KIN 3339 - rehab concepts and special topics in athletic training exam 1 Questions with 100% correct answers + detailed rationales
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
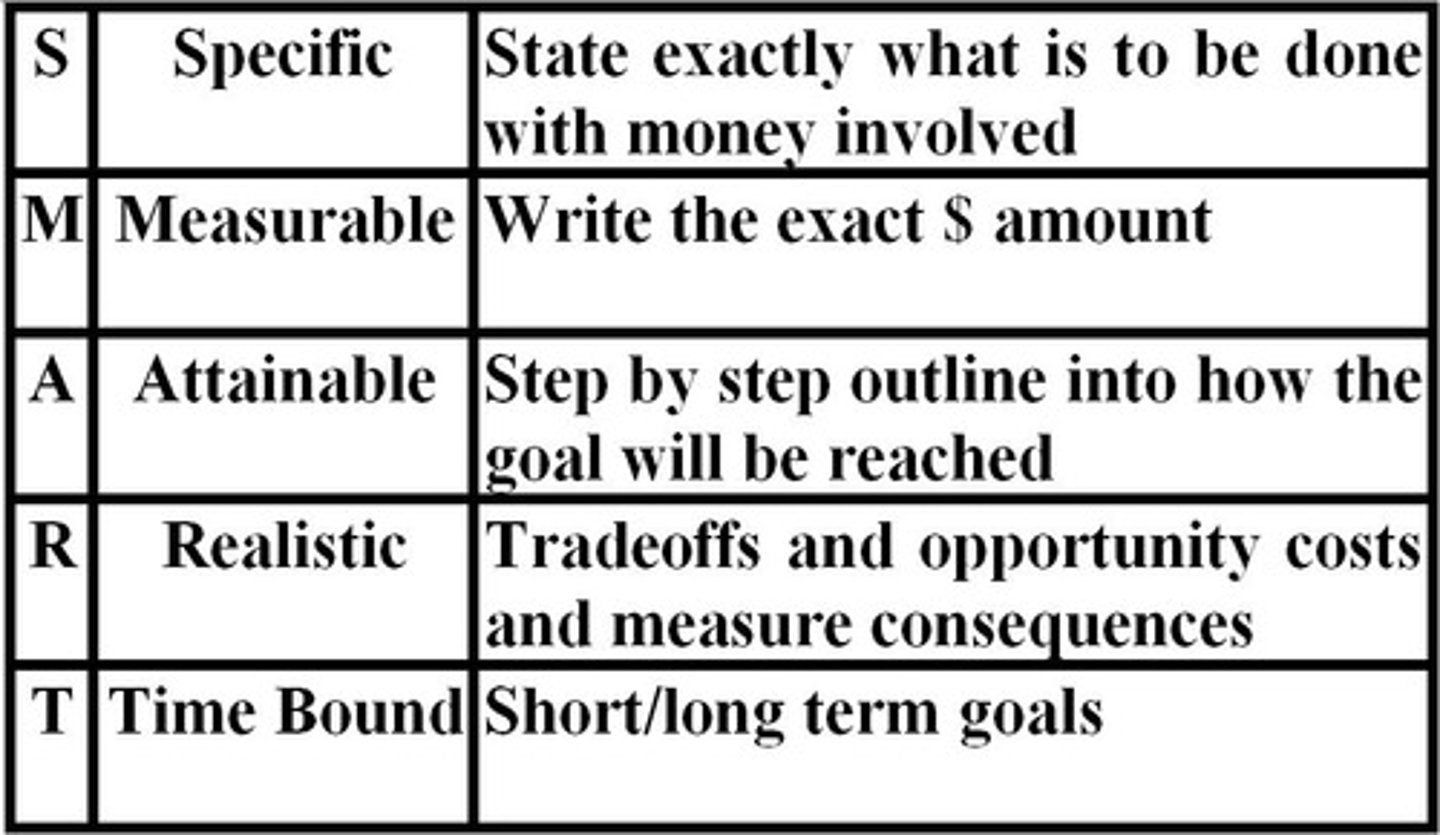
What are SMART goals?
specific, measurable, attainable (action), realistic, time bound
What is Rehab? What is the goal? What does Rehab entail?
- The process of treatment and education that helps disabled people to attain maximum function, a sense of well-being, and a personally satisfying level of independence.
- WHO Definition: A set of measures that assist individuals who experience, or are likely to experience, disability to achieve and maintain optimal functioning in interaction with their environments.
How should we as clinicians act when conducting a rehab? Why?
- Professionalism
- Abiding by ethical standards (e.g. NATA Code of Ethics)
- Abide by legal standards (e.g. state regulations)
- we are expected to be professional. That includes looking like a professional and acting like a professional. Dressing appropriately for the job as well as conducting ourselves in an appropriate manner.
- And being involved in professional organizations is also vital to being a professional. Stay up to date on continuing education and EBPs
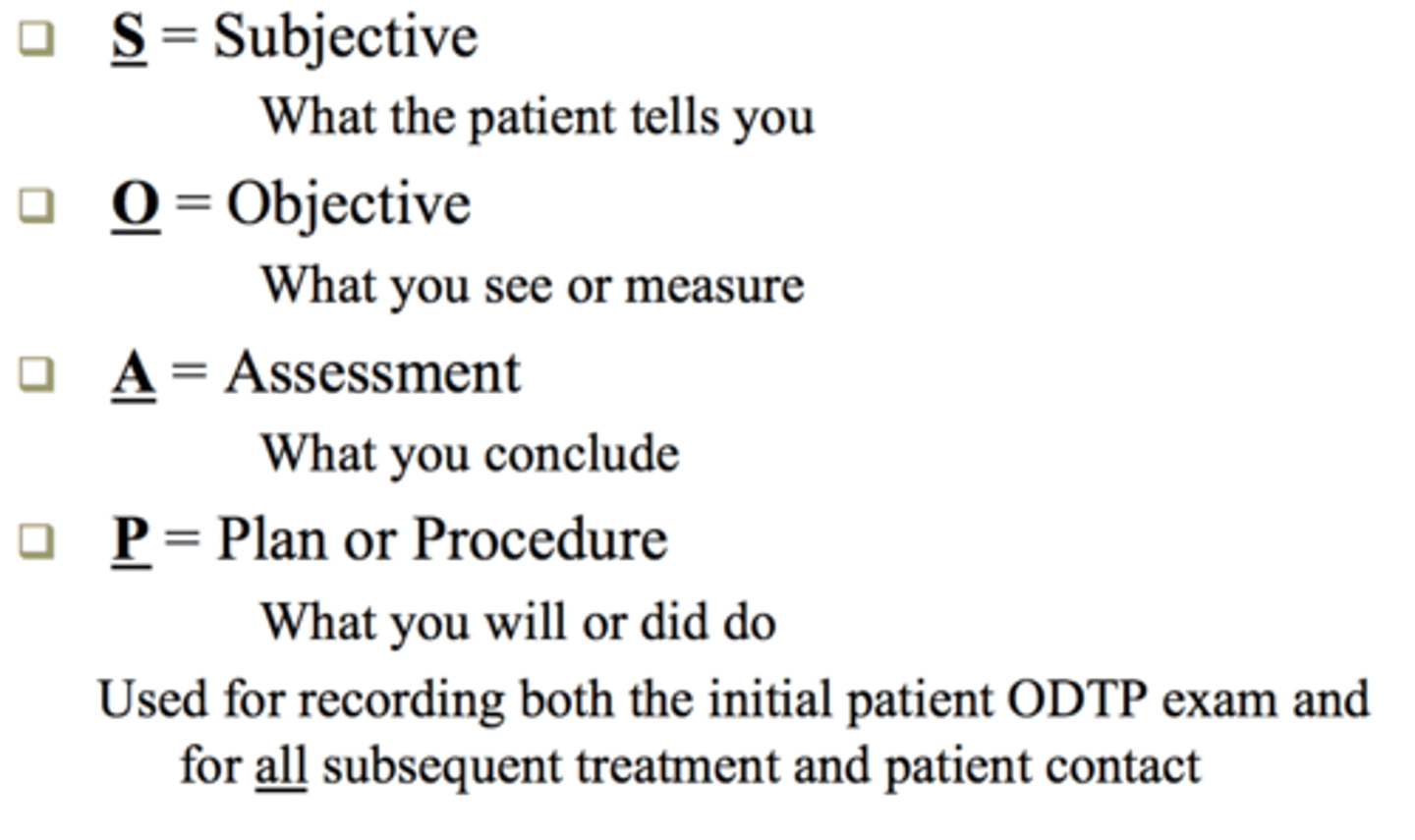
what is SOAP Notes?
format used to document an evaluation of a patient
S: subjective data
O : objective data
A : assessment
P : plan of action
Objective Component of the Evaluation
Data from objective:
•Finite measures that are readily reproducible regardless of individual collecting the information
•Provides baseline measures for reevaluations and rehab protocols
Clinical Purpose:
•Determine Diagnosis
•Create Asterisk Signs
⚬Measure patient's condition and progress
Rehabilitative Purpose:
•Identify impairments and functional limitations
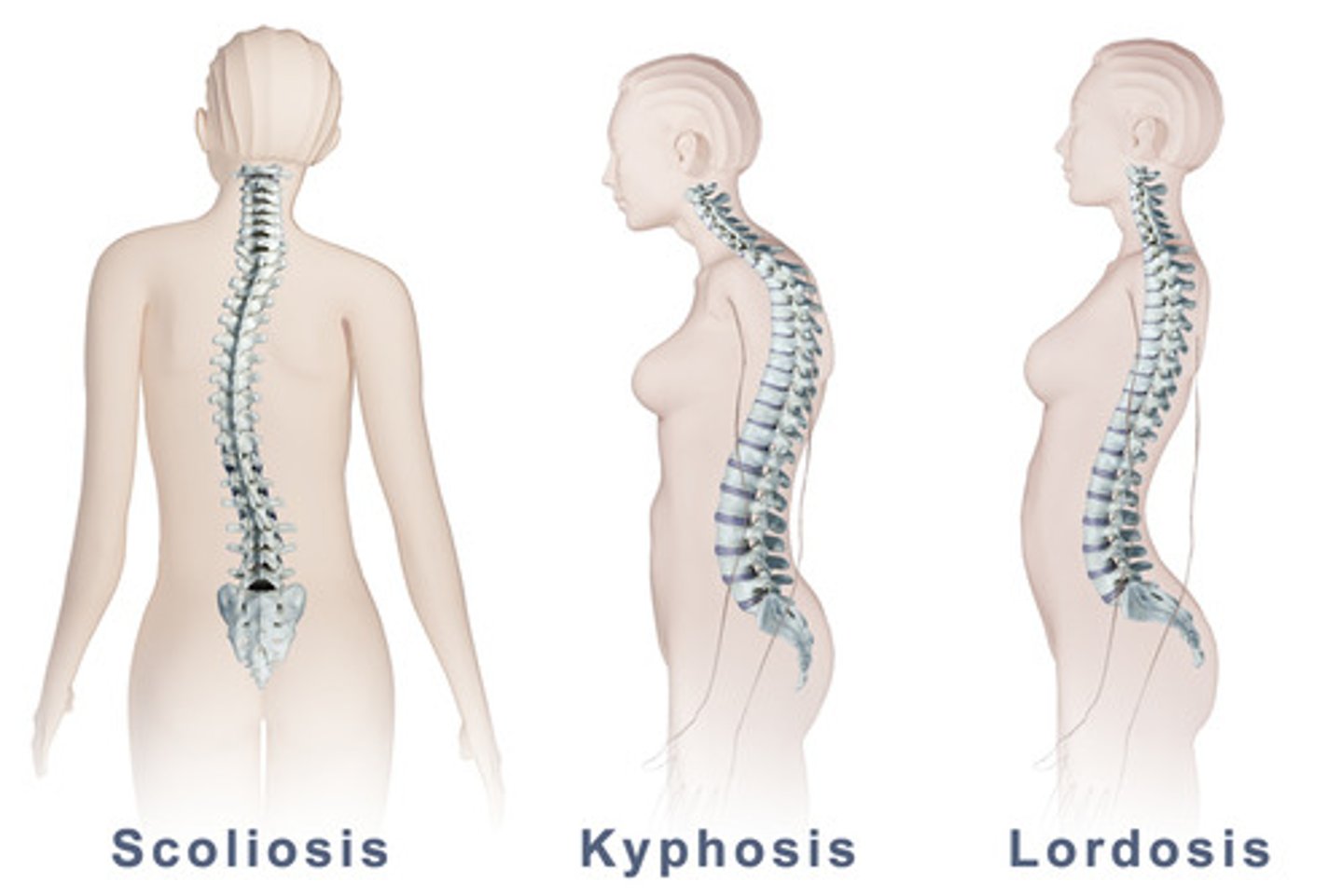
Posture abnormalities: the Spine (lumbar, thoracic, cervical)
LUMBAR
Lordosis
•Excessive is >40 degrees
•Anterior Pelvic Tilt
•Overactive hip flexors and low back extensors
•Weak abdominals, glutes, hamstrings
•Increased difficulty in diaphragm inhalation
THORACIC
Flat Back
•Hyperactivity in erector spinae and scapular protractors
•Weakness in scapular retractors and posterior rotator cuff
Kyphosis
•Excessive rounding of thoracic area
•Shortened pectoralis and intercostals
•Lengthened erector spinae, rhomboids, and trapezius
•Protracted scapulas
•Can lead to Thoracic Outlet Syndrome
Scoliosis
•Lateral or Rotational curve of the spine
•Cause muscle fatigue and increased ligament stress and impingement of the nerve roots
•May be corrected
CERVICAL
Forward Head Posture
•Upper Crossed Syndrome
•May increase
⚬Irritation to cervical disk
⚬Nerve root pressure
⚬Risk of impingement
•Can lead to
⚬Dowager’s Hump
⚬Temporomandibular joint disorders
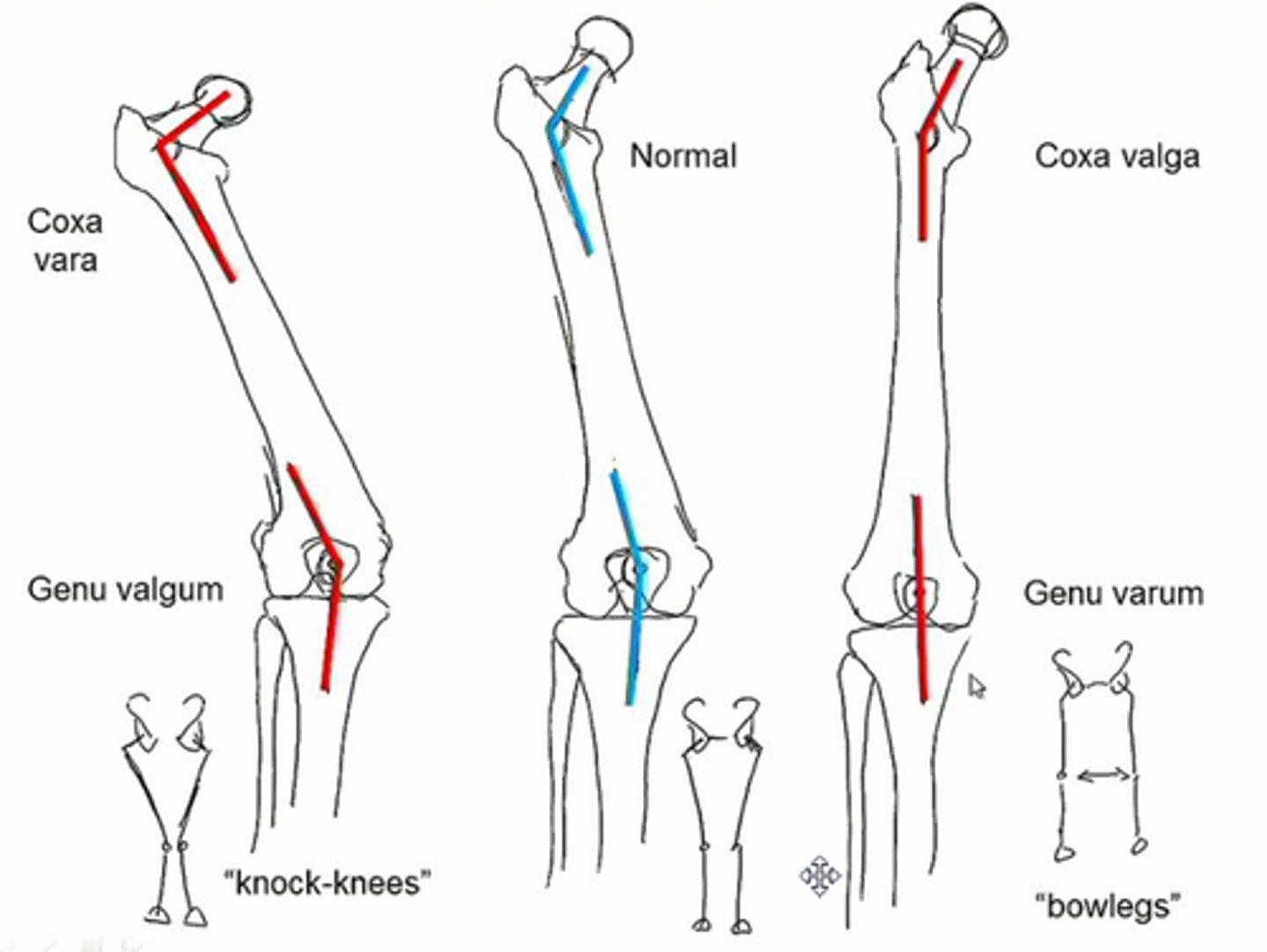
Posture abnormalities: the Hip
Coxa Valga
Higher risk of hip arthritis (170 degrees)
normal position 125 degrees
Coxa Vara
Higher risk for femoral neck fractures (100 degrees)
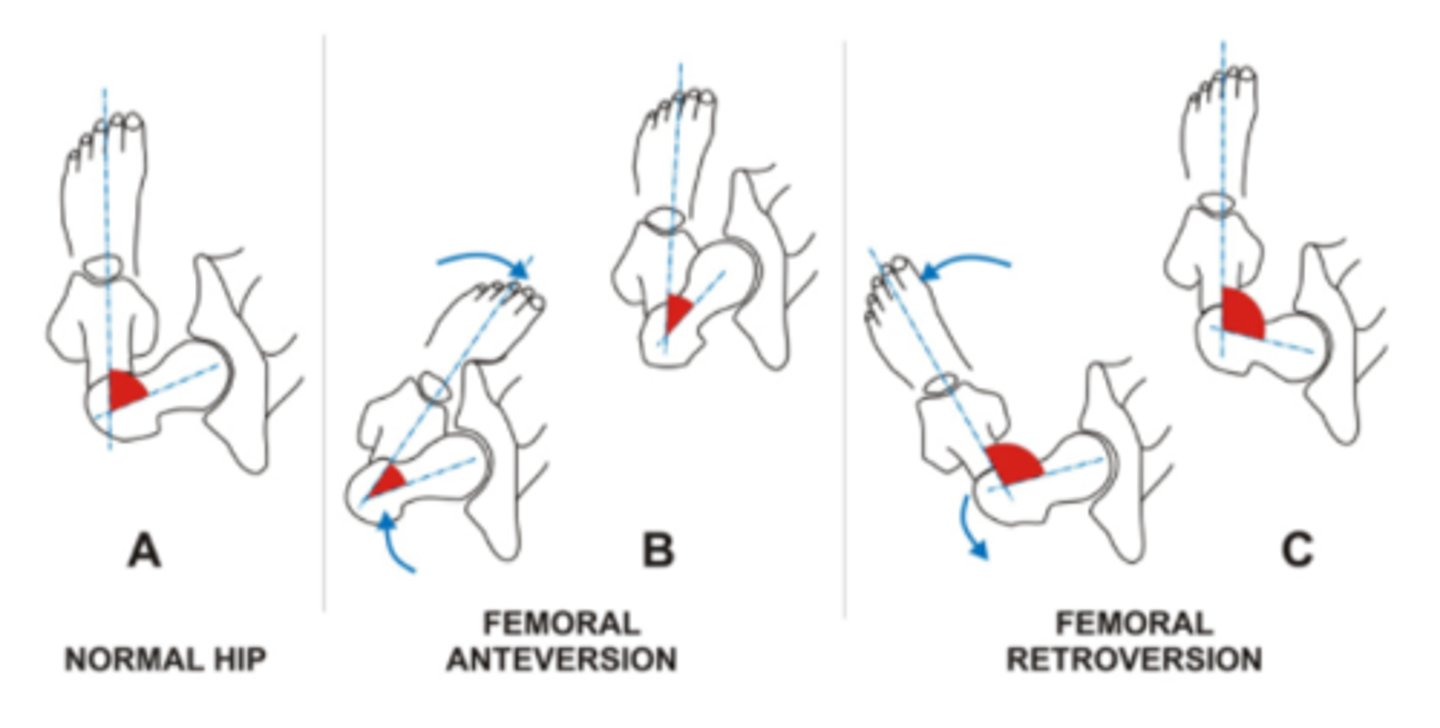
Abnormal Hip Rotation
Anteversion
Hip IR, decreases joint stability
Retroversion
Hip ER, increases joint stability
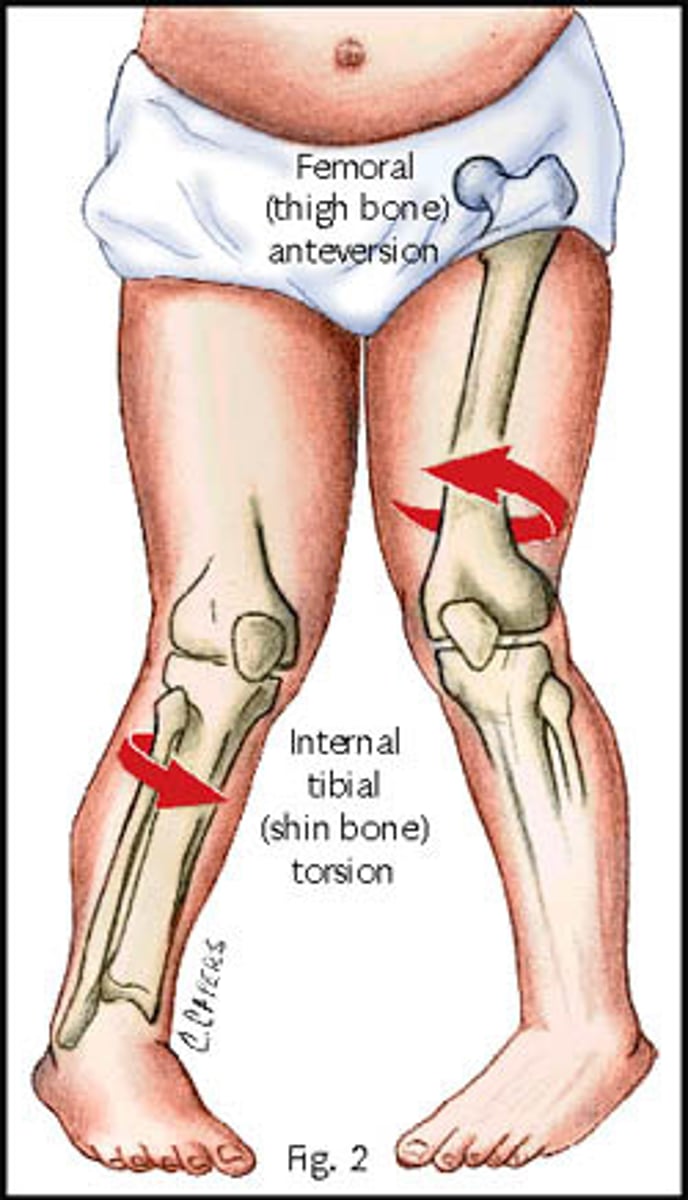
Posture abnormalities: the Feet
Tibial Torsion
•Leg looks rotated relative to thigh
•Usually lateral torsion
•Patient is supine with patella facing upwards
•Line bisects the medial and lateral malleoli
•The angle from that line to horizontal line is measured
•Angles greater than 20-25 degrees is positive sign
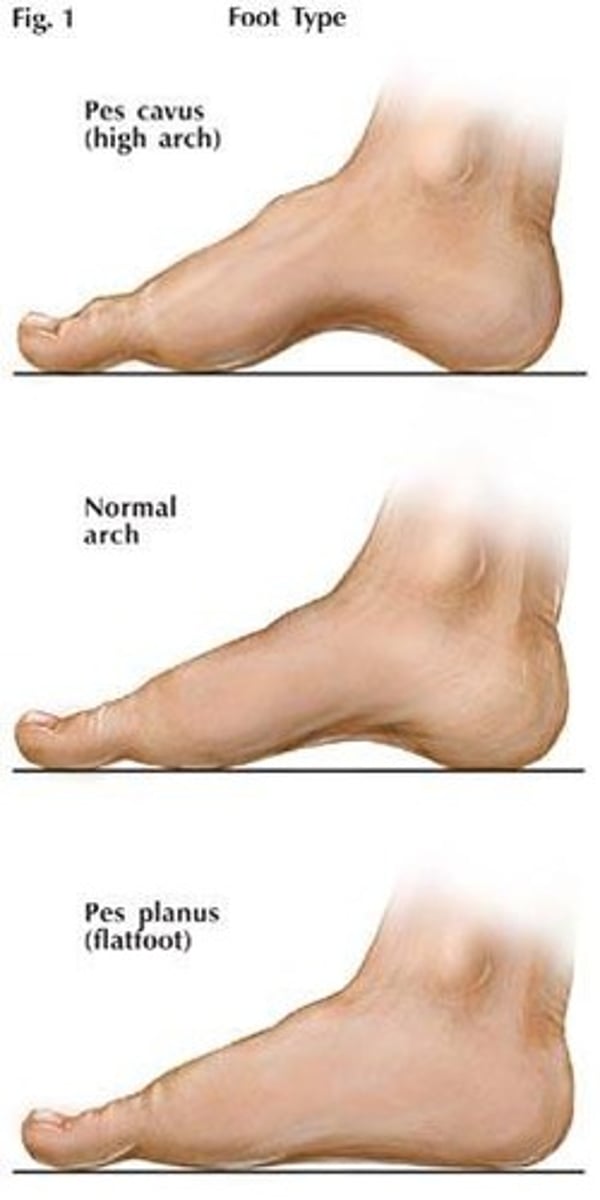
Abnormal Arch Alignment
Pes Planus (flat foot)
Foot Pronation & Calcaneal Eversion
Associated with genu valgum and Femoral anteversion
Pes planus is usually hypermobile, so we have more excessive rearfoot and forefoot motion during gait. Places excessive stresses on soft-tissue structures during power and agility activities.
Pes Cavus (high arch)
Foot Supination
Associated with hammertoes and Femoral retroversion
Pes Cavus produces less mobility of the rearfoot and forefoot. It's ability to absorb stresss is decreased, so the probability for stress fractures is increased
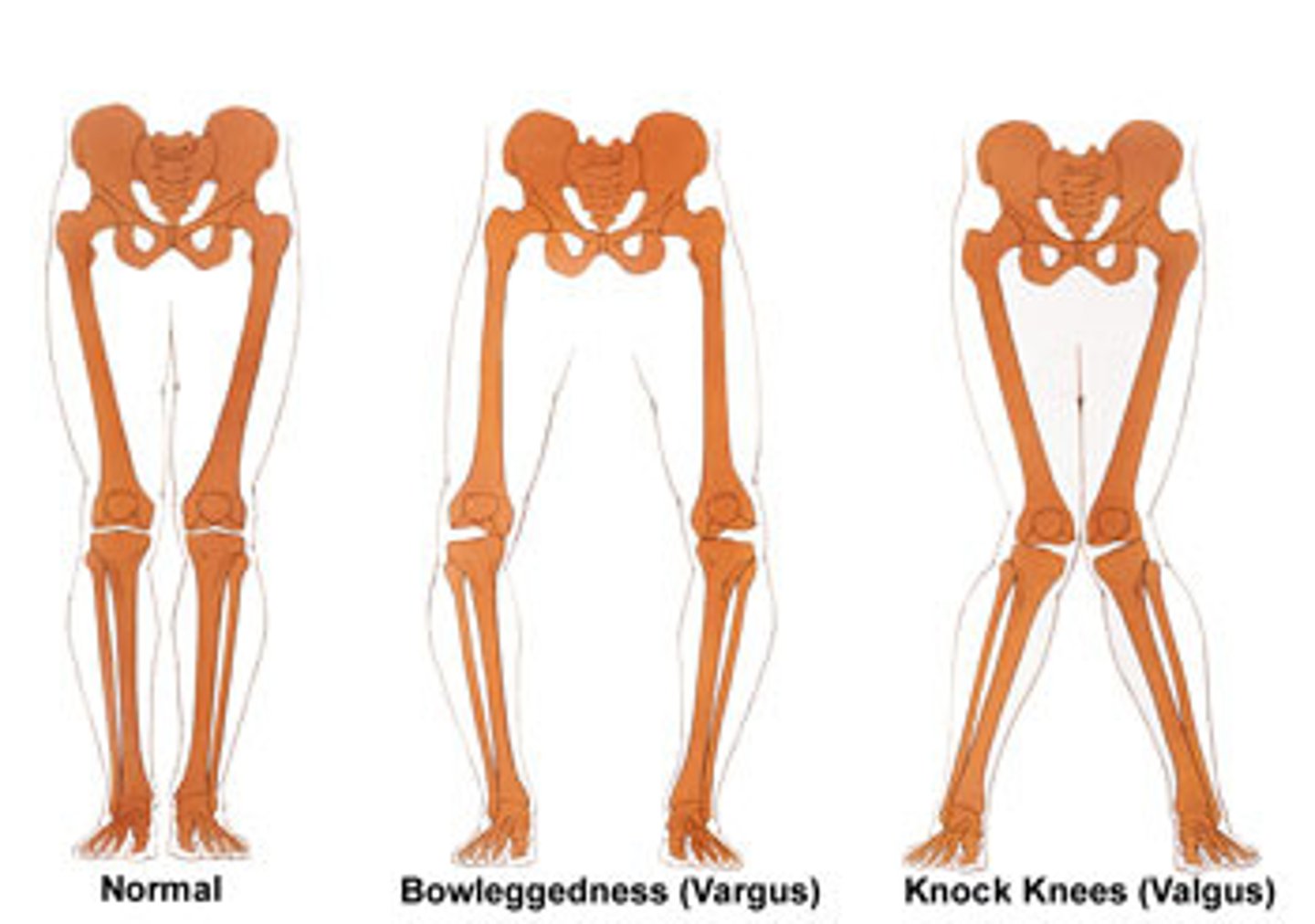
Posture abnormalities: the Knees
Genu Varus (bowleggedness)
Can be related to high arches
Genu Valgus (knock knees)
Can be related to excessive foot pronation
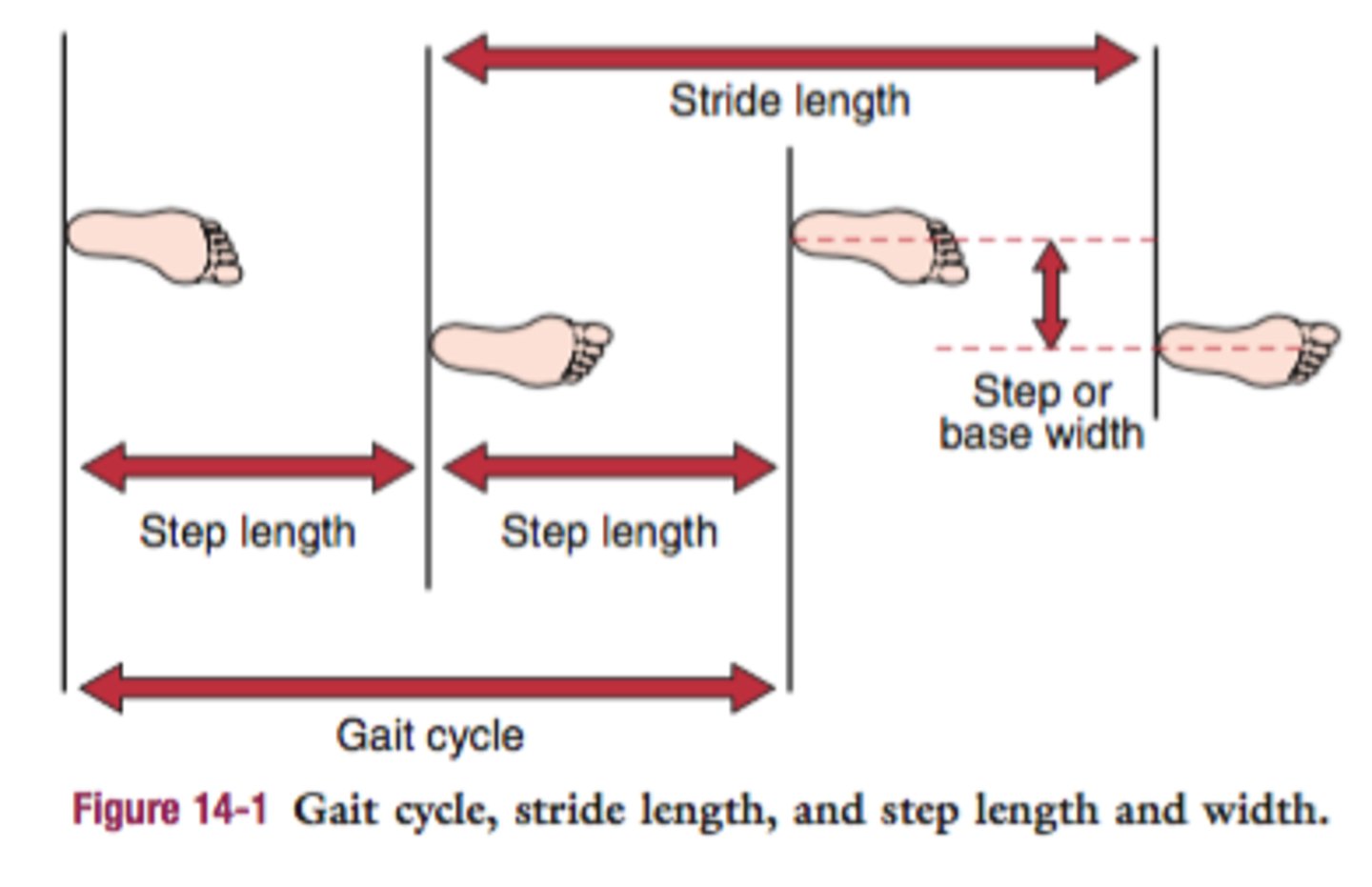
Step Length vs Step Width vs Stride Length
Stride Length
Distance from heel strike of one foot to heel strike of same foot in one cycle
Step Length
Distance from heel strike of one foot to heel strike of the other foot in one cycle
Stride Width
Distance between midline of one foot at midstance and the midline of the other foot at midstance
Purpose of Palpation and Special Test
palpation
•Detect tissue damage
•Identify areas of point tenderness
special tests
Confirm or Rule Out a Suspicion
Specific procedures applied to specific tissues in various ways
Described as Positive (+) or Negative (-)
Ex. O’Brien’s, Lachman’s, Talar Tilt
Active AROM
Active AROM
•Assess first
•Can they move it?
⚬Quantity/Quality
⚬Compensatory patterns?
Should be tested before PROM unless contraindicated
•Patient moves body through ROM
•Bilateral (Uninjured side first)
•Observe for Regional Interdependence
measurements
Subjective: Normal, WNL, or limited compared bilaterally
Objective: Goniometric measurement
What can cause abnormal AROM?
Pain
Muscle weakness
Spasm
Paralysis
Tight / shortened muscles
Joint injury
Limited neuromuscular control
Painful Arc- Represents compression, impingement or abrasion of the underlying tissues
passive PROM
Passive PROM
•Assessed second
•Can I move it?
⚬Quantity?
⚬What provokes pain?
•Clinician moves the patient through ROM
•Assessing the intra-articular barrier
•Only stressing the non-contractile structures since muscles are relaxed
•When the end of the available range is reached, pressure (overpressure) is applied in order to determine the end feel
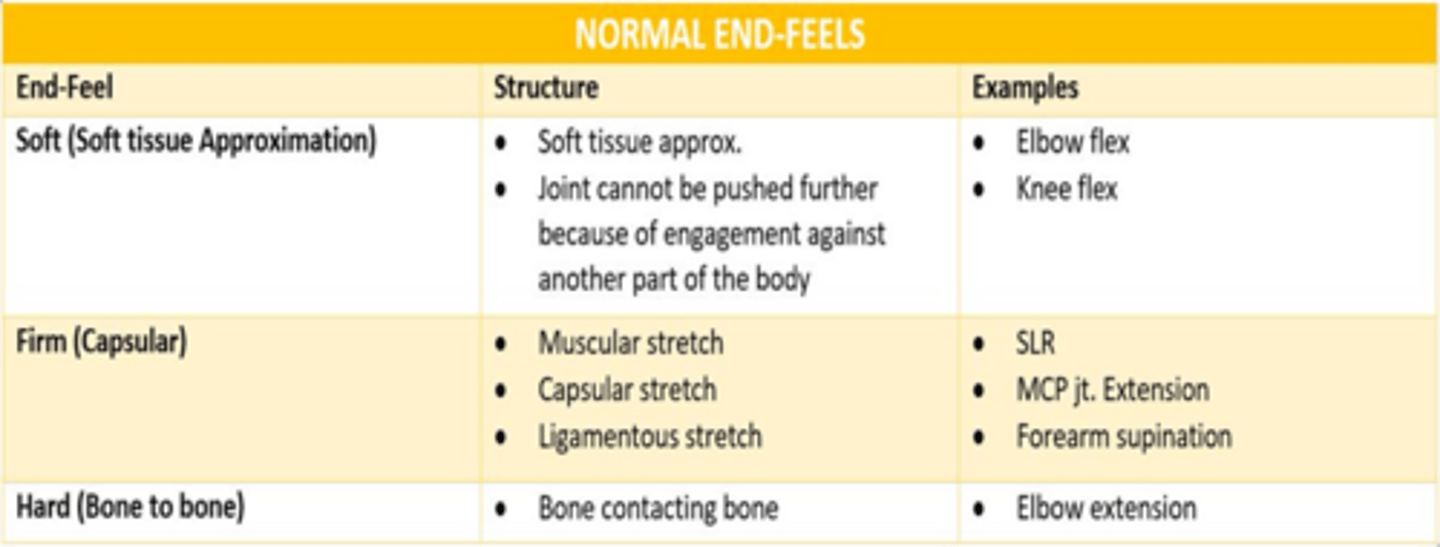
PROM End Feels (soft, firm, hard)
End Feel: soft; Before complete ROM, feels boggy
structure: Soft Tissue Approximation
EX: Soft Tissue edema, Synovitis
end feel: Firm; Before complete ROM
structure: 1.Muscular Stretch 2.Capsular Stretch 3.Ligamentous Stretch
EX: Hypertone, soft tissue shortening
end feel: Hard; Bony grating/Bony Block
structure: Bone to Bone
EX: Arthritis, loose bodies
Empty: No end feel, pain prevents full ROM
EX: inflammation
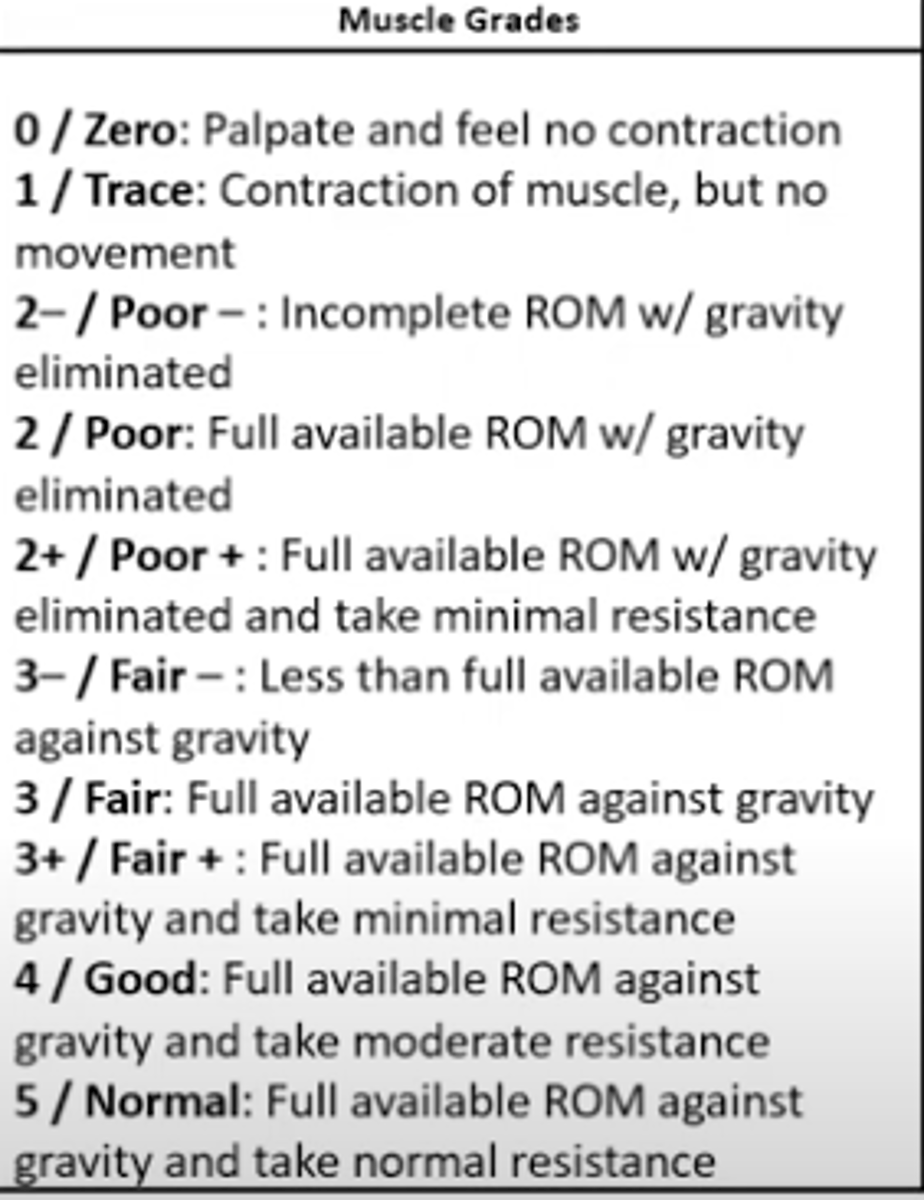
Manual Muscle Testing Purpose and Grading
Important to compare bilaterally!
•Is there break away weakness?
•Is there gross weakness?
What is normal for this patient?
•Consider age and ability and contributing pathology
Procedure
•Position against gravity
•Ask PT to perform AROM
•Then position at midrange and hold position
Evidence Based Practice
•Results from the history and functional assessment can reduce the number of tests to be performed
⚬Example: Symptom is gradual onset
■No need to perform acute fracture special tests
•Crucial to providing optimal care
•Clinician’s skills and experience
•Reliable research investigations
•Patient’s needs, goals, and priorities
•Efficient: Eliminate time wasted performing unnecessary special tests
•Accurate: Eliminate false positives
Phases of Healing
Phases of Healing
Hemostasis Phase:
Begins immediately, Lasts up to 3 days
•Shortest healing phase
•Stops blood flow originating the damaged vessels from flowing into the injury site
•3 steps
⚬Vasospasm
⚬Primary Hemostasis
■Platelet Plug
⚬Secondary Hemostasis
■Fibrin Plug
Inflammation:
•Begins once clot is formed
•Lasts 2-10 days
•Necessary “evil” (Needs control)
•Process of Debridement
⚬Chemicals released to:
■Destroy damaged microorganisms
■Remove the debris
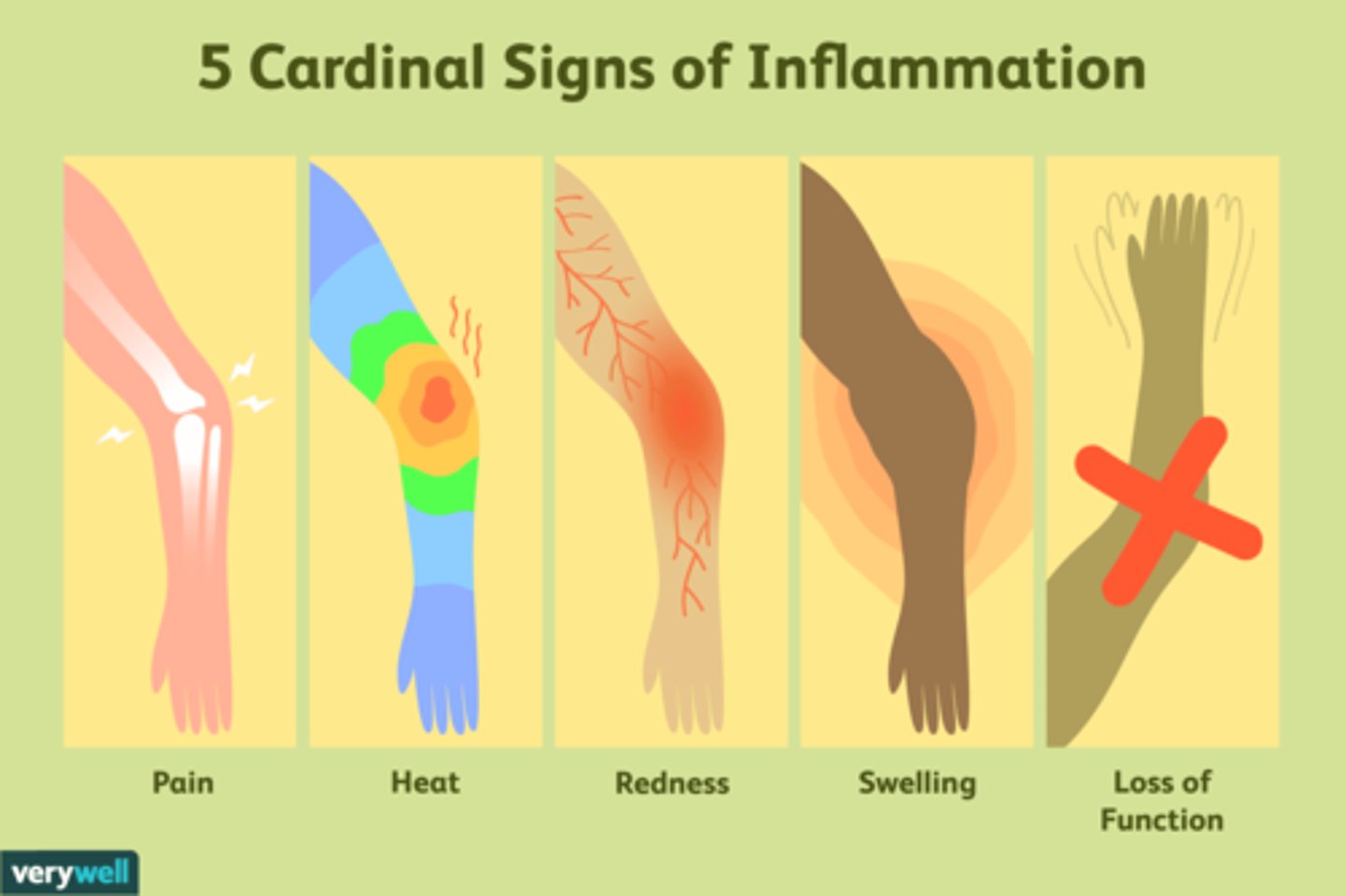
5 Cardinal/Clinical Signs
Begins immediately, Lasts 2-10 days
Proliferation:
•Duration is 2-4 weeks***
•Overlaps with Inflammation and Remodeling Phase
•Angiogenesis and granulation are formed
•Type III collagen is laid down almost haphazardly
•Increase in fibroblasts; reduced Leukocytes
•Clinical Signs
⚬Redness from increased number of capillaries
⚬Swelling from increased capillaries and water volume
⚬Pain from pressure-sensitive nerve endings
Day 3 - Week 6
Remodeling:
•Can last 6-18 months
•Wound matures and converts to scar tissue
•Type 1 Fibers replace Type III Fibers
•Reduction in fibroblasts, macrophages, and capillaries
•Scar tissue gains tensile strength through completion of healing process
•Clinical signs
⚬Reduced redness
⚬Reduced edema
Reduced pain
Day 7 - over a year
Cardinal Signs of Inflammation
Heat, redness/discoloration, swelling, pain, and loss of function
Tensile Strength
•Original stress that tissue could withstand decreases up to 50% during inflammation phase
•During the first 5 days, the strength of the injured site is weak, because it's given from the injured area
•At day 5, tensile strength increases and continues to increases as collagen arrives and properly aligns
•Tensile strength may take up to a year to attempt to reach maximum, but will still remain below pre-injury strengths
Factors impacting healing
oxygen:
Increased need for oxygen
Poor vascular status may develop into chronic or unhealed
Surgical Repair Techniques
Injured Size
Infection
Nutrition
Muscle Spasm
drugs:
Beneficial or harmful
Absorption and Interactions
NSAIDS
•Detrimental for fractures and chronic inflammation
•Inhibits prostaglandin production, which then reduces local nociceptors and vascular permeability
•Can cause GI issues
age
swelling
3 R's of Rehab
Relieve Symptoms
- Initial efforts aimed towards relieving the signs and symptoms that occur
- Modalities & Therapeutic Exercise
Restore Deficiencies
- Begins once injury advances from inflammation stage to proliferation stage
- Modalities & Therapeutic Exercise
Return to Function
- Occurs in later proliferation and re-modeling phase to regain pre-injury function
- Therapeutic Exercise
what does ATC IS IT stand for? NEED TO KNOW
Avoid Aggravation: Do no harm using knowledge of phase of healing
Timing: phase of healing
Compliance: Empower the patient, so they buy into the program
Individualization: Physiological, biochemical,
biomechanical, non-physical
Specific Sequence: Refer to the Rehab Pyramid
Intensity: Progress from: easy to hard, closed to open chain,
low to high impact
Total Patient: Cardiovascular & un-injured pair considerations
Phases of Rehab
Inactive phase (inflammation phase)
Clinician Goals/Aim:
Relieve Pain, Edema, Muscle Spasm
Protect injured tissue
Prevent deconditioning
Therapeutic Actions
Refrain from exercise
Use of modalities
Manual Therapy
Assist with controlling the Inflammation
active phase (proliferation phase)
Clinician Goals/Aim:
Restore Range of Motion and Mobility
Therapeutic Actions
Modalities as needed
Stretches
Manual Therapy
Advance from PROM -> AROM
Initiate Balance and Coordination
Eventually add resisted exercises
resistive phase (Proliferation and Remodeling
Phases)
Clinician Goals/Aim:
Restore muscle strength and endurance, proprioception, and agility
Therapeutic Actions
Strength exercises
(Progress from straight plane to diagonal plane)
Continue flexibility routine
Proprioception and agility
advanced phase (Remodeling Phase)
Clinician Goals/Aim:
Restore to optimal performance
Resume all pre-injury participation
Maintain flexibility and strength
Therapeutic Actions
Plymometrics
Functional Exercise Progression to Performance Exercises
Immobilization
- There are soft tissue changes. It can cause the Type I Collagen Fibers to produce a dense meshwork, which limits tissue mobility
Pros
•Decrease pain
•Stabilize joint
Cons
•Decrease in activity can cause loss of:
⚬Muscular Strength and Endurance
⚬Oxygen capacity and decreased blood flow
⚬Coordination
•Decrease in Range of Motion and Mobility
⚬Leads to increase of collagen binds and scar tissue
⚬Increased risk of atrophy
Fat infiltrates the muscle
Components of Rehab
Progress from one step to the next throughout the rehab
Remember to evaluate at each step to adapt the rehab program to determine patient's goals and outcomes
Therapeutic Goals of Phases of Rehab and Healing
Therapeutic Modalities:
•Tools used in conjunction with rehabilitation
•Assists in reaching particular goal
•Considerations of Modalities
⚬What’s the treatment site? How will modality affect the tissue and/or structure?
⚬What are the indications/contraindications?
■Is it appropriate? Will it do harm?
⚬What is the protocol to administer treatment?
Therapeutic Interventions to Improve Flexibility & ROM:
Manual Therapy: Alter connective tissue to improve ROM, reduce spasm and pain, increase blood flow
Stretching: Increase flexibility through various techniques to promote increased stretch tolerance
Facial Mobilizations:
Manipulation of mature collagen fibers to stretch and lengthen the fascia
Sports Psych Techniques
•Arousal Regulation
•Goal Setting
•Imagery
•Pre-Performance Routines
•Self-Talk
Barriers to Recovery
fear of re-injury, low self-efficacy, negative self-talk, lack of social support, poor coping mechanisms, anxiety about returning to play, depression, denial of injury severity, perfectionism, and negative expectations about recovery
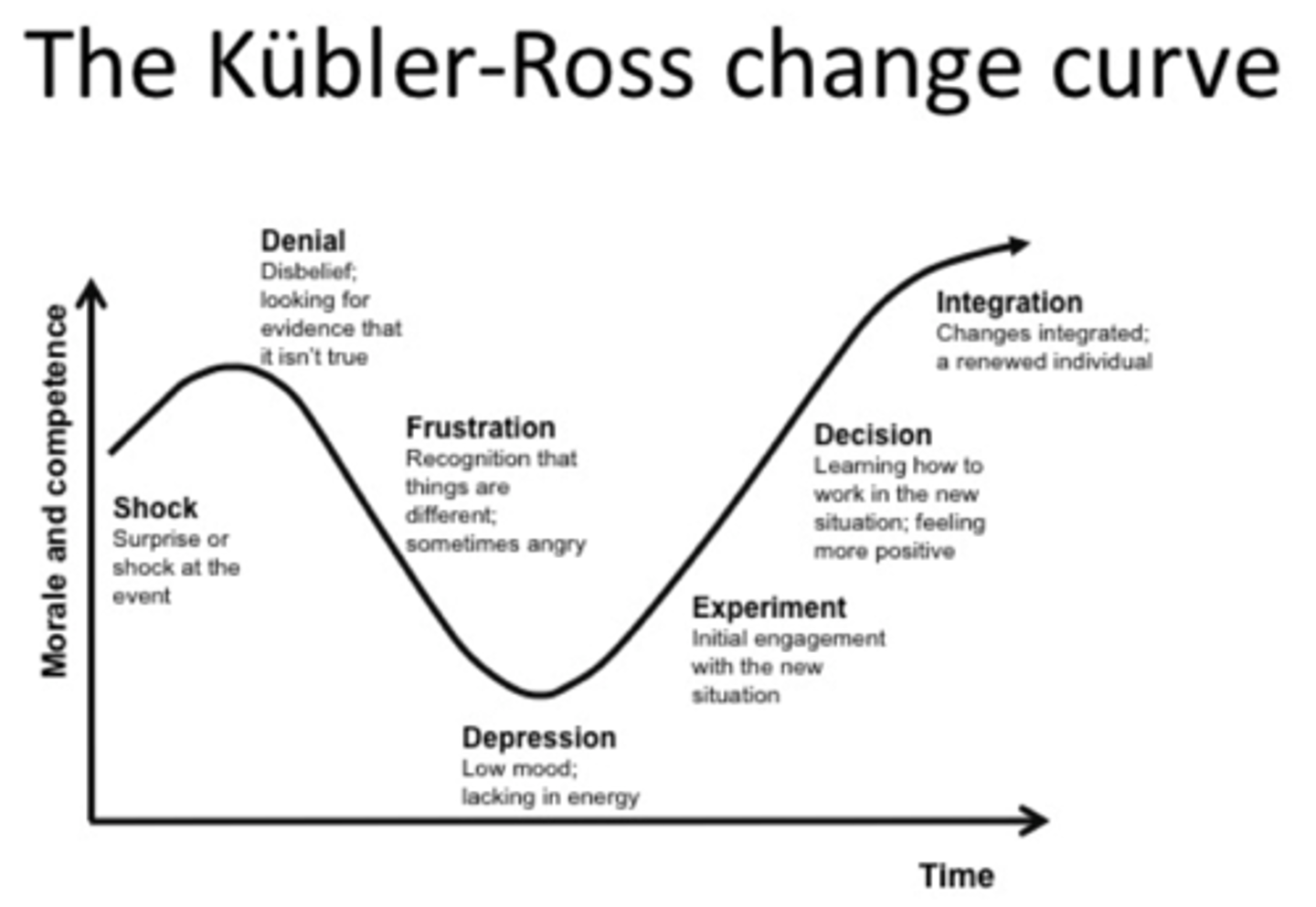
Kubler Ross cycle AKA Grief Cycle
denial > anger > bargaining > depression > acceptance
Psychology Coping Skills
Distraction:
Pros:
•Gives your heart & mind a break
•Great for short term relief
Cons:
•Can’t do it for very long or in every situation
•Doesn’t resolve the issue
EX: Talk to friend, read, puzzle, doom scroll, watch tv, play a game, clean, learn something new, arts & crafts
Grounding:
Pros:
•Helps slow/stop numb feeling
•Reduces physical anxiety
•Increases relaxation
Cons:
•Sometimes brain needs to stay busy or distracted
EX: Use the 5 senses.
Take a breath, smell the air, feel the ground, what sensations are you experiencing?
Emotional Release:
Pros:
•Great for anger & fear
•Releases the pressure of overwhelming emotions
Cons:
•Can’t always do depending on where you are or who you’re with
EX: Scream into pillow, cold shower, punch a pillow, throw a ball around
Psychology Coping Skills pt.2
Self-Care:
Pros:
•Great for feelings of guilt or shame
•Recharges batteries
•Much deserved
Cons:
•Sometimes can feel hard to do or feels superficial
EX: Do something you enjoy, make your favorite meal, massage, clean space, write in journal, take a nap
Golden Rule:
Pros:
•Reminds us everyone has value & purpose can be found in everyday things
Cons:
•Don’t get stuck trying to save everyone and forget about yourself or have kindness used against you.
EX: Help someone else, smile, pray or meditate, volunteer, random acts of kindness, play with your pet, join a club
Thought Challenge:
Pros:
•Can help shift thinking to positive habits
•Focusing on logic can help reduce extreme emotions
Cons:
•May be more difficult if more emotional- may need another strategy first
EX: Write negative thoughts and list reasons why they may not be true. If a friend had this though, what would you tell them? For every negative, write two positives
Mindfulness Acceptance Commitment Theory (KNOW THE 6 CORE PRINCIPLES!)
Accept what is out of your control and commit to an action which improves and enriches your life
Teaches skills to effectively deal with painful thoughts and feelings to lessen the impact and influence over you
Clarifies your values and priorities, and uses that knowledge to guide, inspire, and motivate you
6 core principles:
Cognitive Diffusion, Acceptance, Contact with Present Moment, Observing Self, Values, Committed Action
Motivation intrinsic vs. extrinsic
Intrinsic:
Self-esteem and self-confidence
I want to play/I love the game
Who am I if I don’t?
Extrinsic:
Playing for your parents not yourself
Coaches/media/fame
Scholarships/NIL/$$$
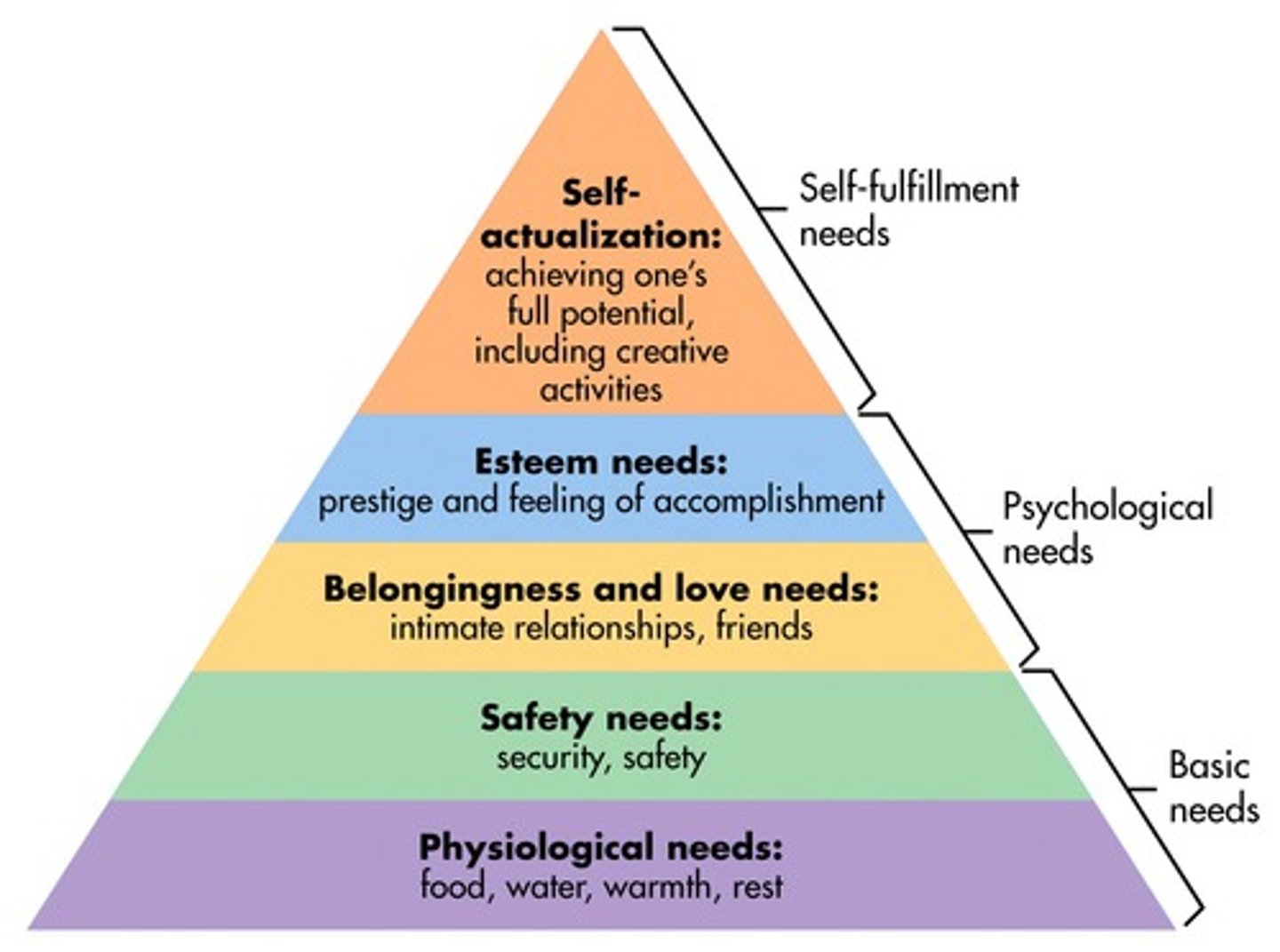
Maslow's Hierarchy of Needs
psychological needs (food, water, warmth, rest)
safety needs (security, safety)
belongingness and love needs (intimate relationships, friends) esteem needs (prestige and feeling accomplishment)
self actualization needs (achieving ones full potential, including creative activities)