Pulseless Arrest - Management of PEA/Asystole
1/27
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
28 Terms
high quality CPR and address underlying cause
give epi!
Treatment of pulseless arrest in general
perfusion
PEA only exists in rhythms that would normally cause ______
perform CPR for 2 min
obtain IV/IO access
epinnephrine 1mg every 3-5 min
advanced airway
reevaluate rhythm
If patient does NOT have a shockable rhythm what must you do?
hypovolemia
hypoxia
hydrogen ion
hypo/hyperkalemia
hypothermia
hypoglycemia
H’s?
toxins
tension pneumo
tamponade
thrombus (MI or PE)
trauma
T’s?
hypovolemia
What is probably the most common H?
hypoxia
Very common cause and may present with mental status changes prior to any changes in the oxygen tension- be wary of the patient who suddenly becomes combative
hydrogen ion excess
Consider with diabetes, renal failure- Tx with ventilation, bicarb
hypo/hyperkalemia
Consider with renal failure, NPO status and lack of replacement, recent dialysis, medications
Tx: calcium chloride, bicarb (less), glucose + insulin, possible albuterol (takes too long for Kexalate resins)
Add magnesium if hypokalemic + cardiac arrest
hypothermia
Environment of the patient, wetness added to the cold increases injury, are Osborne waves present?
Better to obtain core temperature (esophagus, rectum, bladder thermometers)
toxins
◦Pupil size, bradycardia, mental status changes, bottles at bedside
◦Give specific antidote, if available; may need to intubate if respirations are suppressed
tension pneumothorax
◦Neck vein distention, tracheal deviation, decreased/nonexistent breath sounds, hard to ventilate patient
cardiac tamponade
◦No pulse felt with CPR, distended neck veins
◦Treat with pericardiocentesis, pericardial window
pulmonary throbosis
◦Saddle embolism obstructs flow to pulmonary vasculature and causes acute right-sided heart failure (may cause instant death if large enough)- fibrinolytics may be lifesaving in this scenario; ECMO
coronary thrombosis
◦History, EKG, cardiac markers (may not be that helpful). Cath Lab? ECMO?
trauma
Stop the bleeding, Fluids
asystole
patient is in cardiac arrest and has no pulse with straight line on monitor
fine VF
Ensure asystole is really a flat line and not ______
begin chest compressions
What should be done immediately for asystole?
extremely poor
What is survival looking like for asystole?
agonal rhythm
Asystole can be an ____ _____ confirming death rather than a rhythm that needs to be treated
myocardial damage
Persistent asystole can represent extensive myocardial damage from _____ _____ _____ ______
epinephrine
What is the only indicated med for asystole?
10 seconds or less
CPR interruptions should be how long?
IV and IO placement
What is placed as priority over advanced airway placement unless basic airway resuscitation is ineffective or if the arrest is caused by hypoxia?
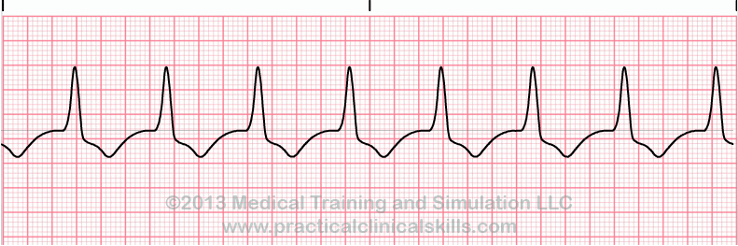
What is this rhythm?
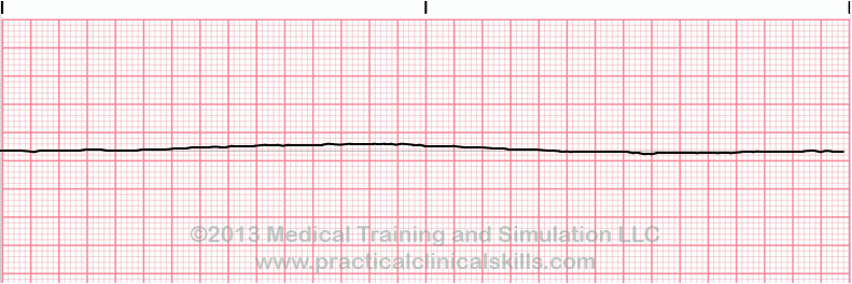
What is this rhythm?