Culture
1/18
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
19 Terms
what is culture?
-What is learned, shared, transmitted intergenerationally, and reflected in a group’s values, beliefs, norms, behaviors, communication, and social roles
*effect individual and group, directly and indirectly; big impact on HB
class discussion: How does culture affect health behaviors?
-attitude towards HB (ex: PA, go to the doctor every year, what symptoms valuable)
-beliefs
-norms
culture trends in the US
-Increased cultural diversity of the US
-Increased disparities in health behaviors and outcomes (*and culture effects disparities)
*15.8% US foreign born, more hispanic and multi-racial, more spanish speaking; can study multiple aspects of culture, but limited
culture transmission
-Process by which specific aspects of a culture are passed down from one generation to the next
*why can study culture at dif levels; aspects=food, holidays/rituals, language, beliefs, normative behavior (what is and isn’t normal)
culture change
-Changes in beliefs and behaviors that occur as a result of “lived experiences”
*ex lived experience=9/11 → safety, patriotic, discrimination; individual ex=college
*insight why hard to change, though can change
acculturation
-Degree to which cultural elements of mainstream culture are adopted by a small cultural group
*ex: geographic migration, nutrition research; strong relationship w/ HB
ethnocentrism
-The belief that one’s own culture is superior to all others
*can be neg or positive/beneficial (ex: preserving culture)
Race and Ethnicity
-Race: group that a person belongs to as a result of physical features
-Ethnicity: group that a person belongs to because of shared characteristics such as geographic or ancestral origins, cultural traditions, and languages (modern=social origins???)
*dif but overlap and used interchangeably
class discussion: Can race or ethnicity be a proxy for culture? (only assessment needed?)
-no; used bc easy to measure, but why does it matter in terms of health?
some diseases are more prevalent with certain races/ethnicities, but usually not biological and more bc lower socioeconomic, envionrmental factors, etc.
differences in subgroups of races (ex: Asian and BMI/obesity)
-more to it than just race/ethnicity; not much biological association, and more the culture, attitudes, beliefs, norms, etc.
culture influences on behaviors: Smoking
-Lower rates of smoking in Hispanic communities…. but U.S born Hispanics and those living in the U.S. longer have higher rates
-Importance of family approval (*indirect effect)
culture influences on behaviors: Screenings
-Mammograms and cervical cancer screenings lowest in Asian American women
-Religions focus on acceptance of natural order of life
-Life events are explained as luck or fate in Chinese culture
culture influences on behaviors: Illness Perception and Disease Management
-Pain perception (*nocireceptors periphery → CNS; dif tolerance bc dif receptors, brain interpret dif; can culture effect? maybe, at cognitive level; dif beliefs in dif cultures)
-Treatment preferences (*white people more likely to choose knee surgery, possibly socioeconomic but also could be cultural)
-May affect providers’ response and treatments (*recommend dif treatments based on patients culture)
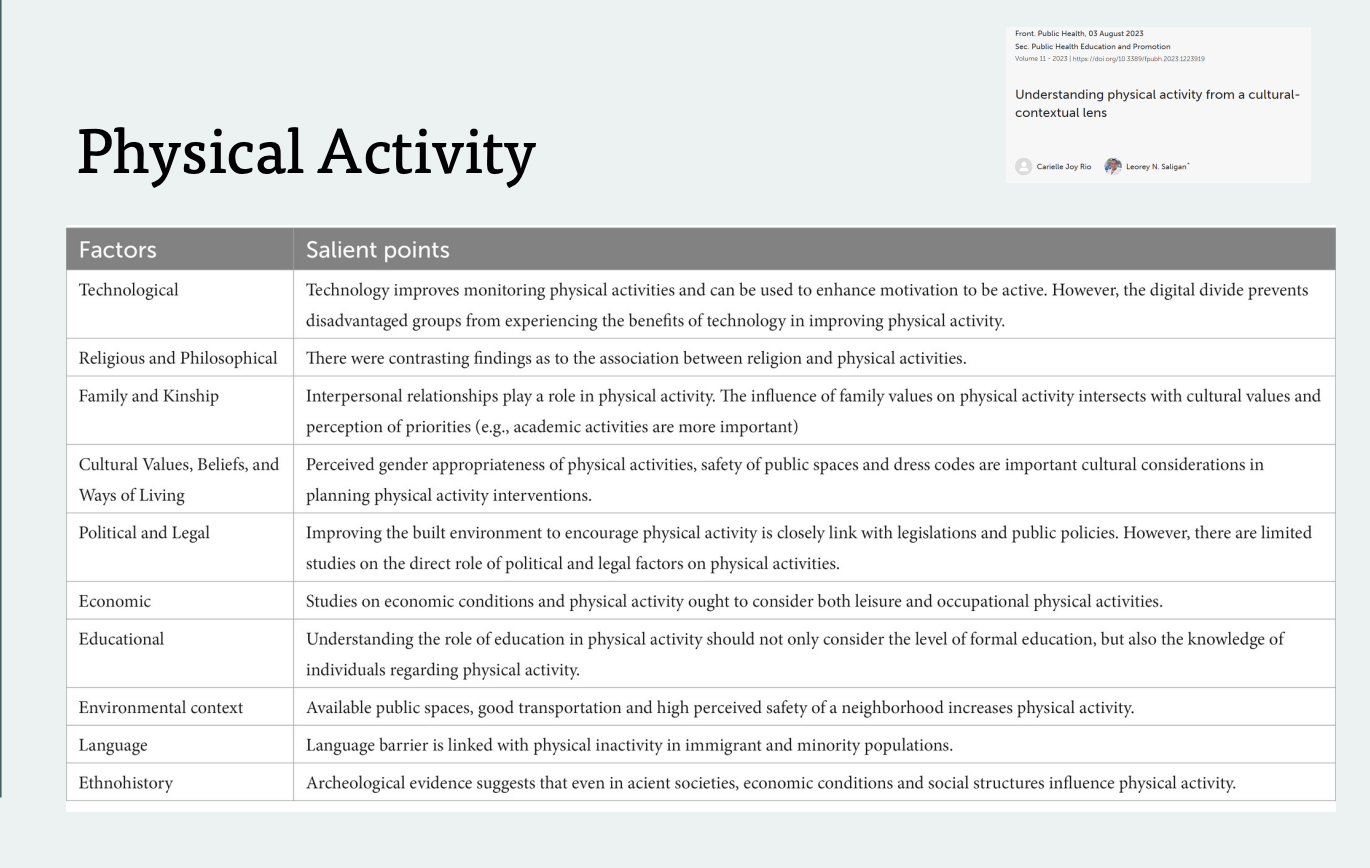
culture influences on behaviors: Physical Activity
-limited data; hard to define how culture impacts PA
*don’t memorize slide!
class discussion: How has your culture influenced your PA behavior?
-”active family” vs “movie family” impacts PA intention (so habit more important)
-sports: Irish dancing, XC skiing
-Reasons why someone active (ex: do for family); motivation for PA
-Female PA overtime
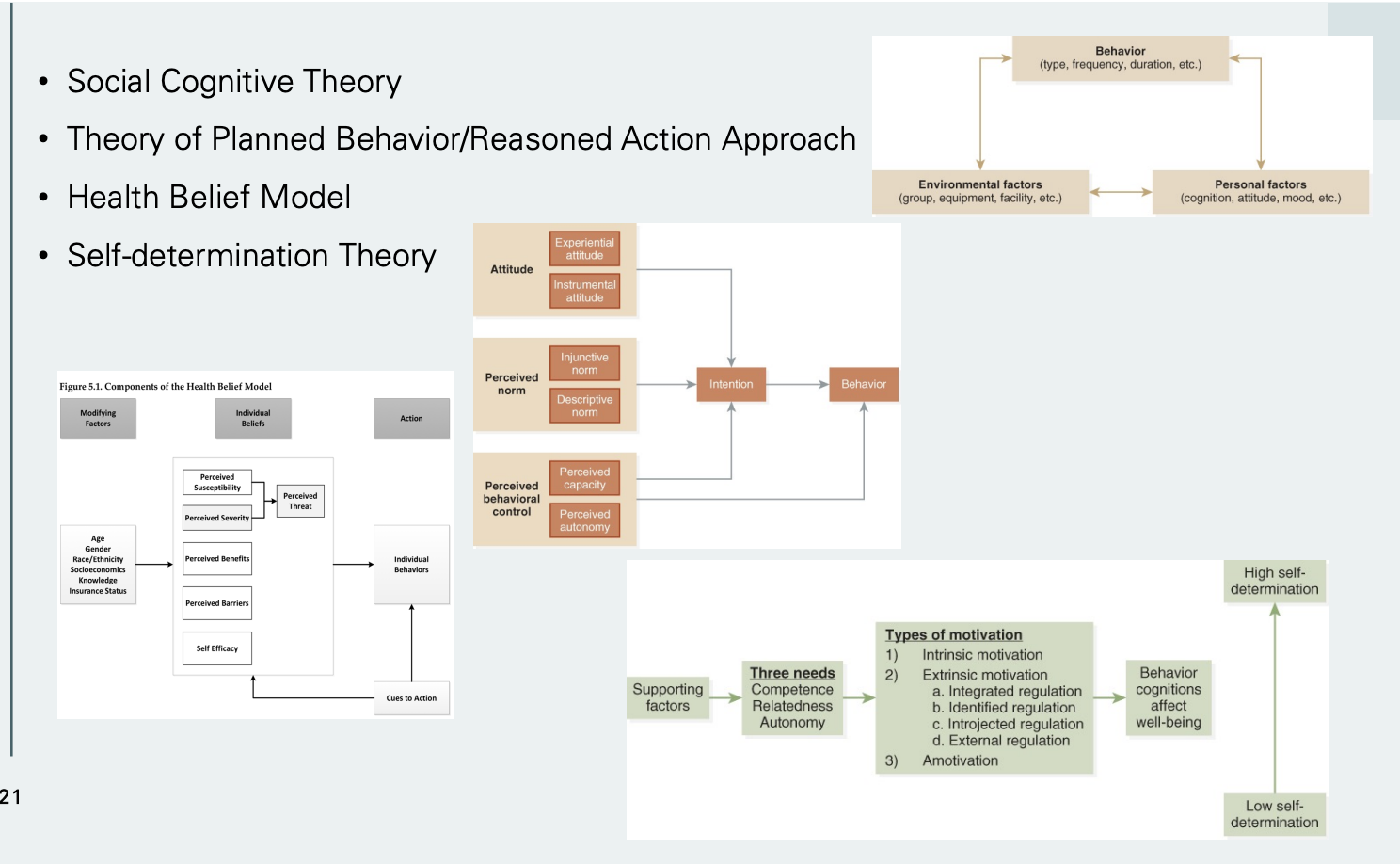
Theoretical Frameworks and Interventions (How could the theoretical frameworks be applied to better understand culture and health behaviors?)
*have similar constructs; try to understand culture, how break it down
-Social Cognitive Theory: self-efficacy, behaviors based on modeling
-Theory of Planned Behavior/Reasoned Action Approach: culture impacts attitude
-Health Belief Model: culture impacts perceived threats (perceived severity and susceptibility)
-Self-determination Theory: relatedness, motivation, intrinsic motivation
*+Dual-Process Theory: cognitive and enjoyment factors
Intervention Design
Integrate aspects of culture
-Surface dimensions: photos, language, dress, music, or images favored by group
-Structural dimensions: messages (*theory of reactance), materials, and delivery strategies (*tech level) that incorporate beliefs, values, and traditions of group (*open to latest treatment?)
Outcome Measurement
Lacks in research
-Need for validated instruments used across cultures (*quality of life, dietary intake differs in populations)
-Literacy level and linguistic variations (*ex: is a questionar about pain appropatiote)
Provider Factors
-Providers must be aware of ethnocentric tendencies (*dif treatments based on how identify race/ethnicity)
-Community health workers (*hesitation to work w/ providers so community health workers sent out so feel more comfortable; lot of interventions try to implement this so more responsive)
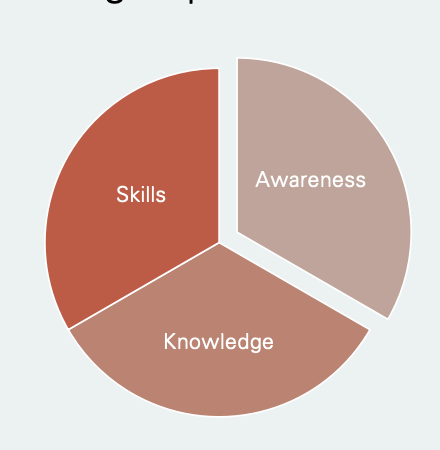
Cultural Competence: definition + 3 factors
-Capacity to function effectively as an individual or an organization within the context of the cultural beliefs, behaviors, and needs presented by a particular group or community
*provider factor; just as important as provider skills
3 Factors
-Awareness (*am I aware? do I know my values and beliefs?)
-Knowledge (*understanding others viewpoints/culture)
-Skill (*skill to change what care provide, culturally appropriate interaction)
*in-class Checklist activity: cultural competence is an issue, bc come from privilege background and not taught but learning always possible?, learned experience and awareness; “Cultural Competency Skills Training” address implicit bias and stereotypes