11- peri implantitis
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
How do hard vs soft tissues heal after inserting an implant?
Osseointegration
Establish peri implant mucosa- via JE and CT zone
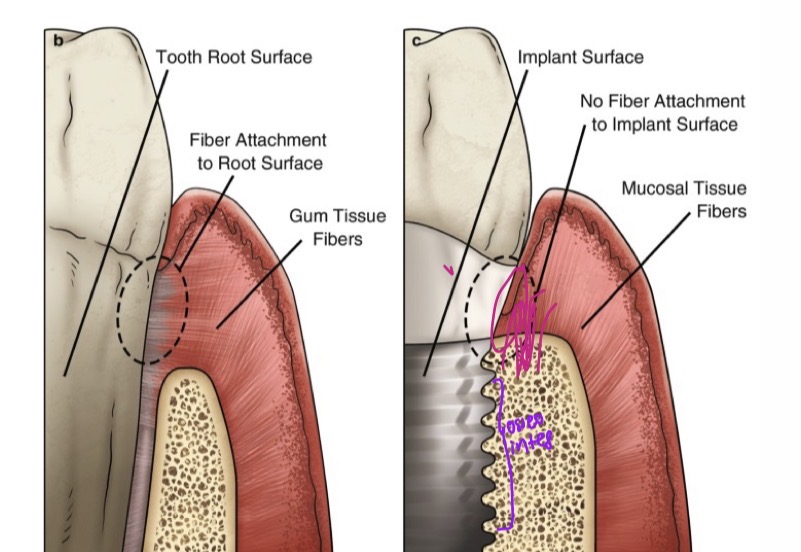
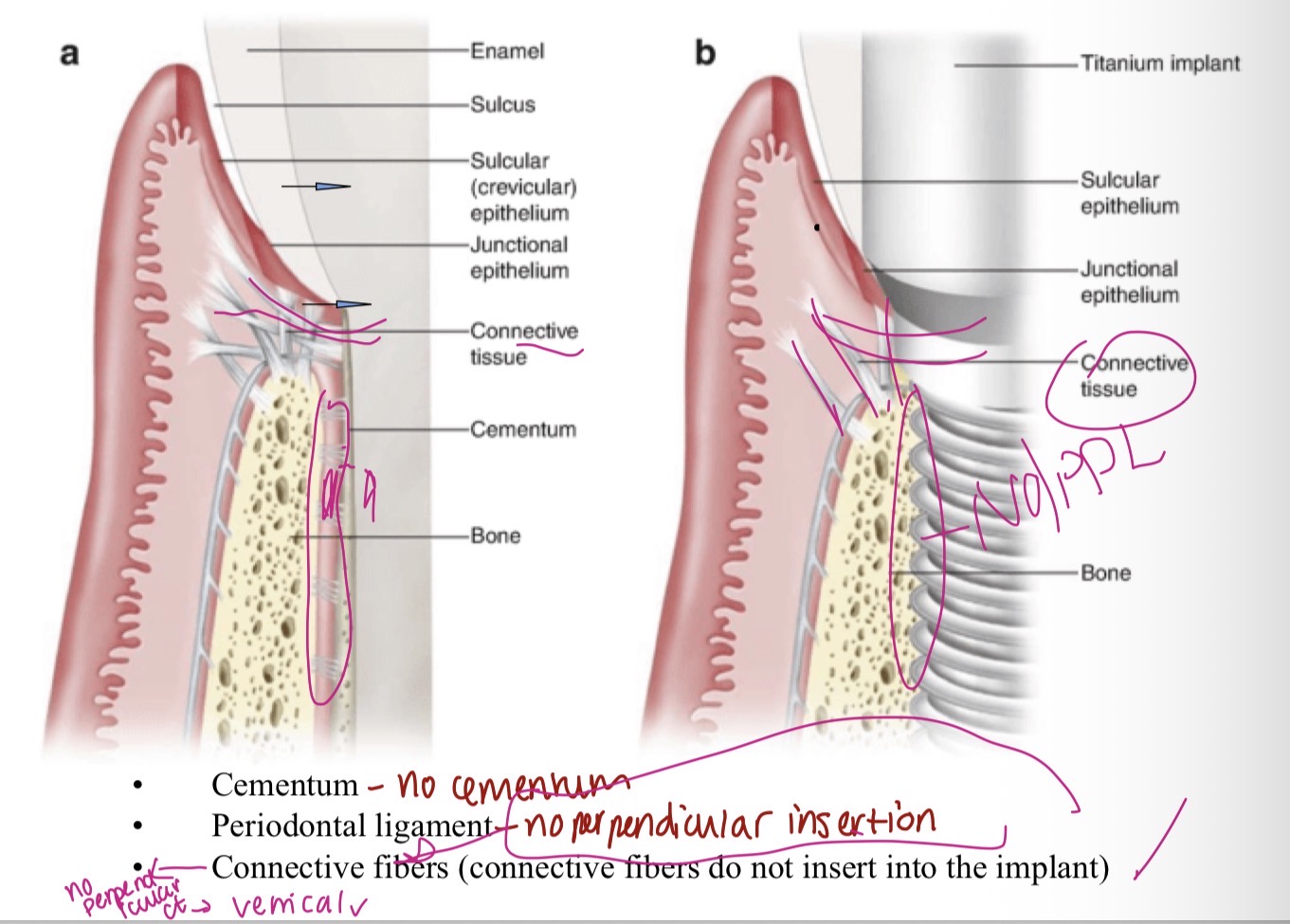
Periodontal structures after implant?
No cementum
No PDL
No perpendicular ct, only vertical
What are the time periods after surgical insertion of an implant?
Integration period (Time for osteointegration)
Prosthesis placement (crown)
Acclimatisation- comfort, hygiene
Baseline moment- closure or definitive Cementation, take records
Healthy peri implant tissues characteristics?
No swelling or redness or BOP or pain
No increased PD
How do you clinically assess implant site for health?
Evaluate soft tissues and biofilm, BOP (due to inflammation not trauma), sulcus probing
Periodic reviews- visual inspection, digital palpation
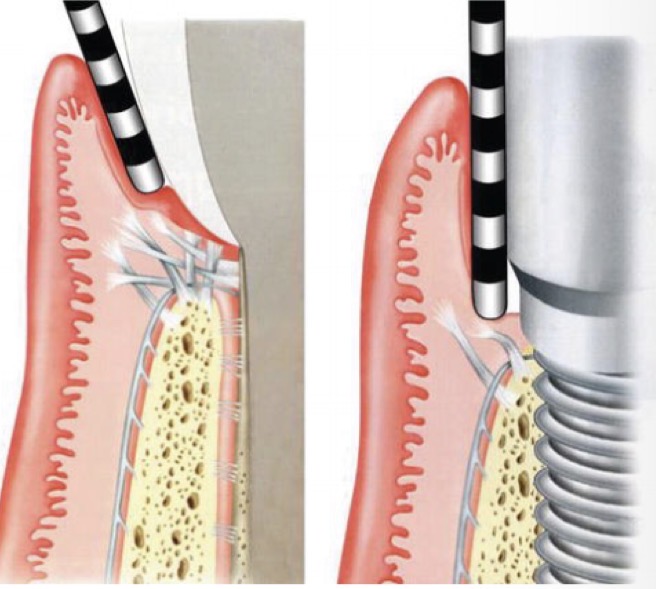
Peri implant tissue probing (6)
Always use same perio probe
For healthy patients- range broader- no CT so pd deeper already
Determined by prosthesis emergence (angle at which prosthesis coming out)
Remove prosthesis for reliable measurements
Maybe resistance, compare to initial records, gentle force
Bleeding suggests instability, positive predicative value greater
How to radiographically assess implant site for health?
Use fixed, non variable points to monitor progression
OPG, periapical
CBCT- BUT only shows interproximal bone levels (need clinical exam to confirm)
6 Clinical characteristics of unhealthy peri implant tissues
Plate detection
Mobility
Sounding depth at 6 points
Redness, swelling, contour, consistency and gum shape changes
Photographic records
No specific bacteria and determine released mediators
How to diagnose unhealthy peri implant tissues with palpation, percussion, stability?
Vb/Pt, tissue traction to check adherence, look for inflammation, suppuration
Check for sounds
Individual for each implant
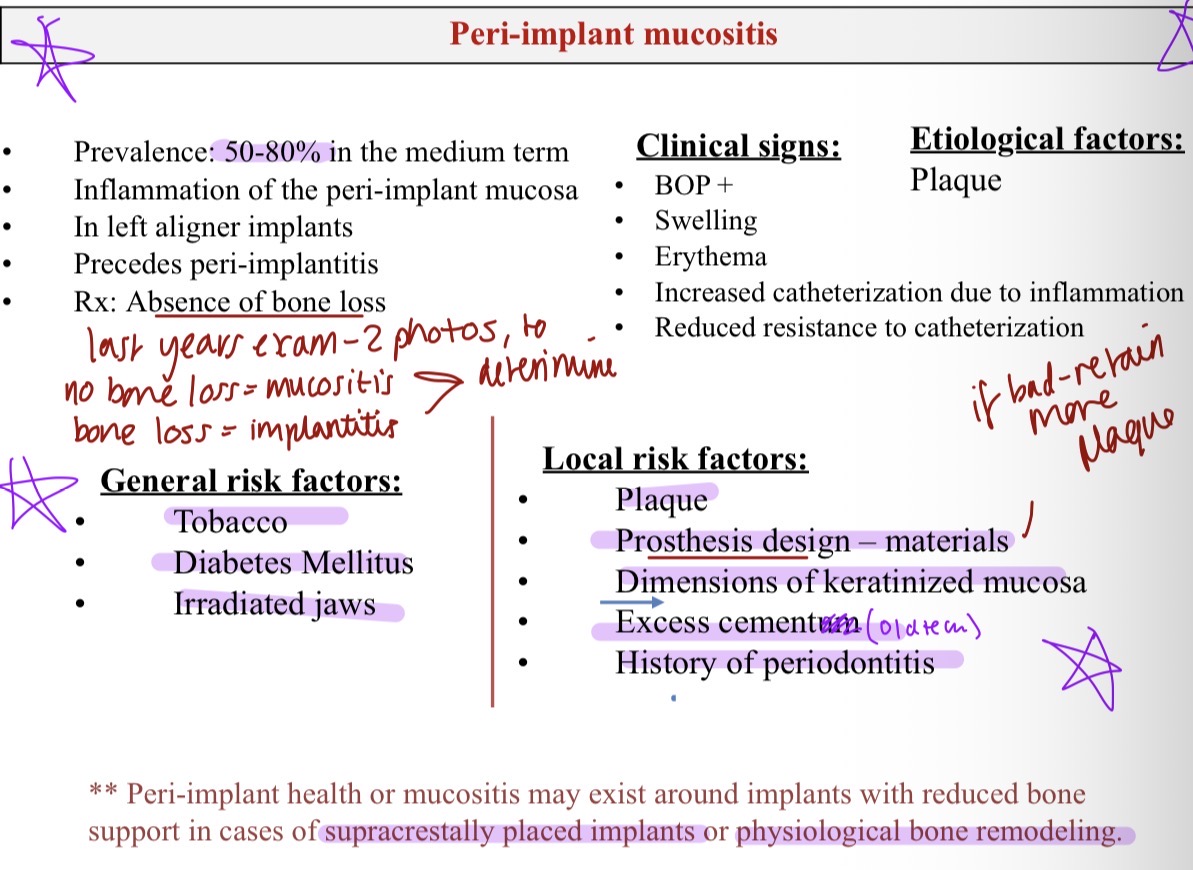
What is peri implant mucositis? (Prevalence, what is it, characteristics) general risk factors 3 local 5
50-80% Medium term
Inflammation of peri implant mucosa due to plaque, precedes peri implantitis
NO BONE LOSS
BOP +, swelling, erythema, increased catheterisation due to inflammation
What is periimplantitis?
25-50% medium term
Progressive loss of bone
BOP with SUPPURATION
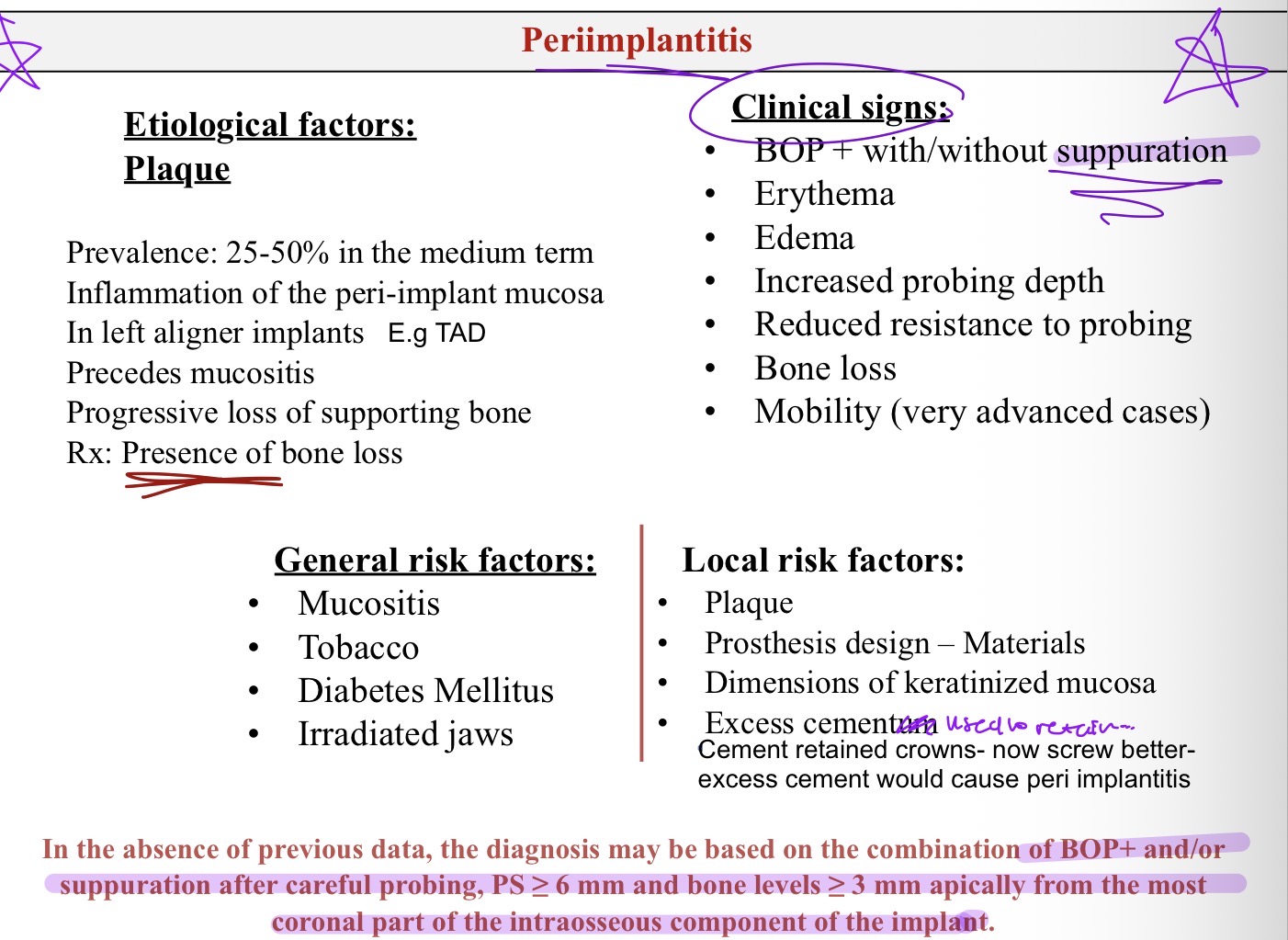
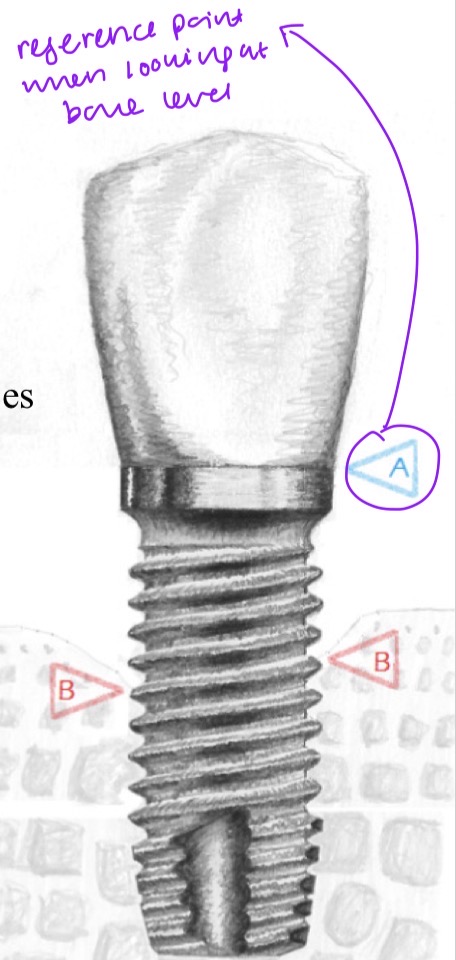
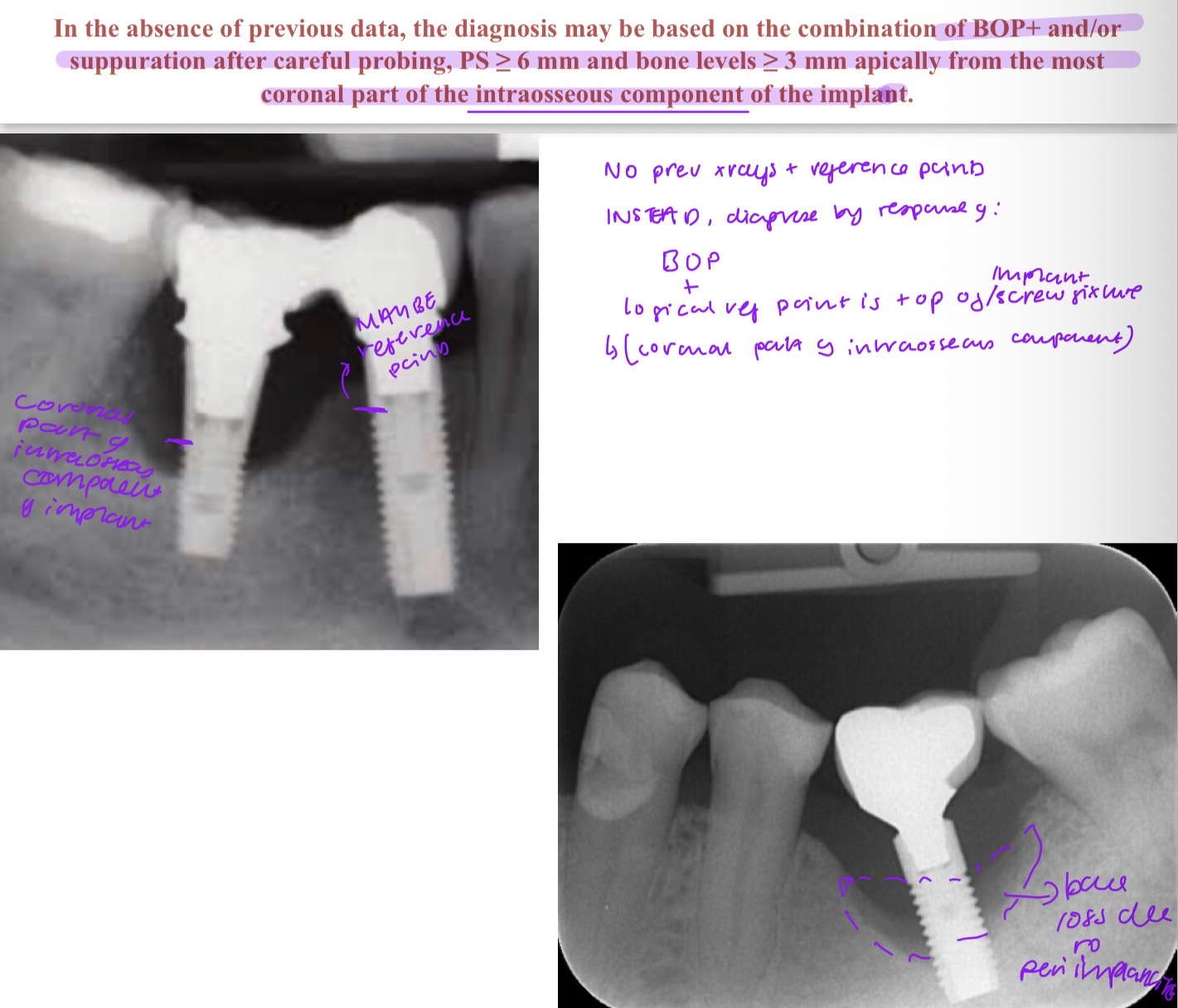
Peri implantitis diagnosis is based on what?
Combo of BOP + and/or suppuration
PD 6mm or over, bone levels 3mm or over apical from most coronal intraossesous component of implant (logical reference point)
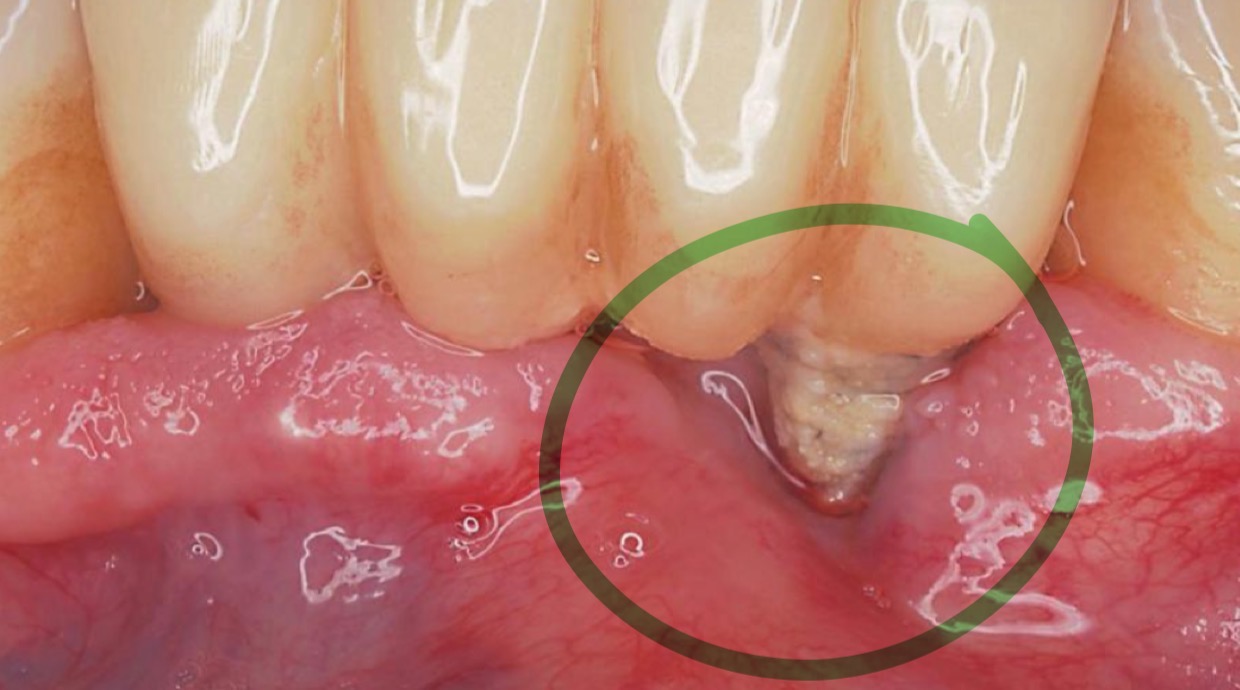
What is this?
Peri implantitis- suppuration
What are 4 non peri implantitis reasons for implant failure?
Failure of osseointegration- early implant loss
Deosteointegration- later implant loss, occlusal overload
Physiological bone remodeling-
translocation (inevitable bacterial colonisation)
specific tissue adaptation
recover of hemostasis (biological width)
Iatrogenic-
remnants of submucosal cement
over contoured prosthesis
implant malposition
10 Possible errors in implant treatment that can lead to peri implantitis
Inappropriate patient selection
Insufficient periodontal treatment
Incorrect implant placement
Insufficient bone thickness
Too apical or too coronal
Error in mesio-distal position
Post op care
Incorrect prosthesis
Lack/absence of maintenance
Lack of diagnosis and management of mucositis
3 Objectives for therapeutic approach
Disinfect tissues surrounding implant
Decontaminated exposed implant surface
Promote favorable conditions to minimise future problems
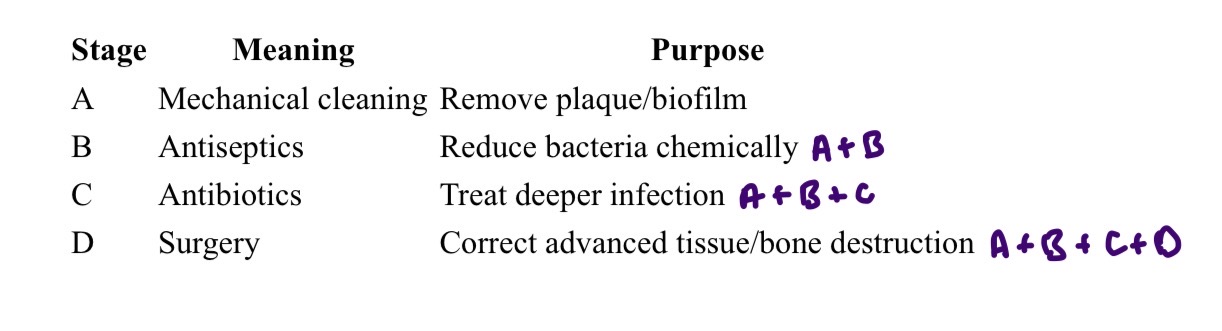
Treatment strategy to cure peri implantitis?
1st - Etiological treatment (eliminate the cause)
2nd - Corrective treatment of sequelae (attempt to correct the consequences of the infection)
What 5 clinical parameters are used in CIST (cumulative interceptive supportive therapy) to assess disease severity? What 4 treatments depending on severity?
Presence of plaque, BoP, suppuration
Increased drilling depth
Radiographic bone loss
What are the 2 types of treatments goals and what ways would you treat the contaminated surface?
Goal- reosseointegration- disinfect titanium surface without altering it so bone can attach
Resective approach- reshape defect and leave part of implant exposed to oral cavity- smooth metal surface (less retentive to plaque)
Aeropolishers initially developed for… risk/not recommended when? What material used? Avoid in (5)
For supragingival removal of plaque
Risk of emphysema during subgingival instrumentation
Glycine 24um and erythritol 14 um
Avoid if thin bio type, no KM, pockets beyond mucogingival junction, adjacent to extracted tooth, endo abscess
When is a titanium brush used? (4)
Highly adherent calcified deposits
Unchanged implant surfaces
Narrow diameter implant
Difficult to reach areas
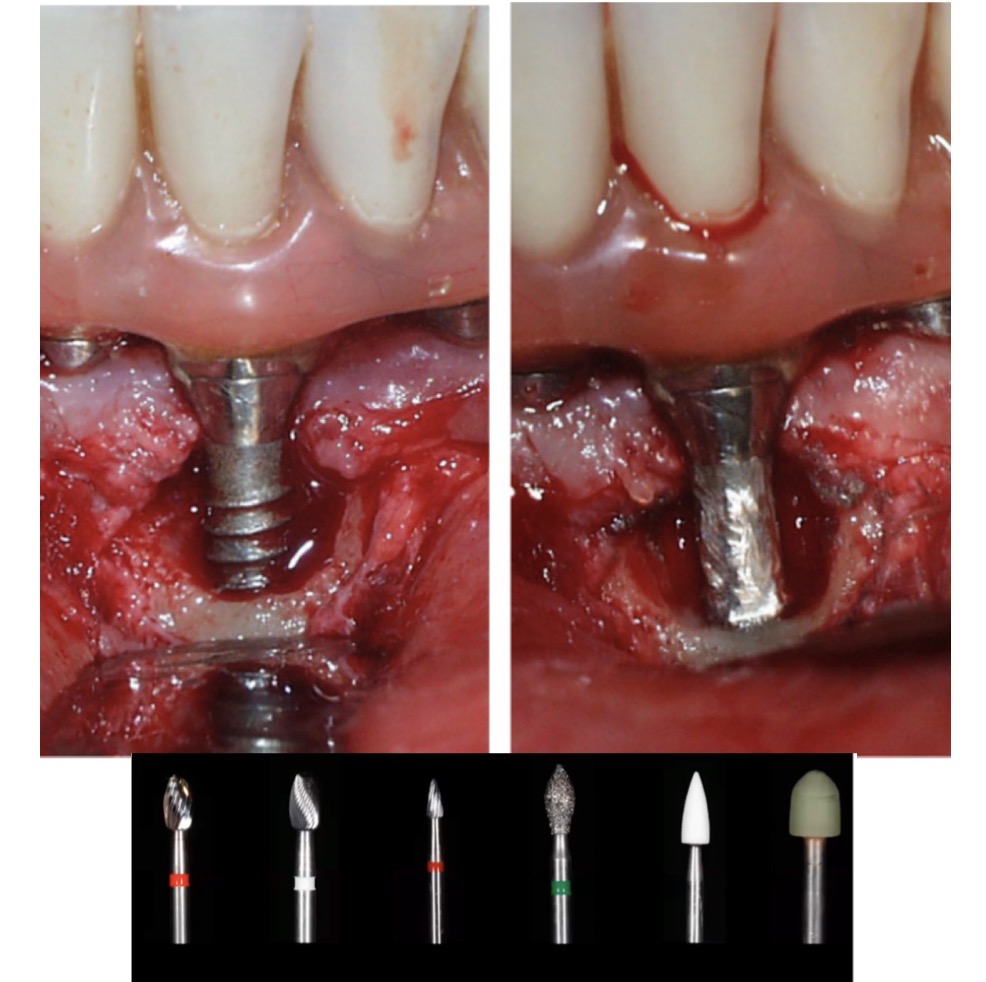
What is an implantoplasty? Do using what? 4 indications- why?
Mechanical removal of thread coils and modified surface of rough implants to decontaminate and create smooth surface
Use tungsten carbide burs
Limited regeneration potential-
Peri implantitis with suprabony defect
Peri implantitis with wide or partially contained intrabony defects (2–3 missing walls)
No need for aesthetics- e.g posteriors
Patient wants to maintain prosthetic resto
Advantages of an implantoplasty?
Adequate cooling
Doesn’t increase strength in standard diameters
Doesn’t have increased rate of fractures
Doesn’t lead to inflammation due to titanium particles
How are lasers catergorised based on their MOA?
Deep penetration- diode or Nd:YAG
Superficial penetration- Er:YAG or CO2
Quick lasers for non surgical mechanical debridement of peri implant lesions
Diode- melanin affinity- pigmentated pathogens (many in peri implantitis)
Nd:YAG- ophthalmology, aesthetic med, oncology- thermal changes + damage bone + slow healing
CO2- good hemostatic effect but not recommended
Er:YAG- mainly absorbed by water- good to remove granulation tissue, bacterial decontamination without damage
B- antiseptic therapy
A + subgingival irrigation 0.2% chx rinses or gel (1x daily 30secs) for 14 days
Chx has non selective cytotoxicity- is to fibroblasts and osteoblasts (compromise healing)
Saline- not bactericide but reduces biomass of biofilm
Sodium hypochlorite 0.25-1.5%- reduce biofilm doesn’t affect host cells
Updated guideline of C- antibiotics therapy? When used? What drug?
Doesn’t recommend use of systemic ATB as an adjuvant to non surgical treatment
Only in more severe cases- pd over 7mm and extensive drainage, many implants affected
Metronidazole 50mg x 8hrs x7 days- avoid as palliative care for lost implants
Effectiveness of surgery influenced by? (10)
Depending of anatomy of bone defect and location of implant
Resective surgery allows (3)? Results influenced by (4)
Better access to surface, proper decontamination, adequate apical replacement of peri implant tissue
Operator skill, extent of bone loss, tobacco, plaque