drug induced liver injury
1/39
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
40 Terms
things the liver does
cleans the blood, metabolizes stuff, makes coag factors + transport proteins (albumin)
transaminases
AST + ALT
proteins w/ physiologic roles to transfer amine groups w/ during gluconeogenesis
high concentrations in the liver + some other tissues
may be elevated in event of hepatocyte death (transaminitis)
alkaline phosphatase
found in many different tissues including liver
excreted through biliary tree
serum alkaline phosphatase levels may elevate in cholestatic disease
elevated GCT increases the likelihood of ^^
hyperbilirubinemia
any bilirubin value above reference range (2 or higher!)
s/sx of hyperbilirubinemia
jaundice usually develops at >2 mg/dl
scleral ictuerus
pruritis
clay colored stool
what does increased AST/ALT mean
hepatocytes are getting injured
what does increased alkaline phosphatase mean
biliary tract is slowing down
what does increased bilirubin mean
pt may be in trouble → more broad hepatic problem!
causes of liver injury
non-alc fatty liver disease
alc associated hepatitis
viral hepatitis
ischemic hepatitis
autoimmune hepatitis
hepatotoxic meds / DILI
types of DILI
direct hepatotoxins, idiosyncratic rxns, other rxns
direct hepatotoxic DILI
caused by direct hepatotoxins → induces a dose dependent liver injury
can be induced by metabolism of parent drug or its toxic metabolites
occurs rapidly after med administration
what are important drugs that can cause direct hepatotoxic DILI
acetaminophen, methotrexate
idiosyncratic rxn DILI
not dose or duration dependent
variable presentation!, thought to occur through aberrant immune rxns
may occur months after med initiation!
medications that can cause idiosyncratic rxn DILI
abx (amox-clavulanate, cephalosporins, nitrofurantoin), CNS agents, many others!
causes of other DILI
indirect hepatotoxicity
aberrations in ca+ homeostasis
carcinogens
mitochondrial injury
alteration of liver transport protein
dx of DILI
need 2 things:
other causes must be excluded!
one of these lab profiles:
AST or ALT ≥ 5x ULN
alk phos ≥ 2x ULN
tbili ≥ 2.5 mg/dl AND either ALT/AST/ alk phos elevated
INR ≥ 1.5 AND either ALT/AST/alk phos elevated
sx of DILI
can be completely asymptomatic
s/sx of hepatitis : abd pain, nausea, acholic stool, jaundice
s/sx of cholestasis : jaundice, feeling “foggy”, pruritis (itchy)
acute liver failure, coagulopathy, encephalopathy
labs for DILI presentation
hep A/B/C negative
anti-mitochondrial antibody ≤ 1:5
ceruloplasmin w/in normal range
antinuclear antibody ≤ 1:40
anti-smooth muscle antibody ≤ 1:40
which 2 labs values are different if they have drug-induced autoimmune hepatitis
should be low but if they take drug that causes this, then it can be higher!
antinuclear antibody ≤ 1:40
anti-smooth muscle antibody ≤ 1:40
what questions should be asked when assessing DILI
any new meds in the last 6 months
any new herbals/supplements in last 6 months
when did you start and when did you stop taking
what dose and what frequency
r factor calculations and values
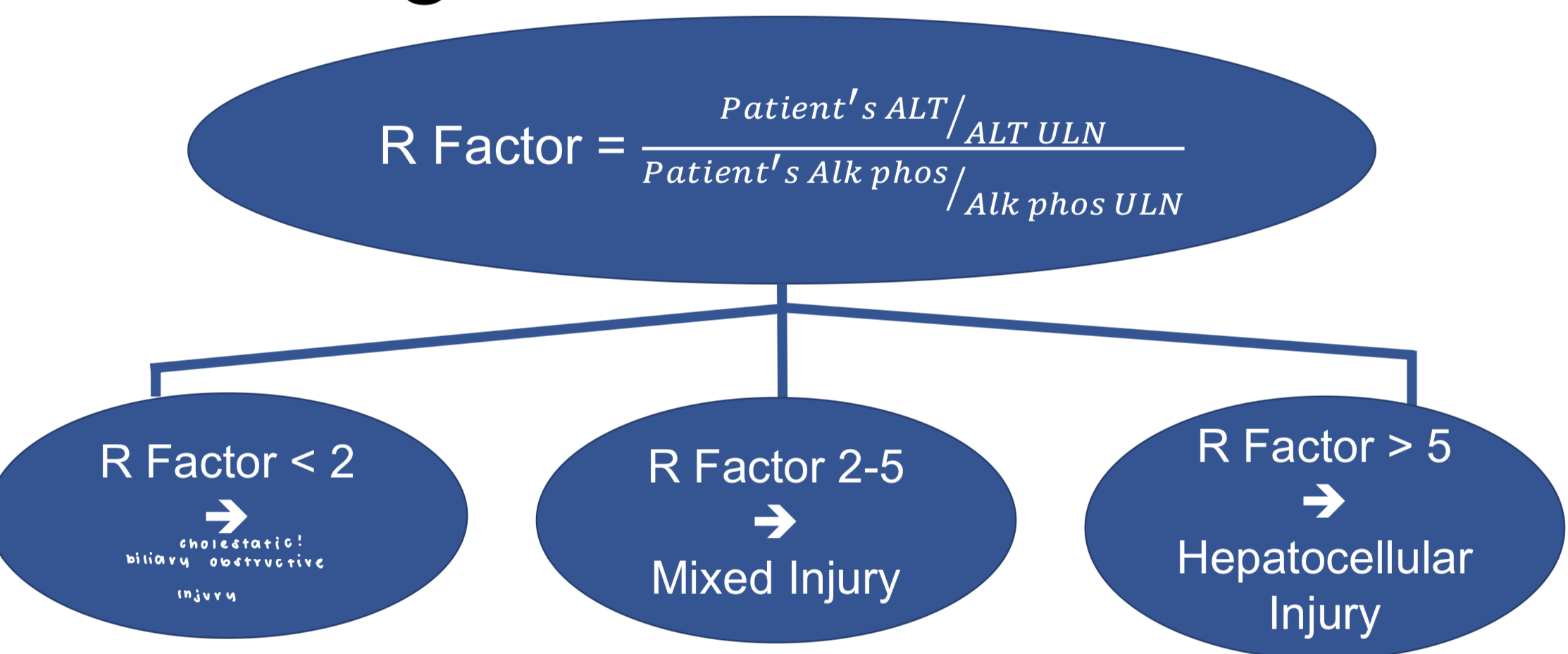
drugs that cause cholestatic DILI
erythromycin, oral contraceptives, amox-clavulanate, enalapril
drugs that cause hepatocellular DILI
acetaminophen, isoniazid, nitrofurantoin, minocycline
drugs that can cause development of drug induced auto-immune hepatitis
nitrofurantoin, minocycline
herbal/OTC supplements that can cause DILI
ashwagandha, green tea extract, garcinia cambogia, polygonum multiflorum, chinese skullcap, scutellaria baicelensis, scutellaria lateriflora, kratom, mitragyna speciosa, anabolic steroids, tumeric/curcumin
what is the main treatment for DILI w/ the drug/herb identified
discontinue the causative drug/herb and give supportive care PRN (antiemetics, antipruritics, fluids)
pruritis supportive care
throught to be d/t increases in serum bile salts
may be treated w/ cholestyramine 4g daily-bid, ursodiol (alt agent)
cholestyramine adrs + interactions
constipation, fat-soluble vitamin deficiency, increases TGs
many absorption interactions, run DDI checker!! but usually separate from other meds by ~4h
ursodiol
alternative agent form pruritis
primary use in gallstone chemodissolution
dosing of ursodiol
10-15mg/kg/d in divided doses
adrs and monitoring for ursodiol
gi distress, dizziness, enteroliths if used >30 ds
no specific monitoring recs
drug induced autoimmune hepatitis
onset, severity, + response distinct from standard autoimmune hepatitis (AIH)
usually use prednisone ~40mg daily after considerations of
biopsy + dx
disease not responding to offending drug DC
severe dx - Hys law
caution glucocorticoid adrs
APAP metabolism
acetaminophen glucuronidation + sulfation → non tox metabolites
acetaminophen CYP2E1 metabolism → toxic NAPQI + glutathione rescue → non toxic metabolites
APAP overdose tx
during APAP overdose glutathione depletion → NAPQI buildup → hepatotoxicity
use activated charcoal! or N-acetyl cysteine (NAC)!
activated charcoal
helps to adsorb APAP
indicated if presenting w/in 4 h of overdose!
1g/kg (max 50g)
contraindications: non-protected airway, gi perforation
N-acetyl cysteine (NAC)
refills hepatic cysteine stores → glutathione → rescues liver from NAPQI
indicated if:
time/concentration matrix above Rumack-Matthew nomogram line
any evidence of liver injury present
detectable acetaminophen in serum >24h after ingestion
acute APAP ingestion of 150mg/kg or 7.5g(whichever is less) & serum levels cant be obtained w/in 8h of ingestion
NAC adrs
hypersensitivity rxns, pruritis, urticaria, hypotension, N/V (po formulation only)
hypersensitivity adrs are less frequent w/ 2 bag admin method
dosing for NAC
traditional dosing: 150mg/kg/hr IV x 1h → 12.5 mg/kg/hr x 4h → 6.25 mg/kg IV x 16h
2 bag method: 50 mg/kg/hr x 4h → 6.25 mg/kg/hr x16h
PO dosing regimen infrequently used
isoniazid
common abx used in tx of tuberculosis
mech of toxicity not fully understood, may involve metabolite
baseline + monthly monitoring recommended:
sx check: anorexia, nausea, fatigue, jaundice, abdominal pain
physical exam
LFTs
statins
frequently used for ascvd risk reduction
known to cause transaminitis in some pts but true hepatic dysfxn rare!
test LFTs at baseline and as clinically indicated (for abd pain, dark urine, jaundice, fever)