DERMATOLOGY
1/99
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
100 Terms
what to ask in a dermatology history
Duration
S - (flexural or extensor surfaces / sun-exposed areas / ‘sweaty’ areas
O
C
R
A
T
E
S
previous episodes
change over time
1 2 Associated features
Itchy
Tender / pain
Bleeding
Oozing
Discharge
Swelling
2 3 Systemic features
Pyrexia
Joint pain
Weight loss
Malaise
1 Drug History and allergies
1 2 Social History
Alcohol
Smoking
Job
Living situation
3 Family history
Family history of skin disease explored
1 ICEF
Explores ideas, concerns, expectations, feelings
Asks patient if they have any questions
Social
Occupation
Exposure to chemicals
Travel history
History of atopy i.e. asthma, allergic rhinitis, eczema
1 2 Sun exposure
Burn or tan in the sun
Use of sun beds
Sunscreen use
1 Past Medical History
describing a lesion
SCAMD
- size
- colour
- associated features
- morphology
- distribution
primary vs secondary lesions
Primary- develops on previously unaltered skin
Secondary- evolves from a primary lesion (scratching or infection)
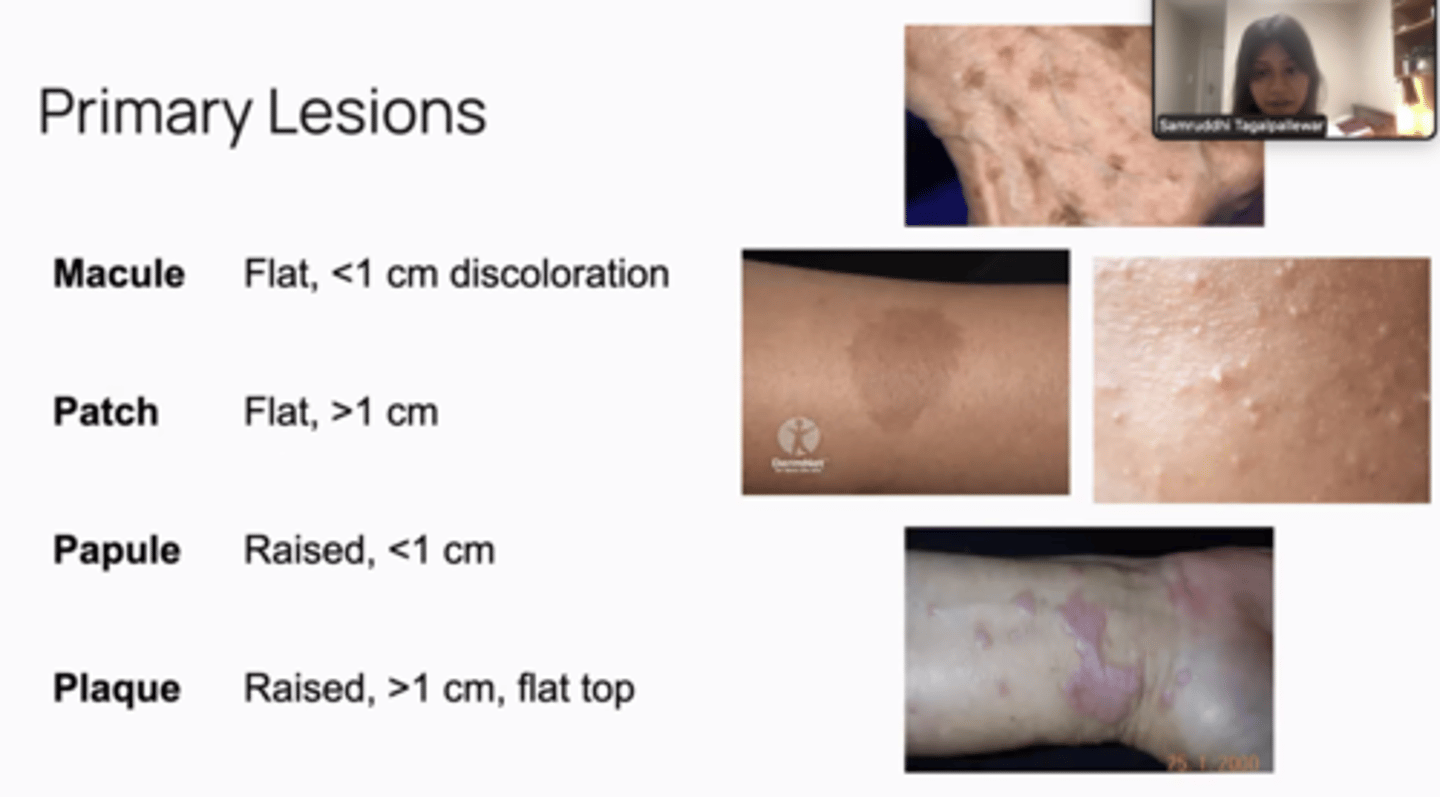
types of primary lesions
macule - flat, < 1cm
patch - flat, > 1cm
papule - raised <1cm
nodule - raised bigger lesions >1cm
vesicle - small, fluid filled (chicken pox)
bullae - large blister
pustule - pus filled
erosion - little dip in skin
ulcer - larger dip in skin
secondary lesions
- scale - flaking
- crust - dried exudate
- erosion - partial epidermal loss
- ulcer - full thickness loss
- fissure - linear crack
- scar- fibrous tissue repair
- atrophy - skin thinning
what do the dollowing terms mean
- purpuric
skin examination
Inspect in general:
- Make a general observation.
- site and number of lesions.
- If multiple, describe the pattern of distribution and configuration.
Describe the individual lesion (SCAM):
Size (the widest diameter) and Shape.
Colour.
Associated secondary change.
Morphology and Margin (border).
Palpate the individual lesion:
Assess the surface.
Check consistency, mobility, tenderness, and temperature.
Systematic check:
Examine the nails, scalp, hair, and mucous membranes.
emergency dermatology presentations
- anaphylaxis and angioedema
- Stevens-Johnson syndrome, toxic epidermal necrolysis (ten)
- acute meningococcaemia
- erythroderma
- eczema herpeticum
- necrotising fasciitis
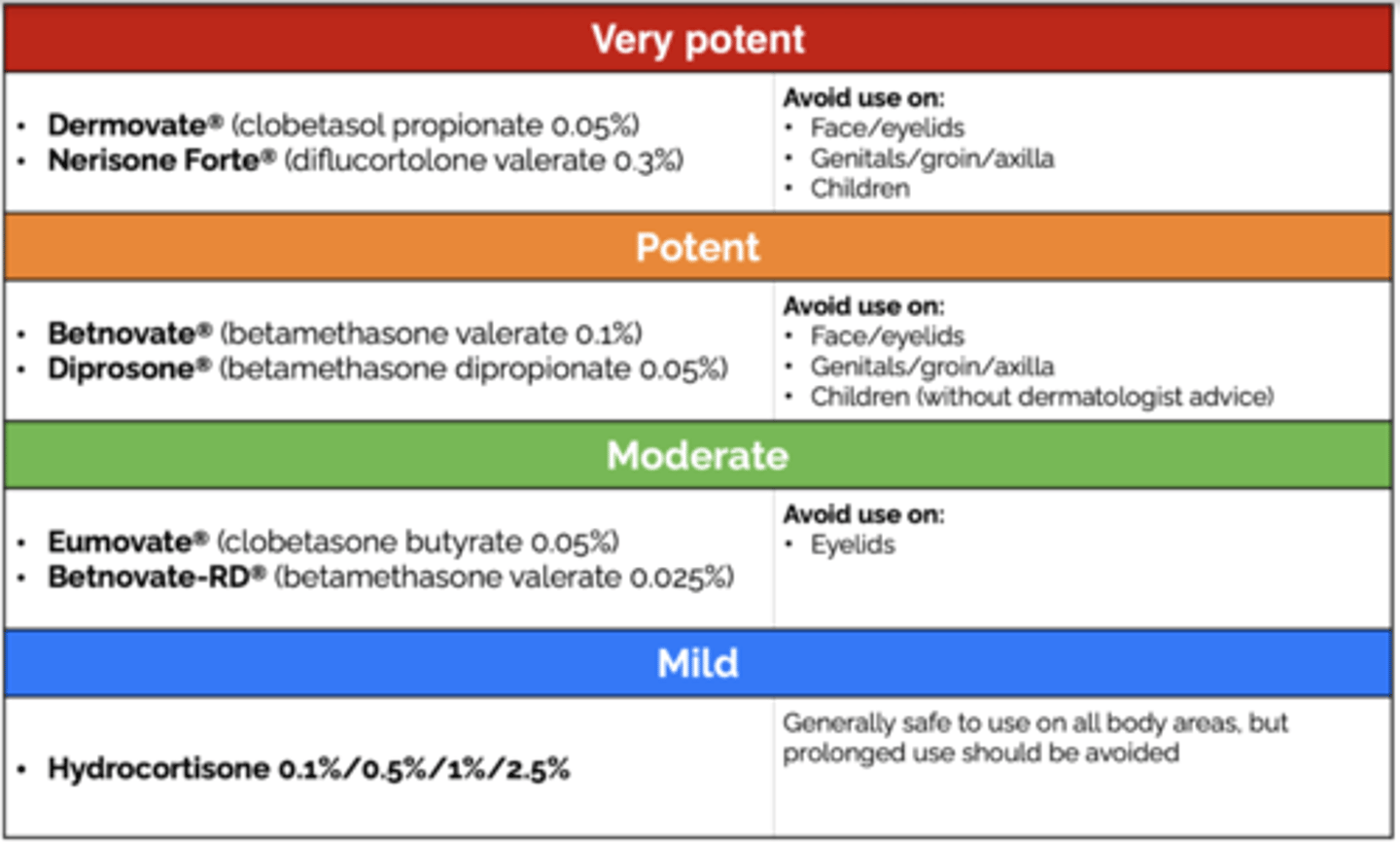
strengths of steroids
•Mild : 1% Hydrocortisone ointment
•Moderate : Clobetasone ointment (Eumovate)
•Potent : Betamethasone ointment (Betnovate), Mometasone ointment (Elocon)
•Super potent : Clobetasol ointment (Dermovate)
•Combination : Betamethasone/Fusidic acid cream (Fucibet) Miconazole/1%HC cream (Daktacort) Clobetasone/Oxytetracycline/Nystatin cream (Trimovate)
what is nikolskys sign
slight rubbing leads to exfoliation of skin
ACNE classification
mild:
- few to several papules/pustules* (<10 usually)
moderate:
- 10-40 papules/pustules
- along with *comedones
- and few to several nodules*
severe:
- numerous or extensive papules/pustules
- many nodules

ACNE management
mild:
- topical retinoids (avoid during pregnancy) e.g topical isotretinoin - stop comedones formation
- topical benzoyl peroxide (drying agent)
(combination of retinoid + benzoyl peroxide = epiduo)
if that doesn't work:
- topical antibiotic + oral antibiotic (e.g azelaic acid + tetracycline)
- COCP
severe:
- systemic antibiotics
- refer to dermatology (for oral retinoids e.g isotretinoin)
ACNE complications
- Post-inflammatory erythema
- Post-inflammatory hyper- and hypo- pigmentation
- Psycho/social/sexual dysfunction
- Scars (atrophic, hypertrophic, keloid)
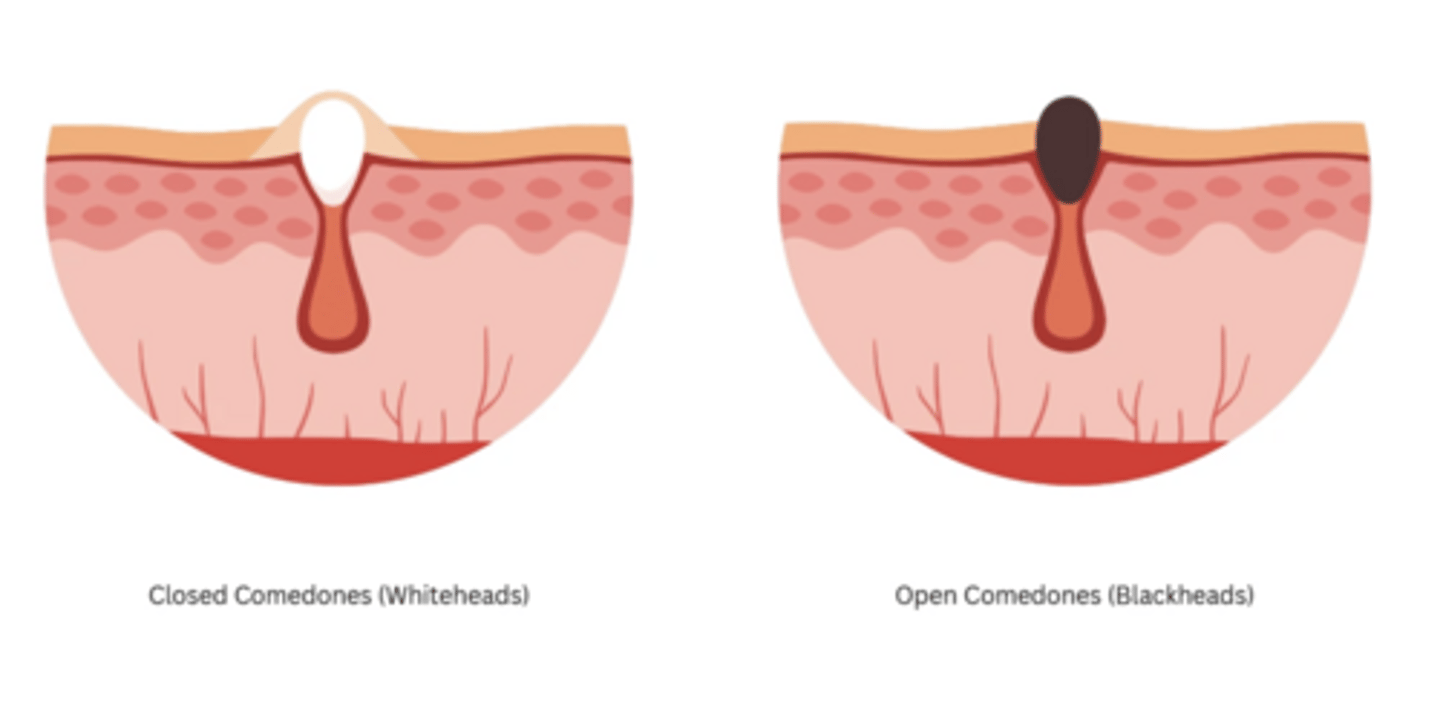
ACNE what are open and closed comedones
isotretinoin - what should be the contraception advice?
Isotretinoin is highly teratogenic
Two methods (e.g., oral contraceptive + condom) is recommend
ACTINIC KERATOSIS definition
Actinic keratosis, also known as solar keratosis, is a premalignant skin condition

ACTINIC KERATOSIS management
The management of actinic keratoses aims to prevent development into SCC.
For localised lesions,
- cryotherapy,
- curettage,
- surgical excision.
Larger or multiple lesions
topical therapies:
- 5-Fluorouracil (a cytotoxic agent)
- NSAIDs
- Imiquimod (an immune response modifier)
Patient education on sun-protective measures
ALOPECIA classification
SCARRING
destruction of the underlying hair follicle = irreversible.
e.g burns, injury, infections
NON-SCARRING
the hair follicle is intact = potentially reversible.
e.g hypothyroidism, physiological stress, male pattern baldness
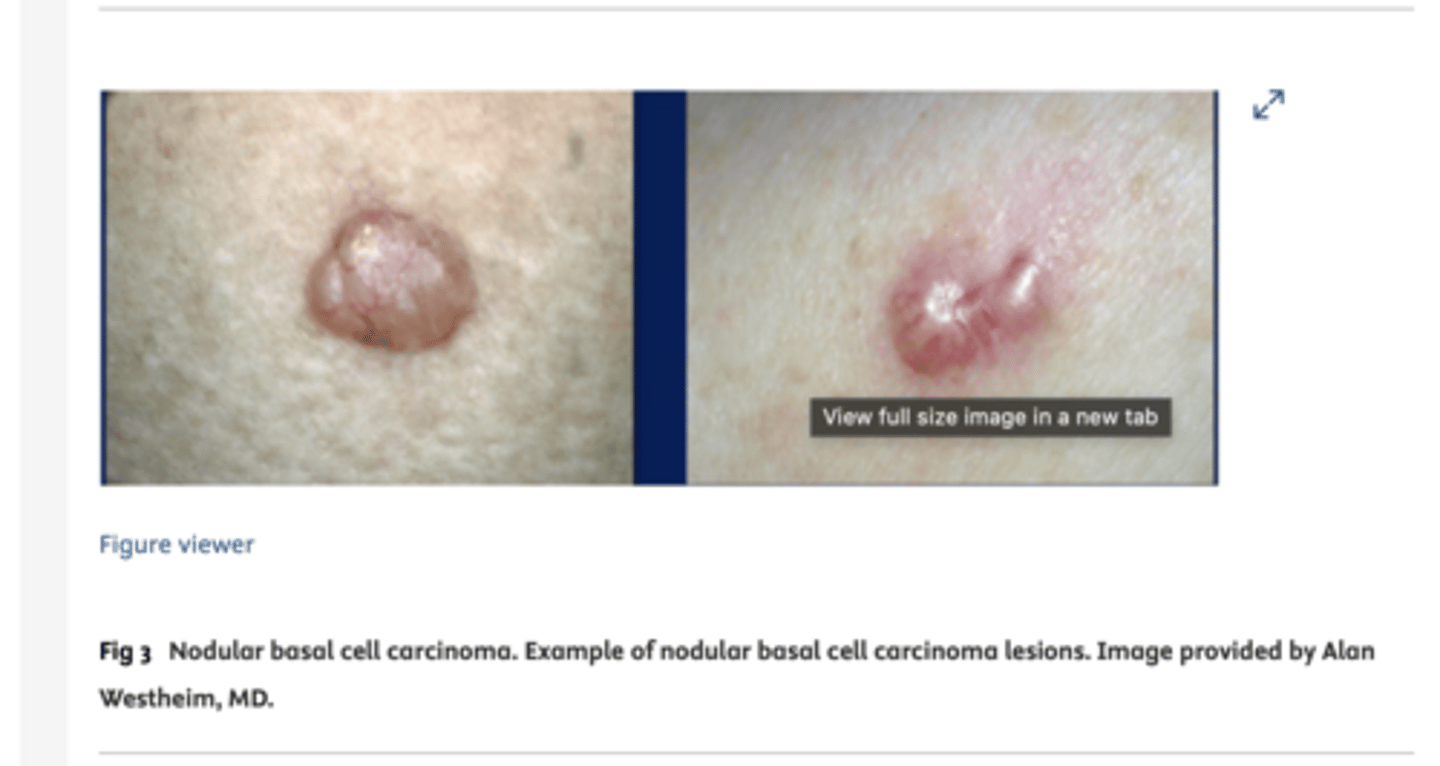
BASAL CELL CARCINOMA definition
A skin cancer originating from the basal keratinocytes within the epidermis
(pretty common - 25-30% of population)
BASAL CELL CARCINOMA risk factors (8)
- Family history
- previous history of skin cancer
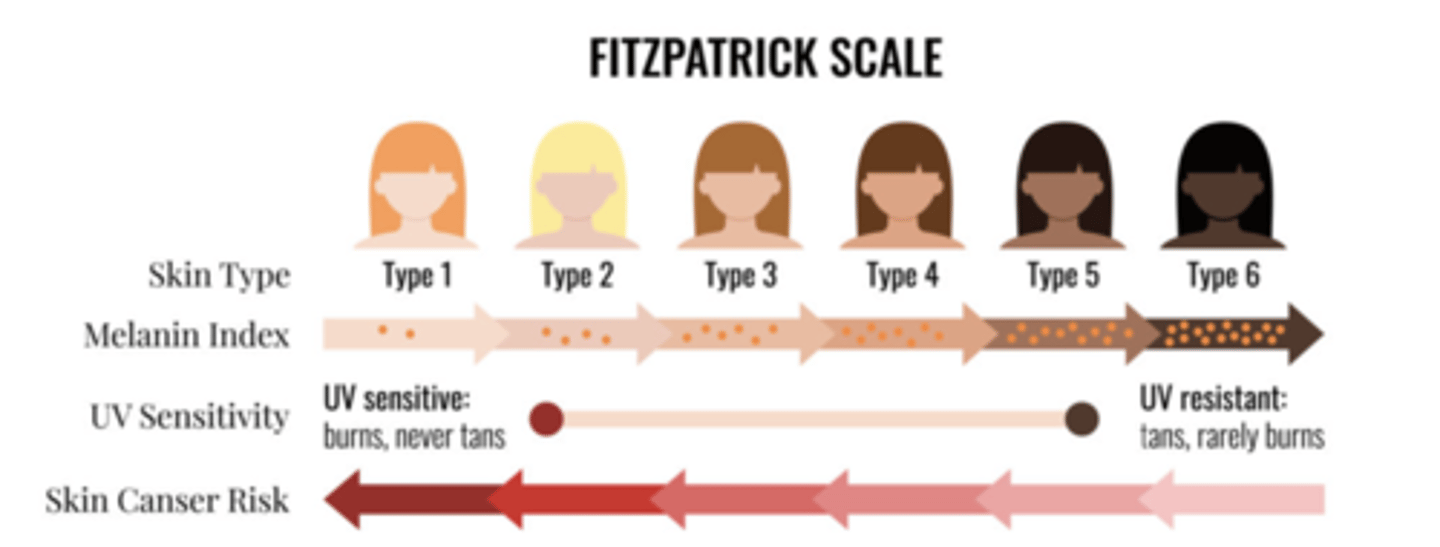
- Pale skin/light hair (always burns, never tans phenotype - Fitzpatrick type I or II skin)
- High levels of sun or UV exposure
- Immunosuppression
- Chronic inflammation, for example at the site of a burn
- Old age
- male sex
BASAL CELL CARCINOMA investigation
Diagnosis is usually made by excision biopsy with a 4mm margin
BASAL CELL CARCINOMA features
- slow growing
- Usually asymptomatic (pain/bleeding rare)
- Flesh coloured nodules with central depression, pearly surface, rolled edge, and telangiectasia
- They can can necrose and ulcerate in the centre
- In sun-exposed areas. There may be background sun-damage such as actinic keratoses
BASAL CELL CARCINOMA management
- Excision using a 4mm margin (6mm for high risk lesions)
sometimes:
- Mohs micrographic surgery (e.g in high risk areas such as nose, mouth, eyes)
- Radiotherapy
- curettage and cautery,
- topical 5-flourouracil,
- topical imiquimod - for more superficial lesions
- cryotherapy if the lesion appears low risk (small, flat, and superficial
- Lifestyle advice to prevent further lesions (sun block)
BOWEN'S DISEASE
- pre-malignant lesions that may turn into SCC
- irregular, red, keratinised, scaly plaques.

BOWEN'S DISEASE management
first line treatment:
5-fluorouracil
BULLOUS PEMPHIGOID definition
- autoimmune blistering disorder characterised by tense subepidermal blisters
- usually affects individuals over 60.
- prodromal phase that involves inflammation of the affected skin, making it very itchy

BULLOUS PEMPHIGOID pathophysiology
Autoantibodies targeting the hemidesmosomes that bind the basal keratinocytes of the epidermis to the basement membrane.
DERMATOFIBROMA what is it
- Dermatofibromas are firm, brown coloured nodules found most commonly on the lower leg.
- Patients may have a history of injuries, such as an insect bite.
- When squeezed, a dimple is present due to the firm tethering of the epidermis to the dermis

ECZEMA definition
•Inflammatory dermatosis characterised by erythema (redness of skin) and pruritus (itch)
- usually in the flexural surfaces, in babies usually presents on the face
can result in lichenification (pic)

ECZEMA investigations
Eczema is a clinical diagnosis and investigations aren’t always needed.
However,
- Bloods: (If concerns regarding superadded infection)
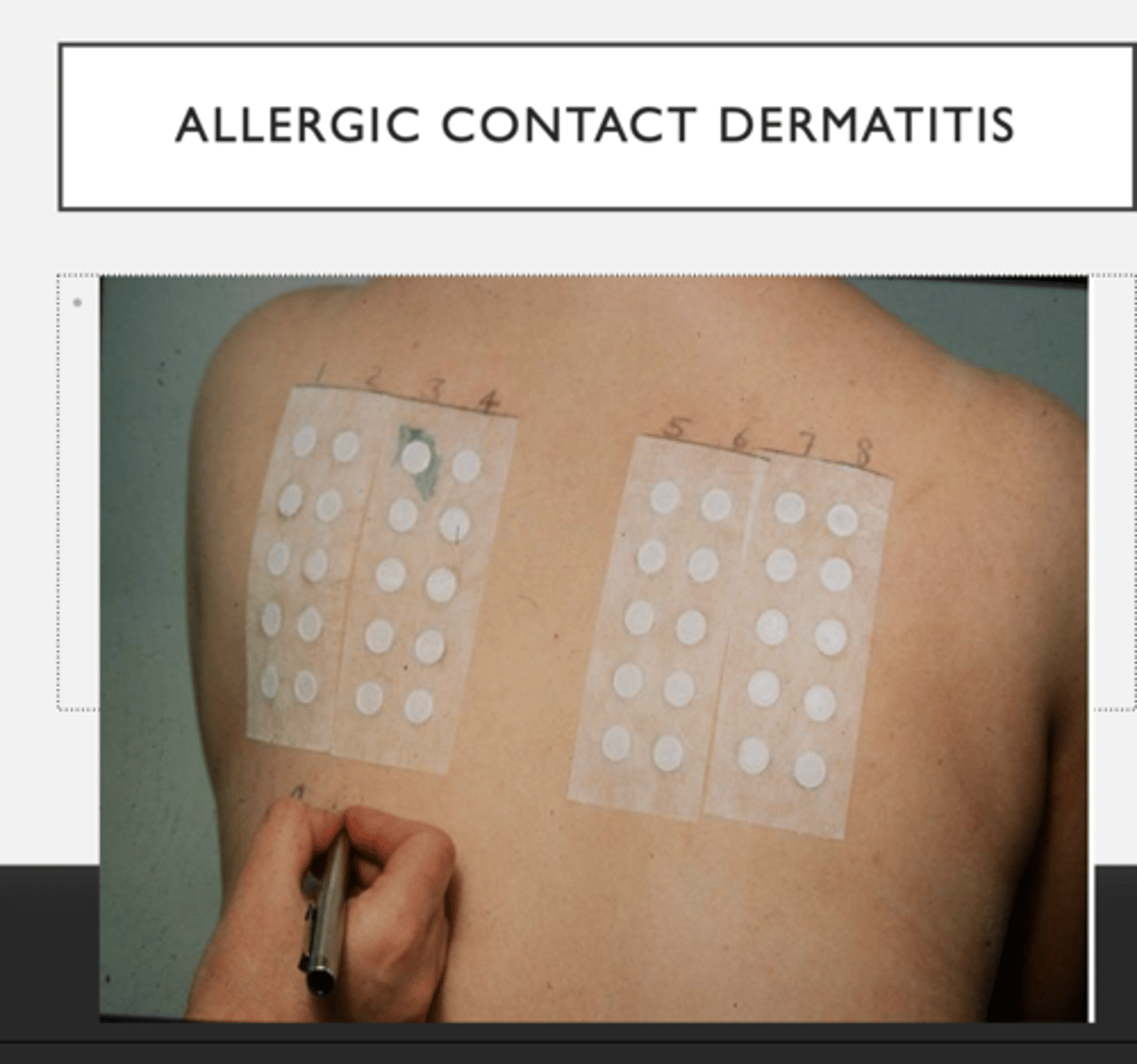
- Patch test: The allergen is applied to the skin under occlusion for 48 hours to confirm a delayed (type IV) allergic process implicated in allergic contact dermatitis.
- Swabs: bacterial and viral swabs if concerns regarding superadded infection.
ECZEMA management
•1st line - emollients
•2nd line - topical anti-inflammatories (e.g steroids) e.g hydrocortisone. Can vary in potency
•3rd line - phototherapy
•4th line - systemic agents e.g biologics, methotrexate
newer drugs - topical calcineurin inhibitors (Protopic),
- anti-histamines - to prevent scratching
ECZEMA (children) management
- emollients
- topical corticosteroids (depending on severity of eczema)
‼️ refer to dermatology if:
• uncertain diagnosis
• multiple flare ups
- not responding to treatment
• recurrent severe infection
• contact allergic dermatitis (e.g from nickel, latex)
• significant social/psychosocial effects
‼️ refer to paediatric allergy service if:
In moderate/severe eczema developing below 12 - 18 months this is highly indicative of food allergy!
ECZEMA HERPETICUM what is it
- caused by herpes simplex virus
- Extensive crusted papules, blisters and erosions which are painful
- Systemically unwell with fever and malaise
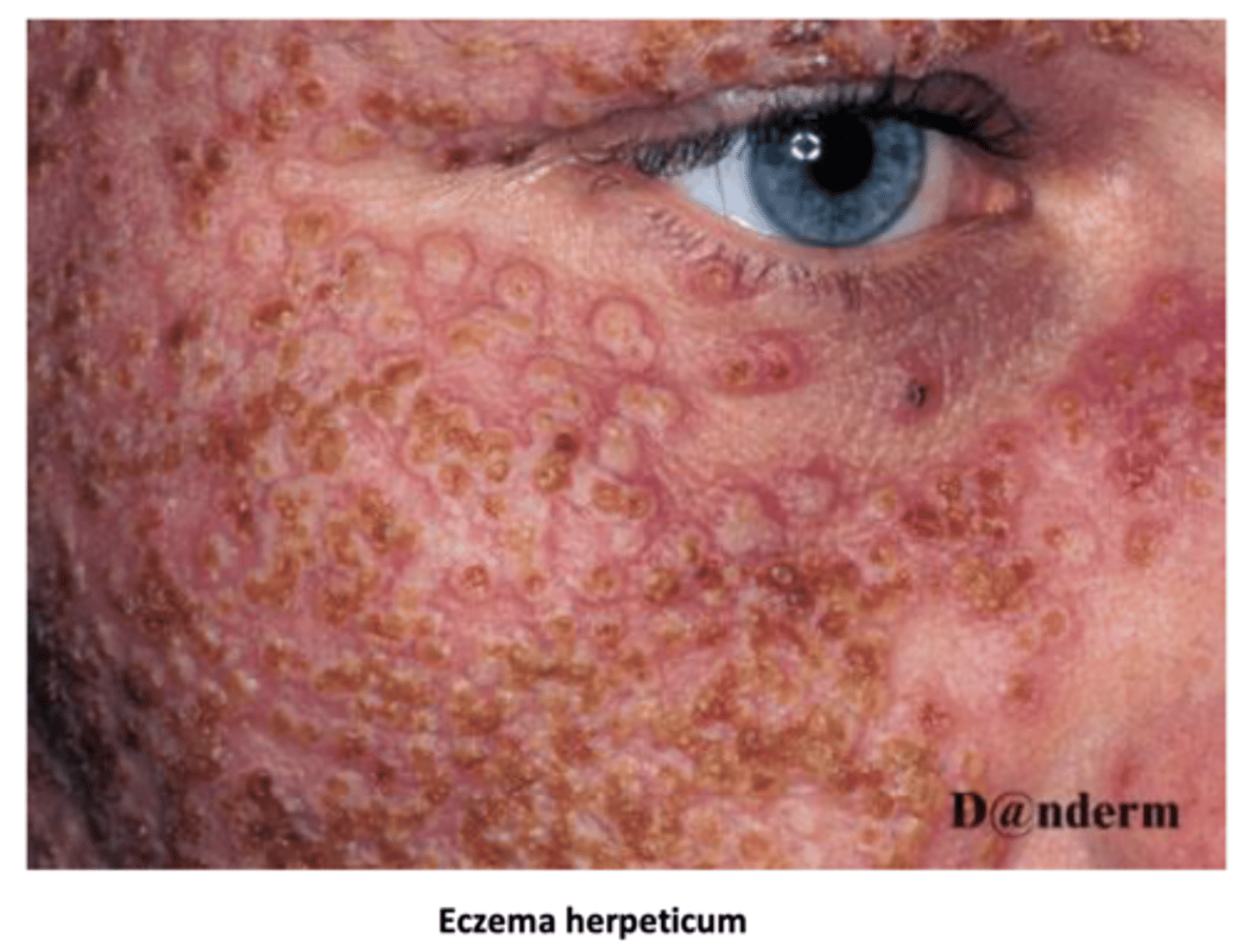
ECZEMA HERPETICUM management
- Antivirals (e.g. aciclovir)
- Antibiotics for bacterial secondary infection
ERYTHEMA MULTIFORME causes
- most frequently = HSV
-less commonly = mycoplasma
- Drug-induced causes (rare)
ERYTHRODERMA definition
life-threatening dermatological condition where there is widespread erythema covering more than 90% of the body's skin surface.

HEAD LICE symptoms
- Persistent itching of the scalp, neck, and behind the ears.
- Presence of actual nits attached to the scalp.
- Secondary changes due to scratching
HEAD LICE management
-Wet combing
- application of dimethicone 4% gel twice, at least 7 days apart
- exclusion from school is not necessary (spread likely occurred before detection anyway)
HYPERHIDROSIS management
excessive sweating
- topical aluminium chloride
eczema - allergic contact dermatitis investigations
patch testing
IMPETIGO features
- It typically starts on the face and spreads to other parts of the body.
- characterised by vesicles that rupture, forming honey-coloured crusts.

IMPETIGO management
Localised non-bullous impetigo:
1st line: topical hydrogen peroxide 1% cream (apply 2/3x daily for 5 days)
2nd line: topical antibiotic: 2% fusidic acid or mupirocin
Widespread non-bullous impetigo:
Topical antibiotics (fusidic acid/mupirocin) or oral antibiotics for 5 days, such as flucloxacillin
Bullous impetigo, or impetigo in those systemically unwell or at high risk of complications:
Oral antibiotics (flucloxacillin) for up to 7 days
Advise general hygiene measures
Children should be off school until all lesions are healed (crusted over) or until 48 hours after starting treatment.
keloid scars - where are they most likely to form?
on the sternum
KERATOACANTHOMA
- similar to an SCC
- but it is benign

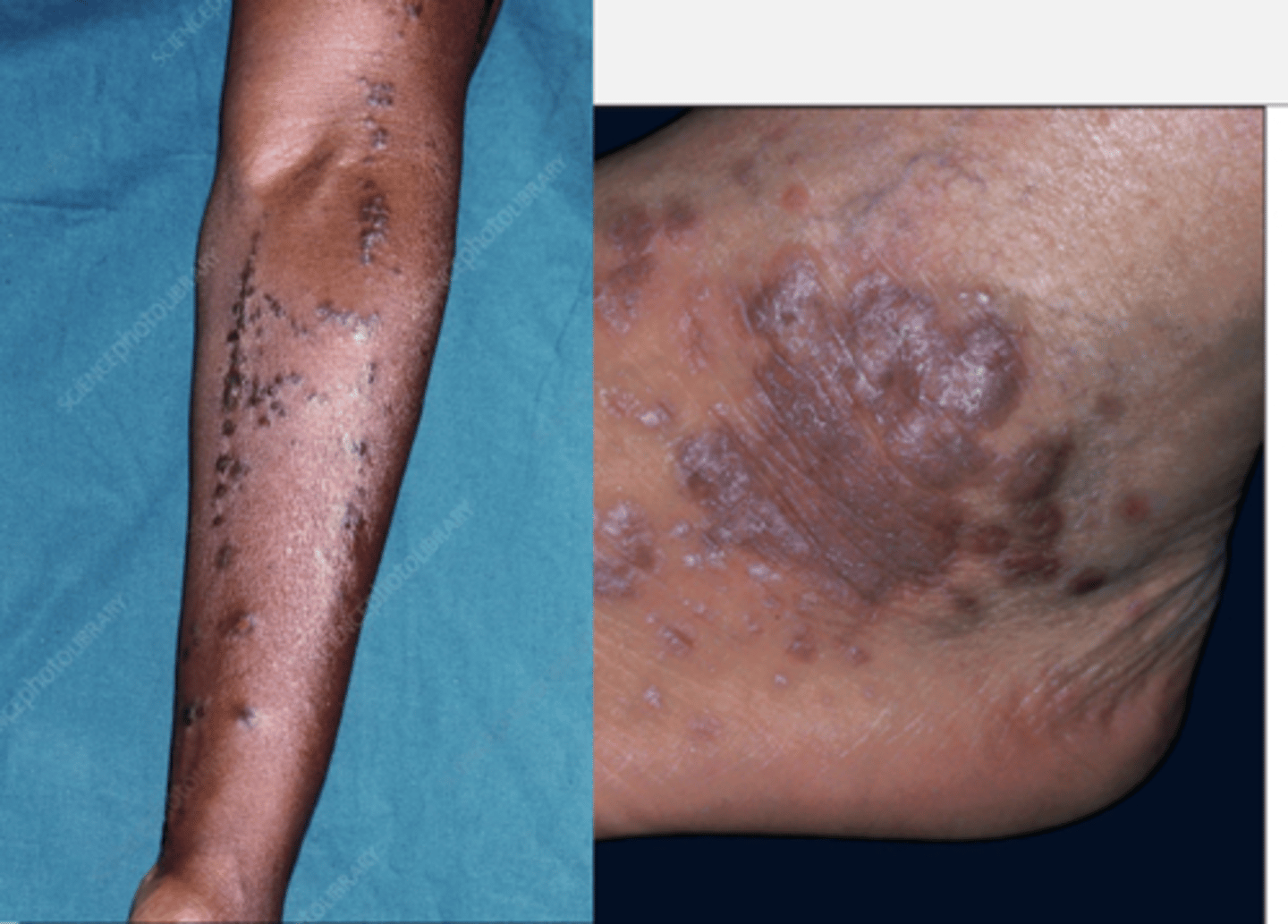
LICHEN PLANUS what is it
chronic inflammatory disorder mediated by T cells, manifesting as
- pruritic,
- polygonal,
- planar,
- purple
- papules or
- plaques
( known as the 6 P's.)
LICHEN PLANUS aetiology
idiopathic or
triggered by factors such as
- Hepatitis C,
- allergic contact dermatitis,
- localised skin injury or infection,
- specific medications.
LICHEN PLANUS management
first line: topical corticosteroids
LICHEN SCLEROSUS what is it
- a chronic inflammatory condition requiring close monitoring due to an increased risk of malignancy.
- Atrophic white patches on the genitalia with itching and dysuria

LICHEN SCLEROSUS treatment
topical corticosteroids (ultra potent)
e.g clobetasol proprionate 0.05%
MELANOMA prognosis
- Breslow Thickness (determined histologically, and is the most important prognostic indicator. measured in mm, from the top of the granular layer in the epidermis to the deepest point that the tumour extends)
(deeper = worse prognosis)
• Ulceration
• Sentinel Node Biopsy (if Breslow >=0.80mm)
MELANOMA features
Asymmetrical
Border irregularity
Colour irregularity (variegated)
Diameter (>=7mm)
Evolution of lesion (change in size/shape)
MELANOMA what are the subtypes
- Superficial spreading - this has a long radial phase, and is the most common type
- Lentigo maligna melanoma- this has a very long radial phase, existing as the pre-malignant lesion lentigo maligna before it starts invading the basement membrane
- Nodular melanoma - this has no radial phase, and is the most aggressive type
- Acral lentiginous - this has a short radial phase, and occurs in patients with darker skin tones more, involves the palms/soles
- Subungual - growing under the nail
- Amelanotic
MELANOMA management
- sentinel node biopsu
based on breslow's depth:
<1 mm = 1cm +/- SLNB
<2 mm = 1-2 cm + SLNB
>2 mm = 2 cm + SLNB
>4 mm or met = 2 cm + SLNB + chemo
MOLLUSCUM CONTAGIOSUM defintion
- common skin infection.
- transmission = close personal contact or shared surfaces such as towels
- mostly in children aged 1-4
MOLLUSCUM CONTAGIOSUM features
- pearly white/pink papule with a central umbilication
- appear in clusters on the body (EXCEPT palms and soles)

MOLLUSCUM CONTAGIOSUM treatment
- self limiting, usually resolves within 18 months
- treatment not usually recommended: but if necessary: cryotherapy, squeezing can be tried
PEMPHIGUS VULGARIS what is it
- autoimmune blistering skin condition characterised by flaccid intra-epidermal blisters
- IgG autoantibodies are targeted against desmosomes: structures that link keratinocytes to other keratinocytes within the epidermis
- The specific antigens are desmoglein 1 and desmoglein 3
- Nikolsky sign positive

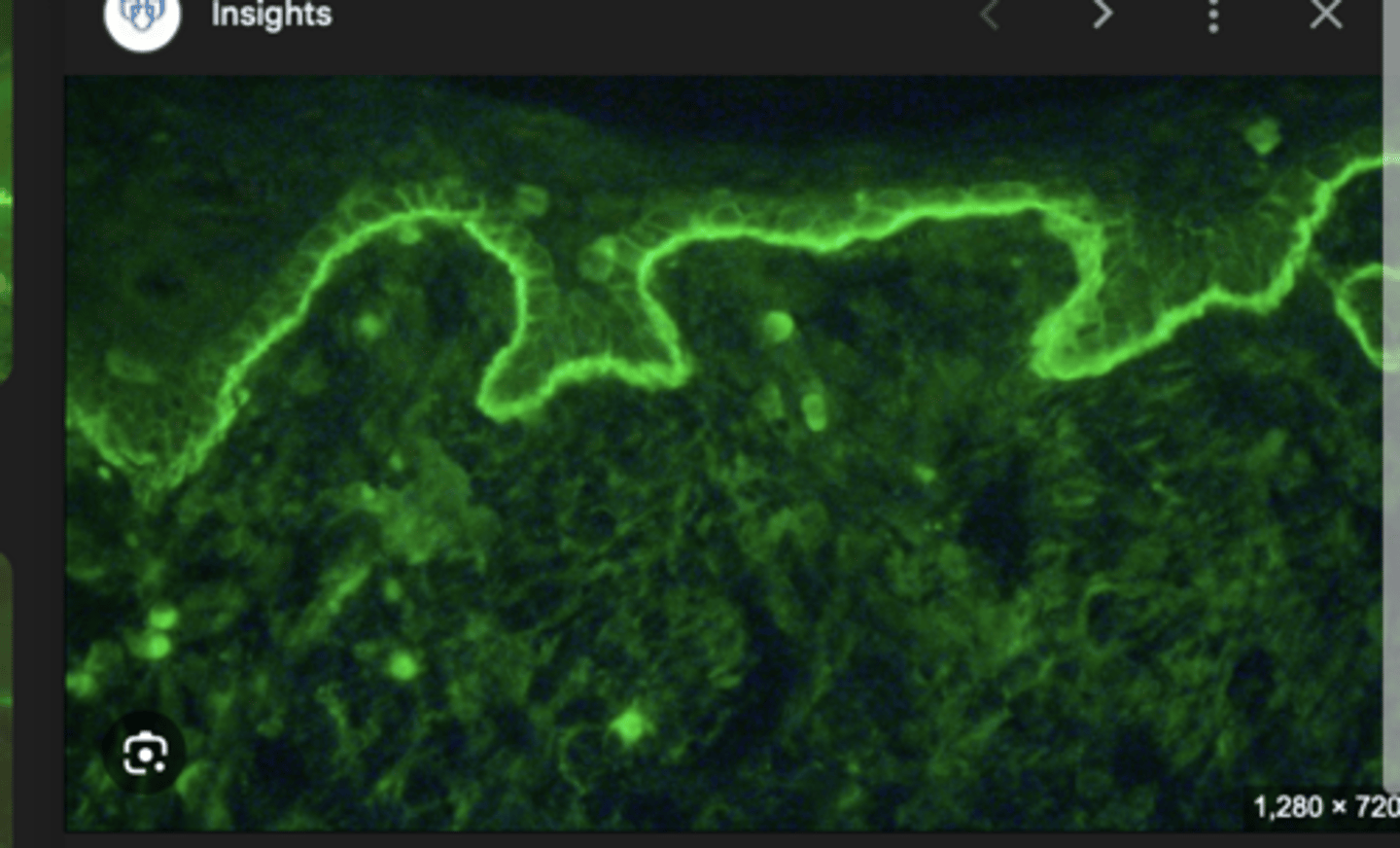
PEMPHIGUS VULGARIS what does immunofluorescence show
a fish-net/chicken-wire pattern of staining within the epidermis
PITYRIASIS ROSEA features
- A self-limiting rash that resolves after 10 weeks
- Characterised by a herald (coin-shaped) patch and subsequent fir-tree (Christmas tree) pattern eruption
- common in individuals aged 10-35
- often have a preceding viral illness

PITYRIASIS VERSICOLOR what is it
a superficial cutaneous fungal infection caused by Malassezia furfur
PITYRIASIS VERSICOLOR symptoms
- commonly on chest and bacj
- patches may be hypopigmented or hyperpigmented (hence versicolor).
- May be more noticeable following a suntan
- scale is common

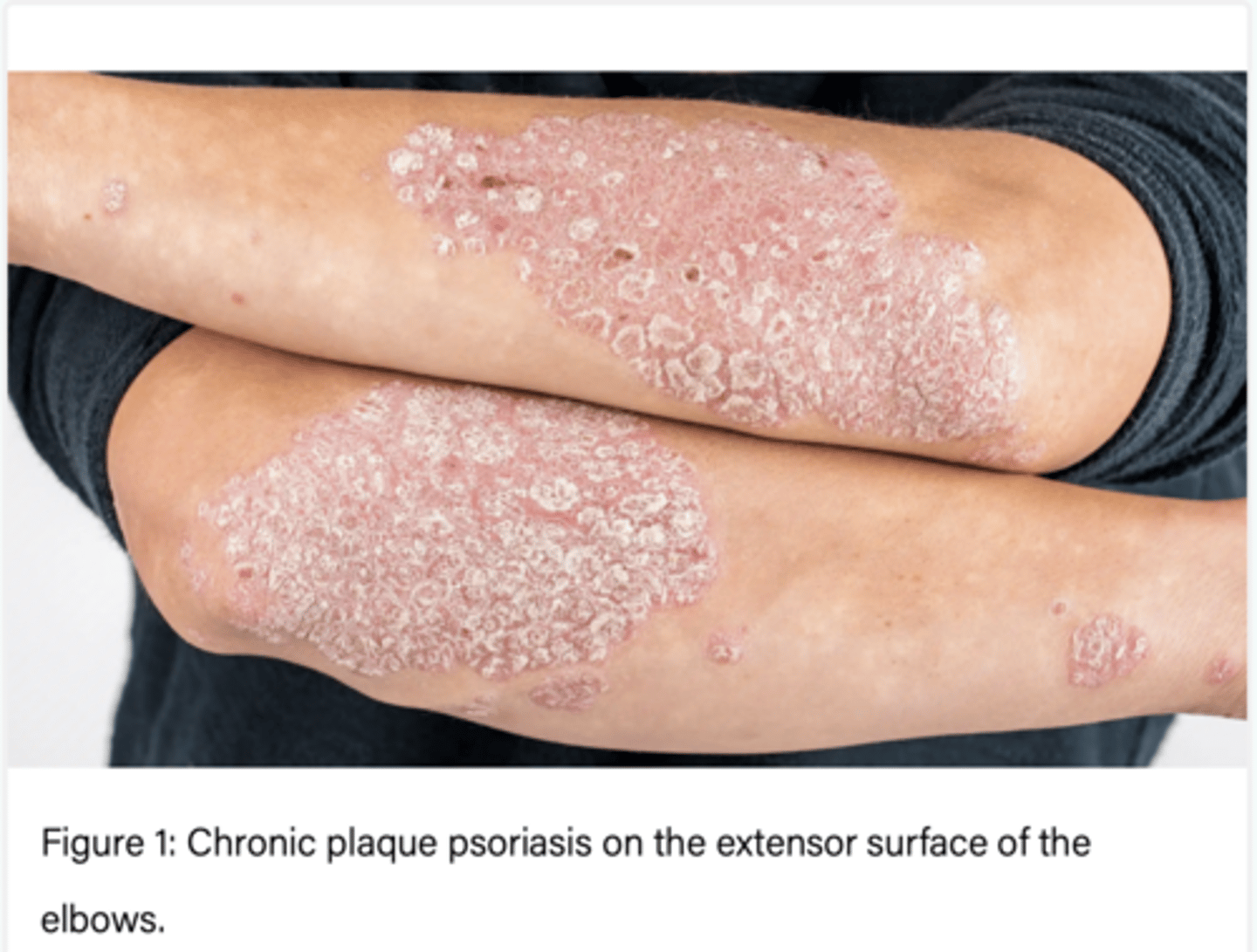
PSORIASIS definition
Psoriasis is a chronic autoimmune disease characterised by well-demarcated, erythematous, scaly plaques.
characterised by inflammation (resulting in redness) and hyperproliferation of keratinocytes (resulting in scale).
PSORIASIS triggers for worsening
TALIBAN
Trauma
Antimalarials/ACE inhibitors
Lithium
Indomethacin
B blockers
Alcohol
NSAIDs
PSORIASIS types
Chronic plaque psoriasis-
- commonest type
- symmetrical plaques on the extensor surfaces of the limbs (knees + elbows), scalp and lower back.
- well defined
Flexural (inverse) psoriasis-
- smooth, erythematous plaques without scale in flexures and skin folds.
Guttate psoriasis-
- multiple small, tear-drop shaped, erythematous plaques occur on the trunk after a Streptococcal infection in young adults.
Pustular psoriasis-
- multiple petechiae and pustules on the palms and soles.
Generalised/erythrodermic psoriasis
- rare but serious form characterised by erythroderma and systemic illness

PSORIASIS what nail changes are seen
- Nailbed pitting: superficial depressions in the nailbed
- Onycholysis: separation of nail plate from nailbed
- Subungual hyperkeratosis: thickening of the nailbed

PSORIASIS what condition is associated
psoriatic arthritis
PSORIASIS management
management can change depending on where the psoriasis presents
1ST LINE: Topical treatment
- All patients should use an emollient to reduce scale and itch
- 1st, potent topical corticosteroid OD (eg Betnovate) + topical vitamin D OD (eg Dovonex, calcipotriol) applied at different times
- 2nd, stop the topical corticosteroid, apply topical vitamin D twice daily
- 3rd, stop the topical vitamin D, apply potent topical corticosteroid twice daily
2ND LINE: Phototherapy
- Narrowband UVB phototherapy
- Psoralen + UVA (PUVA) - rarer
3RD LINE: Systemic treatment
- 1st line: Methotrexate
- 2nd line: Ciclosporin
- 3rd line: Acitretin (vitamin A derivative). teratogenic
4TH LINE: Biologics
- Infliximab
- Etanercept
- Adalimumab
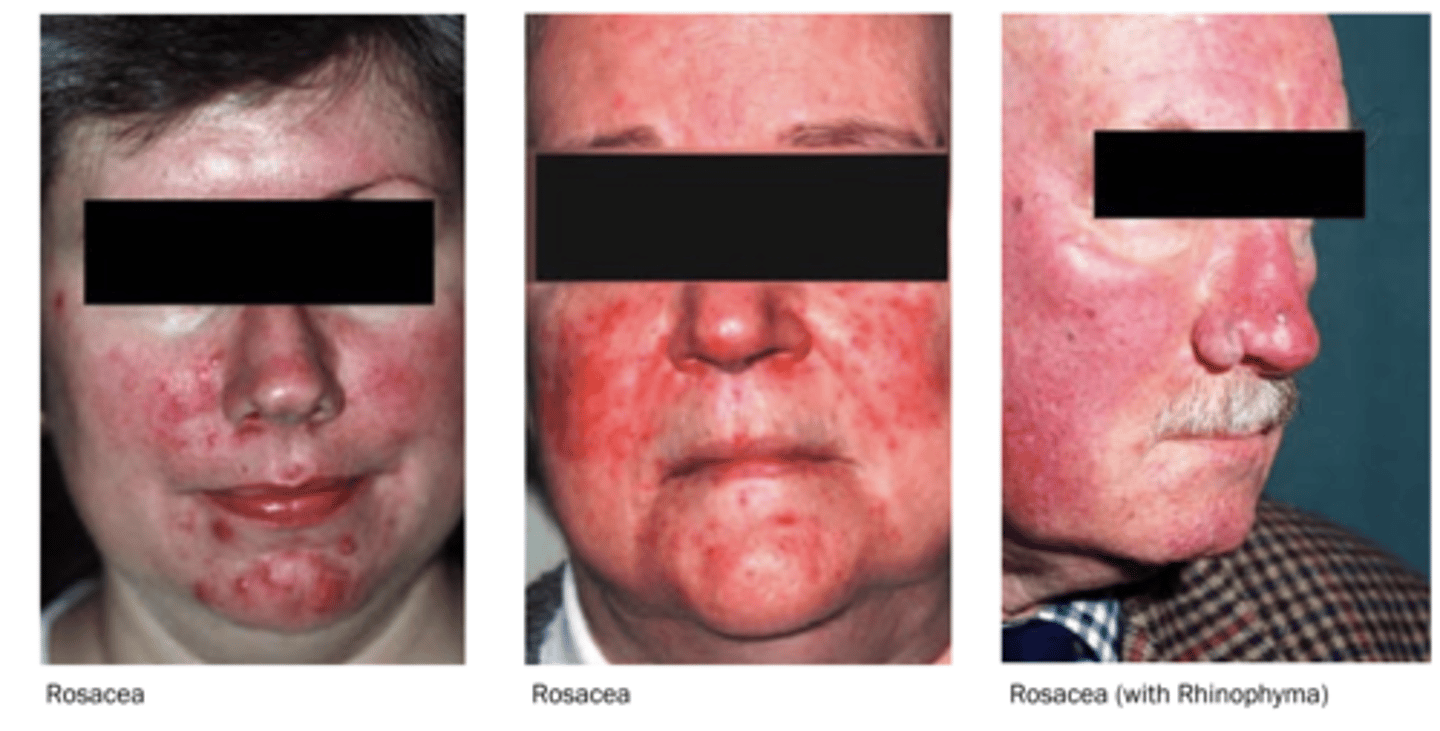
ROSACEA (aka acne rosacea) features
• Flushing often made worse by alcohol, spicy foods, hot drinks, temperature changes or emotion
• Telangiectasia
• Papules on erythematous background
• Pustules
• Facial disfigurement
• Intermittent or permanent
• Rhinophyma
SUNLIGHT can exacerbate it
ROSACEA management
Topical Therapy: , Topical ivermectin (anti-parasitic), Topical Metronidazole
Systemic Therapy: Antibiotics e.g doxycycine if have papules/pustules
Other therapies: Electrocautery; IPL (intense pulsed light)
‼️ refer if: doubt over diagnosis, severe disease, ocular involvement
SCABIES features
- widespread pruritus
- linear burrows on the side of fingers, interdigital webs and flexor aspects of the wrist
- in infants, the face and scalp may also be affected
- secondary features are seen due to scratching: excoriation, infection

SCABIES management
•Apply Permethrin (antiparasitic) lotion over the entire body, except face
•Leave lotion in place for 8-48 hours
•Re-treat in 1 week
•Treat all close contacts at the same time, even if asymptomatic
crusted scabies - what is it
scabies in a immunocompromised person e.g HIV
management: combination of oral ivermectin and topical permethrin
SEBORRHOEIC DERMATITIS associated conditions
- HIV
- parkinsons
SEBORRHOEIC DERMATITIS management
topical ketoconazole
SEBORRHOEIC KERATOSIS features
- classic 'stuck on appearance

SEBORRHOEIC KERATOSIS what is a red flag with these things
The sudden onset of multiple seborrhoeic keratoses may indicate an underlying malignancy, known as the Leser–Trélat sign.
SHINGLES what is it
reactivation of the varicella zoster virus. After feting chickenpox, the virus lies dormant.
Shingles causes an acute, unilateral painful blistering rash
SHINGLES risk factors
- increasing age
- HIV
- immunosuppression e.g steroid and chemo
SHINGLES features
1. there is a prodromal period of burning pain over the affected dermatome
2. then a rash wooers and is characteriscally well demarcated by the dermatome.
SHINGLES management
- Analgesia
- Antivirals
SKIN CANCER types
basal cell carcinoma,
squamous cell carcinoma,
melanoma
STAPHYLOCOCCAL SCALDED SKIN SYNDROME (SSSS) definition
a severe desquamating rash that primarily affects infants.
STAPHYLOCOCCAL SCALDED SKIN SYNDROME (SSSS) symptoms
- Superficial fluid-filled blisters are common,
- Erythroderma (erythema affecting over 90% of the body surface)
- Desquamation (peeling of the epidermis)
- positive Nikolsky sign
- Perioral crusting or fissuring is frequently observed, with the oral mucosa usually remaining unaffected.
- systemic sx - fever
STPAHYLOCOCCAL TOXIC SHOCK SYNDROME (STSS) definition
- Fever >38.9
- Rash with diffuse macular erythroderma
- Desquamation 1-2 weeks after rash onset
- Hypotension SBP <90
- Multiorgan involvement -
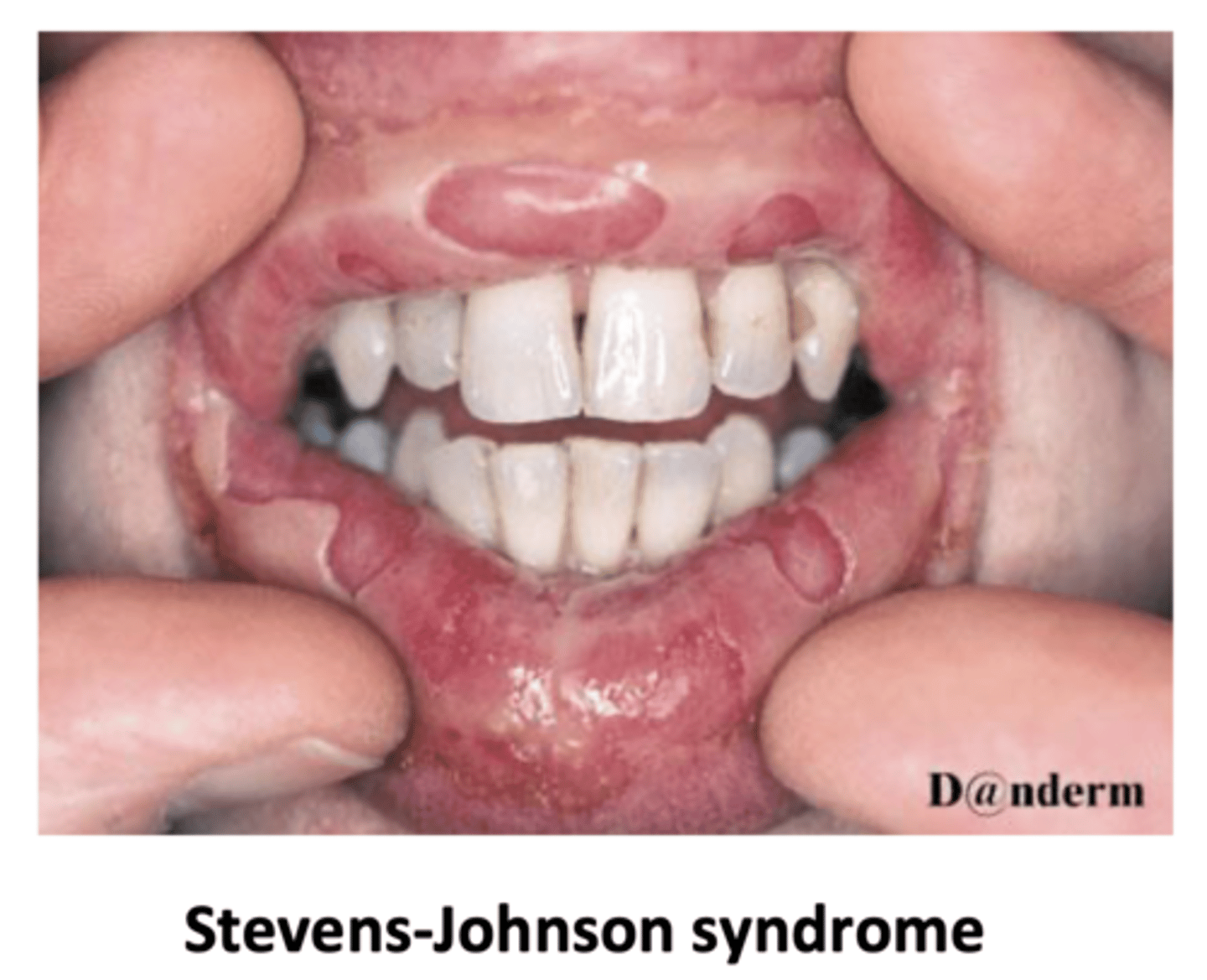
STEVENS JOHNSON SYNDROME what is it
mucocutaneous necrosis with at least two mucosal sites involved.
SJS is when there is <10% pf the body area affected
(SJS-TEN is a spectrum)
STEVENS JOHNSON SYNDROME management
It is a medical emergency requiring immediate withdrawal of the offending drug and urgent supportive management in an intensive care or burns unit.
SQUAMOUS CELL CARCINOMA features
- keratinised, scaly, irregular nodules. On occasion, the keratin may be so developed that it forms a horn or a plug
- Often in sun exposed areas. There may be background sun-damage, for example wrinkled skin and actinic keratoses.
- slow growing, over months
- Pain, tenderness, and bleeding usually present

SQUAMOUS CELL CARCINOMA investigation
- excision biopsy with a 4mm margin (treatment and diagnosis at the same time, based on clinical suspicion)
- Sometimes, a punch biopsy is the first investigation that is performed ,, later requiring an excision biopsy
A 6mm margin is required for high risk lesions, which are defined as:
- 2cm+ diameter
- Location on the ear, lip, face, hands, feet, or genitals
- Elderly or immunosuppressed
- Histological features: thicker than 2mm, poor differentiation, blood or nerve involvement, invasion of subcutaneous tissue
SQUAMOUS CELL CARCINOMA management
- excision using a 4mm margin (6mm for high risk lesions)
what is a marjolin ulcer?
A Marjolin ulcer is a squamous cell carcinoma that develops in previously injured or chronically inflamed skin, often following burns or scars.
TINEA CORPORIS what is it and treatment
fungal infection of the skin that causes an itchy, red, and scaly rash, often with a ring-like shape.
Also known as ringworm. Treatment is topical anti fungal
TINEA CRURIS what is it
also known as jock itch -
Patchy skin lesions which may be red or pink edge surrounding an area of central clearing and grow outwards
Patients may report the lesions becoming scaly or itchy
Lesions are most commonly found in skin folds, including the groin
TOXIC EPIDERMAL NECROSIS (TEN) what is it
- extensive skin and mucosal necrosis accompanied by systemic toxicity.
- usually occurs as a drug reaction (few days -1 month after) - NOT IMMEDIATE
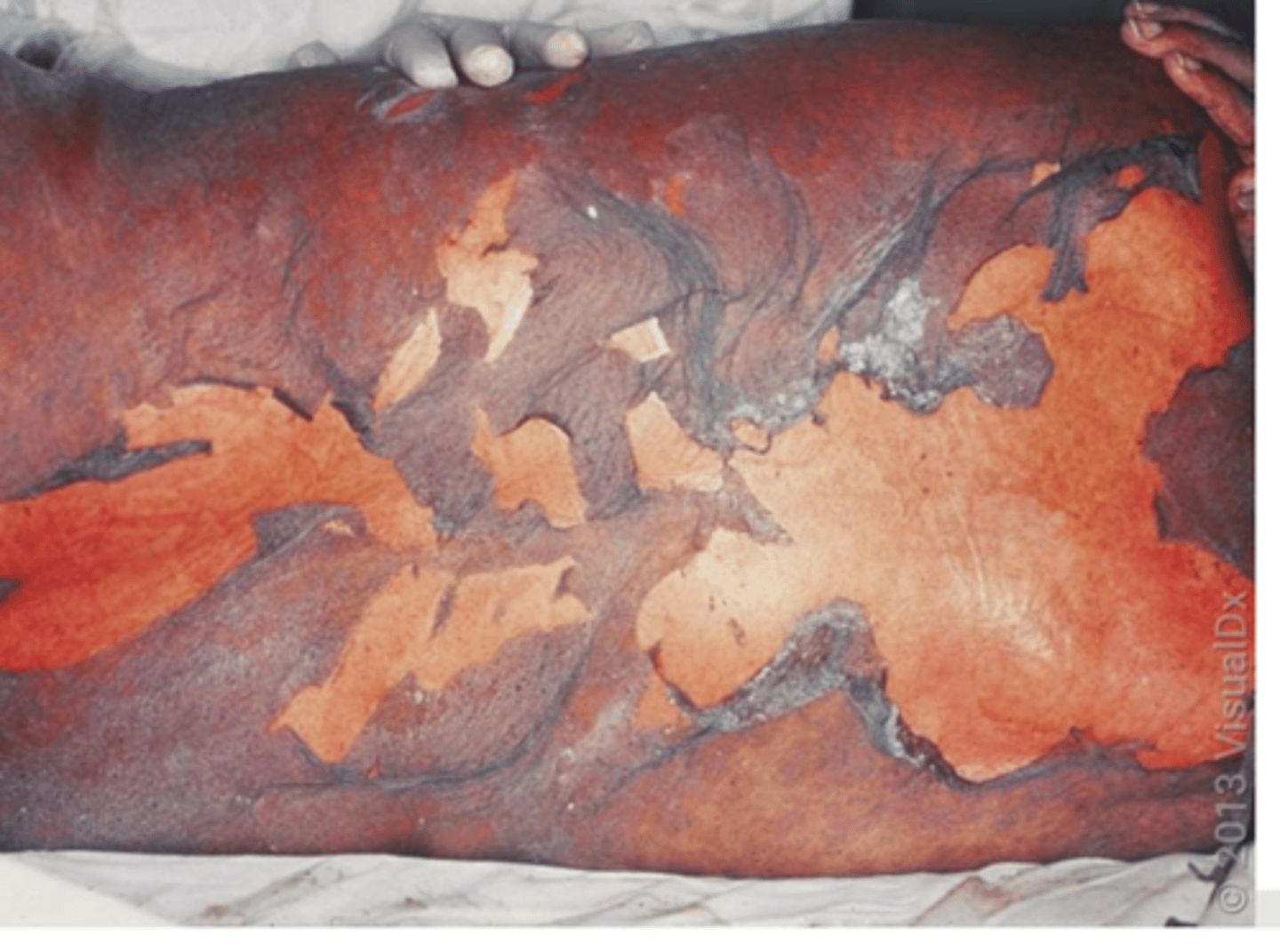
TOXIC EPIDERMAL NECROSIS (TEN) features
- painful rash
- which then blisters
- skin then detaches and peels off
- nikolsky sign = +
(when you touch the skin it peels off)
TOXIC EPIDERMAL NECROSIS (TEN) management
1. stop the drug thats causing it
2. skin care: emollients
3. fluid balance and nutrition
4. pain management
URTICARIA (hives) definition
commonly referred to as hives, is characterised by the rapid development of pruritic (itchy), erythematous (red), raised wheals that may vary in size and shape. These wheals typically resolve within hours to days and can occur anywhere on the body
URTICARIA triggering factors
Urticaria may be triggered by various factors, including:
Allergens (e.g. foods, medications, insect stings)
Physical stimuli (e.g. pressure, cold, heat)
Infections (e.g. viral or bacterial)
Autoimmune processes
Stress and emotional factors
Genetics may play a role in predisposition
URTICARIA signs and symptoms
- Pruritus (itching), often intense
- Erythematous wheals with well-defined borders (sometimes with a central clearing - as seen in picture)
- Wheals that vary in size and shape
- Rapid onset and resolution (usually within 24 hours)
- Occasionally, angioedema (swelling of deeper tissues), which can involve the lips, eyelids, or extremities

URTICARIA management
- Identification and removal of triggers
Pharmacological treatment:
- First-line: Non-sedating antihistamines (e.g., cetirizine, loratadine;)
- Second-line: higher doses of antihistamines or other medications like leukotriene receptor antagonists or omalizumab may be considered.
- If symptoms are severe, oral corticosteroid can be given e.g. 40mg prednisolone for 7 days, in addition to the above.
- Symptomatic management includes antipruritic creams such as calamine lotion or topical menthol 1% in aqueous cream.
- If there is sleep disturbance, sedating antihistamines such as chlorphenamine can be given.
VITILIGO definition
- autoimmune dermatological disorder where there is loss of melanocytes
- occurs over time (not from birth)
- smooth falt patches of skin depigmentation
