FSHN 3620 • Exam 1 - Study Guide Questions
1/78
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
79 Terms
Principles of the Science of Nutrition
Food is a basic need of humans.
Foods provide energy (calories), nutrients, and other substances needed for growth and health.
Health problems related to nutrition originate within cells.
Poor nutrition can result from both inadequate and excessive levels of nutrient intake.
Humans have adaptive mechanisms for managing fluctuations in food intake
Malnutrition can result from poor diets and from disease states, genetic factors, or combinations of these causes.
Some groups of people are at higher risk of becoming inadequately nourished than others
Poor nutrition can influence the development of certain chronic diseases.
Adequacy, variety, and balance are key characteristics of healthy dietary patterns.
There are no “good” or “bad” foods.
Community-level assessment
can be estimated using existing vital stat data, seeking opinions of target group members & local health experts and making observations.
SNAP
Food banks & soup kitchens
WIC
Individual-level assessment
Data from all 4 are needed to describe one’s nutritional status.
Clinical/physical assessment
Dietary assessment
Anthropometric assessment
Biochemical assessment
Clinical/physical assessment
visual inspection of a person by a trained RDN or other qualified professional to note physical features that may suggest nutrition related problems.
Dietary Assessment
24 hr Recall
List of foods & beverages consumed in last 24 hrs
Dietary Assessment
Dietary History
interview by trained professional, 1 ½ hrs long; includes 24 hr recall, FFQ; more complete accurate data
Dietary Assessment
FFQ
Estimate food & nutrient intake of groups of people
Dietary Assessment
USDAs Multiple-Pass method
Quick list
Forgotten foods
Time & occasion
Detail cycle
Final probe
Dietary Assessment
Healthy Eating Index
assess a person's reported dietary intake based on 10 dietary components that cover intake of the USDA’s basic food groups.
Dietary Assessment
Anthropometric Assessment
measures of body size (H,W, % body fat, bone density, & head/waist circumferences)
Dietary Assessment
Biochemical Assessment
nutrient & enzyme levels, gene characteristics, & other biological markers.
Dietary Assessment
National Nutritional Health
nutrition surveillance & nutrition monitoring
Human chorionic gonadotropin (hCG)
Indicates pregnancy on a pregnancy test
Should approximately double every 2 days in the first weeks of pregnancy
Variance of this may indicate a problem
functions:
Initiates production of estrogen & progesterone
Stimulates growth of the endometrium
Likely contributes to nausea & vomiting symptoms
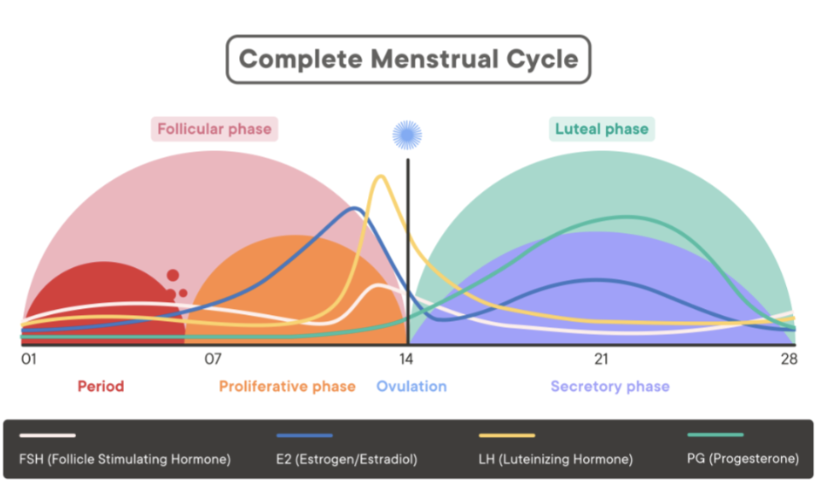
4 Major Hormones in Female Reproductive System
Follicle-stimulating hormone (FSH): Stimulates growth of ova
Luteinizing hormone (LH): Stimulates secretion of progesterone
Estrogen
Progesterone
Describe the Menstrual Cycle
Follicular Phase
Day 1-7: Period
Day 7-14: Proliferative Phase → Estrogen surges
Day 14: Ovulation → LH surges, FSH lesser surge
Luteal Phase
Day 14-28: Secretory Phase → Progesterone & Estrogen surge
Purpose of menstrual cycle
To prepare ovum for fertilization by sperm + uterus for implantation of a fertilized egg
Results from complex interactions among hormones secreted by the hypothalamus, pituitary gland, & ovaries
Luteinizing hormone (LH)
produced by the pituitary gland that stimulates ovulation, the development of the corpus luteum (which secretes progesterone), and the production of testosterone in men.
Estrogen
Enlargement of uterus
Enlargement of breast tissue
Increases blood circulation
Increases protein synthesis
Increases lipid formation and storage
Progesterone
Smooths uterine and GI muscles
Lowers esophageal sphincter tone, causing increased heartburn
Can lead to constipation
Proper functioning of placenta
Promotes growth of endometrium
Promotes lipid accumulation
Loosens joints and ligaments
Prepare breasts for lactation
Decreases immune system function
Anti-inflammatory effect
Follicle-stimulating hormone (FSH)
produced by the pituitary gland that stimulates ovarian follicle growth and maturation, estrogen secretion, and endometrial changes characteristic of the first portion of the menstrual cycle in women. It stimulates sperm production in men.
Gonadotropin-releasing hormone (GnRH)
produced in the hypothalamus and is responsible for the release of FSH & LH by the pituitary gland.
Energy deficits can suppress this
Importance of preconception nutrition
Optimized nutrition → optimal fertility → successful pregnancy
Folate (natural) /Folic Acid (supplement) – 400 mcg/day
Prevents NTDs & SGA newborns
Prevents spina bifida & anencephaly
Iron
Fertility
Brain dev.
Properly timed delivery
Iodine – thyroid hormone function
Zinc
Important in males & females
Sperm maturation & testosterone syn.
Egg quality & maturation
Fertilization
DNA syn.
Antioxidants – Protect eggs & sperm from oxidative stress
Limit or omit alcohol
Infertility
fail to conceive within 12 months of attempting pregnancy.
Infertility risk factors for men & women
Endocrine/hormonal abnormalities
Severe stress
STDs: pelvic inflammatory disease (PID)
Endometriosis: abnormal growth of endometrium in other places.
Toxic substances & environmental contaminants (heavy metals)
caffeine, alcohol, nicotine, etc.
Underweight & overweight
Old age >40
Potential health problems of women with Celiac
Amenorrhea
Increased rate of miscarriage
Fetal growth restriction
Low birth weight deliveries
Short lactation duration
Potential health problems of men with Celiac
Alterations in androgens
Delayed sexual maturation
Hypogonadism: deficiency of sex hormones, poor development & functioning of reproductive system.
How does PCOS affect fertility?
Infertility is primarily due to the absence of ovulation
Polycystic ovaries: presence of a high number of immature eggs surrounded by fluid-filled sacs in the ovary.
How does Celiac disease impact fertility?
Somewhat high to substantially high rates of infertility
Malabsorption-induced deficiencies in nutrients like zinc, folate, & iron
Direct inflammation on intestines & other tissues
How does diabetes impact fertility?
Tetrogenic
Congenital abnormalities
Malformations of pelvis, CNS, and heart
Increased risk of miscarriage
Physiological changes during the anabolic phase (first half) of pregnancy
Approximately 10% of fetal growth
Mother’s body is building capacity to deliver all the blood, oxygen, & nutrients the baby will need during the second half of pregnancy
Increased appetite
Increased anabolic hormones
Decreased exercise tolerance
Physiological changes during the catabolic phase (second half) of pregnancy
Approximately 90% of fetal growth
Support fetal development by mobilization of stored nutrients to the developing fetus
Increased catabolic hormones
Increased exercise tolerance
Increased req. of fetus & preparation for birth & lactation
Cardiovascular system changes in pregnancy
Increased heart rate
Cardiomegaly: increased heart size, move up to the left.
Decreased BP (middle of pregnancy)
Cardiac output increases 30 - 50%
Hematological system changes in pregnancy
Plasma volume increases by 50%
Increase in oxygen carrying capacity
Increase in clotting factors
Respiratory system changes in pregnacy
40% increase in ventilation (tidal volume)
Increased oxygen consumption
Renal system changes in pregnancy
Kidneys grow in size
Increase in sodium retention
Increased risk of UTI
Gastrointestinal system changes in pregnancy
Progesterone decreases esophageal sphincter tone and GI track muscle tone
Slower GI transit time
Nausea (70%), vomiting (40%)
Heartburn
Constipation
Immune system changes in pregnancy
Suppressed immunity because progesterone
Increased risk of infections
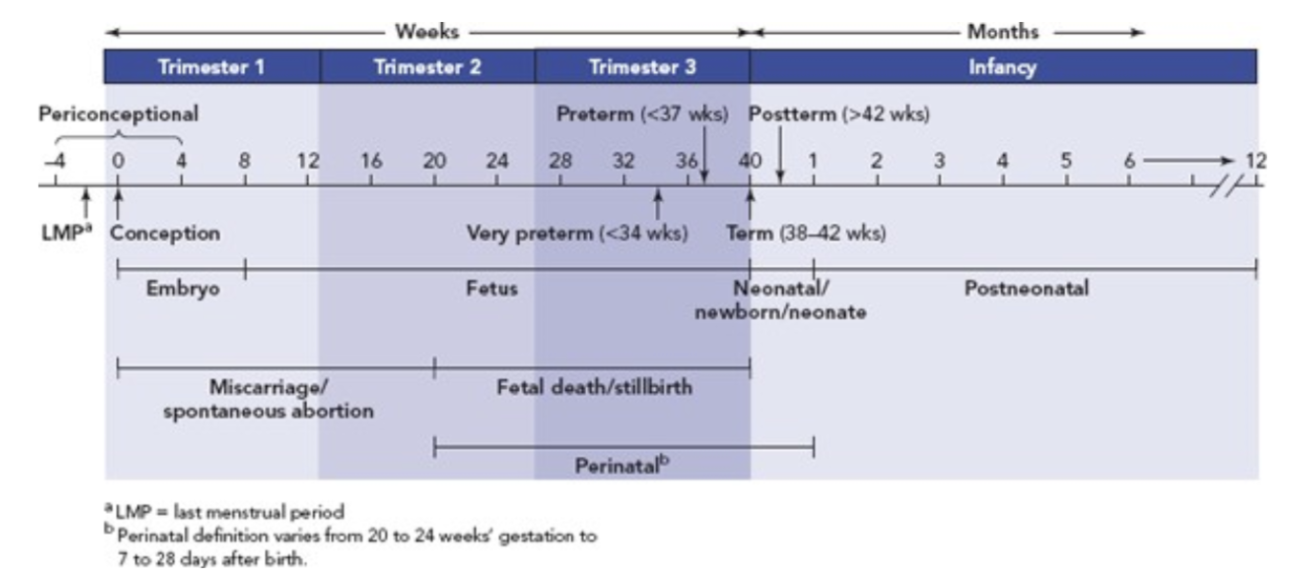
Fetal growth stages, starting from conception
Day 1:
Conception – 1 zygote exists
Fetal growth stages, starting from conception
Day 2-3
8 cells formed (morula) & enter uterine cavity
Fetal growth stages, starting from conception
Day 6-8
Morula becomes fluid filled, now a blastocyst (250 cells)
Fetal growth stages, starting from conception
Day 10
Embryo implants into uterine wall where glycogen accumulates
Fetal growth stages, starting from conception
Day 12
Embryo (1000s of cells) differentiation, uterine placental circulation being formed
Fetal growth stages, starting from conception
Week 4
¼ in long, rudimentary head, trunk, arms, heart “practices” beating, spinal cord & 2 major brain lobes present.
Fetal growth stages, starting from conception
Week 5
Rudimentary kidney, liver, circulatory sys, eyes, ears, mouth, hands, arms, and GI tract; heart beats 65x/min (circulating own blood)
Fetal growth stages, starting from conception
Week 7
½ in long, weighs 2-3 g, brain sends impulses, GI tract produces enzymes, kidney eliminates some waste products, liver produces RBCs, muscles work
Fetal growth stages, starting from conception
Week 9
Embryo is a fetus
Fetal growth stages, starting from conception
Month 3
Weighs 1 oz, primitive egg & sperm cells developed, hard palate fuses, breathes in amniotic fluid
Fetal growth stages, starting from conception
Month 4
Weighs 6 oz, placenta diameter is 3 in
Fetal growth stages, starting from conception
Month 5
Weighs 1 lb, 11 in long, skeleton begins to calcify, hair grows
Fetal growth stages, starting from conception
Month 6
14 in long, fat accumulation begins, permanent teeth buds form, lungs, GI tract & kidneys formed (not fully functional)
Fetal growth stages, starting from conception
Month 7
Gains ½ – 1 oz / day
Fetal growth stages, starting from conception
Month 8-9
Gains 1 oz / day, stores fat, glycogen, iron, folate, vit B6 & 12 , riboflavin, calcium, magnesium, vit A, E & D; functions of organs continue; growth declines near term; placenta weighs 500-650 g (1-1 ½ lb) at term
Placenta functions
Exchanges O₂ and CO₂ (works as lung)
Two separate circulatory systems
Mom’s blood and baby’s blood don’t mix
Transfers nutrients (works as digestive system)
Removes wastes (works as kidney)
Immune barrier; double lining of cells
Secretes hCG, estrogen, progesterone, hCS
Cannot block all harmful substances (alcohol passes)
Develops gradually during the first 3 months of pregnancy
Large spongy disc
You should NOT eat the placenta
CHO metabolism in pregnancy — first half
estrogen- & progesterone-stimulated increases in insulin production & conversion of glucose to glycogen and fat
CHO metabolism in pregnancy — second half
rising levels of hCS & prolactin from mother’s pituitary gland to inhibit glucose → glycogen & fat
Insulin resistance builds up, increasing reliance on fats for energy
Increased liver production
CHO metabolism in pregnancy — third trimester
fasting maternal glucose levels decline bc of increased utilization of glucose by fetus
Post-meal blood glucose conc. are elevated and remain so (longer than pre-pregnancy)
Fat metabolism in pregnancy — first half
accumulation of maternal fat stores
Fat metabolism in pregnancy — second half
enhanced fat mobilization
Preeclampsia
typically diagnosed after the 20th week of pregnancy. It is characterized by BP readings that exceed 140/90 mm Hg documented on two occasions by BP measurements made at least four hours apart.
Preeclampsia symptoms
headache, blurred vision, abdominal pain, low platelet count, abnormal liver enzyme values
Preeclampsia characteristics
Oxidative stress, inadequate antioxidant defenses, inflammation, & endothelial dysfunction
Platelet aggression & blood coagulation due to deficits of prostacyclin relative to thromboxane
Blood vessel spasms & constriction, restricted blood flow
Increased blood pressure
Insulin resistance
Adverse maternal immune system responses to the placenta
Elevated blood TGs, free FAs & chol
Pregnancy exercise recommendations
Frequent rest periods
Don’t hold breath
Don’t exercise until exhaustion
Avoid exercise in heat & humidity
No twisting & bouncing
Non-weight bearing → cycling, swimming, yoga
Drink plenty of liquids
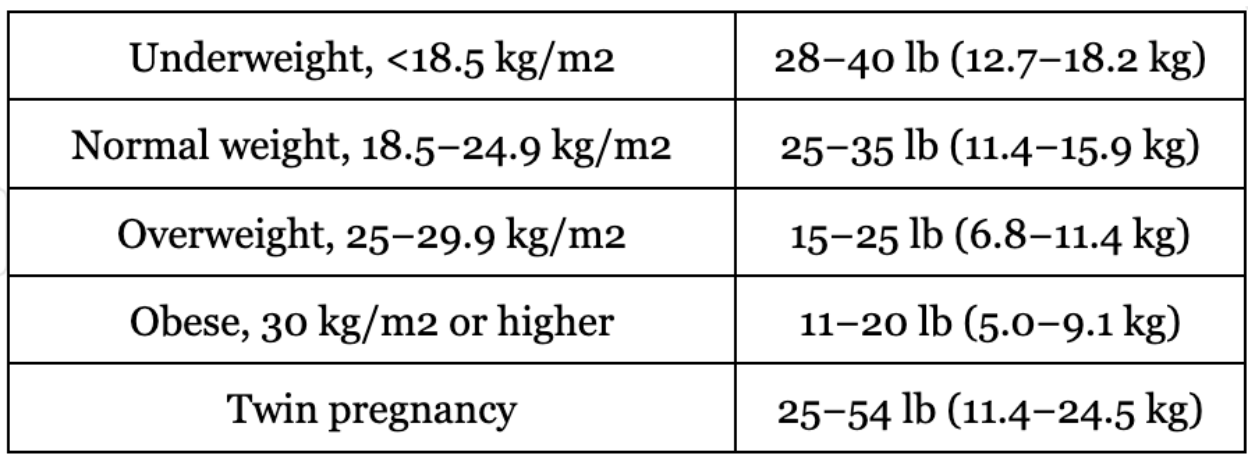
Weight gain (know this table)
Protein needs in pregnancy
Increased protein & N – 2 lbs pure protein accumulated
Micronutrient needs in pregnancy
Vit D → 15 mcg
Vit A → <10,000 IU
Iron → 27 mg/day
Folate → 300 mcg
Increased sodium & calcium → bone formation
Magnesium → 350 mg
Iodine → 220 mcg
Calcium → 1,000-1,300 mg
Birth defects caused by nutritional issues
Neural tube defects – Folate deficiency
Fetal malformations – Vitamin A deficiency & toxicity
PKU – genetic factor
Congenital abnormalities & hypothyroidism – Iodine deficiency
Abnormal bone development → Vitamin D deficiency
High Risk Pregnancies
Age: 18> and >40
Low birthweight
Perinatal death
C-section
Cephalopelvic disproportion: head to large for birth canal
Preeclampsia
Iron-deficiency anemia
Delayed, reduced educational achievement
Poverty
Poor diet quality
High Risk Pregnancies
Multifetal (mother’s risks)
Preeclampsia
Iron-deficiency anemia
Gestational diabetes
Hyperemesis gravidarum
Placenta previa
Kidney disease
Fetal loss
Preterm delivery
C-section
High Risk Pregnancies
Multifetal (newborn’s risks)
Neonatal death
Congenital abnormalities
Respiratory distress syndrome
Intraventricular hemorrhage
Cerebral palsy
Low birthweight
High Risk Pregnancies
Obesity
Gestational diabetes
Preeclampsia
PP hemorrhage
PP depression
Preterm delivery
High Risk Pregnancies
Diabetes (mother’s risks)
Caesarean delivery
Shoulder dystocia
Increased risk for preeclampsia
Increased risk of type 2 diabetes, hypertension, & obesity later in life
Increased risk for gestational diabetes in a subsequent pregnancy
Hypoglycemia
Maternal death
High Risk Pregnancies
Diabetes (newborn’s risks)
Stillbirth
Spontaneous abortion
Congenital anomalies
Macrosomia (10lb)
Neonatal death
Neonatal hypoglycemia, hypocalcemia, & hyperbilirubinemia
Increased risk of insulin resistance, type 2 diabetes, high BP, & obesity later in life
Factors contributing to high risk pregnancy
Socioeconomic status
Lifestyle factors
Short inter-pregnancy interval
High Parity
Pre-existing health conditions
Lifestyle Factors
Mother’s Body Weight
Underweight - premature membrane rupture, anemia
Obesity – LGA baby, hypertension, diabetes
Medications & toxins in pregnancy
Avoid all of them unless approved by a doctor
May cause: birth defects, bleeding, miscarriage, infant death
Classifications:
A → controlled studies show no risk to fetus
B → no controlled studies on humans, animal studies show no risk to fetus
C → no controlled studies on humans or animals
D → evidence of human risk to fetus, benefits may outweigh risks
X → controlled studies in animals & humans demonstrate fetal abnormalities
Mineral metabolism
Sodium accumulation in mother, placenta, & fetus
Calcium absorption & mobilization
Iron stores accumulate in fetus late pregnancy
Pregnancy outcome measures
Today 2.5% babies die before first birthday
Most desirable birthweight: 7lb 11oz to 8lb 13oz (3500 to 4000 g)
Less likely to develop heart & lung diseases, diabetes, & hypertension for the rest of their lives
Female intra-abdominal fat
reduces SHBG because of elevated blood insulin levels, prompts ovaries to release more testosterone, disrupting egg development.
Insulin resistance
Oxidative stress
Chronic inflammation
Metabolism syndrome
Male intra-abdominal fat
fat contains aromatase that converts testosterone → estradiol
Low testosterone & elevated estradiol
Increased estradiol inhibits secretion of LH & FSH which can lower testosterone synthesis, then decreases sperm production promoting infertility
Gestational diabetes
Carbohydrate intolerance with onset of, or first recognition in, pregnancy.
It is closely related to type 2 diabetes.