MLS II 4.7: GU Malignancies
1/31
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
32 Terms
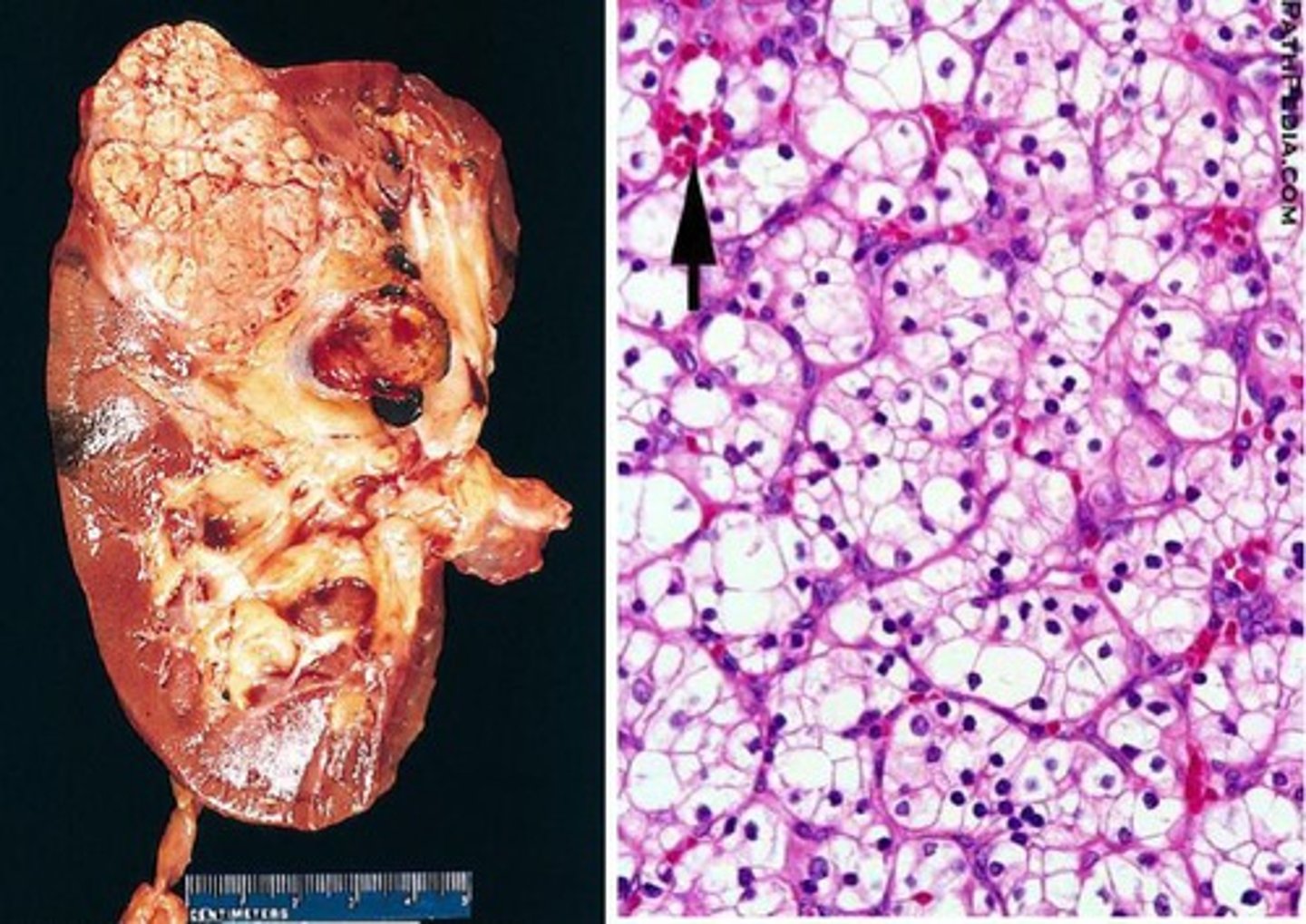
What is the most common type of primary renal cancer overall?
Renal cell carcinoma (RCC)
Do most cases of RCC have an identifiable cause? What is the biggest risk factor?
NO - the vast majority of cases are considered sporadic; if there is a risk factor, smoking is the biggest one
What are some possible RCC subtypes? Which is the most common?
Clear cell (most common), papillary, chromophobe, collecting duct, sarcomatoid
What is the classic triad of RCC s/sxs (even tho they only occur in ~10% of cases)? What are some others?
(1) Flank pain, (2) hematuria, (3) palpable abdominal mass; FUO, weight loss, L-sided scrotal varices, incidental finding on imaging (very common), paraneoplastic sxs
How is RCC diagnosed?
Abdominal CT w/ & w/o contrast plus delayed imaging, urine cytology, renal biopsy required for definitive diagnosis

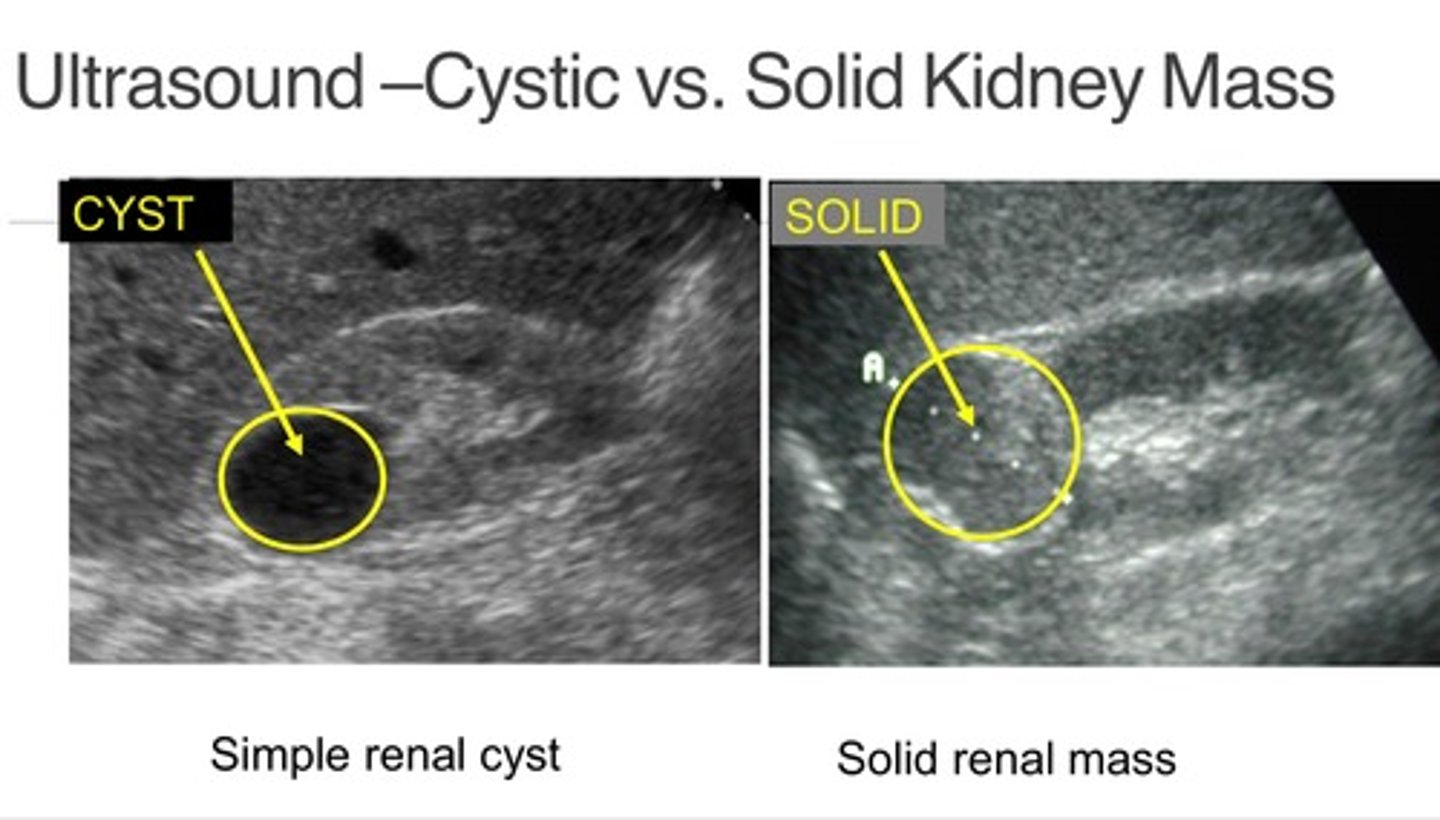
What is the difference between what renal cysts & a true renal mass will look like on ultrasound?
Cysts: hypoechoic & fluid-filled
Mass: hyperechoic & solid
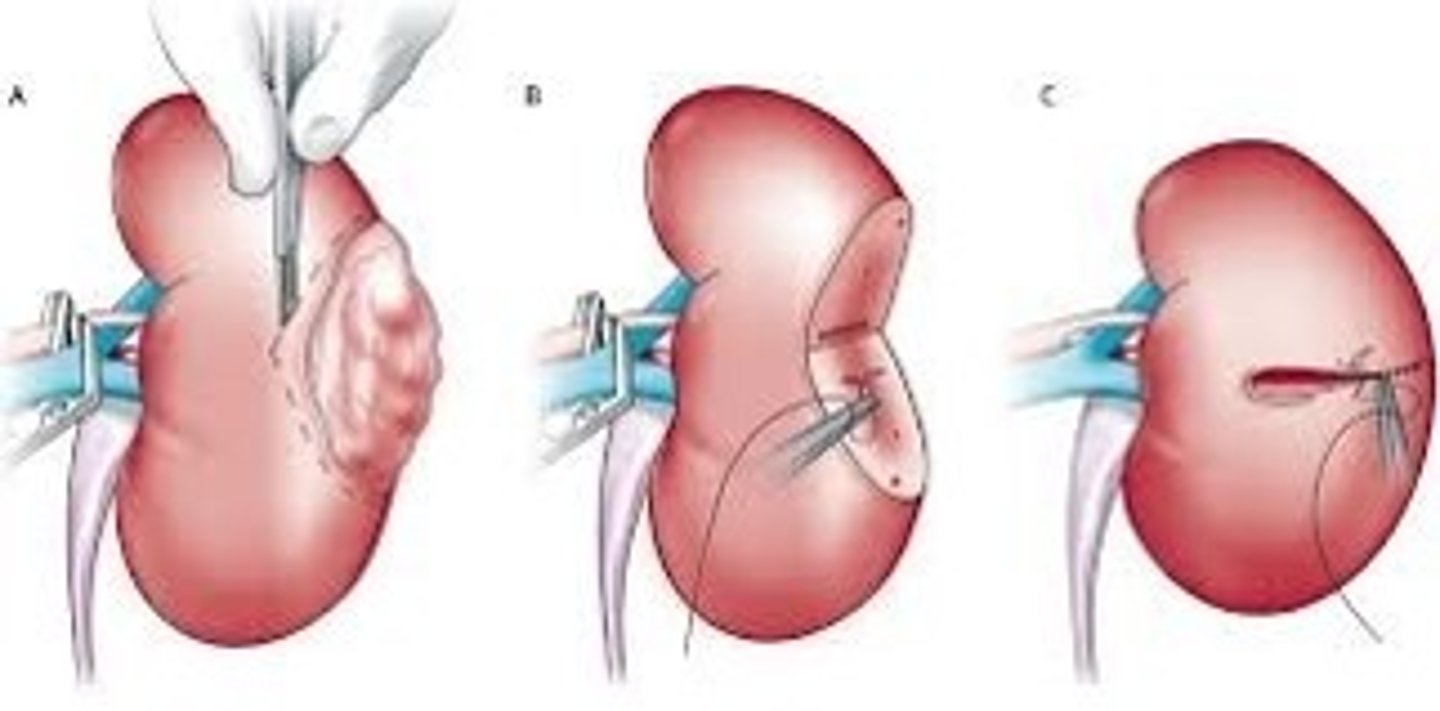
What is the best treatment for localized RCC? What are some other options?
Resection = best; ablation (if poor surgical candidate), active surveillance, adjuvant therapy (immunotherapy, molecularly-targeted therapy)
How is advanced RCC treated?
Immunotherapy (IL-2, INFa), other medical therapy (molecularly-targeted), palliative surgery, no chemo options
What is the biggest risk factor for developing bladder cancer?
Cigarette smoking
What are some s/sxs of bladder cancer?
Painless hematuria (in a patient > 40, is transitional cell bladder cancer until proven otherwise!!!), +/- pain, frequency, urgency, weight loss, fatigue, PE findings typically absent
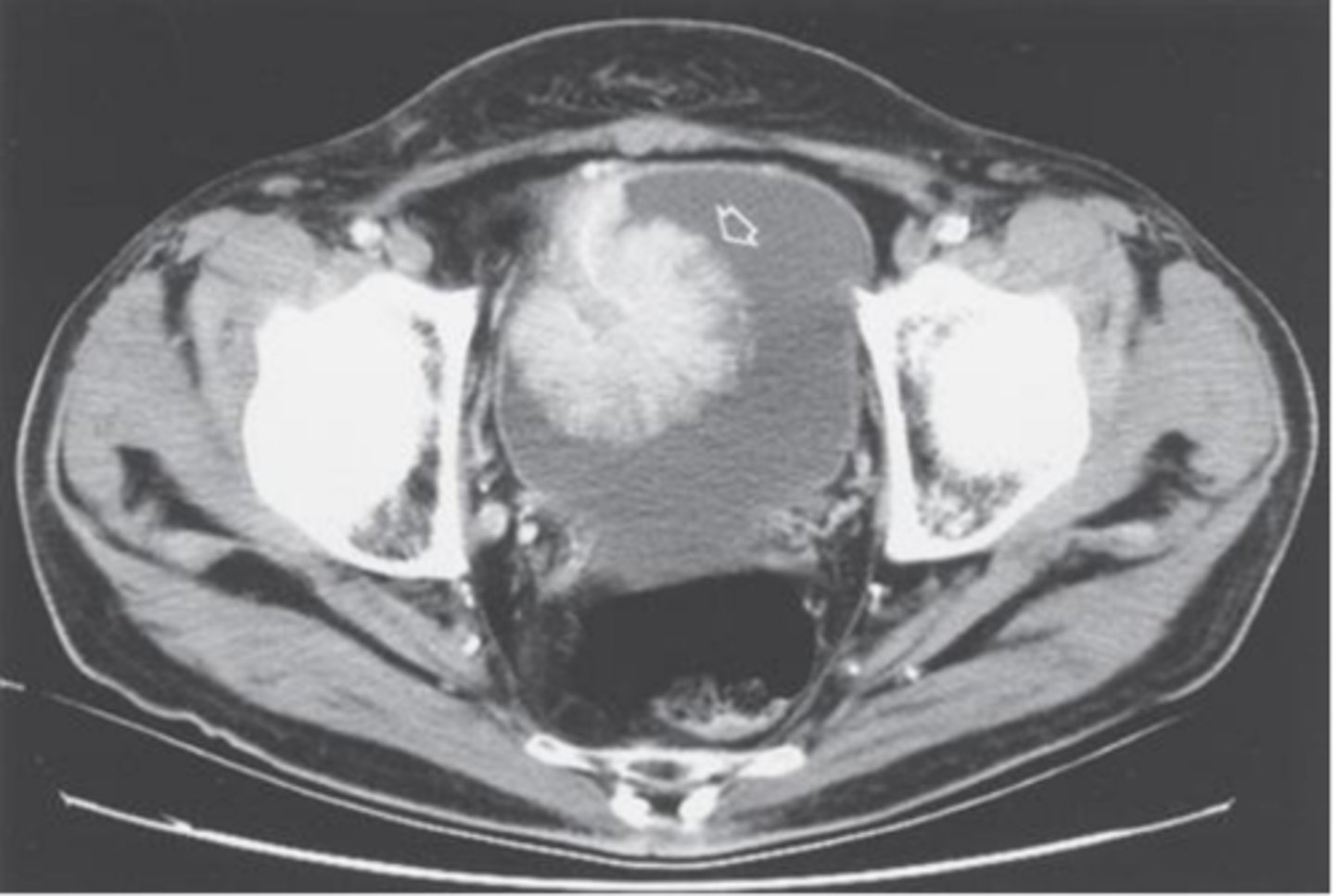
How is bladder cancer diagnosed? What is the gold-standard?
UA (looking for hematuria), urine cytology (not sensitive, very specific tho), CT abdomen & pelvis w/ & w/o contrast plus delayed imaging (most sensitive), IVP or retrograde pyelogram (safe for patients w/ IV contrast allergies), cystoscopy w/ biopsy is definitive (gold-standard)
How is bladder cancer treated?
Transurethral resection of the bladder tumor (TURBT) + intravesical therapy
partial or radical cystectomy for more invasive case
radiation + cisplatin-based chemo for advanced cases
How common is prostate cancer?
It is the most common cause of cancer in men & is the most common urologic malignancy - extremely common
What are some risk factors for developing prostate cancer?
Age**, ethnicity (AA > white), family history, diet/supplements (red meat, testosterone products)
In general, do most cases of prostate cancer tend to develop in the peripheral zone of the gland or in it's core?
In the peripheral zone (often caught on DRE)
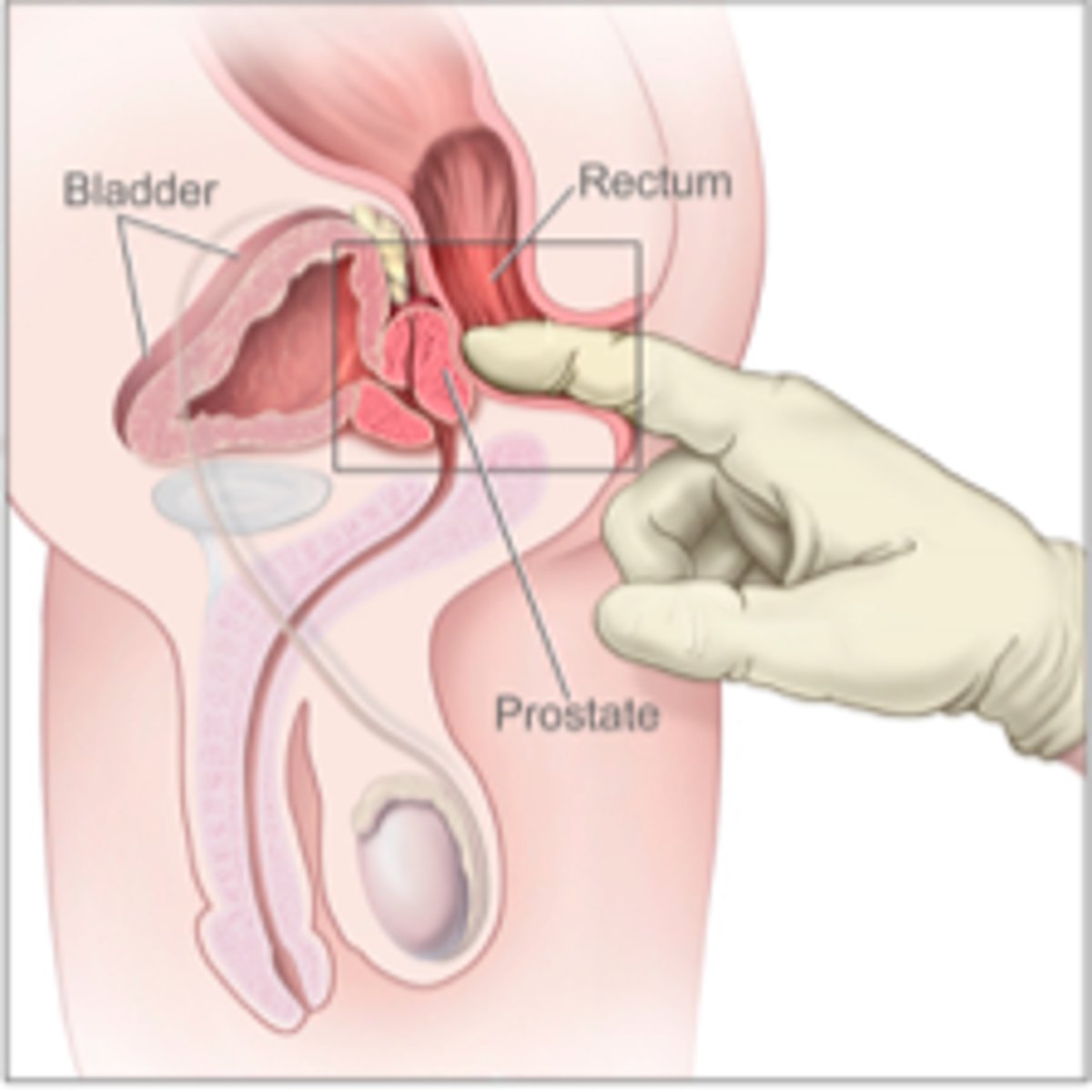
What are some s/sxs of prostate cancer?
Often asymptomatic, urinary sxs rare, hematuria, weight loss, constitutional sxs if spread, asymmetry/nodules of the prostate on DRE
What are some groups of people that we would NOT screen for prostate cancer? Who do we screen?
Anyone w/ a life expectancy < 10-15 years (prostate CA extremely slow-growing), age < 40, age 40-49 at average risk, age > 70
We do screen men age 50-69 based on shared decision making weighing the benefits & risks
What role does serum PSA play in diagnosing prostate cancer?
Its role is very controversial (since there are many things that can increase PSA levels besides cancer), but it does play an important prognostic role
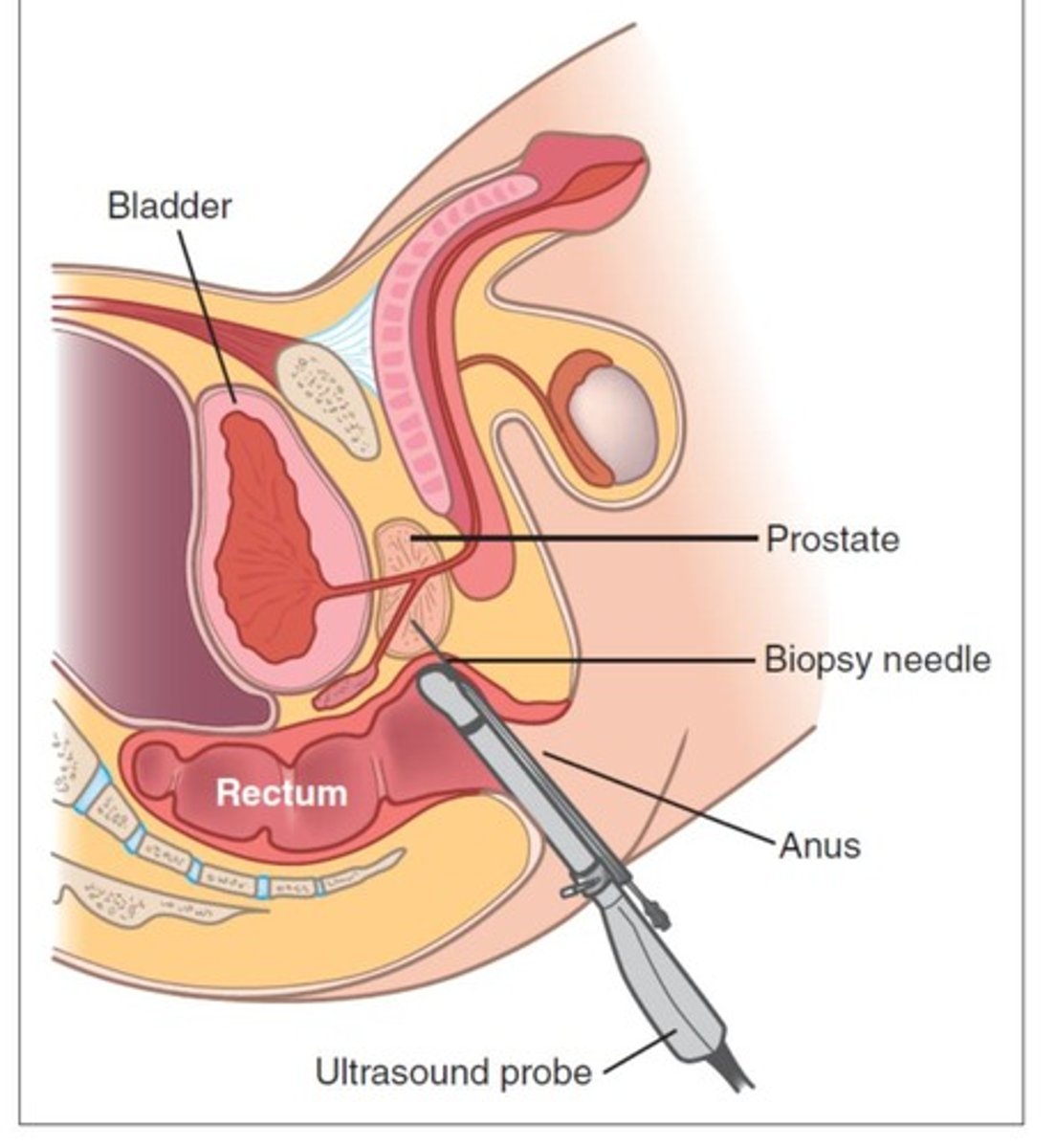
How is prostate cancer diagnosed?
Possible MRI to aid decision making, prostate needle biopsy is definitive & required for diagnosis
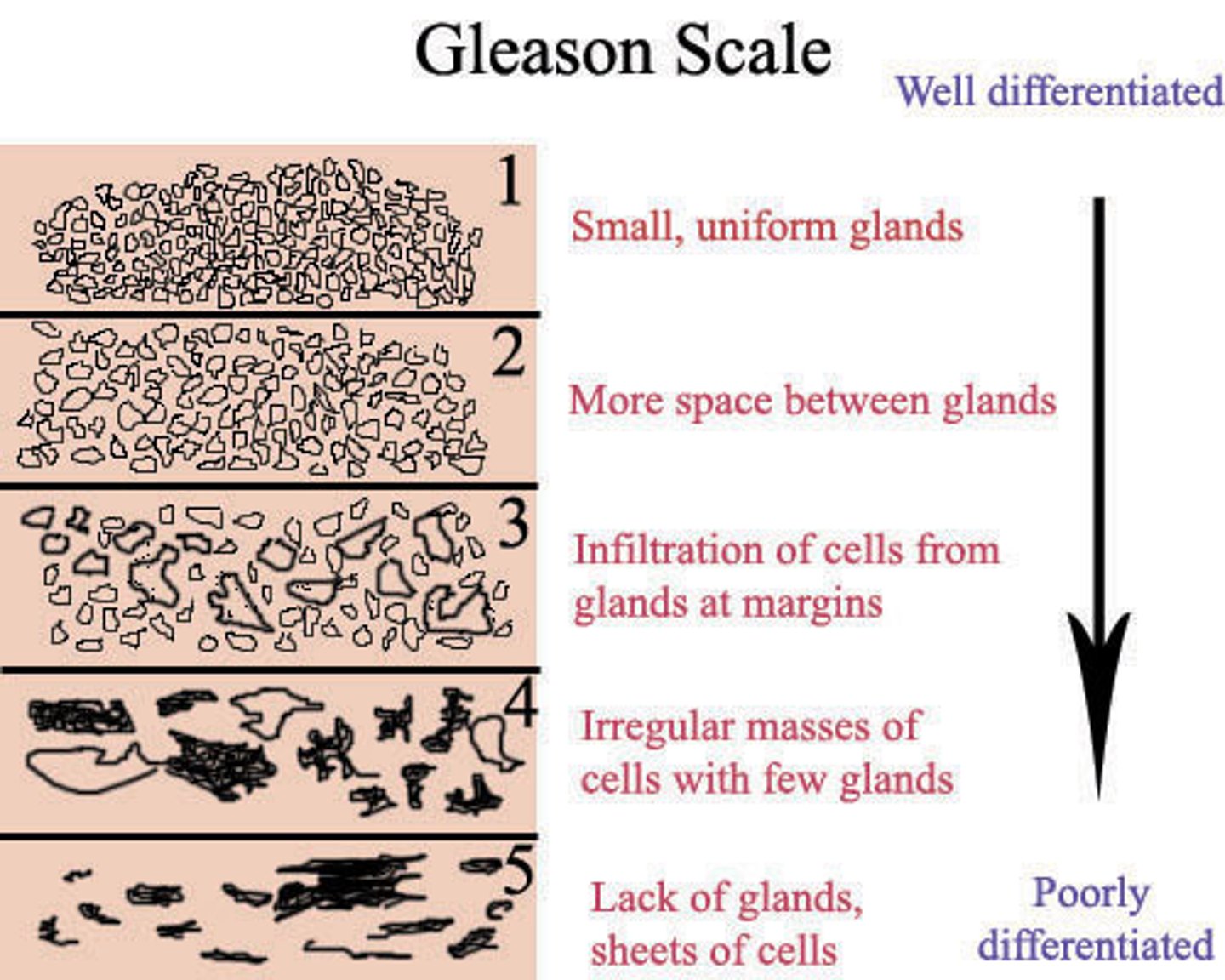
What is the role of the Gleason score in prostate cancer, & how can we interpret its results?
Preferred system of tumor grading; a higher score is consistent w/ more advanced disease and/or worse prognosis of localized disease
How is prostate cancer treated?
Active surveillance (patient-dependent), radiation, radical prostatectomy, androgen deprivation therapy (esp. good for metastatic disease)
What age range does testicular cancer tend to affect? What is a big risk factor for this pathology?
Young men age 20-35; cryptorchidism
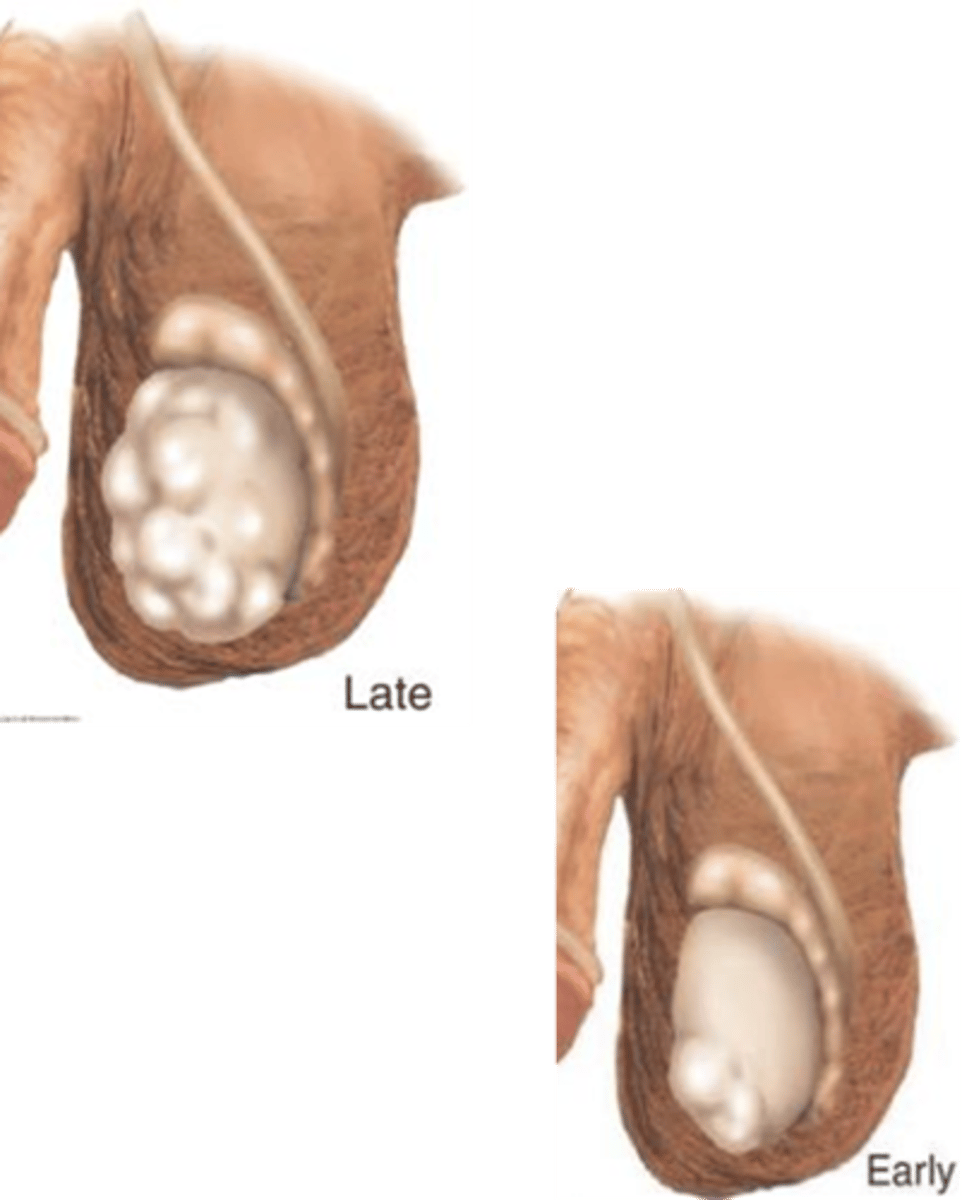
What are some s/sxs of testicular cancer?
Unilateral nodule, painless testicular enlargement (any firm large area is suspicious, CA is the diagnosis until proven otherwise), ache or heavy sensation, secondary hydrocele, +/- pain, possibly asymptomatic, gynecomastia
What is the role of scrotal ultrasound in diagnosing testicular cancer?
Seen as an extension of the PE, can differentiate intrinsic vs. extrinsic & solid vs. cystic masses
What role does radiographic evaluation (imaging) have in testicular cancer?
Used for staging purposes
What is gold-standard for diagnosing testicular cancer? When would we use retroperitoneal lymph node dissection?
Histological sampling; indicated in patients w/ aggressive malignancies or following chemo for those w/ residual disease (gold-standard for staging cancers of the retroperitoneum)
In general, what is the difference between seminoma & non-seminoma germ cell tumors?
Seminomas: typically localized & slow-growing
Non-seminomas: more likely to be advanced w/ aggressive growth
What is treatment of testicular cancer based on, and how does this system work?
based on stage; generally, Stage I cancers require just surgery (orchiectomy) whereas higher stages will often need additional chemo regimens and/or lymph node dissection
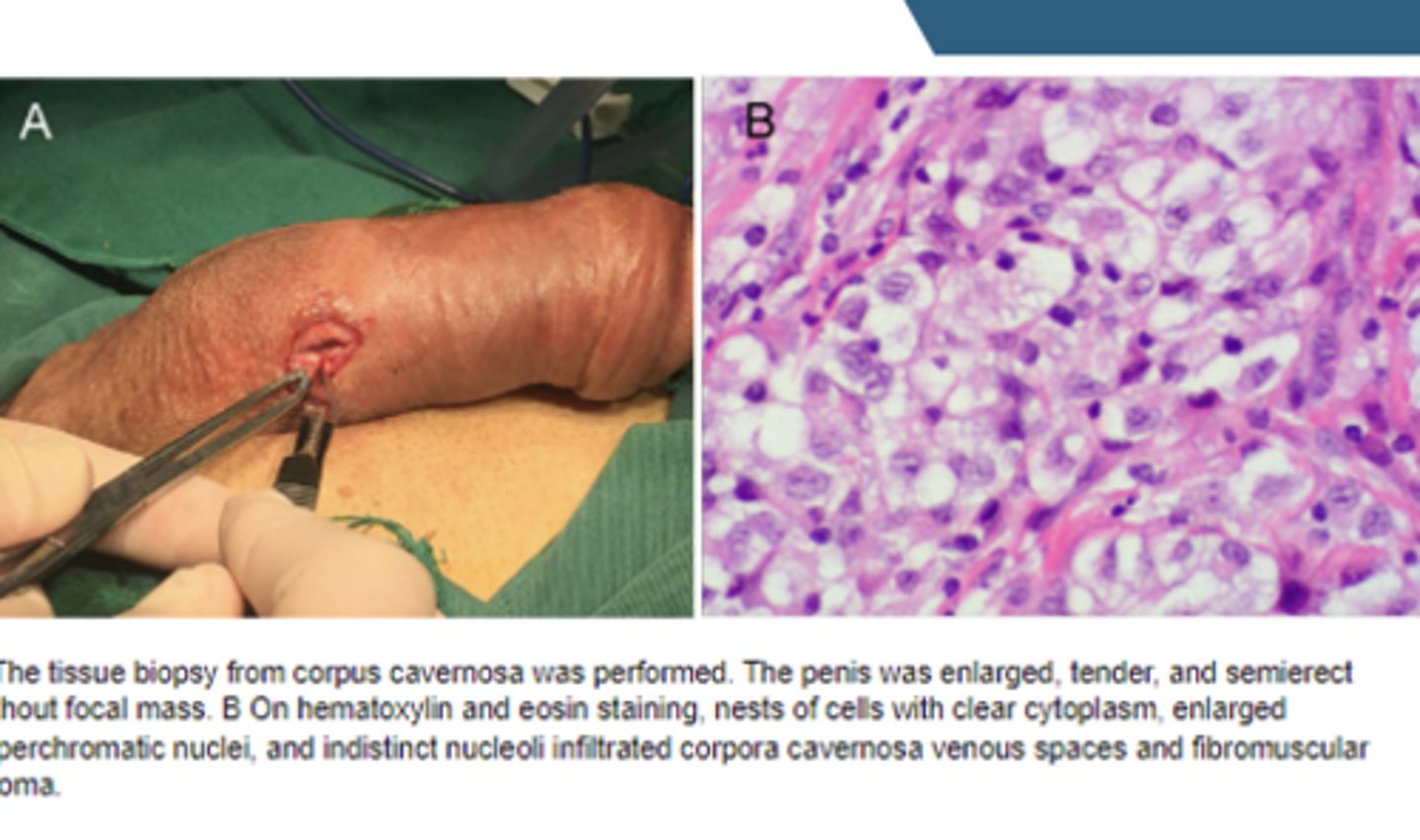
What type of cancer does penile cancer tend to be?
Squamous cell carcinoma (SCC)
What are some s/sxs of penile cancer?
Penile skin abnormality/palpable mass (painless lump/ulceration, rash, bleeding, balanitis, etc.) inguinal LAD

How is penile cancer diagnosed?
Biopsy (gold-standard), may need ultrasound-guided fine needle aspiration of the inguinal lymph nodes if they're involved
How is penile cancer treated depending on if the patient is at a low vs. high risk of recurrence?
Low: limited excision, nodal evaluation
High: partial or total penile amputation, nodal evaluation