Lecture 16 and 17: Heart Failure with Reduced and Preserved Ejection Fraction
1/63
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
64 Terms
Heart Failure
inability of the heart to maintain sufficient cardiac output to perfuse the vital organs
Systolic Heart Failure
Systolic or Diastolic HF:
-impaired myocardial contractility
-dilated heart
Systolic Heart Failure
Systolic or Diastolic HF:
-reduced ejection fraction
Diastolic Heart Failure
Systolic or Diastolic HF:
-normal ejection fraction
Diastolic Heart Failure
Systolic or Diastolic HF:
-impaired relaxation and filling
-hypertrophied heart
Systolic Heart Failure
Systolic or Diastolic HF:
-volume overload
Diastolic Heart Failure
Systolic or Diastolic HF:
-Pressure overload
Right
pulmonary arterial hypertension -----> _______ Heart Failure
Left
stenoses or malignant hypertension -----> _______ Heart Failure
Left Heart Failure
most common cause of right heart failure
1. The adrenergic nervous system
2. RAAS
3. Increased production of antidiuretic hormone (ADH)
the three compensatory mechanisms for reduced CO
HFpEF
Decreases
Diastolic Heart Failure __________________ Compliance
Diastolic Heart Failure
• Ventricular concentric hypertrophy decreases ventricular compliance
• Ventricular filling pressure increases which lead to decreased ventricular filling and increased LVEDP.
• LV ---> Increased left atrial and pulmonary venous pressure ---> pulmonary congestion ---> pulmonary edema
• RV ---> Increased RAP and systemic venous pressure ---> peripheral edema
Sympathetics and RAAS
In Diastolic Heart Failure, decreased arterial BP leads to activation of _________________ and _____________
Left
Left or Right-sided HF:
-dyspnea
-orthopnea
-pasozysmal nocturnal dyspnea
-fatigue
Left
Left or Right-sided HF:
-diaphoresis
-tachycardia
-pulmonary crackles
-loud P2
-S3 gallop (in systolic dysfunction)
-S4 gallop (in diastolic dysfunction)
Right
Left or Right-sided HF:
-peripheral edema
-right upper quadrant pain
-hepatic enlargement
Right
Left or Right-sided HF:
-jugular venous distension
-hepatomegaly
-peripheral edema
Dyspnea
pulmonary edema, shunt, and hypercarbia leads to ______________
Orthopnea
dyspnea that occurs when lying flat and is relived by elevation of the head with pillows
- paroxysmal nocturnal dyspnea or orthopnea
- jugular vein distention
- rales (crackles, whistling, sloshing)
- cardiomegaly
- acute pulmonary edema
- S3 gallop
- increased venous pressure >16 cm
- circulation time >25 sec
- hepatojugular reflux
according to Framingham Criteria, what are some major criteria for heart failure
- ankle edema
- night cough
- dyspnea on exertion
- hepatomegaly
- pleural effusion
- vital capacity decreased 1/3 from maximum
- tachycardia (>120)
according to Framingham Criteria, what are some minor criteria for heart failure
(2) major or (1) major and (2) minor criteria
what is the Framingham criteria requirements for diagnosing heart failure?
Echocardiogram
the best single diagnostic test for assessment of valves and ventricular function
• Wall thickness
• Chamber size
• Wall motion abnormalities
• Valvular structure and function
• Ejection fraction
• Pericardial effusion
what are some echocardiogram findings that are indicative of Heart Failure?
• Cardiomegaly (including chambers)
• Pulmonary vascular redistribution
• Pleural effusion
• Kerley B lines
what are some CXR findings that are indicative of Heart Failure?
Cardiac Catheterization
best assessment of coronary arteries and hemodynamic function
Cardiac Catheterization
- Assess presence of CAD
- Wall motion abnormalities
- Ejection fraction
- Assess intracardiac pressures
Exercise Testing
- Assess ischemia
- Assess exercise capacity
- Assess cardiac reserve (MaxVO2)
- Assess blood pressure and heart rate response to stress
- Hematocrit
- Thyroid function
- Neurohormones (research mainly)
- BNP
what things should you look at when blood testing that can be indicative of heart failure?
Class I
Classification of chronic heart failure:
-no limitation of physical activity
Class II
Classification of chronic heart failure:
-slight limitation of activity
-dyspnea and fatigue with moderate exertion
Class III
Classification of chronic heart failure:
-marked limitation of activity
-dyspnea with minimal exertion
Class IV
Classification of chronic heart failure:
-severe limitation of activity
-symptoms are present even at rest
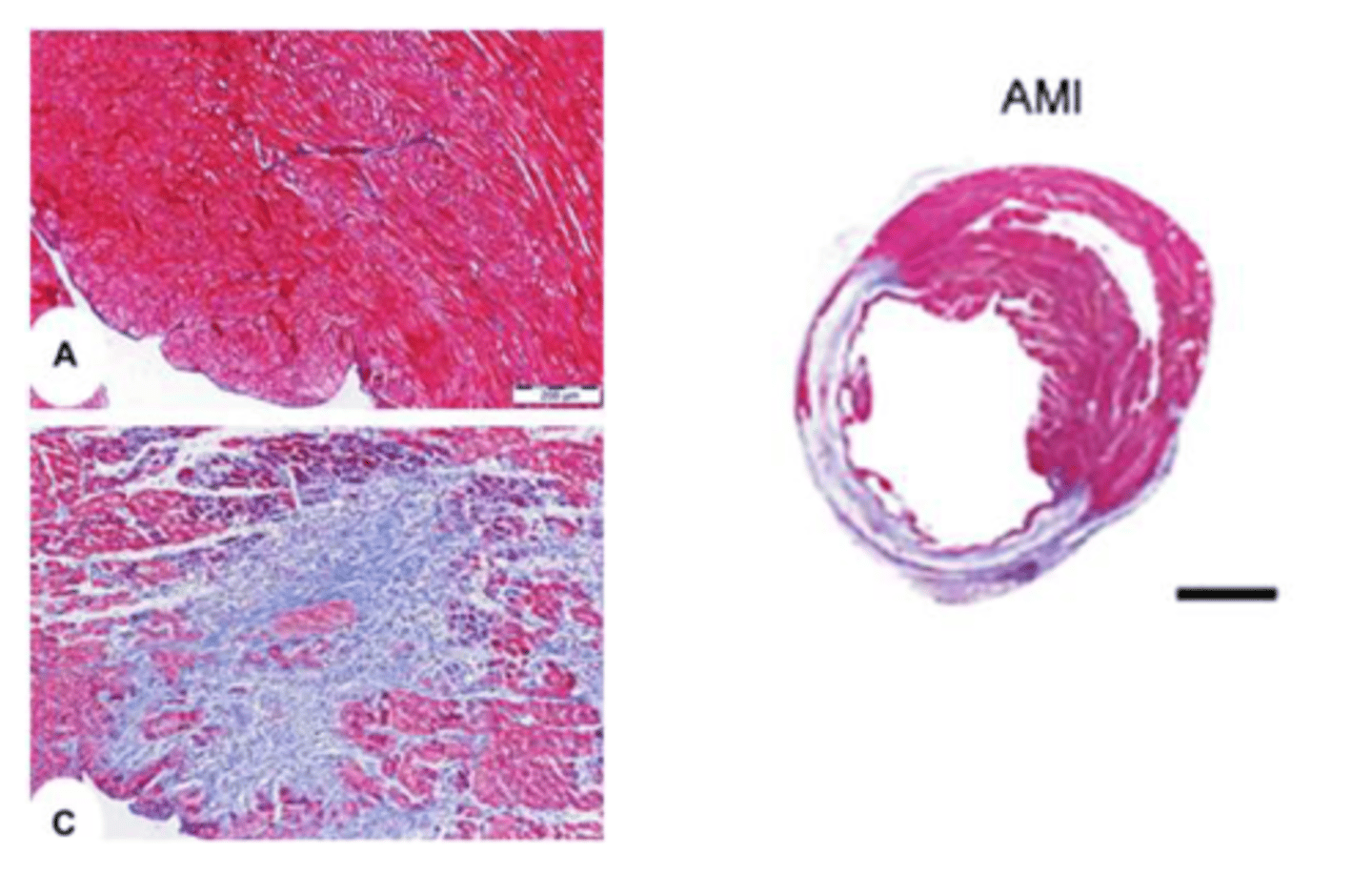
STEMI
• Injured and dying cells leak K+ into the extracellular space
• The Na+-K+ ATPase cannot maintain the K+ gradient in the injured cells
• Increased extracellular K+ causes peripheral healthy myocytes to depolarize
Local Reflex (short term compensatory mechanism for MI)
-increase in interstitial metabolites that allow all immediate resistance vessels to dilate reflexively
Central Reflex (short term compensatory mechanism for MI)
-death of myocytes impairs myocardial contractility
-reduction in SV adn CO
-decreased MAP
-trigger of baroreceptor reflex
decreased in MAP which activates RAAS
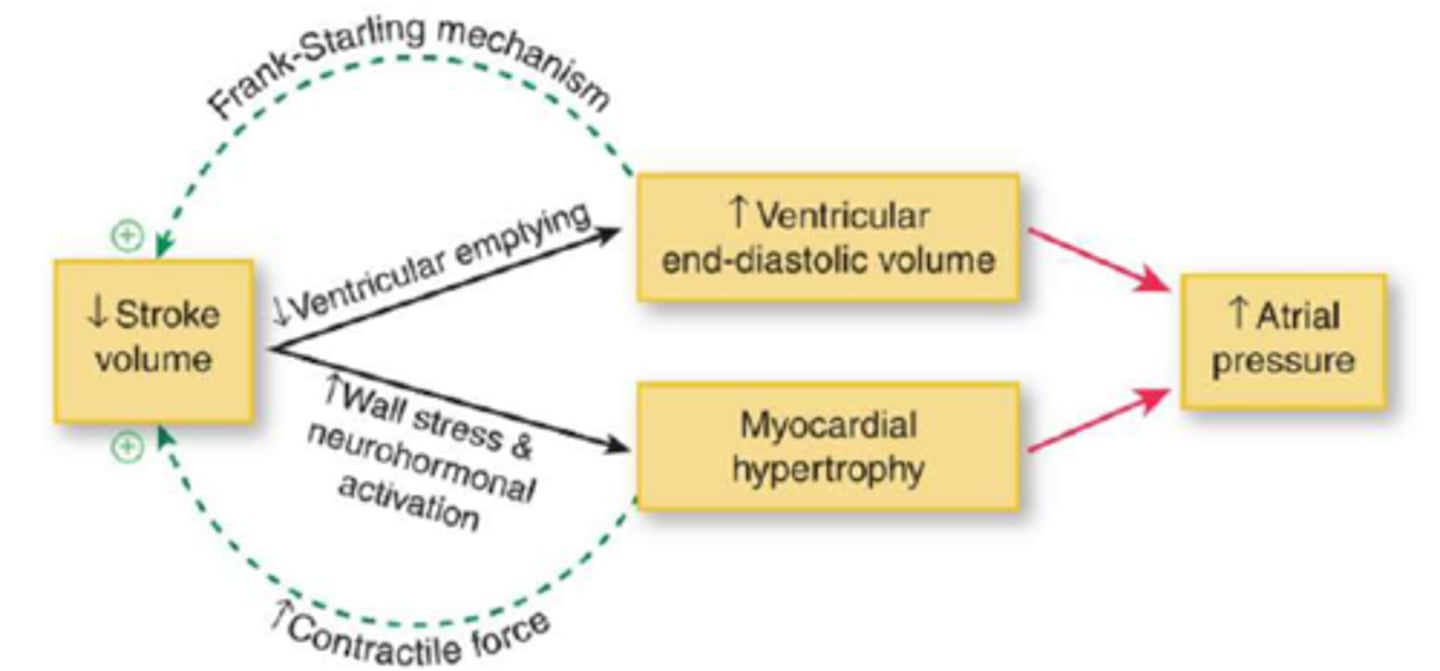
describe long term compensatory mechanism for MI
Preloading
____________________ the heart increases CO through length-dependent activation of sarcomeres
Increases
Preloading ________________ wall tension
Systolic Heart Failure
Preload penalty is associated with which HF?
Preloading
-increases wall stress
-predisposes myocardium to potentially fatal dysrhythmias and arrhythmias
-stretches and distorts cartilaginous valve rings and unseats the valves
-edema
filtration
CVP elevation raises mean capillary pressure (↑Pc) and favors _______________ from capillary into the interstitium
Pulmonary Congestion
fluid filters from pulmonary capillaries and collected in alveolar sacs where it interferes with gas exchange
Congestive Heart Failure
-retention of fluid to compensate for impaired EF and attempt to maintain sufficient tissue perfusion
-NaCl and water are retained due to increased RAAS aldosterone
ANP/BNP
the plasma level of ___________________ is increased in congestive heart failure
Systolic Heart Failure
-depressed left ventricular ejection fraction (LVEF)
-dilated/eccentric remodeling
-S3 gallop
-HFrEF
Coronary Artery Disease with subsequent myocardial damage
the most common cause of systolic heart failure
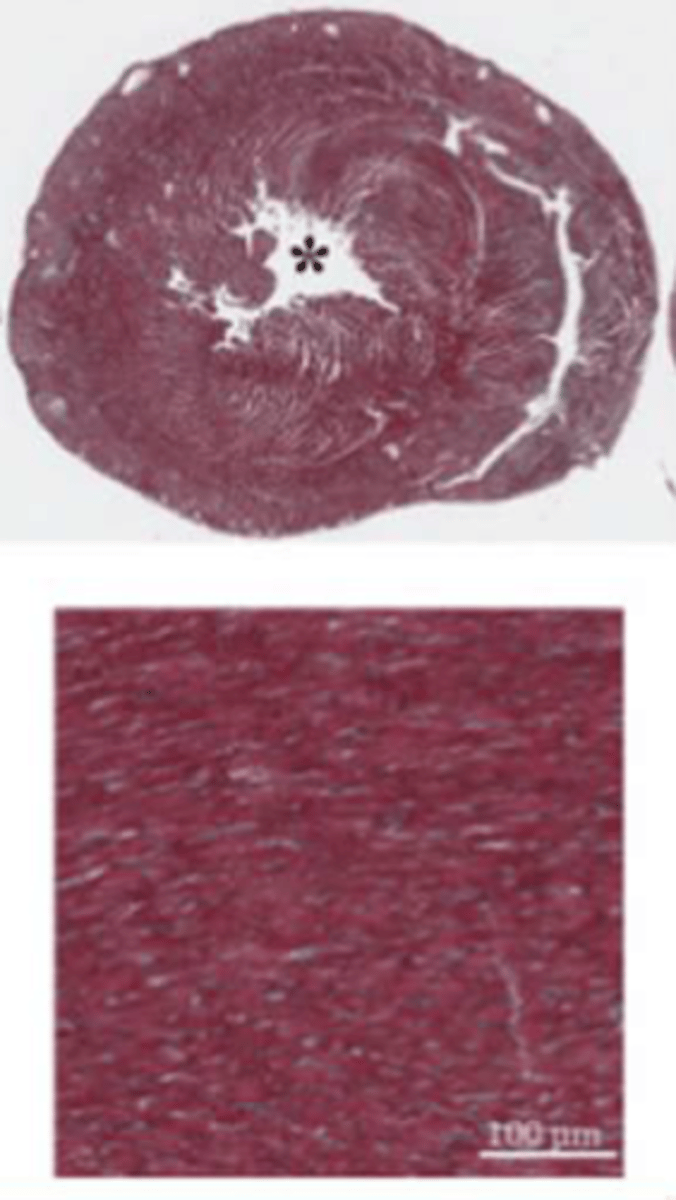
Systolic Heart Failure
Diastolic Heart Failure
-pressure overload induces concentric hypertrophy
-impaired filling
-decreased EDV
-increased contraction force
-increased afterload
-S4 heart sound
thick wall helps offset the effects of high IV pressure on wall stress
what is the advantage of cardiac hypertrophy
LaPlace's Law
P = 𝑟/2𝑇
Diastolic Heart Failure
Inhibits Na+/K+ ATPase
what is the mechanism of Digoxin
Digoxin
-causes an increase in intracellular sodium levels
-increases cytosolic calcium
-decreases HR
-increases SR calcium stores
-CICR of greater magnitude
-leads to increased contractility without increasing heart energy expenditure
ACE Inhibitors
first line therapy for systolic dysfunction
ACE Inhibitors
-prevents adverse remodeling
-improves afterload
-reduces risk for MU and progression of CHF
-may raise potassium, precipitate renal dysfunction in some cases, and cause dry cough
β-blockers
second line therapy in systolic dysfunction
β-blockers
-may raise RF by 10% or more
-for stable patients only
Inotropes
-increase contractility and CO
-oral and IV agents
Digoxin
all inotropes EXCEPT ___________________ increase mortality in CHF
Diuretics
• Needed by most patients to correct water retention
• Use minimum doses required to remove excess volume
• May cause magnesium/potassium depletion, raise uric acid levels, and induce gout, hyperlipidemia, and renal failure
ACEi
ARBs
Beta-blockers
Diurectics (edema)
initial therapies for HFrEF