Clin Pharm - Metabolic Disorders
1/94
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
95 Terms
is defined as elevated total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), or triglycerides (TG); low high-density lipoprotein cholesterol (HDL-C); or a combination of these abnormalities.
Dyslipidemia
Primary Dyslipidemia
Genetic defects resulting in hypercholesterolemia (e.g., Familial Hypercholesterolemia).
Secondary Dyslipidemia
Acquired via diet, medications (thiazides, steroids), or comorbidities (obesity, diabetes).
Key Lipoprotein Factors
LDL-C
HDL-C
Triglycerides
What lipoprotein?
The primary carrier of cholesterol; strongly associated with ASCVD risk.
LDL-C
What lipoprotein?
Facilitates reverse cholesterol transport; low levels are an independent risk factor
HDL-C
What lipoprotein?
Transported via VLDL and chylomicrons; levels >500 mg/dL increase pancreatitis risk.
Triglycerides
Lipid-Protein Complexes
Apolipoproteins
Atherogenic Particles
HDL
__ are hydrophobic and require transport vehicles in the blood.
Cholesterol, triglycerides, and phospholipids
What Lipid-Protein Complexes?
Provide structural integrity and direct receptor binding.
Apolipoproteins
What Lipid-Protein Complexes?
Include LDL, VLDL, and remnant particles.
Atherogenic Particles
What Lipid-Protein Complexes?
Facilitates reverse cholesterol transport from vessels to liver.
HDL
is a progressive process initiated by migration of LDL-C and remnant lipoprotein particles into vessel walls.
Atherogenesis
Mechanism of Atherogenesis
LDL-C and remnant particles move into vessel walls.
Migration
Mechanism of Atherogenesis
Particles undergo oxidation and macrophage uptake.
Oxidation
Mechanism of Atherogenesis
Unregulated uptake leads to development of foam cells.
Foam Cells
Mechanism of Atherogenesis
Development of atherosclerotic plaques with a fibrous cap.
Plaque
Mechanism of Atherogenesis
Degradation of collagen leads to instability and thrombosis.
Ruptureasymptomatic
Dyslipidemic Patients are typically ___ for years until ASCVD develops.
asymptomatic
Dyslipidemia Ischemic Symptoms:
Chest pain, palpitations, shortness of breath.
Dyslipidemia Physical Signs:
○ Eruptive Xanthomas
○ Peripheral polyneuropathy
○ Abdominal obesity
Dyslipidemia Comorbid Assessment:
Hypertension, Diabetes, CKD status.
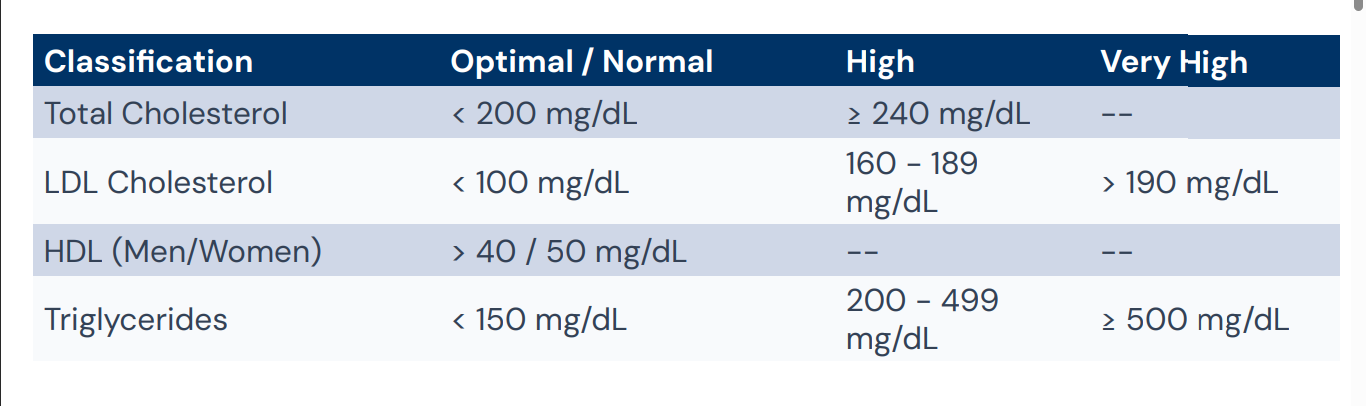
Adult Lipid Classification
For primary prevention (ages 40-79), use the ASCVD Risk Estimator Plus. A risk ___% suggests benefit from initiating statin therapy.
≥7.5
LDL estimation formula
Friedewald Equation
General Treatment Approach for dyslipidemia
Lifestyle First
Statins as Gold Standard
Combination Therapy
Risk-Based Decisions
General Treatment Approach for dyslipidemia:
__ are first-line for all lipoprotein disorders.
Therapeutic lifestyle changes (TLC)
General Treatment Approach for dyslipidemia:
___ are drugs of choice for reducing CV events.
HMG-CoA reductase inhibitors
General Treatment Approach for dyslipidemia:
Add ___ if LDL goals are not met with maximally tolerated statins.
ezetimibe or PCSK9 inhibitors
General Treatment Approach for dyslipidemia:
Initiate therapy based on individual __risk, not just plasma levels.
ASCVD
Non-Pharmacologic Treatment for dyslipidemia
Nutrition: Mediterranean pattern; limit saturated/trans fats; increase fiber.
Activity: Moderate-to-vigorous intensity activity 3-4x/week (40 mins/session).
Counseling: Smoking cessation; weight management (target 5-10% loss).
Medications used in Dyslipidemia
Statins
PCSK9 Inhibitors
Targeting Triglycerides (TG) [Fibrates (Gemfibrozil, Fenofibrate) and Omega-3 PUFAs]
Cholesterol Absorption Inhibitors (Ezetimibe, Bile Acid Sequestrants)
Adjunct and Non-Statin Therapies (Niacin,Mipomersen,Lomitapide)
Interrupt the rate-limiting step in cholesterol biosynthesis.
HMG-CoA Reductase Inhibitors
HMG-CoA Reductase Inhibitors LDL-C reduction:
20% - 60%.
HMG-CoA Reductase Inhibitors HDL-C increase:
6% - 12%.
Proven reduction in CV mortality
HMG-CoA Reductase Inhibitors
Potency Rank of statins:
Rosuvastatin > Atorvastatin > Pitavastatin >
Simvastatin > Lovastatin.
Pharmacologic Treatment for dyslipidemia LDL-C Lowering
High Intensity: Avg >=50% Reduction
Moderate Intensity: 30% to 49% Reduction
Low Intensity: <30% Reduction
High-Intensity Statins Dosing Examples
Atorvastatin 40-80 mg
Rosuvastatin 20-40 mg
Moderate-Intensity Dosing Examples
Atorvastatin 10-20 mg
Rosuvastatin 5-20 mg
Simvastatin 20-40 mg
Low-Intensity Dosing Examples
Simvastatin 10 mg
Pravastatin 10-20 mg
Lovastatin 20 mg
Simvastatin 80 mg is not recommended for initiation due to __.
myopathy risks
Reported by 10-25% of users. Includes myalgia (achiness/cramps) and weakness.
Statin-Associated Muscle Symptoms
Statin-Associated Muscle Symptoms:
Rare but fatal. CK > 10x ULN with "tea-colored" urine.
Rhabdomyolysis
Management Strategies Statin-Associated Muscle
Switch to hydrophilic statin (Rosuvastatin).
Every-other-day dosing with long half-life agents.
Rule out Vitamin D deficiency or hypothyroidism
Human Monoclonal Antibodies
Prevents LDL receptor degradation, allowing more receptors on the cell surface to clear LDL-C from circulation.
PCSK9 Inhibitors
LDL-C reduction of PCSK9 Inhibitors:
Up to 60%.
PCSK9 Inhibitors administration
Subcutaneous injection biweekly or monthly
PCSK9 Inhibitors Limitation
High cost and injection site reactions.
Targeting Triglycerides (TG) drugs
Fibrates (Gemfibrozil, Fenofibrate)
Omega-3 PUFAs
This drug’s Primary use is TG > 500 mg/dL to prevent pancreatitis
Fibrates (Gemfibrozil, Fenofibrate)
This drug increases statin concentrations (SAMS risk).
Gemfibrozil
Fenofibrate is preferred in __
combination therapy.
This drug in 2-4g/day reduces TG and VLDL secretion.
Omega-3 PUFAs
FDA approved for CV risk reduction.
Icosapent Ethyl (Vascepa)
Potential side effect of Omega-3 PUFAs:
Prolonged bleeding time.
Cholesterol Absorption Inhibitors
Ezetimibe
Bile Acid Sequestrants
What Cholesterol Absorption Inhibitors:
Reduces LDL-C (15-24%) by inhibiting NPC1L1 protein in the small intestine. Preferred adjunct therapy
Ezetimibe
What Cholesterol Absorption Inhibitors:
Reduce LDL by 13% - 20%
Reduce CV events when used as monotherapy.
First line during pregnancy
Bile Acid Sequestrants
Bile Acid Sequestrants examples
Colesevelam, Colestipol, Cholestyramine
Gemfibrozil should not be used with statins due to glucuronidation interference; use __if combination is required.
fenofibrate
What Adjunct and Non-Statin Therapies?
Lowers TG levels (20%–50%) by inhibiting lipolysis with a ↓ in free FA in plasma and ↓ hepatic esterification of TG.
Niacin
Niacin is contraindicated in?
px with active liver disease and active PUD
What Adjunct and Non-Statin Therapies?
An oligonucleotide inhibitor of apolipoprotein B-100 synthesis.
Mipomersen
What Adjunct and Non-Statin Therapies?
Indicated in patients with homozygous FH.
Mipomersen
What Adjunct and Non-Statin Therapies?
Adds 25% reduction in LDL-C when combined with other lipid-lowering therapy
Mipomersen
What Adjunct and Non-Statin Therapies?
A microsomal triglyceride transfer protein (MTP) inhibitor
Lomitapide
What Adjunct and Non-Statin Therapies?
Reduced LDL-c by 40% in patients on maximum tolerated lipid-lowering therapy and LDL apheresis
Lomitapide
Dyslipidemia in Diabetes Mellitus phenotype
Hypertriglyceridemia, low HDL-C, and dense, highly atherogenic LDL particles.
Dyslipidemia in Diabetes Mellitus first line tx
Statins are mandatory as they reduce mortality even if LDL is "near normal."
Dyslipidemia in Diabetes Mellitus combination therapy
Statin + Fibrate did not show additional CV benefit in trials (ACCORD).
Dyslipidemia in Diabetes Mellitus Glycemic Control
Colesevelam can modestly improve both A1C and LDL-C.
Hypertriglyceridemia Management
Lifestyle: Weight loss, carb restriction, alcohol avoidance.
Secondary: Address DM control and medications (e.g. Protease inhibitors).
Statin: Initiate for ASCVD risk reduction if TG 175-499.
Fibrate: Add if TG > 500 to prevent Pancreatitis.
Monitoring Intervals of dyslipidemia in Short-term:
Complete lipid panel 4-12 weeks after initiation or dose adjustment.
Monitoring Intervals of dyslipidemia in Long-term:
Repeat lipid panel every 3-12 months for adherence.
Dylipidemia safety monitoring
Routine liver enzyme and CK monitoring is NOT recommended unless symptomatic.
Dyslipidemia goals of treatment
The reduction of ASCVD-related events:
Prevention of MI and Ischemic Stroke
Reduction in revascularization procedures
Improvement in intermittent claudication
Reduction in CV-related mortality
Dyslipidemia Takeaways
● Statins are the primary tool for CV risk reduction.
● Lifestyle (TLC) is the foundation of all therapy.
● Risk-based treatment (ASCVD) is superior to number-base treatment.
● Monitor for safety (SAMS) and adherence at every visit.
Obesity occurs when there is a chronic imbalance between:
• Energy Intake: Dietary calories.
• Energy Expenditure: BMR, thermic effect of food, and physical activity.
Result of obesity based on energy homeostasis imbalance:
Increased Energy Storage Over time, this positive net balance leads to excess adipose accumulation.
Obesity Multifactorial Factors
Genetic: Primary determinants of fat distribution and metabolic set-points in some individuals.
Environmental: Sedentary lifestyles, high-fat food availability, and cultural/religious factors.
Physiologic: Neurotransmitter regulation of appetite networks and leptin signaling.
The brain regulates caloric intake through complex neurotransmitter signaling:
Stimulators,Suppressors,Hormonal Input
What neurotransmitter signaling in obesity:
Neuropeptide Y (NPY), Agouti-related peptide (AgRP).
Stimulators
What neurotransmitter signaling in obesity:
Pro-opiomelanocortin (POMC), Serotonin, Dopamine.
Suppressors
What neurotransmitter signaling in obesity:
Leptin (satiety) and Ghrelin (hunger).
Hormonal Input
Secondary Causes of Weight Gain
Medical Conditions and Psychiatric/Genetic
Medical conditions as secondary cause of weight gain
• Cushing disease
• GH Deficiency
• Insulinoma
• Leptin Deficiency
• Polycystic Ovary Syndrome (PCOS)
Psychiatric/Genetic as secondary cause of weight gain
• Depression & Schizophrenia
• Binge-eating disorder
• Prader-Willi Syndrome
• Bardet-Biedl Syndrome