Di Imaging Exam 2
1/167
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
168 Terms
What is enchondral ossification?
cartilage is the precursor on which new bone is laid down (majority of skeleton)
What is intramembranous ossification?
direct laying down of bone into the primitive tissue, without intermediate cartilage (most of skull, clavicle and fibula)
What is calcification?
laying down of calcium-based salts and crystals within cells and tissues
The primary ossification centers first appear where in spine at 9 weeks in utero followed by _
cervicothoracic junction
upper cervical then thoracolumbar vertebrae
lumbar neural arches is the last to appear at 14 weeks
C3-L5 vertebrae typically have _ primary ossification centers
3→ one in centrum (vertebral body) and one for each half of the neural arch
C1 has how many primary ossification centers in total?
3→ one for anterior arch and one for each side of posterior arch
C2 has how many primary ossification centers?
5→ same as typical vertebrae but has two extra for the dens
C3-L5 vertebrae have _ secondary ossification centers that fuse by 25-30 years
5→ one at tip of spinous, one at the tip of each TVP, two as ring epiphyses at upper and lower surfaces of bodies
T/F C1 has NO secondary ossification centers NBCE
True
C2 has a secondary ossification center where?
tip of the dens
Posterior arch agenesis can be _
complete or partial→ if cartilage template is present then partial
If you have a posterior arch agenesis, you may see an enlarged C2 spinous which is called _
C2 megaspinous sign
What are some additional things to look for with posterior arch agenesis?
C2 megaspinous sign
hypertrophy of the anterior tubercle
How do you determine trauma vs congenital?
congenital will have well corticated (white) borders
What is a non-union of the C1 posterior arch?
failure of fusion
aka SBO
aka Midline cleft
aka Dysraphism
cartilage of neural/posterior arches is present but the synchondrosis of the right and left posterior arch segments is faulty
margins are smooth, rounded, and corticated
What is non-union anterior arch of C1?
failure of fusion of the anterior arch RARE
What is chiari malformation?
herniation of cerebellar tonsils is over 3 mm
What is the significance of chiari malformation?
Wrong way scoliosis aka left thoracic scoliosis
Bony anomalies→ klippel-feil
Syrinx/syringomyelia
What is assimilation of atlas/occipitalization?
one of MC carniocervical junction anomaly
complete or partial
What is clinical significance of assimilation of atlas?
instability/basilar impression
What are some clinical signficance of assimilation of atlas?
Non-segmentation (blocked) of C2 and C3 is Common
Basilar invagination
Cleft palate
Cervical ribs
Urinary tract anomalies
Cranio-cervical instability
What are the classic features of congenital non-segmentation (block vertebra)?
Rudimentary disc
Smooth concave anterior vertebral body margins (Wasp waist)
Combined vertebrae are taller
Large foramen seen on lateral view
What is clinical significance of non-segmentation vertebra?
Non-segmentation is more accurate than fusion
MC at C5/C6, C2/C3, and L4/L5
How can you tell the difference between congenital and acquired/post-surgical block vertebra?
Congenital→ rudimentary disc, smooth concave anterior vertebral body margins, combined vertebra may be of greater height and large foramen on lateral view
Acquired→ Obliterated disc, flat/squared anterior vertebral body, no change in height, no change in foramen size
Today, most surgical fusion is performed with hardware alone or hardware with autograft, or allograft, and and not with _ alone
autograft
What is the surgery where you get a surgical fusion performed called?
COF→ anterior cervical discectomy fusion
What are multiple segmentation anomalies of cervical spine called?
Klippel-feil
What are some features of klippel-feil syndrome?
short webbed neck
low posterior hairline
reduced cervical range of motion
What are some associated conditions with klippel-feil syndrome?
Renal anomalies→ 50%
Hearing loss, possibly deafness→ 30%
Arnold chiari and or syringomyelina
Sprengel deformity→ non descended scapula (3:1 female to male)
What feature is associated with sprengel’s deformity?
omovertebra bar
What is a posterior ponticle?
arcuate foramen (ponticulus posticus) is a normal variant of atlas
calcification of the posterior atlanto-occipital membrane
can be complete or incomplete
What is the clinical significance of posterior ponticle?
possible vertebral artery occlusion with trauma related instability

What is this?
Epitransverse process→ bony extension originating from transverse process of C1 upward to the skull bone
What is the difference between epitransverse process and paracondylar process?
Epitransverse process→ variant of atlas where bony outgrowth arises from TVP and articulates with occiput
Paracondylar process→ variant of occipital bone where enlarged bony process extends caudally from paracondylar region towards TVP of atlas (can be unilateral or bilateral)
What imaging could be used for epitransverse processes to see?
CT, CBCT
What is the clinical significance of epitransverse processes?
May create lateral head tilt
may affect adjusting technique
effectively results in fusion of C1 to occiput
What is os terminale? (Ossiculum terminale aka bergmann ossicle)
failure of union of the secondary center of ossification found at the tip of the dens
appears at age 3-6
Not considered anomaly unless persists after age of 12
not associated with instability
Os terminale is almost always in what shape?
“V” shaped
look at cortical borders to rule out fracture
Os odontoideum is associated with what condition?
down syndrome
People with os odontoideum are at risk for _
VBAI
Os terminale is oftenly confused for _
Type 1 Dens fracture
always stable
What type of dens fracture is the most common?
Type 2 dens fracture→ heal bad
confused for os odontoideum
Type 3 fracture has the best _
prognosis
Most os odontoidium is a result of _
old un-united odontoid fracture
If a patient is stable and asymptomatic what is the treatment?
leave alone/monitor
If a patient is unstable and symptomatic, what is the treatment?
surgical referral
Castelvi classifcation is used for _
transitional segment classification
If L5 doesn’t fully segment from sacrum and looks like S1 it is called _
sacralization
If S1 doesn’t full segment rom L5 and looks like L6 it is called _
Lumbarization
What is a typical feature of lumbosacral transitional segments?
hyperplasia of transverse process→ L3 MC
occasional accessory joint degeneration→ Bertolotti’s syndrome
Spatulated TVP
Rudimentary disc space
What is bertolotti syndrome?
lumbo-sacral transitional segment with accessory bone degeneration
low back pain
Transitional segment and iliolumbar ligament calcification=
DISH unilaterally or bilaterally
What is facet tropism?
asymmetrical orientation of facet joints
common in sub axial cervical spine
coronal and sagittal facets at one level
8 degree difference side to side
highest at c2-c3 whereas lowest at c6-c7 level
common at L5-S1
What is the clinical significance of facet tropism?
Facet tropism could be predisposing factor to disc degeneration, facet degeneration, and degenerative spondylolisthesis
What is transverse process accessory articulation?
TVP grow towards eachother→ forming pseudoarticulation
What is persistent apophysis?
look for well corticated borders
DDX→ old clay shoveler fx
Apophyseal injuries occur most commonly during _
sporting activities→ MC at growth plates
What is a risser sign?
how to measure skeletal maturity
Where is most apophyseal injuries occur?
occur in pelvic region due to numerous apophyses and strength or attaching muscles
other location are tibial tuberosity, inferior patellar pole, calcaneal tuberosity, 5th metatarsal base, acromion, proximal humerus, medial epicondyle and distal radius
What is the best imaging for persistent apophysis?
X-ray
MRI→ BEST MODALITY
shows physeal widening without displacement
increased signal of the physis on fluid-sensitive sequences
bone marrow edema of apophysis
soft tissue edema
What are oppenheimer ossicles?
accessory ossicles of the facet joints
found in 4% lumbar spines
single, unilateral ossicle of the inferior articular processes
What are image findings with oppenheimer ossicles?
Best seen on sagittal CT
usually seen at L2/L3
Smooth corticated
Synovial space of adjacent facet may communicate with the cleft between the ossicle and articular process
Associated with neural arch malformations
What is an absent pedicle?
can be congenital agenesis or acquired destruction
Congenital→ RARE condition
Destructive→ BAD
Tumor→ Primary bone tumor, soft tissue tumor, secondary tumor (lytic metastasis MC)
Winking owl sign (unilateral absence of spine pedicle)
What are some items that may help differentiate congenital absence from other etiologies?
May have stress hypertrophy (enlargment, cortical thickening and sclerosis) or contralateral pedicle
May have accessory transverse process sign, small inferiorly directed transverse process with small joint like space seperates it from pedicle or vertebral body
May have spinous deviation sign→ deviation of spinous towards contralateral side
If you see a winking owl sign that is congenital you should assume it is _
lytic metastasis
What is Hahn vascular cleft/groove/canal?
vertebral vascular foramina
intraosseous nutrient arteries: foramen usually seen anterolaterally
basivertebral veins which can be seen on posterior surface of vertebral body in midline
What is clinical significance of developmental dysplasia of the hip (DDH)?
congenital dislocation of the hip
occurs from ligamentous laxity and abnormal position in utero
What are the risk factors for DDH?
Female gender
firstborn baby
family history
breech presentation
oligohydramnios
metatarsus adductus
spina bifida
What orthopedic exam is performed on infants for developmental dysplasia of the hip?
Ortolani and Barlow
What are some image findings of DDH?
left hip is more frequently affected
ULTRASOUND is the modality of choice
Alpha angle needs to be greater than 60 degrees (normal)
ultrasound is less than 50 degrees is DDH
Bony coverage is greater than 50% coverage of the femoral epiphysis by the acetabular roof is normal
What are some other lines that diagnosis DDH?
Hilgenreiner line
Perkin line
Shenton line
acetabular angle
extrusion index
center-edge angle
What is hilgenreiner’s line?
horizontal line connecting inferior aspect of tri-radiate cartilages bilaterally
What is perkin’s line?
drawn vertically through lateral aspect of acetabular roof perpendicular to Hilgenreiner’s line
ossified femoral head should be inferomedial quadrant
What is the acetabular angle?
plain film measurement used when evaluating DDH
measured between Hilgenreiner’s line and line parallel to acetabular roof
What is the measurement for acetabular angle?
Under 1= Less than 22 degrees
Adults= over 45 degrees (33-38 degrees)
What is Putti’s triad? TQ
Absent or small proximal femoral epiphysis
Superolateral/lateral displacement of femur
Increased acetabular angle
What is the clinical significance of DDH?
acetabular protrusion→ intrapelvic displacement of acetabulum
Primary→ developmental or post-surgical DDH
Secondary→ bone softening diseases like paget disease, psoriatic arthopathy, RA, ankylosing spondylitis
What are some image findings of DDH?
Center-edge angle (Wiberg)→ greater than 40 degrees (Kohler’s line)
Projection of the femoral head medial to the iliioischial line (acetabular protrusion)
What are femoral herniation pits?
“schmorl’s node in femoral neck”
Synovial herniation pits have no clinicial significance (LEAVE IT ALONE LESION)
seen in 5-33% of the cam form of femoral acetabular impingement FAI
“Pitt’s pit”
What is Femoral acetabular impingement? FAI
presents with hip pain secondary to mechanical impingement from abnormal hip morphology
What are the three types of FAI?
Pincer morphology→ overcoverage of the femoral head
Cam morphology→ bump formation at the femoral neck and asphericity
Both forms of morpholigcal changes can co-occur in a mixed type
What is accelerated with FAI?
Labral and cartilage injury→ leads to OA
What views are recommended for FAI?
frog-leg lateral
What are the possible features on imaging of FAI?
Cam or pincer morphology
Pistol grip deformity (CAM)
Acetabular overcoverage (PINCER)
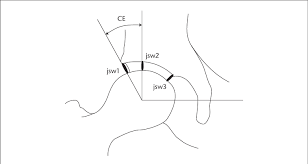
what is this angle?
wiberg angle→ should be 25-40 degrees
if excessed 40→ Pincer type FAI
What does the alpha angle measure with FAI?
extent to which the femoral head deviates from spherical
What are the measurements for an alpha angle in hip?
Normal→ less than 50 degrees
CAM type FAI→ greater than 50 degrees
What is a ischiopubic synchondrosis?
little bump on the ischiopubic region
DDx→ fracture
What is paraglenoid sulcus?
little archs at the ASIS seen in pelvic view
DDX→ sacroilitis
What are the types of soft tissue calcification?
Dystrophic→ tissue trauma, prior infection, inflammation MC
Metabolic/metastatic→ widespread soft tissue calcification secondary to metabolic and endocrinological diseases
Physiological→ normal, within cartilaginous tissue
What is the significance of a stylohyoideus ossificaiton?
Eagle syndrome→ neck pain, neurovascular compromise
CBCT can help measure elongation adn approximation to C1
What is the differential diagnosis for costal cartilage calcification?
lung cancer
What is a falx cerebri calcification?
calcification of dura
right down middle of head (separates R and L hemispheres)
What is petroclinoid ligament calcification?
calcification of the dura
runs horizontal above eyes
What is pineal gland calcification?
les than 1.0 cm is good
50% of population has it
rare
in less than 6 years suspect pinealoma
should not exceed 10 mm
Where is thyroid cartilage calcifications seen?
C6-C7 area
vertical lines over the TVP in the AP cervical view
What is phleboliths?
calcified venous thrombi
perirectal veins (not midline)
If you see phleboliths in other areas, what does it indicate?
hemangioma/AV fistula/ malformations
What is carpal coalition?
carpal and tarsal fusion are misnomers so called (coalition)
connection between two bones without indicating the etiology
MC involved bones are hamate and triquetrum although many combinations are reported
What are the associations with multiple carpal coalitions?
ellis-van creveld syndrome
Holt oram syndrome
Arthrogryposis
Turner syndrome
symphalangism