Cellular Pathology
1/82
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
83 Terms
What is Cellular Adaptation?
Reversible changes to the size, number, phenotype, metabolic activity or function of cells in response to changes in their environment.
What are examples of Cellular Adaptation?
Hyperplasia
Hypertrophy
Atrophy
Metaplasia
How does Cellular response to stimulus?
Via Physiological and Pathological response
Physiological: in response to normal stimulus
Pathological: in response to abnormal stimulus
An increase in the number of cells in an organ or tissue that may then have increased volume:
Hyperplasia.
What is the Physiological cause of Hyperplasia?
Cause by normal Stressors such as:
Hormonal: Increased number of glandular epithelial breast cells during pregnancy
enlargement of breasts
preparation for lactation
Increases functional demand: living at high altitude leads to hyperplasia of erythrocyte precursors in the bone marrow.
Compensatory:
Regeneration of liver following partial hepatectomy
Regeneration of epidermis after abrasion
What is the Pathological cause of Hyperplasia?
Occurs due to an abnormal stressor (e.g., excessive stimulation of hormones or growth factors)
Endometrial hyperplasia (increased estrogen)
Benign prostatic hyperplasia (androgens)
Epidermal hyperplasia in psoriasis
What Is Hypertrophy and its Physiological and Pathological cause?
Hypertrophy is an increase in the size of cells, which leads to an increase in the size of an organ or tissue.
Physiological causes include increased workload (e.g., muscle growth from exercise)
Pathological causes include stress or damage, such as cardiac hypertrophy due to hypertension or aortic stenosis
Hyperplasia vs Hypertrophy
They both frequently occur together
both can result win increase organ size
A decrease in size of a cell:
Atrophy-
May be due to loss of blood supply, loss of endocrine stimulus, disuse, decreased workload, aging.
What is Physiological cause of Atrophy?
Physiologic:
Atrophy of brain with aging
Atrophy of gonads after menopause
(decreased hormones)
Decrease in the size of the uterus after
pregnancy
What is pathological cause of Atrophy?
Immobilization of a limb after fracture
(disuse)
Cachexia (starvation, insufficient nutrients)
Ischemic process (inadequate supply of
oxygen)
A change in epithelium at a site, or location form one type to another: (change in cell)
Mataplasia
Mechanism: epithelium normally present at a site cannot handle the new environment so it converts to a type of epithelium that can adapt.
What is the Physiological and Pathological cause of Metaplasia?
Physiologic:
Cervical changes
Pathologic:
Cigarette smoke
Barrett’s esophagus
Occurs when the cells cannot adapt to their new environment:
Cell Injury.
Can be reversible or irreversible
What are the Vulnerable systems in cellular injury:
DNA, Cell membrane, Protein generation, Adenosine triphosphate (ATP) production.
What are the causes of cell injury?
Hypoxia, ischemia, Physical agents, Chemical agents, Infectious agents, radiation and toxins, metabolic abnormalities, Immune dysfunction, Nutritional imbalances, Aging.
4 mechanism of cellular injury:
Hypoxia, Free radicals, chemical injury, Increased mitochondrial cytosolic calcium (mitochondria injury)
What is Hypoxia?
Hypoxia is a lack of oxygen in tissues, leading to decreased ATP production, cellular dysfunction, and potentially cell death if prolonged.
Hypoxia (↓ O₂)
↓
↓ Oxidative phosphorylation in mitochondria
↓
↓ ATP production
↓
Failure of ATP-dependent pumps
↓
Cell swelling + ↑ intracellular Ca²⁺
↓
↑ Anaerobic glycolysis
↓
↑ Lactic acid
↓
↓ Intracellular pH
↓
Cell dysfunction
↓
Reversible injury
↓ (if prolonged/severe)
Irreversible injury
↓
Necrosis
What are free radicals in cellular injury?
Free radicals are chemically unstable and react with other molecules —>damage
Produced by physiologic oxidation-reduction reactions, UV light, ionizing radiation, metals, chemicals (smoking, pollution), inflammation, stress
What are free radicals in Cellular Injury?
Chemical injury = toxins damage cells either directly or through toxic metabolites, causing membrane damage, mitochondrial dysfunction, free radical formation, ATP depletion, and ultimately cell death.
what happens in increased mitochondrial calcium:
Results in:
Lipid peroxidation
Mitochondrial injury
Loss of calcium homeostasis
↓ ATP production
Apoptosis
Increased cytosolic and mitochondrial calcium is a key mechanism of cellular injury because it activates destructive enzymes, damages mitochondria, decreases ATP production, and triggers apoptosis or necrosis.
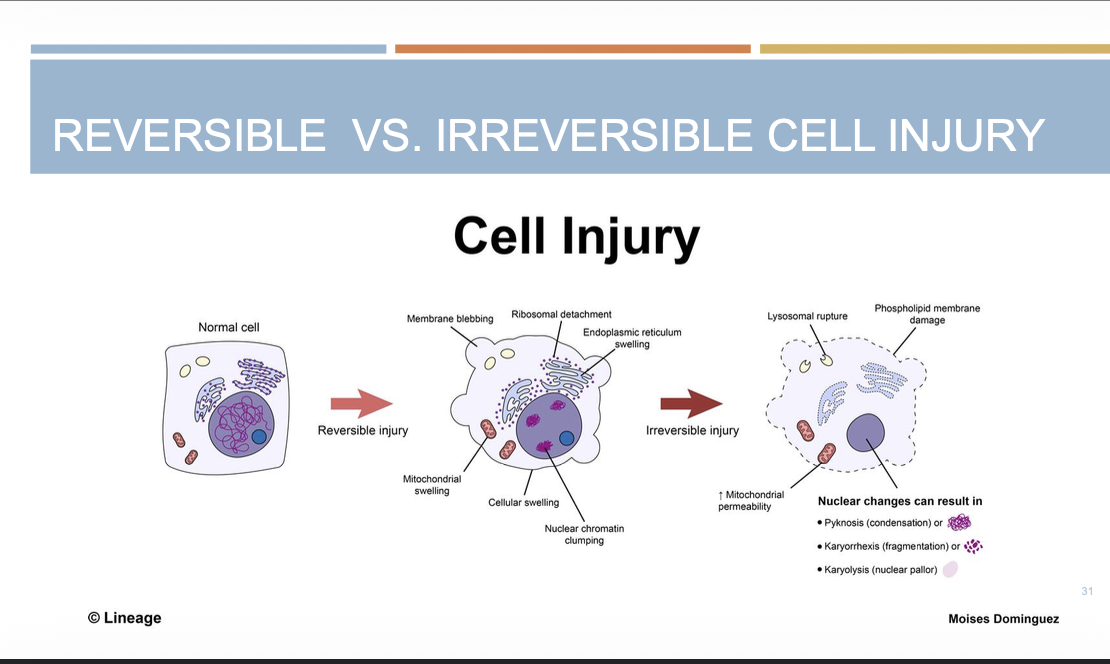
Cell Injury diagram:
Reversible injury is characterized by cellular swelling and recovery after removal of the stress, whereas irreversible injury involves severe mitochondrial and membrane damage leading to necrosis or apoptosis.
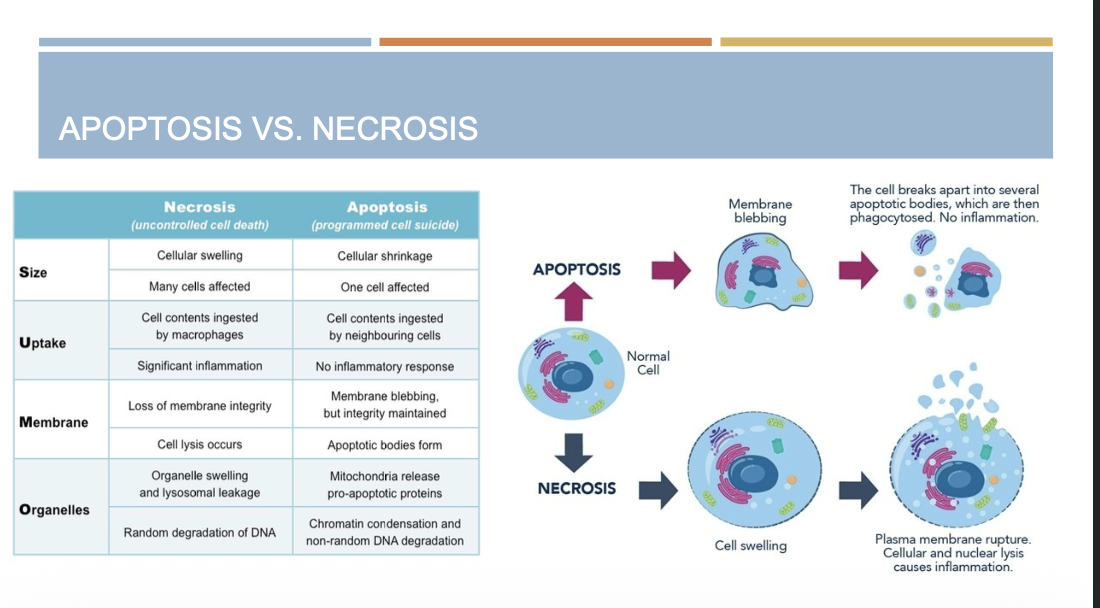
Two types of cell death:
Apoptosis: controlled (programmed) cell death/breakdown of cells occurring in response to irreversible cellular damage or as part of normal growth and development.
Necrosis: uncontrolled breakdown of cells/cell death in response to irreversible cellular injury
Phases of Apoptosis:
Initiation: caspases (enzyme) become catalytically active.
Execution: action of caspases causes cell death.
PATTERNS OF OCCURRENCE OF APOPTOSIS
During growth and development, some cells serve a function in the growth phase but then need to be removed after their purpose is fulfilled.
In neonates, a rapid cell growth rate is necessary.
In adults, unrestrained cell growth can cause cancer.
When DNA sustains irreparable damage, the cell must be destroyed so any mutations that may have developed will not be propagated.
Apoptosis removes damaged cells from the body = safety step
What is Intrinsic pathway in apoptosis?
The intrinsic pathway is a form of apoptosis initiated by internal cellular signals, often due to stress or damage, activating caspases and leading to programmed cell death.
What is extrinsic pathway in apoptosis?
The extrinsic pathway is a form of apoptosis initiated by external signals, such as ligands binding to death receptors on the cell surface, which activates caspases and leads to programmed cell death.
What does cell death look like microscopically?
Chromatin condensation and fragmentation
Uncontrolled (randomized) breakdown of cells/cell death in response to irreversible cellular injury; triggers inflammatory response:
Necrosis
Gross morphology of necrosis:
softening and discoloration

Different types of microscopic morphology of necrosis:
Coagulative necrosis- firm
Liquefactive necrosis- liquid
Fat necrosis- chalk
Caseous necrosis- cheese
Apoptosis vs necrosis
Apoptosis- blebbing
Necrosis- swelling
The most common type of necrosis, usually caused by ischemia (loss of blood supply) or infarction in solid organs.
Coagulative necrosis
protein denaturation (loos of blood)
Infarction = tissue death (necrosis) caused by a loss of blood supply (ischemia)
Organs affected: any organ (except brain- liquefactive)
Gross morphology of necrosis
dry, hard, yellow- white appearance to tissue
What organ is affected by liquefactive necrosis?
Brain
abscess formation (bacterial infection in lungs etc.)
Enzymatic breakdown in lipid-rich organs
Liquefactive necrosis
occurs when tissue becomes transformed into a liquid mass due to enzymatic breakdown, often seen in lipid-rich organs like the brain. (Loss of cellular architecture)
Gross morphology of liquefactive necrosis?
Tissue transformed into a liquid, viscous mass.
LIQUEFACTIVE NECROSIS – MICROSCOPIC MORPHOLOGY
loss of organ cellular architecture
lipid-laden
macrophages replace the dead tissue
change in adipose tissue due to trauma or the release of enzymes from adjacent organs:
Fat necrosis
Breakdown of lipid + release of fatty acids + calcium chalky deposits.
Due to infections, trauma, ischemia, toxins
what are the common organ affected by fat necrosis?
Organs affected: commonly breast and pancreas
What is Gross morphology of fat necrosis?
Gross morphology: yellow, white/chalky deposits
Microscopic morphology of fat necrosis?
large, lipid filled vacuoles
Occurs when the immune system cannot successfully remove a foreign stimuli (e.g., tuberculosis).
Caseous Necrosis:
Immune system seals off the foreign matter by forming a granuloma.
A type of necrosis characterized by the appearance of cheese-like (caseous) material, often seen in tuberculosis infections.
organs affected of Caseous necrosis?
any organs
Gross morphology of caseous necrosis
Gross morphology: yellow-white, soft, “cheesy” appearance
Microscopic morphology of caseous necrosis
granuloma with central necrosis, eosinophilia
Cellular Accumulations
Cellular accumulations occur when substances build up inside cells because they are produced too much, not metabolized properly, or cannot be removed.
Substances can accumulate in cells due to cellular damage or intrinsic abnormality in metabolic function (e.g. genetic disease)
Substances that can accumulate:
Lipofuscin
Calcium
Protein
Iron
Fat
Cholesterol
Glycogen
Pigments
Lipofuscin
“wear-and-tear” pigment, endogenous production
Mechanism of formation: product of lipid peroxidation which accumulates in lysosomes as cells ages; cells cannot get rid of it.
Organs affected: commonly in the heart, liver, skin.
Gross morphology of lipofuscin
brown discoloration to organs
Microscopic morphology of lipofuscin:
finely granular, yellow-brown pigment, which often surrounds the nucleus
What are the causes of hypercalcemia
Causes of hypercalcemia:
Increased parathyroid hormone (PTH)
Destruction of bone by tumors
Vitamin D intoxication
Renal failure
Sarcoidosis
Organs affected: vasculature, kidneys, lungs
deposition of calcium salts in normal tissues due to high blood calcium levels (hypercalcemia).
Metastatic calcification.
Dystrophic calcification.
deposition of calcium salts in damaged, dying, or necrotic tissues despite normal blood calcium levels.
Tuberculosis
Atheroma, infarct
Fat necrosis (pancreatitis)
Gross morphology of calcium accumulation
Hard, yellow nodules
Microscopic morphology of calcium accumulation
chunky, smooth, purple granules
CELLULAR ACCUMULATIONS - PROTEIN
Gross and microscopic morphology of protein accumulation
Gross morphology: blue-black foci on tissue once stained.
Microscopic morphology:
Amyloidosis: amyloid deposits
stain eosinophilic/pink-pale; pink
or red on Congo red stain
Alzheimer’s disease:
neurofibrillary tangles
Fatty liver: Mallory hyaline-
eosinophilic, pink, rope-like
deposits
Two type of calcium accumulation
dystrophic and metastatic
patients who have hypercalcemia have deposition of calcium within normal or abnormal tissue
Mechanism of metastatic calcification- form of calcium accumulation.
patients who have normal levels of calcium have deposition of calcium only within abnormal tissue (necrosis or damage)
Mechanism of dystrophic calcification:
Sites of abnormal tissue:
Tuberculosis
Atheroma, infarct
Fat necrosis (pancreatitis)
Sites of accumulation of calcium
Organs affected: vasculature, kidneys, lung
Mechanism of formation of protein?
Increased protein absorption in proximal renal tubule (renal disease)
Increased cytoskeletal proteins
Neurofibrillary tangles (Alzheimer’s disease)
Intermediate filaments (Mallory hyaline) in the liver due to alcoholism, fatty liver
Increased protein production
Defect in intracellular transport and protein secretion
Abnormal proteins (protein aggregation diseases)- amyloidosis
Mechanism of iron accumulation:
accumulation of hemosiderin due to ↑ iron
Sites of accumulation of Iron
liver, skin, pancreas, heart
accumulation of iron in organs without resultant side effects
Hemosiderosis
Accumulation of iron in parenchymal cells resulting in side
effects (e.g. DM, cirrhosis)
Hemochromatosis
Organs affected by hemochromatosis: liver, skin, pancreas, heart
Gross morphology of Iron accumulations
Gross morphology: dark brown color
Microscopic morphology of Iron accumulation
chunky, yellow-brown granules on H & E stain; blue on Prussian blue stain.
mechanism of of formation of fat accumulation (steatosis)
Intrinsic abnormality in fat metabolism.
Can indicate reversible damage.
Sites of accumulation of Fat (steatosis)
Organs affected: liver, kidney, heart, skeletal muscle
Gross and Microscopic morphology of Steatosis
Gross morphology: yellow discoloration of an organ.
Microscopic morphology: one or several clear vacuoles within the cell.
Mechanism of cholesterol accumulation
Hypercholesterolemia: elevated blood cholesterol levels lead to disruption in cellular function, oxidative stress, inflammation.
Sites of Cholesterol Accumulation
Organs affected: blood vessels (atherosclerosis)
CHOLESTEROL- GROSS & MICROSCOPIC MORPHOLOGY
Gross morphology: yellow discoloration of an organ
Microscopic morphology: foam cells (lipid-laden macrophages)
mechanism of accumulation- Glycogen
accumulates due to glycogen storage disorders or disease of glucose metabolism.
Sites of accumulation of glycogen
Organs affected: liver and skeletal muscle
Microscopic morphology of Glycogen accumulation
clear vacuoles in the cytoplasm
Gross morphology of glycogen accumulation
Gross morphology: Usually no obvious changes visible to the naked eye.
Mechanism of accumulation of pigments
Pigments are colored substances that accumulate in cells. They can be endogenous (made by the body) or exogenous (from outside the body).
Sites of Pigment accumulation
skin, eyes
Necessary for chromosomal integrity and genomic stability
Telomere
Telomeres get progressively shorter with each cell division until cells become senescent or die.
Cellular aging occurs partly because telomeres shorten with each cell division, eventually causing cells to stop dividing (senescence) or die.
Telomere biology disorders
(dyskeratosis congenita, progeria)