Ch 14 intrapartum fetal surveillance
1/64
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
65 Terms
fetal strip features to describe
uterine contraction patterns
baseline fetal heart rate (FHR)
FHR variability
presence of accelerations
presence & type of decelerations
external fetal monitoring
fetal monitor
ultrasound
toco transducer
all connected!
traces FHR/contraction pattern
toco transducer
monitors contractions
hard shell w/ soft button
firm abd presses w/ squeezing
placed at top of fundus, where contractions are strongest
palpate!
ultrasound monitor
measures FHT/FHR
hard plastic
place on abd w/ gel
place where fetal spine felt & palpated toward fetal head
specifically neck-shoulder connection
ie: baby head down? where monitor goes!
move w/ baby repositioning
internal fetal monitoring
mom has amniotic membrane ruptured
pt at least 1 ½ cm dilated
indicates labor progression & how fetus is tolerating
2 devices
fetal scalp electrode
intrauterine pressure catheter
fetal scalp electrode/clip
aka FSE
monitors FHR
used when fetal positioning/high maternal weight make external monitoring difficult
tones NEED to be tracked
be cautious of eyes w/ face presenting babies
placement of fetal scalp electrode
vaginal exam + sliding electrode in
feel for hard spot on fetal head
insert metal coil tip!
twist into tissue
connect to machine & monitor
mind what you are feeling
can be placed in dangerous spots
ie fontanelle
intrauterine pressure catheter
aka IUPC
used w/ high maternal weight
monitors contractions
+ strength! may indicate pictocin need
soft, flexible
placed similarly to scalp electrode
w/ vaginal exam
intrauterine pressure catheter placement
like fetal scalp electrode
w/ vaginal exam
placed btwn uterine wall & fetal back
mostly an MD thing
can accidentally be placed into edge of placenta → increased bleeding & placental issues
FSE complications
can be placed in eye
can cause insertion site infection!
rare, but can happen
antibiotic ointment usually put on opening to prevent it
often when mom has infection too
outweigh pros & cons!
IUPC complications
placenta previa/separation
bleeedingggg
contraction characteristics
frequency
duration
intensity
contraction frequency
how often?
measured start → start of 2 contractions
normal contraction frequency
5 or less in 10 min over 30 min
more? tachysystole!
contraction duration
how long?
measured in seconds
start → end of one contraction
big box on fetal strip
~60 seconds
small box on fetal strip
~10 seconds
whole fetal strip
~7 minutes
contraction intensity
how strong?
mild, moderate, strong
measured in montevideo units (MVU)
from internally!
mild contraction intensity
like nose
moderate contraction intensity
like chin
strong contraction intensity
like forehead
external contraction intensity monitoring
palpate during the contraction!
toco does not pick up strength
don’t depend on wave - not indicative of strength
super thin? bigger wave
vice versa w/ larger pts
normal uterine activity
abt 12 min strip
5 contractions
normal!
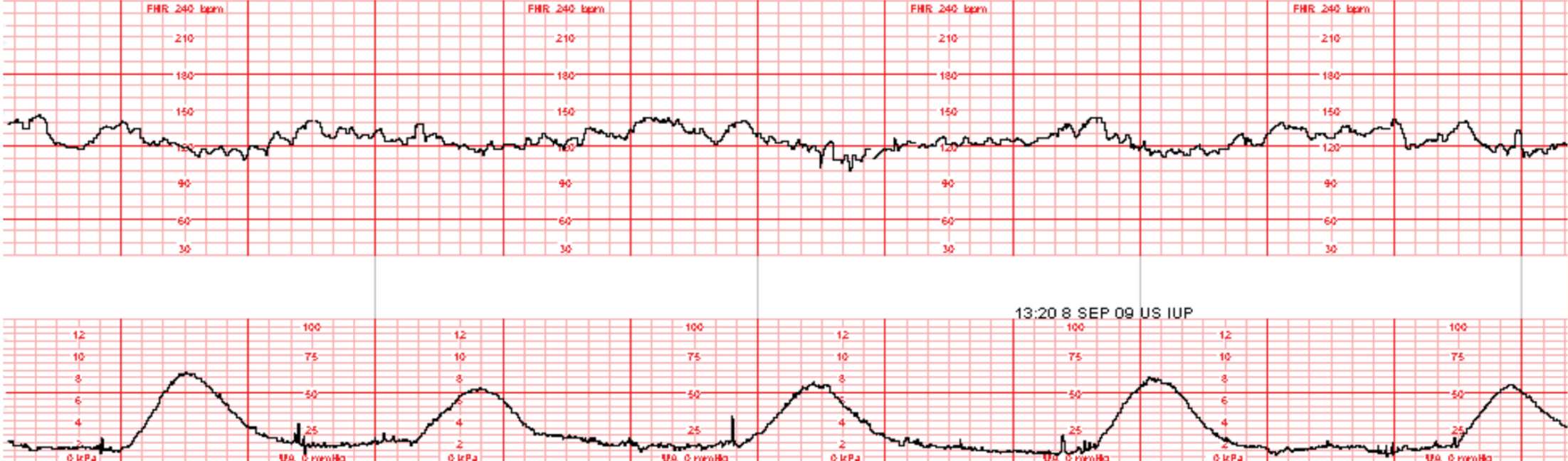
tachysystole
more than 5 contractions in 10 min over abt 30 min
regardless of FHR decelerations
oxygenation issue!
uterus supposed to relax & replenish O2 to fetus stores → baby continuously squeezed instead
late decels
no meds being given? give something!
7 contractions in 10 min
PIC HERE
pictocin & tachysystole
decrease the dose!
FHR characteristics
baseline
variability
accells & decels
FHR baseline
where the HR stays!
look @ tracing - where is the line mostly?
taken as an average
FHR BPM normal
110-160
FHR variability
periodic changes/fluctuations in baseline rate
we want this!
irregular in amplitude & frequency
measured beat-to-beat
4 types
FHR variability estimation
highest point
lowest point
diff btwn them!
how much does the line flucturate above & below baseline?
FHR variability types
absent
minimal
moderate
marked
absent variability
straight line
bad.
practically asystole
amplitude range undetectable
PIC HERE
minimal variability
changes of <5 bpm
<5 changes in 1min period
subtract high point from low somewhere in the duration!
moderate variability
what we really want!
changes of 6-25bpm
marked variability
very high # of changes
excited periods!
okay for short time frames
pt causes of FHR bradycardia
sympatholytic mecs (methyldopa)
beta blockers (labetalol [normodyne], propranolol)
sjogren’s antibodies
hypoglycemia
hypothermia
viral infection (cytomegalovirus)
fetal causes of FHR bradycardia
cardiac conduction abnormalities
heart block
fetal HF (hydrops)
structural cardiac defects
heterotaxia
hypothyroidism
interrupted fetal oxygenation pathway (umbilical cord prolapse)
pt causes of FHR tachycardia
beta-sympathomimetic drugs (terbutaline, epinephrine)
parasympatholytic drugs
fever
hyperthyroidism
infection (chorioamnionitis, appendicitis)
cocaine
fetal causes of FHR tachycardia
acute blood loss
fetal anemia
heart failure
hyperthyroidism
hypoxia/hypoxemia
increased metabolic rate
infection & fetal sepsis
tachyarrhythmias
preterm FHR
at upper end of normal
closer to 160
fetal tachycardia
baseline FHR >160
fetal bradycardia
baseline FHR <110
acceleration
any FHR baseline increase that then returns to normal
PIC HERE
variable deceleration
like a carrot!
rapid
drops then rises again suddenly
how u tell its diff from early/late decels
bc of cord compression
have mom change positions
not always associated w/ contractions - don’t pay attention to them
last ~30 sec
decreased by at least 15bpm for at least 15 sec
late deceleration
contractions start → baby squeezed
if goes to O2 reserve and there is none? decel!
hypoxic event
FHR returns to normal after squeeze
smooth, gradual decrease
caused by placental insuffiency
contraction THEN decel - at lowest after contraction has peaked
late to the partayyy
early deceleration
mirror contractions!
gradual, temporary decrease in HR
bc of head compression - esp closer to delivery
occurs during contractions
nothing we can do - benign response
labor & early decels
nothing we can do - benign response
part of labor! intervention would stop it
happen esp as baby drops when further along
typically 8-9cm
VEAL CHOP MINE
acronym to remember acceleration/deceleration details
read as type → cause → intervention
VEAL
V - variable deceleration
E - early deceleration
A - acceleration
L - later deceleration
CHOP
C - cord compression
H - head compression
O - Okay..! things are good!
P - Placental insuffiency
MINE
M - movement (mom repositioning)
I - identify labor progress
N - no special intervention needed
E - emergency action required!
variable decel intervention
change maternal position
decreases the compression
early decel intervention
none needed
continue to monitor pt & fetal strip
acceleration intervetion
no intervention needed
late deceleration intervention
change position
increase IV fluids
help blood flow - easier going thru
start/increase O2
hyperoxygenate mom → O2 to baby
stop pitocin if being used
pitocin & late decels
stop!
gives baby more time to oxygenate
decreases contractions
FHR categories
assign to every strip
3!
category one
category two
category three
FHR category 1
what we want!
normal & strong predictor of normal fetal acid-base status
no distress
FHR category 1 characteristics
FHR baseline 110-160 bpm
moderate variability
accelerations present/absent
variable/late decelerations absent
early decelerations present/absent
<5 contractions in 10 min period
FHR category 2
indeterminate & fetal acid-base balance uncertain
not 1 or 3? 2!
tracings not categorized as I or III
can’t rlly tell baby’s state
FHR category 3
horrible
abnormal & predictive of fetal acid-base status
fetal distress noted
notify MD → prepare for c-section!
get baby outta there!!!
FHR category 3 characteristics
absent variability
AND
recurrent late decels
recurrent variable decels
bradycardia
sinusoidal pattern
any or all!
sinusoidal pattern
from cardiac anomaly
wooooosh smooth wave
very rare!
can be pseudo-sinusoidal → benign
sinusoidal pattern causes
severe fetal distress
hypoxia
fetal distress