthritis, and gastrointestinal disorders. These animals often exhibit a failure to thrive and may have concurrent bacterial infections, particularly in the respiratory tract.
Hallmark Clinical Signs
SCID: Recurrent infections beginning at 2-3 months of age, profound lymphopenia, and failure to respond to standard treatments for infections.
CVID: Chronic bacterial infections in adult horses, poor response to vaccination, and low serum immunoglobulin levels.
IgM Deficiency: Recurrent infections in young horses, particularly affecting the respiratory system and joints.
Immune Deficiency Syndrome:D.X
Diagnosis of immune deficiency syndromes in horses relies on a combination of clinical findings, immunological assays, genetic testing, and other diagnostic tools. The following diagnostics are commonly employed:
Complete Blood Count (CBC) and Differential:
Lymphopenia, particularly of B and T cells, is often seen in SCID foals. In IgM deficiency, there may be low or undetectable levels of IgM.Immunoglobulin Testing:
Serum IgG, IgM, and IgA levels can be measured to assess humoral immune function. In SCID, immunoglobulin levels will be low to absent after maternal antibodies wane. CVID horses may have persistently low levels of IgG and IgM.Flow Cytometry:
This is used to analyze lymphocyte populations. SCID foals will have drastically reduced B and T cells, while CVID horses may show reduced B cells but normal T cell levels.Genetic Testing:
SCID can be definitively diagnosed via a genetic test for the DNA-PK gene mutation. Carrier testing for breeding programs is also available and is a vital tool for reducing the incidence of SCID in Arabians.Post-mortem Examination:
In foals that die from SCID, histopathology typically reveals an absence of lymphoid tissues such as the thymus, spleen, and lymph nodes. The same examination may show evidence of chronic infections.
Immune Deficiency Syndrome:T.X
Treatment for immune deficiency syndromes is largely supportive, as there is no cure for genetic immune deficiencies. The goals are to prevent infections, control symptoms, and manage recurrent infections. Key treatments include:
SCID:
SCID foals are usually treated with broad-spectrum antibiotics for secondary infections and supportive care, but the prognosis is poor. Most affected foals die from overwhelming infections by 6 months of age. Bone marrow transplantation and gene therapy have been explored experimentally but are not yet viable treatment options in equine medicine.CVID:
Horses with CVID are managed with aggressive antimicrobial therapy for infections, immunoglobulin supplementation (although its efficacy is debated), and supportive care. These horses may benefit from regular vaccinations, though their response to vaccines is often poor.IgM Deficiency:
Similar to CVID, horses with IgM deficiency are treated with antibiotics and supportive care. The prognosis is variable, depending on the severity of infections.
Lymphoma
Neonatal Isoerythrolysis: Risk Factors
Multiparous mares: Mares with multiple pregnancies are at higher risk, particularly if they have previously carried a foal with incompatible blood group antigens.
Breed predispositions: Certain breeds, such as Thoroughbreds and Standardbreds, have a higher incidence of NI due to a higher prevalence of the Aa and Qa blood group antigens.
Blood group incompatibility: Foals inheriting Aa or Qa antigens from the sire that are absent in the mare are at the greatest risk.
Previous blood transfusions: Mares who have previously received blood transfusions are at risk of developing alloantibodies, increasing the likelihood of NI in future pregnancies.
Leakage of fetal RBCs during pregnancy: If there is placental damage or leakage of fetal red blood cells into the mare’s circulation during gestation, the mare may develop antibodies against the foal’s blood group antigens, sensitizing her to future pregnancies.
Neonatal Isoerythrolysis: C.S
The hallmark clinical signs of neonatal isoerythrolysis typically present within 24 to 72 hours after birth, once colostrum is absorbed and hemolysis begins. Classic signs include:
Icterus (jaundice): The breakdown of hemoglobin from destroyed RBCs results in elevated bilirubin levels, causing yellowing of the sclera, mucous membranes, and skin.
Weakness and lethargy: Anemia reduces oxygen-carrying capacity, leading to general weakness and reduced activity in the foal.
Tachycardia and tachypnea: Compensatory mechanisms for anemia may include an increased heart and respiratory rate.
Dark or reddish-brown urine (hemoglobinuria): In severe cases with intravascular hemolysis, free hemoglobin can be excreted in the urine, leading to discoloration.
Pale mucous membranes: The foal may have pale or white mucous membranes, reflecting significant anemia.
Collapse: In severe or rapidly progressing cases, the foal may become recumbent or show signs of shock due to profound anemia and hypoxia.
Neonatal Isoerythrolysis:D.X
Early recognition and diagnosis of neonatal isoerythrolysis are essential for appropriate management. The following diagnostic tests are commonly used:
Complete Blood Count (CBC):
Decreased hematocrit/PCV: A low packed cell volume (PCV) is indicative of anemia, which is often severe in NI cases.
Hemoglobinemia/hemoglobinuria: Free hemoglobin in the blood and urine may be present in cases of intravascular hemolysis.
Blood typing:
Blood typing of both the mare and foal to assess for blood group incompatibility is essential. Testing for the Aa and Qa blood groups, which are most commonly implicated in NI, is standard.
Direct Coombs’ test:
A positive Coombs’ test indicates the presence of antibodies bound to the foal’s red blood cells, confirming immune-mediated hemolysis.
Jaundice Foal Agglutination Test (JFA):
This bedside test involves mixing the mare’s colostrum with the foal’s RBCs. Agglutination (clumping) indicates incompatibility between the mare's antibodies and the foal's RBCs, supporting the diagnosis of NI.
Bilirubin levels:
Elevated serum bilirubin (both direct and indirect) indicates hemolysis and is typically seen in foals with NI due to the breakdown of hemoglobin from lysed RBCs.
Neonatal Isoerythrolysis:T.X
Blood transfusion:
In foals with severe anemia (PCV < 12-15%), a blood transfusion may be necessary. Ideally, the donor blood should be from a gelding or mare that is negative for the Aa and Qa antigens (a "universal donor"). If this is not available, washed RBCs from the foal’s dam (removing the alloantibodies) may be used for transfusion.
Colostrum management:
Prevent further ingestion of maternal colostrum: To stop the absorption of further antibodies, the foal should be muzzled and removed from the dam's udder. The foal can be fed an alternative source of colostrum, such as colostrum from a mare without the relevant alloantibodies or commercial colostrum substitutes.
Intravenous fluids:
In cases where hemolysis is severe, IV fluids may be required to support circulation and reduce the risk of hemoglobin-induced nephropathy (kidney damage due to hemoglobin deposition in the renal tubules).
Corticosteroids:
While controversial, corticosteroids may be used to reduce the immune response and slow down hemolysis. However, their use is typically reserved for severe or refractory cases due to concerns about immunosuppression and the risk of infection.
Oxygen supplementation:
Foals with severe anemia may benefit from oxygen therapy to counter the reduced oxygen-carrying capacity of their blood.
Monitoring and supportive care:
Regular monitoring of the foal’s PCV, heart rate, respiratory rate, and mucous membrane color is necessary to gauge the response to treatment. Continuous nursing care, warmth, and fluid management are essential components of supportive care.
Pigeon Fever ( Corynebacterium Pseudotuberculosis):C.S
External Abscesses
Firm + Painful swelling in pectoral region or ventral abdomen
Internal Abscesses
More subtle systemic signs
Signs of organ dysfunction @ location of abscesses
Ulcerative Lymphangitis
Pigeon Fever ( Corynebacterium Pseudotuberculosis):D.X
U/S
Culture + Sensitivity
Pleomorphic Rods
Serology: Synergistic Hemolysis inhibition
PCR*
Pigeon Fever ( Corynebacterium Pseudotuberculosis):T.X
External
Drainage
ABX: Penicillin or TMS)
NSAIDs
Internal
Long term ABX
Supportive care
U/S drainage
Piroplasmosis: What other names is this disease called
Babesiosis: Babesia caballo
Theileriosis: Theileria equi
Piroplasmosis: C.S
Fever + Anemia + Icterus
Hemoglobinuria + Edema of lower limbs + abdomen
Neuro signs : T. Equi
Weight loss + Depression
Piroplasmosis: D.X
PCR*
Blood smear
Serology
CBC: Anemia + Thrombocytopenia + regen anemia
CHEM: ^ Live enzymes + Bilirubin + Hypoglobinemia
Urine: Hemoglobinuria
Piroplasmosis: T.X
Imidocarb
Supportive Care: Fluids, Blood, NSAIDs
Oxytetracycline
Purpura Hemorrhagic: What type of sensitivity is this disease
Type II Hypersensitivity: Immune- complex
Purpura Hemorrhagic:C.S
Edema: Limb + Head + Ventral Abdomen
Petechial + ecchynotic hemorrhage
MM, Scleral, Skin
Necrosis + Skin sloughing
Fever + Depression
Lameness
Purpura Hemorrhagic:D.X
CBC: Leukocytosis, anemia, thrombocytopenia
CHEM: Hyperfibrinogenimia
Prolonged coag factors
Serology
Histopath
U/S
Purpura Hemorrhagic:T.X
Corticosteroids: Prednisolone/ Dexmethasone
ABX: Penicillin/ TMS
Supportive Care: IV Fluids, Limb bandage, Cold therapy
Plasma transfusion
Manage necrotic skin
Strangles (Streptococcus equi var. equi):C.S
Fever 3- 14 days after exposure
Purulent nasal discharge, Swelling + Pain of neck
Cough, Dysphagia, Dyspnea, Depression, Thick + Yellow abscess rupture
Can lead to:
Bastard strangles
Purpura hemorrhagica
Guttural Pouch empyema
Strangles (Streptococcus equi var. equi):D.X
PCR
Serology
Culture
U/S
Endoscopy
Strangles (Streptococcus equi var. equi):T.X
Supportive: Isolate, anti-inflam, soft feed, hot pack on LN for drainage
ABX: Controversial: For bastard, purpura, empyema
Penicillin, ceftiofur, tms
Can do a lavage
Prevention: Intranasal Vaccine
Ulcerative Lymphangitis:C.S
Severe limb sweling
Ulcers + Draining Abscesses
Stiff + Lame
Fever + Systemic Illness + Thickened Lymphatic vessels
Ulcerative Lymphangitis:D.X
Culture + Sensitivity
U/S
CBC: Leukocytosis, neutrophilia, PCR
Ulcerative Lymphangitis:T.X
ABX: Penicillin, TMS, Tetracycline or macrolides for svrl wks
NSAIDs
Wound Management
Compression Therapy
Supportive Care
SX Drainage