RPD Technique Manual Section 1
1/78
Earn XP
Description and Tags
Examination of the Partially Edentulous Patient
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
79 Terms
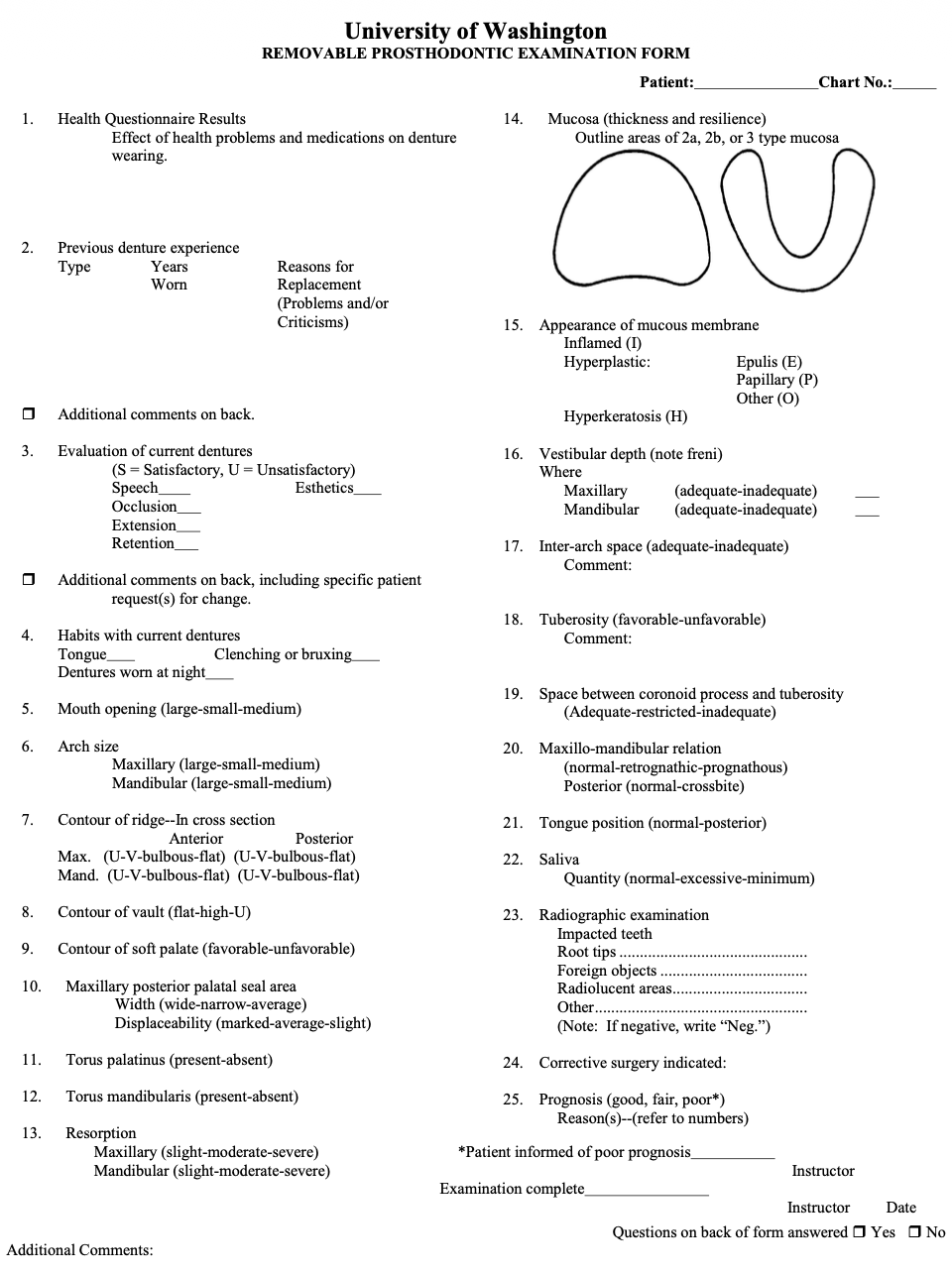
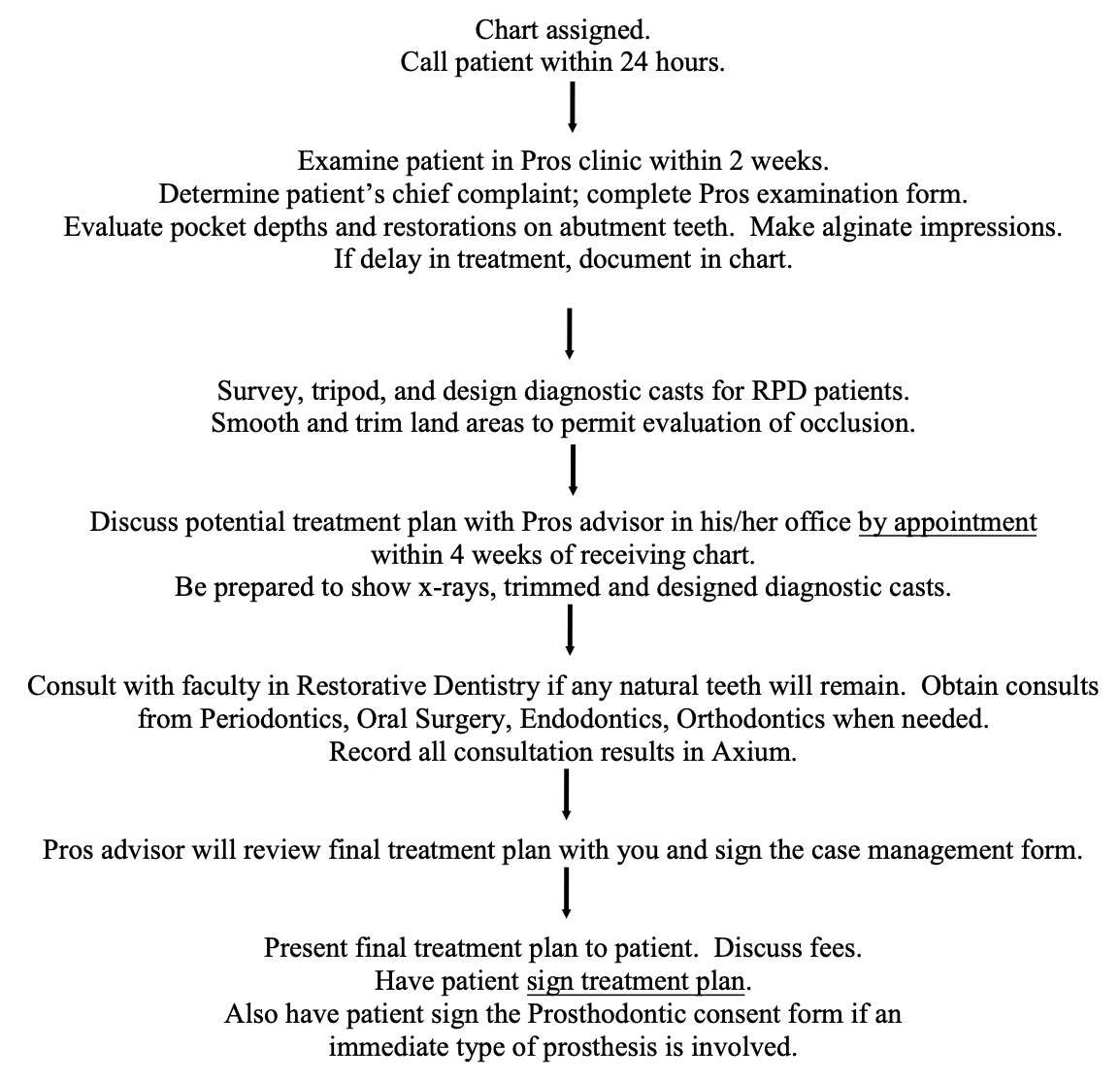
The first step in treating a partially edentulous patient is conducting a comp exam. What needs to be done during this appointment?
Review med history, examine mouth, complete RPD exam form, obtain alginate impressions for diagnostic casts
What can you do at the comp exam if you see caries or bone loss?
Consider a nutritional assessment
Should you take an impression of the opposing completely edentulous arch at the initial comp exam?
It can be delayed until later
How does a patient's medical health affect satisfaction with a mandibular RPD?
Patients with chronic health problems are less able to adapt to RPD-related frustrations and are nearly twice as likely to be dissatisfied compared with healthier patients. Consider alternatives or discuss expectations before treatment
Why might a patient who was successful with a previous RPD be unsuccessful with a new RPD?
The patient may now have fewer teeth, poorer health, or may be unable to tolerate the increased bulk of the new prosthesis
What are two possible reasons a patient has had multiple unsuccessful RPDs?
Inability to adapt to the inconvenience of wearing an RPD.
Failure due to caries or periodontal disease affecting abutment teeth.
Why is it important to know the type of previous RPD appliance a patient wore?
The type of prosthesis (temporary acrylic vs. conventional metal RPD) may help explain the severity of current disease and/or reasons for past success or failure
It is helpful to note the patient’s problems or criticisms with their previous dental care or previous RPD. Arch size affects the relationship of the edentulous ridges to each other. Why may problems arise if the max arch is small and edentulous and mand arch is large and partially dentated?
Esthetic arrangement of maxillary ant teeth will be difficult to accomplish
Force delivered to a small edentulous ridge may result in soreness and/or alveolar bone resorption
Why might a bulbous ridge or any ridge with substantial undercut areas create problems with an RPD?
Because of the definite path of insertion and removal of partial dentures in contrast to a complete denture. Surgical correction should definitely be considered. However, excessive relief can result in unesthetic lip contour and space for food to collect
Torus palatinus can create problems in the placement of a maxillary major connector, what can be done about that?
Surgical removal BUT usually an anterior-posterior bar major connector design that doesn’t cover the torus is all that is needed
Torus mandibularis usually creates an undercut and is covered with very thin tissue. What can this result in?
Soreness in class I or II RPD, especially if the torus is located distal to abutment tooth so RPD can “settle” onto torus.
In which Kennedy Classification is torus mandibularis usually not a problem?
Class III
What if a patient does not want to undergo surgery to remove torus mandibularis?
A lingual plate could be used to stay above the torus rather than trying to cover to with a lingual bar

What support discrepancy is magnified by 2b tissue in distal extension RPDs?
The difference between rigid tooth support and compressible soft-tissue support

Why can 2a tissue worsen problems with soft-tissue undercuts?
Because the tissue is minimally displaceable and cannot flex around the denture framework
Why is gingival recession important when designing an RPD?
It can affect the location of undercuts and influence clasp placement and design
What does inflammation or tissue changes in edentulous areas suggest?
A poor tissue response to a previous appliance, often due to an ill-fitting denture or RPD
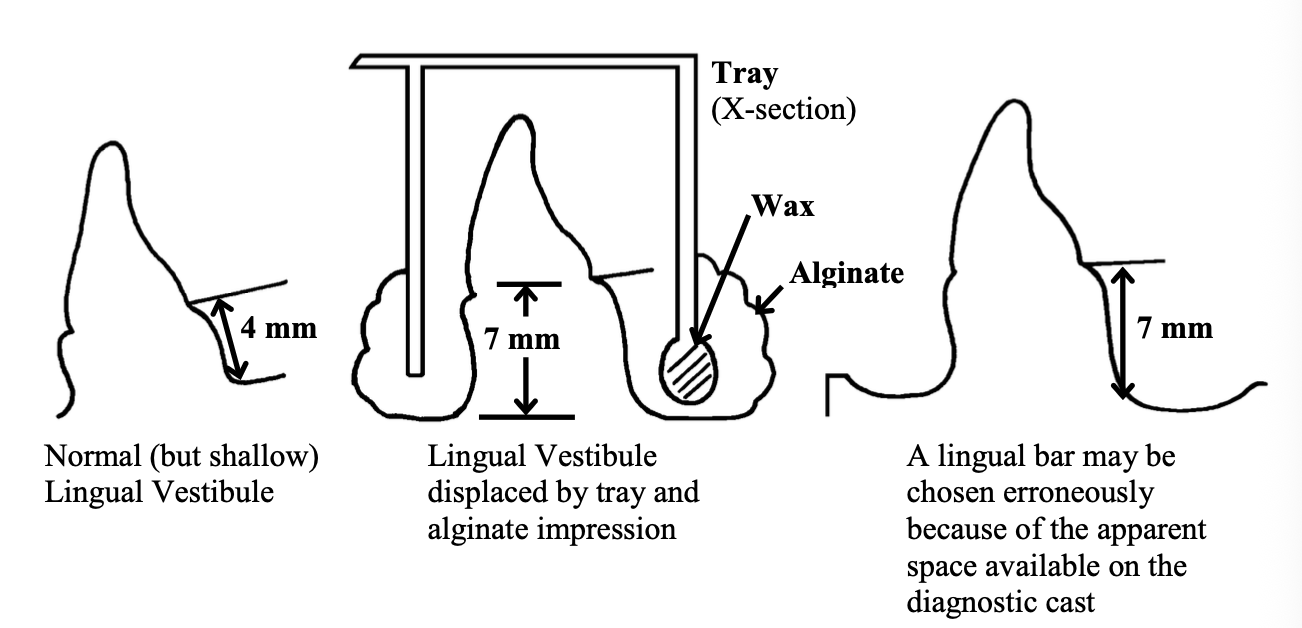
The anterior lingual area of the mandible is often not evaluated adequately during an examination because it's hard to see. How do you evaluate the area?
Put a mirror between tongue and vestibule
Tell pt to elevate tongue - determine the functional level of vestibule + lingual frenum
Use a probe to measure distance from gingival margin to functional level of vestibule
The choice of major connector (lingual bar vs. lingual plate) depends on the amount of space available.
Normal vestibule is 4mm, but alginate captures displaced tissue at 7mm. Now u chose a lingual bar because u thought u had space

Which anatomical structures are especially important to evaluate before fabricating a swing-lock RPD?
The labial frenum and buccal frena
Why must the labial vestibule be measured when planning a swing-lock RPD?
To ensure proper placement of the labial bar without interfering with soft tissue function
How does a flat, resorbed distal extension ridge affect an RPD?
It provides less support. More movement of the RPD can be expected
What does movement of the RPD do? What can you do in the maxillary and mandibular posterior areas to combat the movement?
Movement places added force on the abutment teeth. Splinting of abutment teeth should be considered
What are the two most common causes of inadequate inter-arch space?
Low tuberosities
Excess eruption of an opposing tooth
How can a dentist evaluate the amount of space available in the posterior part of the mouth - tuberosity?
Dentist observes whether one or both tuberosities project below the remainder of the maxillary arch
Ask the pt to let jaw assume rest position while dentist separates the lips to observe how much space is available. 5-6mm is needed
What does a prominent-appearing tuberosity mean?
There is a lack of space for prosthetic appliances
What is the fate for an extruded tooth?
Extraction or recontouring + restore OR endo for adequate correction of length
Why can overclosure create limited restorative space?
Loss of vertical stop; loss of VDO, and maybe the bite collapsed
In which situation is correcting overclosure usually more difficult: CD/RPD or NAT/RPD?
NAT/RPD (or RPD/RPD), because extensive restorative dentistry is often required
What is maxillo-mandibular relations?
The antero-posterior relation of the mandible to the maxilla in CR.
What if a patient has retrognathic maxillo-mandibular relation?
Occlusal balance is difficult to achieve. Patients occlude varying distance anterior to CR, deep anterior vertical overlap. Interocclusal rest space is often greater than 3mm
What if a patient has prognathic maxillomandibular relation?
Results in posterior crossbite. Stability of opposing CD may be poor be anterior teeth have to be positioned forward of the ridge
What if a patient has normal maxillo-mandibular relation?
Mandible will function at or near CR
What factors should be considered when determining the prognosis for an RPD?
Medical history, dental history, oral hygiene, patient expectations, mechanical challenges, motivation, and ability to adapt to the prosthesis
What should be done if a poor prognosis is assigned?
Document the reasons, record supporting findings, and ensure the patient is informed and the discussion is documented
What is the ideal crown-root ratio for an RPD abutment tooth?
1:3
What is the minimum generally acceptable crown-root ratio for an abutment tooth?
1:1
Why is a 2:1 crown-root ratio unfavorable?
The crown is longer than the root supported by bone, creating a lever effect and reducing tooth stability
What is the most common cause of an unfavorable crown-root ratio?
Periodontal disease with subsequent alveolar bone loss
What treatment options may be considered for an abutment tooth with an unfavorable crown-root ratio?
Extraction, splinting, swing-lock RPD design, or additional rests on adjacent teeth
Why are short, conical roots considered unfavorable abutments for RPDs?
Does not effectively resist forces directed to the tooth (ex. mand first and second premolar) splinting to adjacent tooth may be desirable
What are desirable roots to have as abutment teeth?
Longer, irregular shaped root (canine) or multiple roots (man first molar)
How does the lamina dura commonly change after a tooth has tipped and then stabilized?
Becomes thicker on the side toward which the tooth tipped
What does an irregular or poorly defined lamina dura suggest?
Adjacent missing tooth or traumatic occlusion
What are index areas?
Areas that indicate how well the bone holds up to additional stress
How can you determine if a patient has a “positive bone factor"?
If a patient has a favorable response to increased stress they have a better long-term prognosis since the abutment teeth will be subjected to additional loads
What does it mean if a patient has a “negative bone factor”?
Loss of bone due to added stress. The prognosis is poor due to increase in stress from the RPD.
To observe the lateral occlusal plane, have the patient at a slight distance while standing. If it does not harmonize with the horizon or interpupillary plane, you can determine if it is possible to change the plane. In which cases is it possible to change the level?
CD/RPD by reshaping the natural teeth and/or performing restorative dentistry.
When observing lateral relation of teeth to desirable occlusal plane, in which cases is it more difficult to change the plane? Why?
RPD/RPD or NAT/RPD because extensive restorative procedures are required in both arches
In CD/RPD cases, what teeth dictate the occlusal plane and can greatly affect the esthetics of the CD?
Mandibular premolars. The mandibular premolars will often be worn down by porcelain teeth on an old CD/.
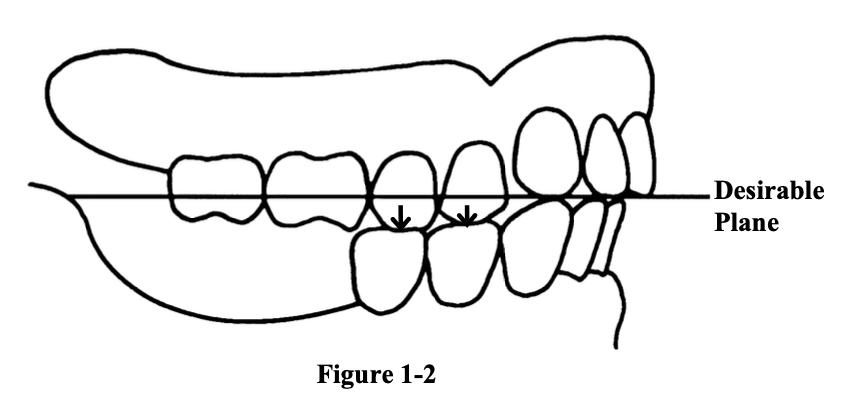
How can you estimate the amount of wear in the antero-posterior view of the occlusal plane?
Project a line from canine to middle of RPD. The buccal cusp tips of the premolars should be within 1-2mm of this line. If not, tooth position on new CD may not look good
What is the consequence if CR does not coincide with CO in RPD/RPD or NAT/RPD cases?
Occlusal adjustment can affect the placement of rests on RPD
What are some periodontal contraindications of creating a new RPD?
Extensive caries, periodontal disease, or a history of problems with previous RPDs
Why are patients with a unilateral loss of 1 or 2 molars not good candidates for an RPD?
Because the inconvenience of the RPD is greater than the chewing benefits, and the RPD is simply not worn
Even when the remaining teeth have a poor prognosis, when might an RPD still be indicated?
When the remaining natural teeth occlude against less than half of the supporting areas of the complete denture
What happens if a maxillary complete denture opposes only a few mandibular anterior teeth?
Occlusal forces become concentrated anteriorly
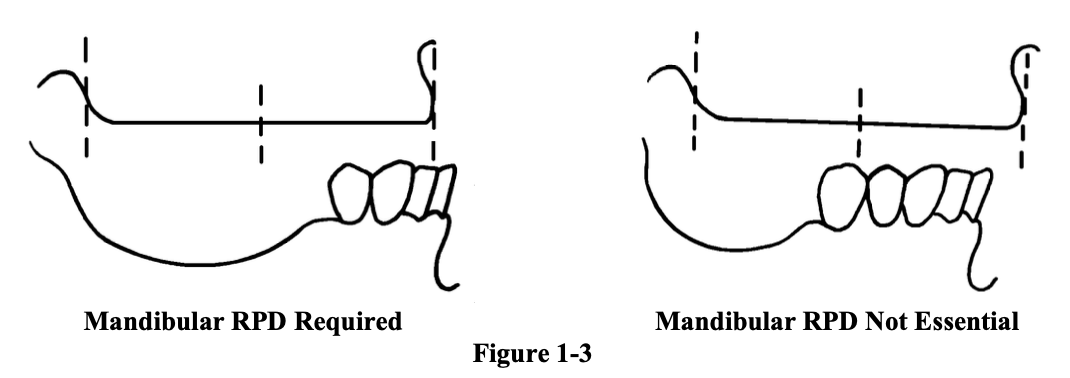
Not every patient with missing mandibular posterior teeth absolutely needs an RPD. In which jaw relationship can patients manage nicely without an RPD?
Class II
Relation of plaque to RPD success
Good oral hygiene, careful design and construction of RPD is essential for favorable long-term results with an RPD
Should you place a tissue conditioner in the old denture at the initial appointment?
No, tissue conditioner must be replaced periodically. It is better done closer to the final impression appointment, but only consider it if retention is an urgent problem
Why shouldn't RPD patients use a Calgon-Clorox soak?
Clorox corrodes and blackens the metal framework
What denture cleanser is recommended for CDs and RPDs?
Fixodent Denture Cleanser becuase it is safe, effective, and does not damage metal
Why are RPD patients often placed on 0.4% stannous fluoride gel?
To reduce caries risk on the remaining natural teeth
What OTC fluoride rinses are recommended if active caries are present?
ACT or FluoriGard
Steps in treatment planning prosthodontic patients
What effect will patient’s health or medications have on use of a denture or retention of natural teeth?
Poor health = poorer prognosis and greater likelihood of dissatisfaction
What impact will patient's previous denture experience have on use of a new denture?
Previous failures may reflect patient factors rather than prosthesis factors
How likely can the problems identified with the natural teeth or in the current dentures be solved with a new prosthesis?
Evaluate whether the patient's complaints can be correlated with mechanical deficiencies in the existing prosthesis and whether those deficiencies can realistically be corrected. The prognosis depends on whether the new prosthesis is likely to improve speech, esthetics, comfort, function
Will habits create problems with new dentures?
Evaluate tongue size and position, clenching, bruxism, night-time denture wear. Bruxism and clenching increase forces on dentures and abutment teeth. Tongue position may affect retention and stability. Night-time wear may increase tissue irritation and inflammation
How does arch size contribute to failure of a new prosthesis?
Small maxillary arches may cause esthetic problems and increased ridge loading
How does ridge contour contribute to failure of a new prosthesis?
Bulbous ridges and severe undercuts may interfere with the path of insertion and may require surgery
How does mucosa contribute to failure of a new prosthesis?
Type 2b tissue in Class I and II RPDs increases denture movement and stress on abutment teeth
How does torus palatinus contribute to failure of a new prosthesis?
May create soreness and interfere with major connector placement
How does vestibular depth and frena contribute to failure of a new prosthesis?
May affect lingual bar, lingual plate, or swing-lock design
How do tuberosities and interarch space contribute to failure of a new prosthesis?
Low tuberosities and supraerupted teeth can limit prosthetic space
What preprosthetic surgery is needed?
Removal of bulbous ridges or severe undercuts
Torus palatinus removal when major connector placement is compromised
Torus mandibularis removal when soreness or interference is expected
Tuberosity reduction
Removal of impacted teeth, root tips, or other radiographic findings
Surgical correction of inadequate interarch space when indicated
What treatment of the mucosa is needed before constructing a new prosthesis?
Patients should receive oral hygiene instruction and denture cleaning instruction. Tissue conditioning may be indicated before final impressions if tissues are inflamed or distorted
Which teeth are suitable for use as abutment teeth? Are surveyed crowns necessary?
Teeth with crown:root ratio (Ideal = 1:3), long roots or multirooted roots, good bone levels. Surveyed crowns may be necessary when guide planes are inadequate, undercuts are unfavorable, tooth contour is unsuitable for clasping
What kind of record is necessary to occlude the diagnostic casts?
In NAT/RPD or RPD/RPD: check if centric relation coincides with centric occlusion. In CD/RPD more extensive jaw relation records may be needed