Drugs and glucose handling
1/15
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
16 Terms
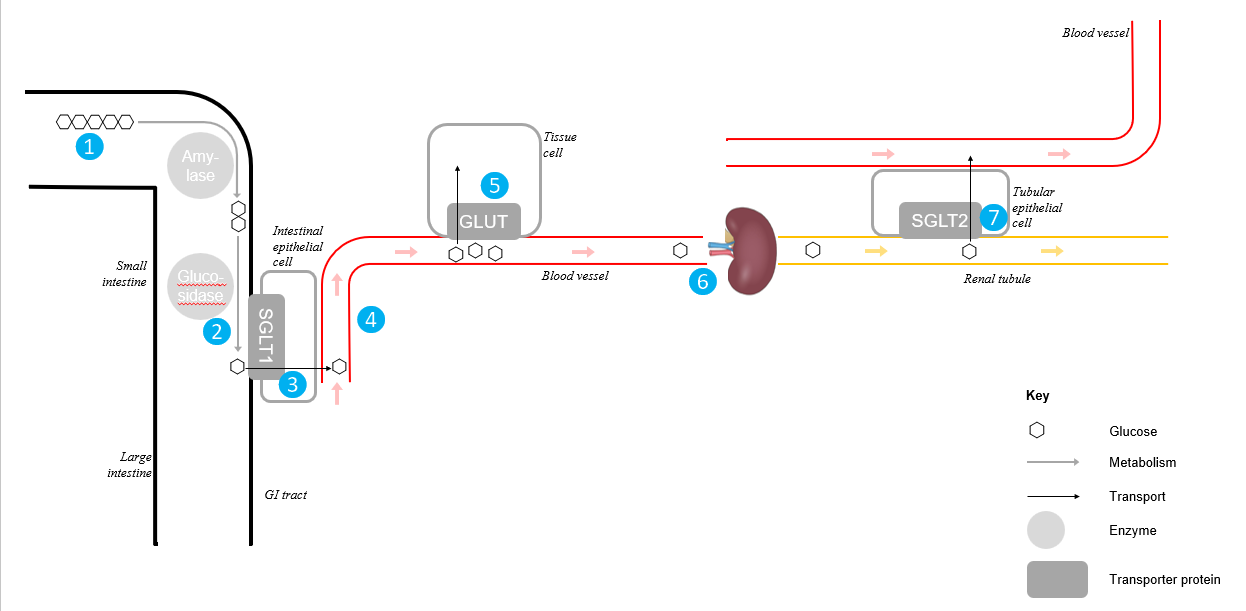
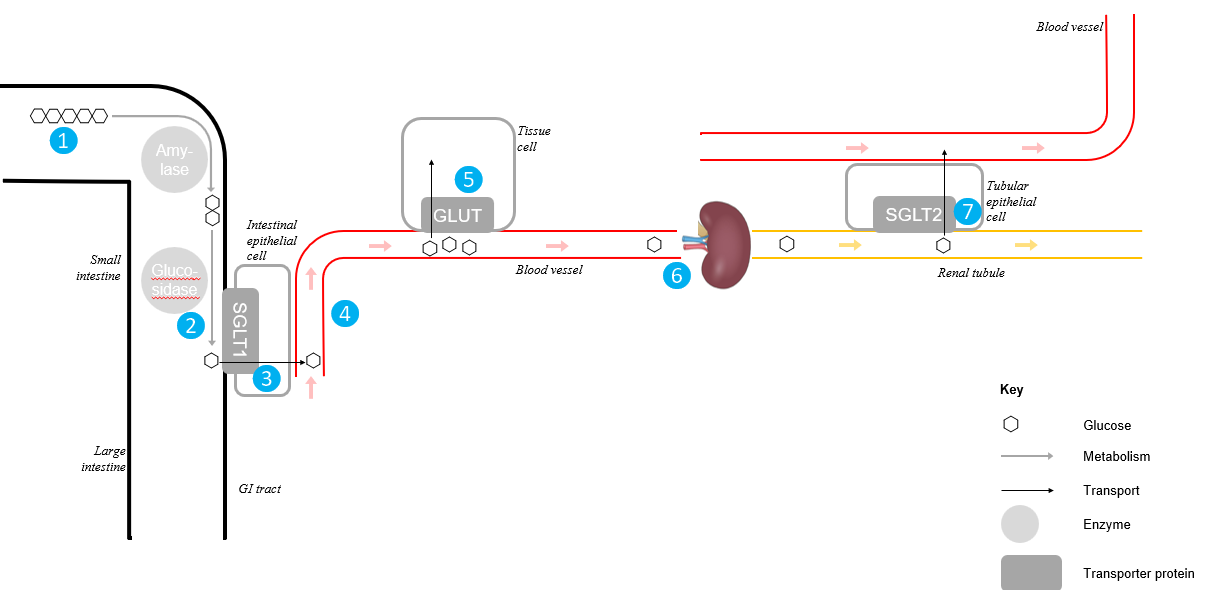
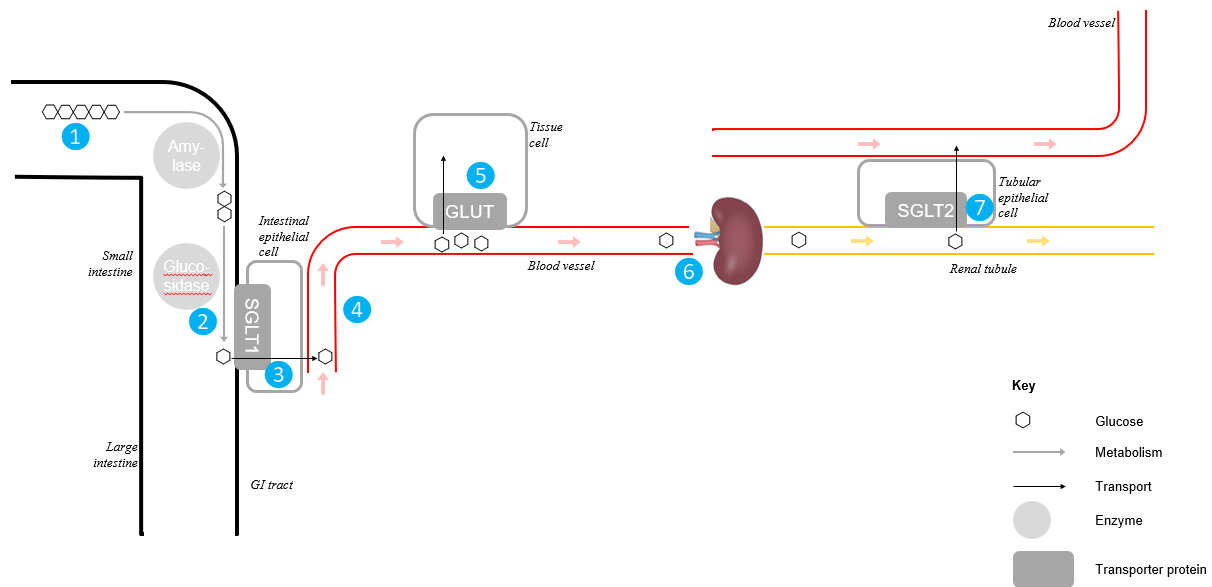
❶ Polysaccharides (mostly starch) are ingested
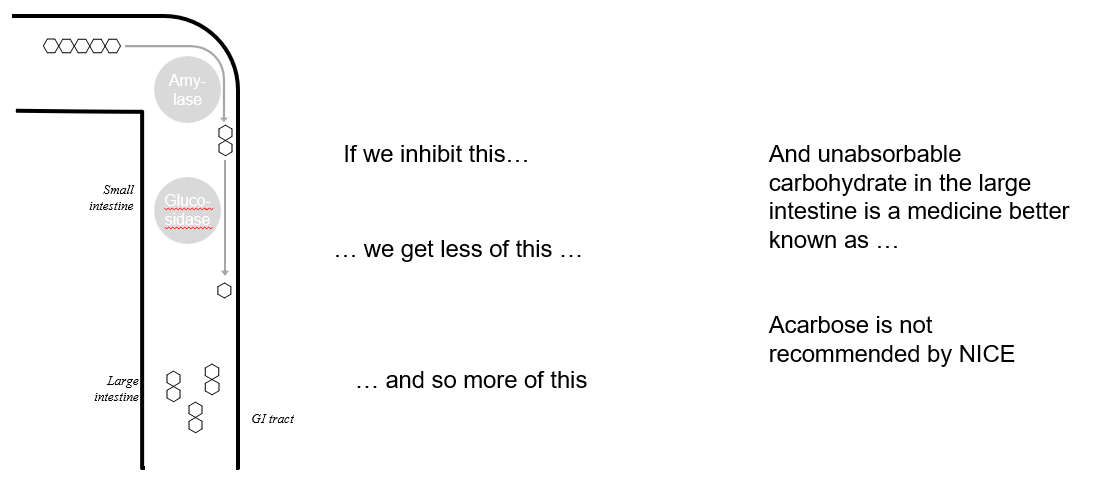
❷ Hydrolysis of polysaccharides by amylases and glucosidases yield monosaccharides
❸ Monosaccharides (e.g. glucose) are absorbed from the small intestine using the SGLT1 transporter. From the gut epithelial cells the glucose enters the blood
❹ Monosaccharides circulate in the blood
❺ When tissues (e.g. muscle, liver, heart…) need glucose they import it from the blood using the GLUT transporters
❻ Glucose remaining in the blood arrives at the kidney and passes into the glomerular filtrate
❼ Rather than be excreted in the urine, glucose in the glomerular filtrate is reabsorbed (ultimately to the blood) using the SGLT2 transporter
What would happen if we inhibited …
… glucosidases?
… SGLT1
… the GLUT transporters?
… SGLT2?
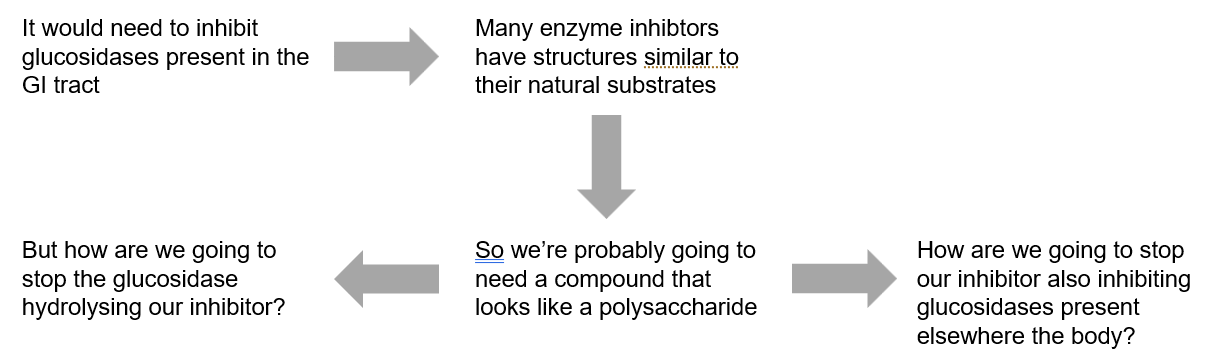
What properties would a glucosidase inhibitor need?
Acarbose
Isolated from a bacterium
Ki = 62 μM against MGAM – one of the key gut glucosidases
This is the bit that binds to the enzyme’s active site
Almost certainly not selective, but bioavailability is 2%
Taken with food
Not recommended by NICE
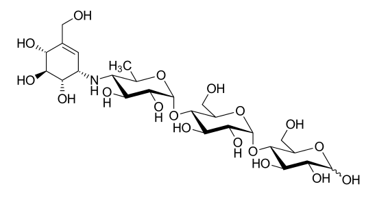
Acarbose problem
Targeting GLUTs
Inhibiting glucose uptake by tissues
Targeting the GLUT transporters is a terrible idea because the patient already has an impaired ability to handle glucose blood glucose levels will increase, potentially making the patient’s diabetes worse and you starve some or all tissues of glucose
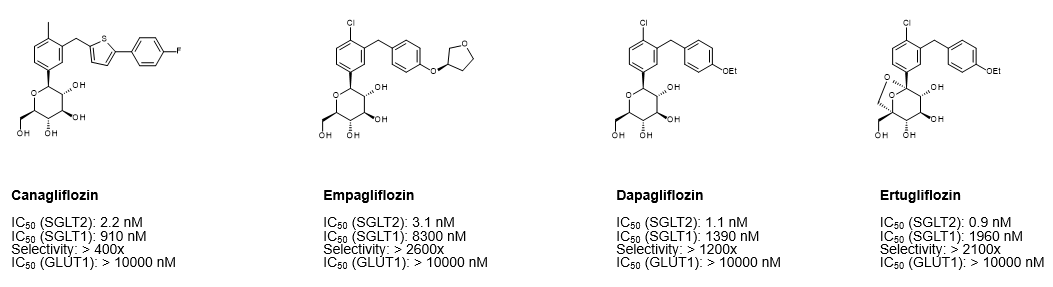
Targeting SGLT2
Inhibit glucose reuptake in kidney
Targeting SGLT transporters potentially increases glucose in the urine correspondingly decreases glucose in the blood
So a drug that inhibits SGLT2 sounds like a good idea. What would we need to make it work?
We need a drug that
Binds SGLT2 more strongly than glucose does
Does not inhibit any of the GLUTs (for reasons we’ve already talked about)
Does not inhibit SGLT1
In other words our inhibitor needs to be potent and selective.
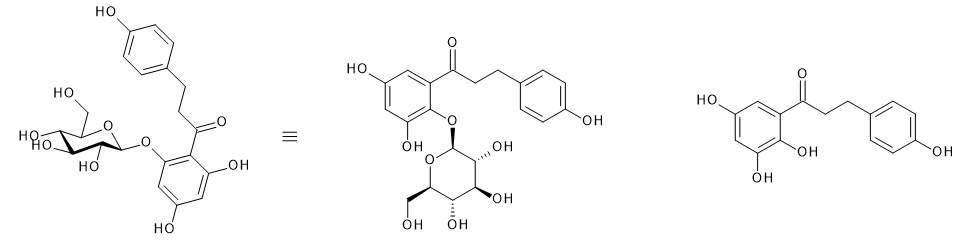
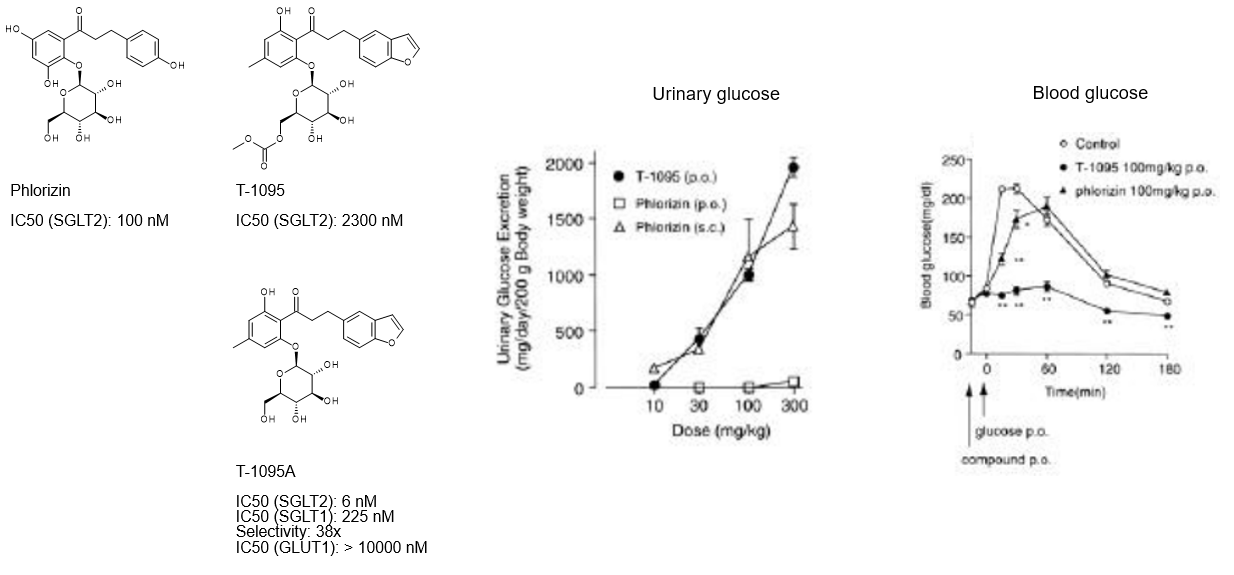
Phlorizin and Phloretin
Phlorizin
Derived from apple tree bark
Known to produce glycosuria since 1886
Identified as SGLT2 inhibitor in 1973
Inactive at GLUTs
Binds to SGLT2 more potently than glucose does.
Explains why the compound gives glycosuria
Implies the aglycone contributes to binding.
Phloretin
Inhibits GLUT transporters
Can we improve phlorizin?
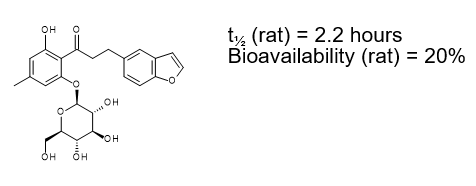
But T-1095 never made it to market
Reasons have never been disclosed, but hydrolysis to glucose and the aglycone is as good a guess as any
Phlorizin and T-1095 show us that
You can gain potency and retain selectivity by changing the aglycone
in vitro potency does not always translate to in vivo efficacy
So if the O-glucose bond is the problem
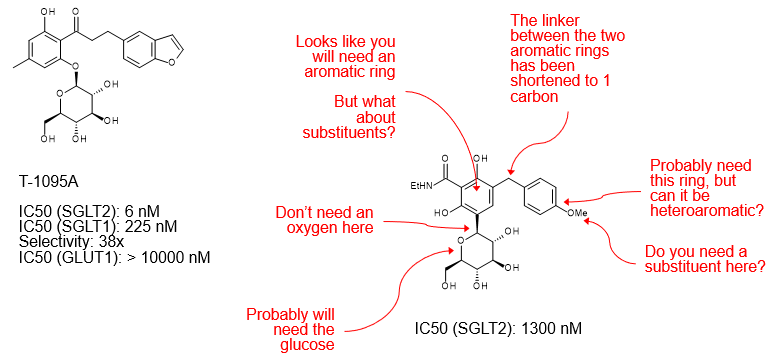
Let’s make some changes
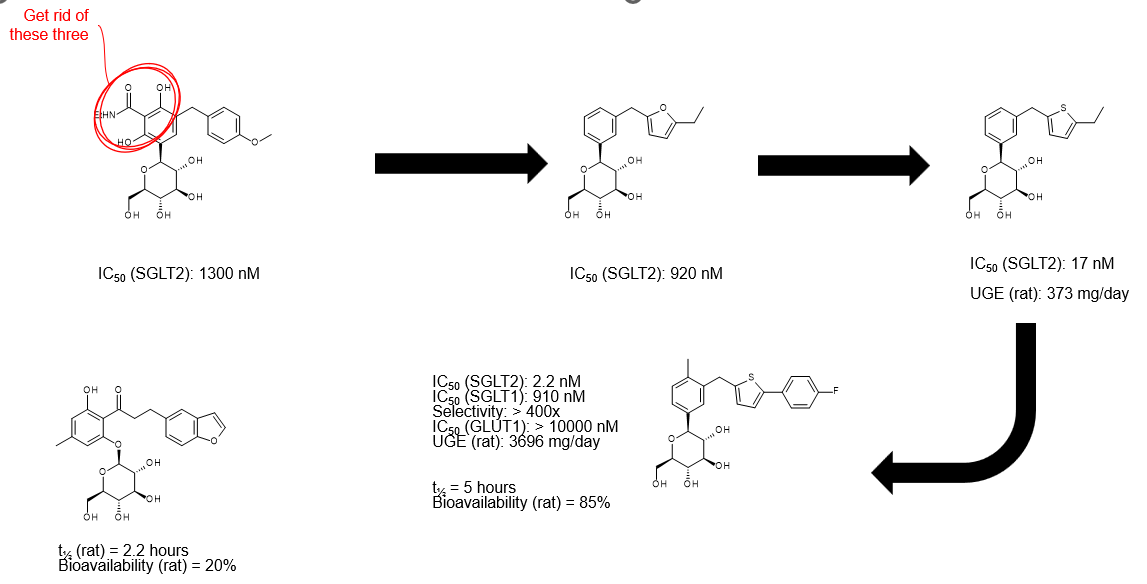
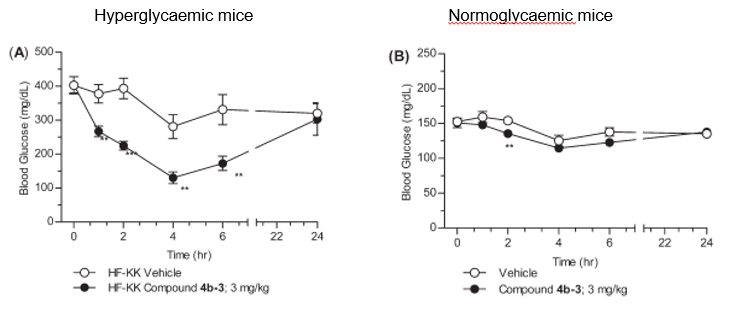
But what about in vivo?
We have been following the discovery of…