Lecture 30: Anesthesia for Cesarean Sections, Neonates, and Geriatrics
1/41
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
42 Terms
changes in pregnancy
increases:
increased cardiac outout due to increased heart rate and stroke volume
blood and plasma volume
minute ventilation due to increased resp rate
oxygen consumption (around 20%)
intragastric pressure
GFR
changes in pregnancy
decrease
Hb and PCV
plasma protein
PaCO2
tidal volume, functional residual capacity and total lung capacty
total pulmonary resistance and peripheral vascular resistance
GI motility, gastric emptying, and gastric pH
BUN and creatinine
potential complications in dam
venous return may be decreased when placed dorsally due to compression of vena cava by gravid uterus —> resulting in what effects on the heart?
relative anemia
maternal blood volume increases by around 20 %, with larger increase in plasma volume
PCV within the normal range may mean the bitch is actually dehydrated
hypocalcemia in small breed dogs, large litters, or with uterine inertia
ionized calcium preferred test —> why?
increased myocardial work and reduced cardiac reserve
increase in alveolar ventilation —> rapid response to inhalant anesthesia
prone to hypoxemia
increased risk of regurgitation, if possible —> plan for surgery
elevated renal values may indicate dehydration or underlying kidney disease
emeregency vs. planned c-section
emergency:
paatient has been in active labor for >1 hour with no fetus delivered
may be in a compromised metabolic state
viability of puppies a concern
planned
gestation length known
during “normal” hours… plenty of help
patient is fasted
most common cause of dystocia?

assessment of patient:
signalment: brachycephalic breeds are common
history: other medical conditions; any current meds
how long bitch has been in labor and if any puppies have been delivered (dead or alive)
PE: abdominal ultrasound (more sensitive in detecting fetal viability) or radiographs to determine number, size, and position
fetal heart rate of 150-200 bpm = healthy; 100-150 bpm = fetal stress
bloodwork:
PCV, T.S., BUN, calcium, glucose, and electrolytes
what bpm is fetal stress?
100-150 bpm
stabilization and patient prep prior to surgery
correct fluid deficits and electrolyte imbalances prior to surgery if possible, otherwise during surgery
± blood type and cross match patient since blood transfusion may be needed if blood loss is severe during surgery
shave abdomen and dirty scrub prior to induction if possible
induce in the OR and have surgeon scrubbed and gown/gloves on —> goal is to have puppies/kittens out within 5-10 mins of induction
personnel devoted to anesthesia, surgery, puppies based on availability
increased gastric acid and decreased lower esophageal tone —>
esophageal reflux
maropitant and ondansetron help with nauseea/vomiting, but not:
Regurgitation
observe and treat —> injectable PPI —> suction and lavage —>
sucralfate after recovery
preoxygenation:
rapid eeoxygenation at induction, decreased lung expansion
maternal hypoxemia = fetal hypoxemia and acidosis
preoxygenate with 100% oxygen for minimum of 5 mins before induction —> don’t oxygenate the room!
be prepared for rapid intubation!
how is preoxygenation accomplished?
premedications:
premeds will affect the fetus, move quickly!
opioids are useful —> pure mu agonists = reversible!
treat early with anti-emetics
most drugs cross the placenta, so short-acting drugs that can be antagonized are preferred
drugs that are highly protein bound do not readily cross the placenta - buprenorphine (highly protein bound but hard to reverse and not as much analgesia)
how do you make buprenorphine work?
benzodiazepines as premed
mild sedation and skeletal muscle relaxation
Dr. Wilson avoids because it decreases fetal viability
fetal livers do not metbolize due to immature enzyme systems, so you get prolonged sedation
can antagonize flumazenil after delivery
phenothiazines
cause maternal hypotension and leads to fetal hypoxemia
acepromazine has a long duration and cannot be reversed; requres hepatic metabolism
decreases ability of neonate to thermoregulate
NOT recommended for c-sections!!!
alpha2-agonists
increased chance of puppy mortality?
CV effects include bradycardia, arrythmias, decreased contractility and initial hypertension followed by hypotension
xylazine has an oxytocin-like effect on uterus
consider low doses after puppies removed
low doses may be beneficial at other times also
induction:
swiftly securing airway reduces the risk of aspiration. Have suction available. Keepe P in sternal and head above stomach
injectable technique recommended over inhalent induction. Disadvantages of “masking down” include:
takes longer than injectable
inhalation induction is more rapid in pregnant animals because of decreased functional reserve and increased minute volume, so this could lead to overdose compared to non-prenant p
stress and catecholamine release = fetal stress
hypoxemia in dam and fetuses
risk of regurgitation and aspiration from unprotected airway
do NOT mask anything down!!!
injectable induction agent:
propofol
dose 2-6 mg/kg, IV to effect, higher dose if alone - lower dose if with other drugs
metabolized in liver and crosses placenta
may cause hypotension due to vasodilation
respiratory depression may necessitate IPPV
provides no analgesia
not cumulative
this is a great induction agent in c-sections
injectable induction agent:
alfaxalone
1-2 mg/kg, IV for c-section in the dog and similar puppy survival rates to propofol and was associated with better neonatal vitality during first 60 minutes after birht
Alfaxalone CRI has been compared to maintenance with iso - slower recovery and lower APGAR scores, but no difference in survival
injectable induction agents NOT to use during c-sections:
ketamine + modazolam should not be used in c-sections
ketamine —> significant depressant effects in neonates
decreased likelihood of puppies breathing spontaneously at birth with use of ketamine
inhalent anesthesia for c-section maintenance
all inhalants cross the placenta because lipid solubility and low molecular weight
CV and resp depression
keep % as low as possible to avoid neonatal resp depression
MAC is decrased during prenancy by 16-40% for iso
manual or mechanical ventilation
may be needed due to pressure on diaphragm from uterus
avoid hyperventilation —> decreased uterine and umbilical blood flow —> fetal hypoxemia
comparison of protocols
use of propofol, alfaxalone, and isoflurane was associated with a lower puppy mortality rate
use of xylazine associated with an increased puppy mortality rate
use of ketamine, or inhalation anesthetics was associated with decreased puppy vigor, mortality?
use of local anesthesia in c-sections
line block with lidocaine (2 mg/kg) or bupivicaine (1 mg/kg) prior to surgery and after, block the layers as you close
Nocita - liposome encapsulated bupvacaine works extremely well as pre and post line block for extended analgesia
epidural anesthesia
decrease volume by 25% because of decreased epidural space due to increased collateral circulation
epidural lidocaine (2%; 2-3 mg/kg up to 6m) provides good regional anesthsia and muscle relaxation
use lidocaine instead of bupivacaine because shorter onset (5-10 mins) and duration (60-90 mins)
can combine with morophine (0.1 mg/kg) to prolong anesthesia
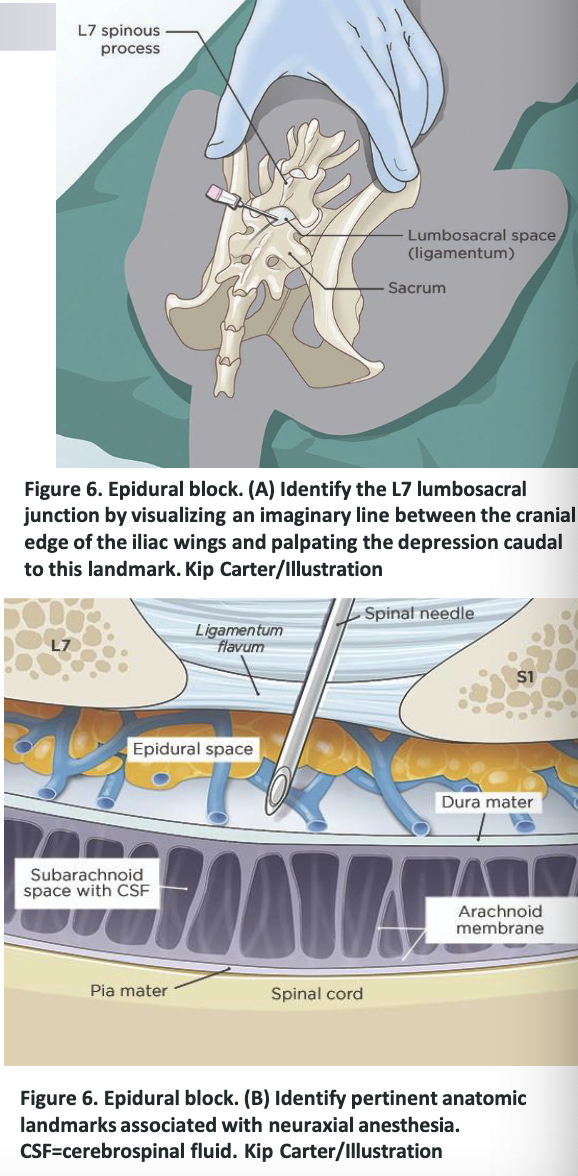
epidural block
complications during anesthesia
hypotension
hemorrhage and increased intra-abdominal pressure decrease cardiac return
treat if MAP below 60 mm Hg or sysstolic below 80 mmHg
decrease anesthetic depth —> PIVA
crystalloid fluid bolus (5-10 mL/kg)
± colloid therapy (Vetstarch or 5mL/kg IV bolus over 15 mins)
opioid bolus or alpha-2 agonist if fetus(es) out
atropine to treat bradycardia and improve CO
vasopressor and chronotropic drugs
less effectve during pregnancy… thought to be due to downregulation of alpha and beta receptors and increases in prostaglandin leading to vasodilation —> vasopressin?
positive inotropes
ephedrine (0.03-0.1 mg/kg IV bolus)
improves BP without decreasing uterine blood flow
dobutamine and dopamine
improve maternal BP but decrease uterine blood flow
aggressive fluids if able!
management of newborns:
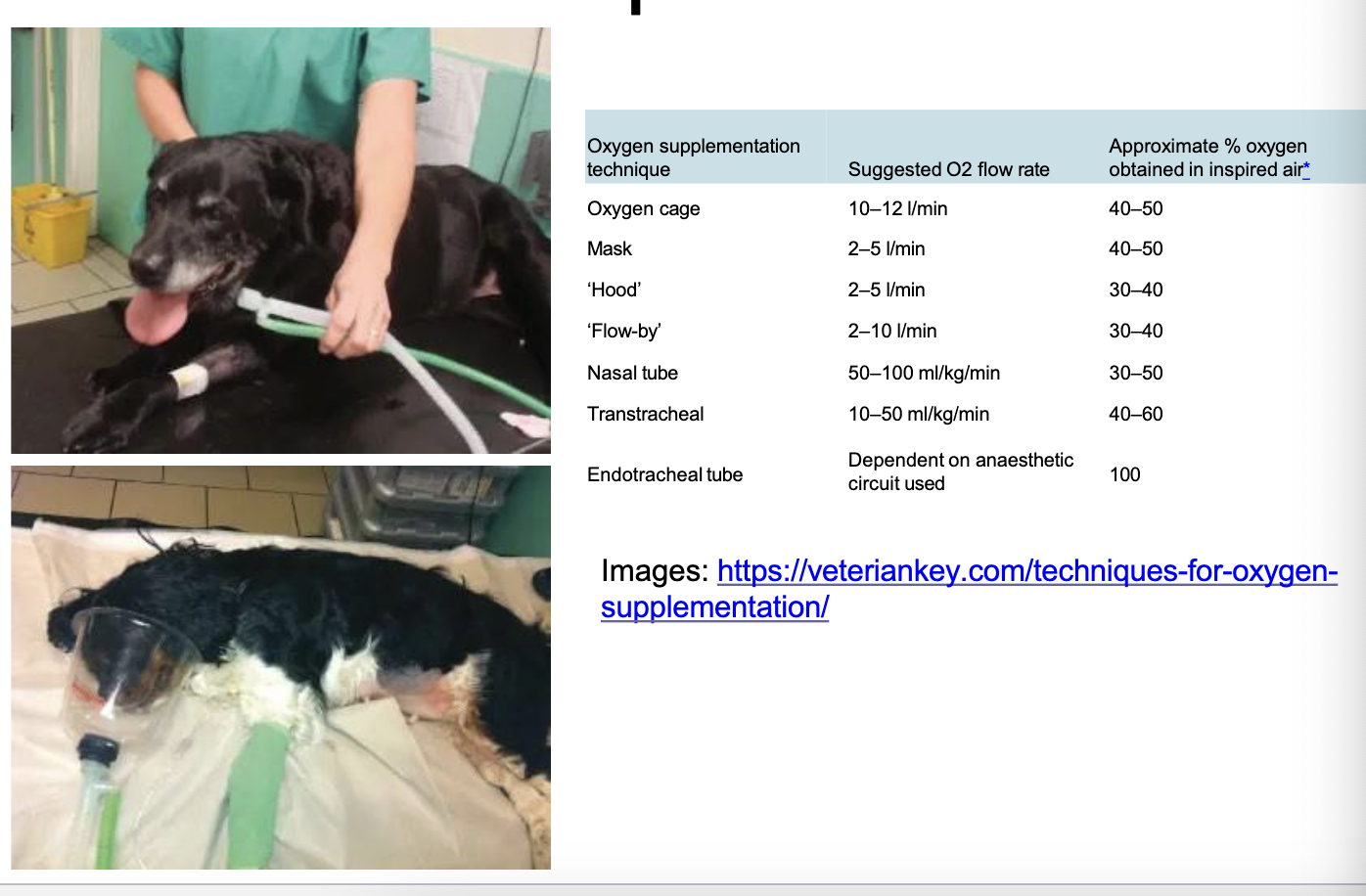
fetal oropharyngeal cavities must be cleaned/suctioned to avoid upper airway obstruction
if bradycardic (HR should be >180 bpm) —> supplement with oxygen, make sure able to breathe and oxygenate
supplies to gather for management of newborns?
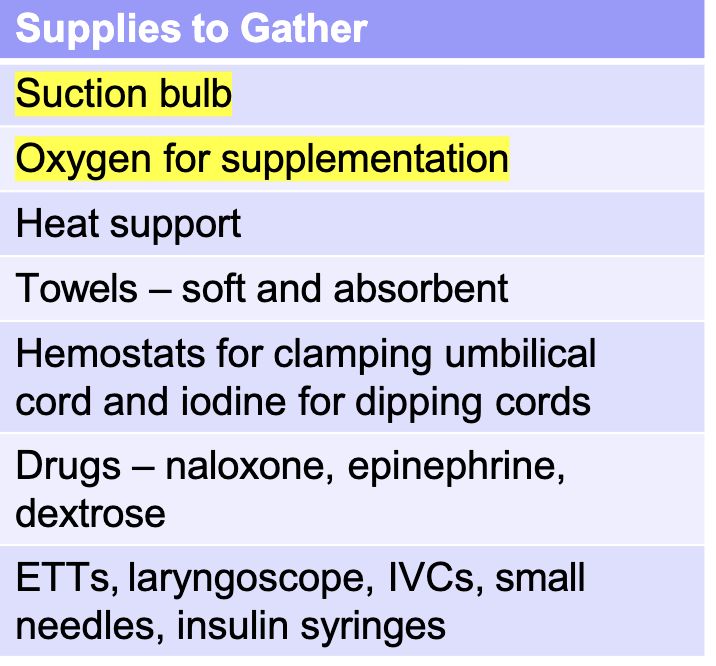
rules for puppies:
deliver as quickly as possible
rub the newborn vigorously to stimulate breathing and movement
do not swing them! Risk cerebral contusion and hemorrhage ):
supplement with O2 using face mask or in oxygen chamber
may be able to intubate with an IVC
Acupuncture at GV-26 stimulates what?
breathing! 25 g needle
what can you give under tongue of newborns to stim breathing?
epinephrine
what do you place a drop or two of under the tongue of newborns if dam was given opioids to remove fetuses?
naloxone - readily absorbed by mucous membranes
summary for c-section cases
stabilize/prep with IV fluid therapy, gastroprotectants, and preoxygenetion
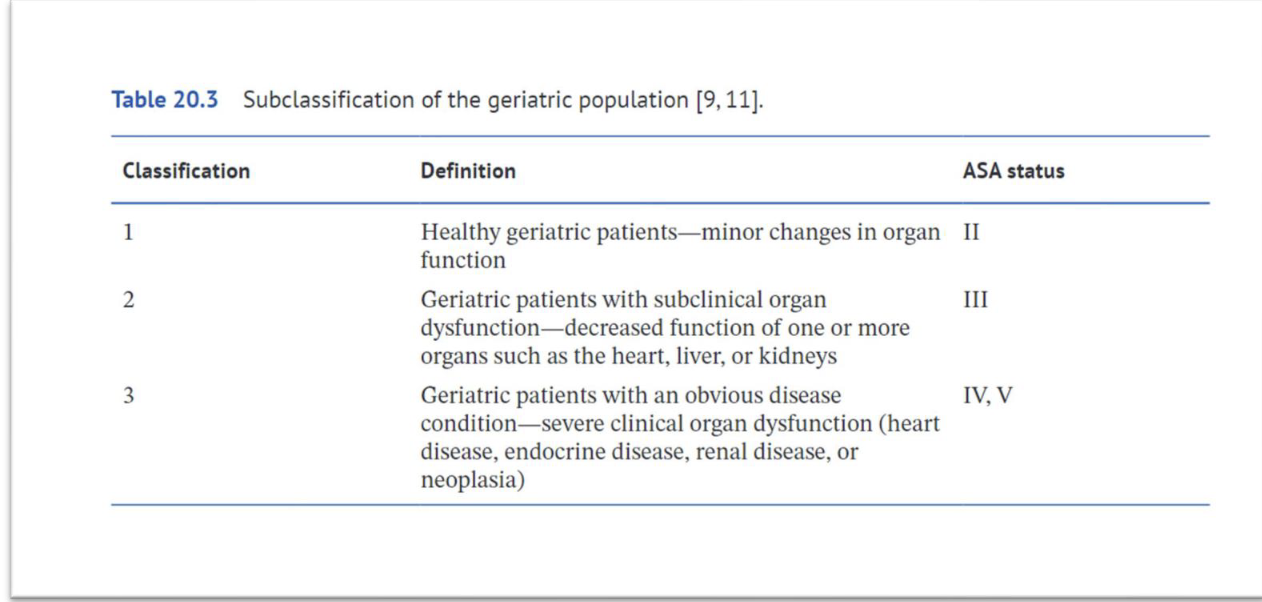
formulate a protocol based on patient’s ASA status
premed: make them work for you
induction: propofol or alfaxalone ± CRI for maintenance
local anesthesia
minimize time under GA
return dam to puppies as soon as she has revocered and send home to decrease stress/encourage bonding
post-op meds to consider
NSAIDs and line block for dam, can consider acetaminophen as well
may consider dose of opioid (e.g. buprenorphine at 10-20 mcg/kg)
stay tuned for info on longer acting buprenorphine formulations for dogs…
cats - zorbium —> transdermal buprenorphine
gaba may be added
anesthesia for neonatal and pedes patients
cardiac output is mostly heart rate dependent, so avoid bradycardia!!
airway obstruction, hypoventilation, and hypoxemia can occur; tissue oxygen demand is 2-3 x greater
hepatic and renal systems not fully functional until about 6-8 weeks, so avoid drugs with extensive metabolism or reduce dose
hypoglycemia can occur from fasting and minimal glycogen stores, so add dextrose to IV fluids. avoid high fluid rates!
no fasting
many drugs have a greater effect due to lower plasma proteins and higher free drug fraction to cross BBB
poor thermoregulatory ability, so have warming devices ready
age of neonate:
up to 4-6 weeks
age of pediatric =
6 - 12 weeks
considerations for premends in neonates and pedes cases
obtain accurate weight, use smaller syringes and dilute drugs for accurate dosing
avoid acepromazine and a2-agonists in pedes patients
younger p’s do not tolerate bradycardia like adults
midazolam is a great choice for some, but requires liver metabolism and lead to excitement
opioids may cause bradycardia, so consider anticholinergic
have naloxone available for reversal if needed
some young animals will be sedated well enough from opioid alone
glycopyyrolate lasts longer and less likely to produce sinus tachycardai than atropine
geriatric patients:
gather hx, PE!! other tests as indicated
BP… activity hx and stress test
lower drug dosages and use of short-acting drugs that can be antagonized. Balanced anesthesia plan ideal
careful titration of IV fluids before, during, and after anesthesia
decreasing mental status may mean prolonged recoveries in some
remember…
AGE IS NOT A DISEASE!