Week Ten - Medical Conditions in Pregnancy
1/44
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
Respiratory Changes in Pregnancy
diaphragm ^ 4cm
rib cage diameter increases 2cm
breathing becomes thoracic not abdominal
O2 consumption and RR ^
tidal volume increases
increased CO2 release
Pulmonary Thromboembolic Disease
Leading cause of maternal mortality accounting for approximatley 10% of pregnancy related deaths
It results from a blood clot that obstructs the pulmonary artery, often originating from deep vein thrombosis. Risk factors include prolonged immobility, cesarean delivery, and obesity.
Most common chronic medical condition in pregnancy?
Asthma
Reasons for Respiratory Distress in Pregnancy
asthma
tuberculosis
smoking & obesity
cystic fibrosis
viruses
anemia
pulmonary embolus
Pulmonary Oedema
A condition characterized by excess fluid in the lungs, leading to breathing difficulties. It can be caused by heart problems, high blood pressure, or fluid overload, particularly in pregnant women.
Can be contributed to by left heart failure, preclampsia etc..
How does Preeclampsia result in Pulmonary Oedema?
increased LV afterload
reduced systolic or diastolic function = reduced CO
pulmonary hypertension
Uncontrolled Asthma in Pregnancy Risks
higher risk of gestational diabetes
higher risk of gestational hypertension
risk of placental abruption
risk of pulmonary admissions
increased risk of babies being born premature or low birth weight
COVID 19 Maternal Risk
mild disease
higher risk of developing higher risk illness
COVID 19 Fetal Risk
increases risk of complications for baby (ie. stillbirth, prematurity)
no risk of congential defects or miscarriadge in early pregnancy
How is Stable Asthma managed in pregnancy
symptom relievers (ie. ventolin)
symptom preventers (ie. symbicort)
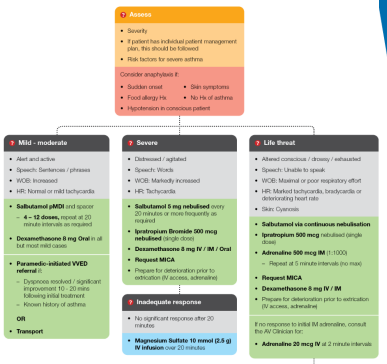
Asthma in Pregnancy Management AV
SAME AS NON PREGNANT PATIENTS - but be aware of quick deterioration (get backup!)
Diabetes T1 VS T2
T1: chronic condition in which pancrease stops producing insulin, genetic
T2: body becomes resitant to insulin/doesnt make enough, life style
T1DM Management in Pregnancy
continuous BSL monitoring
manage morning sickness and vomiting
precautions around excercise
glucagon kit on hand
regular small meals
T2DM Management in Pregnancy
increase insulin requirements
increased BSL checks
no oral hypogylcaemics other than Metformin!
anti lipid medications to be ceased
Gestational DM
Diabetes diagnosed in the second or third trimester of pregnancy that was not clearly overt diabetes prior to gestation.
Pathophysiology of Glucose Regulation in HEALTHY PREGNANCY
early pregnancy = increase insulin sensitivity, higher risk of hypoglycemia. glucose being stored in adipose tissue for later in pregnancy
later pregnancy = hormones work to create state of insulin resitance
bsl is elevated allows for easy transfer to fetus
promotes endogenous glucose production and breakdown of fat stores
Pathophysiology of GDM
b cell dysfunction: reduced B cell mass, number or general dysfunction (or all 3!)
insulin resistance: rate of insulin stimulated glucose uptake is reduced by 54% in GDM
GDM Risk Factors
ethnic backgrounds of any kind
close family history of diabetes
>30 >40
high BMU
big baby
PHx of GDM
PHx of PCOS
rapid weight gain in early preg
Maternal Risks in GDM
preterm birth
preeclampsia
increased risk of t2dm
increased risk of induction and csection
Maternal Risks in GDM
big baby
neonatal hypoglycemia
stillbirth
increased risk of obesity, t2dm and gdm in females in future
How is GDM tested for
via oral glucose test (26-28 weeks)
0 hour: >/= 5.1, 1 hour >/= 10.0, 2 hour >/= 8.5
GDM Treatment AV
left lateral tilt
standard bsl management
alert obstetric team
General GDM Management
increased care visits
increased scans
promote low gi diet
excercise for 30min gentle every day post meals
metformin, insulin
Intrapartum Care
bsl monitoring every 2 hours
induction for poorly controlled GDMs
CTG monitoring in labour
Maternal Postnatal Care GDM
diabetic diet lifelong change
bsl monitoring
another glucose test after 6wks
Neonate Postnatal Care GDM
frequent breastfeeding
bsl monitoring every 3 hours until 3 stable bsls in a row
Heart Changes in Pregnancy
rotates up and to the left as uterus enlarges and causes diaphragm to elevate (apex at 4th ICS)
lext axis shift on ECG
systolic murmurs due to increased load, diasoltic murmurs due to increased blood flow
Why does CO increase during pregnancy?
30-50% increase due to HR
preload is increased due to the associated rise in blood volume
afterload reduced due to decline in systemic vascular resistance
CVS Changes Per Trimester
1st: systemtic vasodialtion, SVR drops, CO rises, HR slow rises
2nd: SVR plateus, CO rises, HR slow rises
3rd: CO peaks, HR peaks
Plasma & Red Blood Cell changes in pregnancy
plasma volume increases in 1st trimester, rapidly expands until 30-34/40 which helps to protect mum & baby, and meet perfusion demands
begins to increase at 8/40 and rises steadilty, supports higher oxygen metabolism
3 Kinds of Hypertension in Pregnancy
chronic hypertension
non-proteinuric pregnancy induced hypertension (GHTN)
preeclampsia
Chronic Hypertension
hypertension prior to pregnancy or BP >140/90 diagnosed before 20/40
Chronic Hypertension Risk Factors
renal disease
diabetes
obesity
age >40
HTN on OCP
Gestational Hypertension Definition
HPT > 140/90 on >2 occasions
no others signs of pre-eclampsia
occurs >20 weeks
Gestational Hypertension Risk Factors
first child with partner
obesity
diabetes
previous pre eclampsia
pre existing cardiovascular disease
age >40
Pre-eclampsia Definition
hypertension after 20 weeks gestation with other symptoms
other symptoms such as high protien urine content, DIC, convulsions, new headache, visual disturbance..
Pre-eclampsia Risk Factors
first pregnancy
pre-eclampsia in previous pregnancy
> 40 y/o
10 years since last baby
MBI >35
family history
Pre-eclampsia Pathophysiology
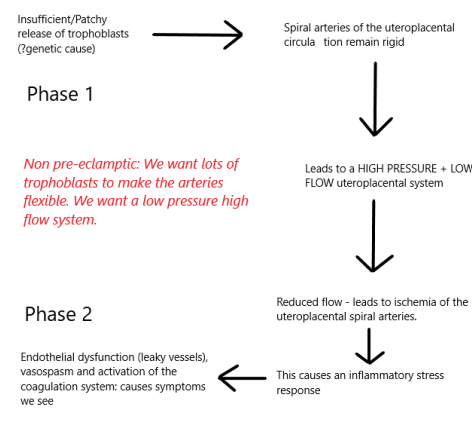
How does PreEclampsia alter the body?
CVS: hypertension with endothelial cell damage affects capilliary permeability, plasma protiens leak resulting in decreased plasma colloid pressure, hypovoleamia and haemoconentration
Coagulation: altered, increased platelet consumption which can result in DIC
Kidneys: hypertension results in vasospasm of afferent arterioles
Brain: Hypertension with CVS endothelial damage, headaches & convulsions
Liver: vasoconstriction, epigastric pain, lowered albumin and increased liver enzymes
Foeto-Placental: vasoconstriction decreased, vascular leisons can occur, hypoxia can lower fetal growth
Pre-Eclampsia Presentation
sharp rise in BP to >140/90 in 2nd half of pregnancy
increased protien in urine, lessened output
swelling sudden and severe, widespread
hyper-refexia
other symptoms such as headache, blurred vision, epigastric pain, visual disturbance, N&V, epigastric pain
HELLP Syndrome
complication of preeclampsia
stands for Haemolysis, Elevated, Liver Enzymes, Low Platelets
HELLP Risk Factors
known preclampsia
multiparity
previous Hx
Eclampsia
new onset convulsions in pregnancy
4 stages of Eclampsia
premonitory: eyes rolling, muscles twitching
tonic: violent spasm, resps cease
clonic: jerky movements, frothy bloody saliva
comatose: deeply unconscious
How do paramedics manage Pre-Eclampsia
EPOMS
monitor & prevent complications
rest and reassure, left lateral tilt, o2 8L hudson mask
manage eclampsia as per seizure CPG