GI week 2
1/401
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
402 Terms
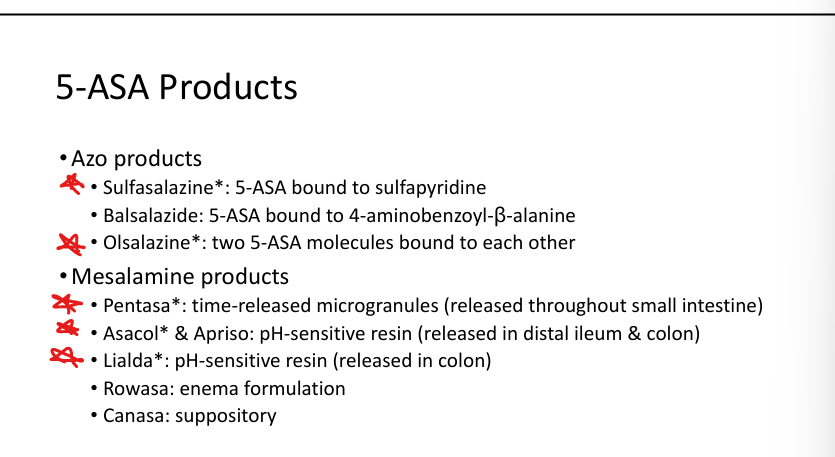
5-ASA MOA
Topical anti-inflammatory effect on diseased GI mucosa
5-ASA uses
Ulcerative colitis, mild Crohn’s (colonic)
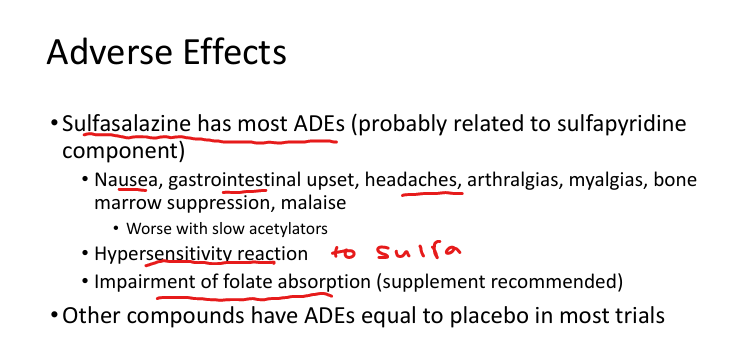
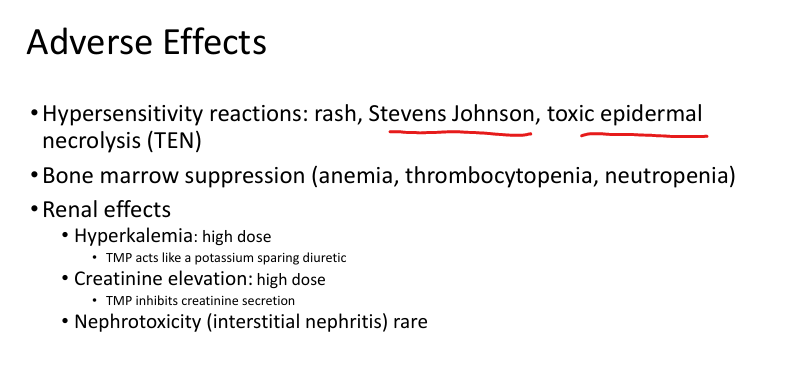
5-ASA adverse effects
Sulfasalazine: GI upset, headache, arthralgia, bone marrow suppression, folate deficiency
Sulfasalazine unique fact
Requires folate supplementation
Pentasa release site
TIme released microngranules throughout small intestine(Only Asa that doesnt do the colon>pentagon is important like small intestine)
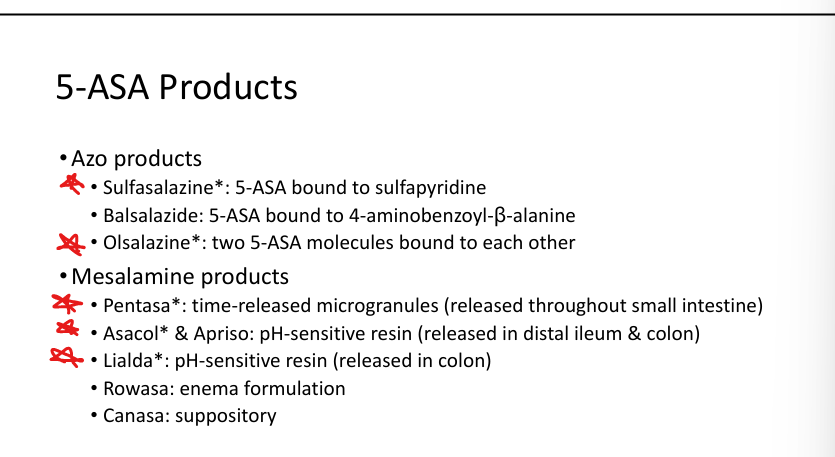
Asacol/Apriso release site
ASA; pH sensitive released into Distal ileum & colon
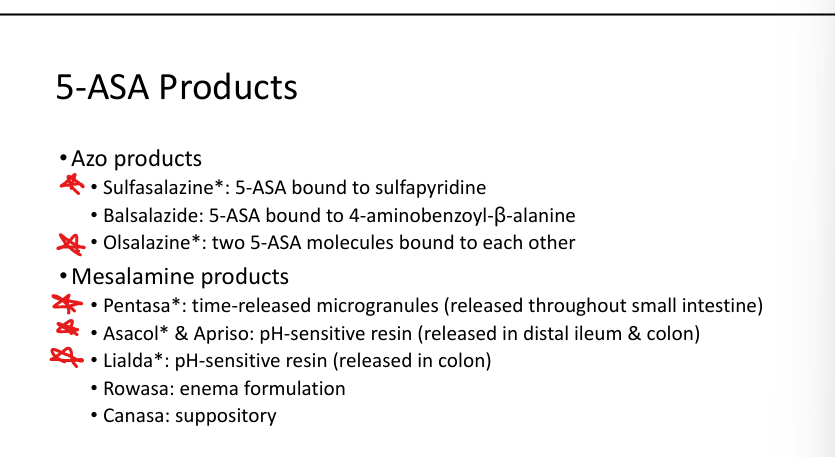
Lialda release site
ASA; pH sensitive release into Colon
Glucocorticoid MOA
Suppress inflammatory cytokines (TNF‑α, IL‑1), chemokines, COX‑2, PLA2, NF‑κB
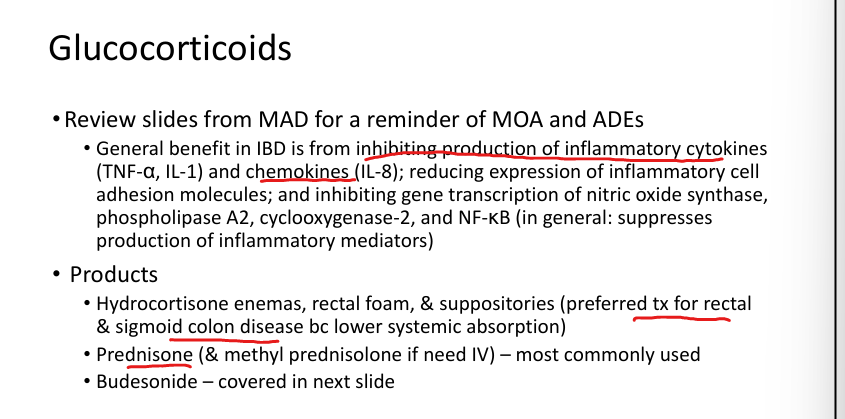
Glucocorticoid uses
Moderate–severe IBD flares

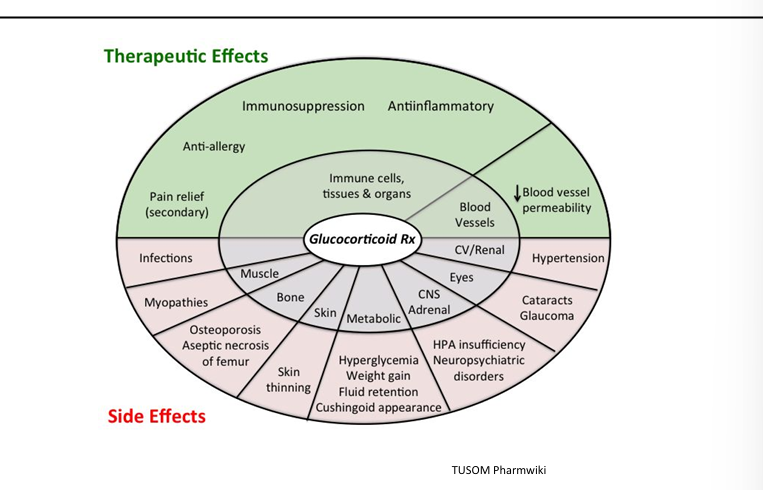
Glucocorticoid adverse effects
Cushingoid features, hyperglycemia, osteoporosis, infections, adrenal suppression
CUSHINGOID: cataracts, ulcers, skin, hump/hypertention, infection, necreosis, growth slowing, osteoporosis, icn ICP, diabetes
Budesonide MOA
Topical steroid with high first‑pass metabolism
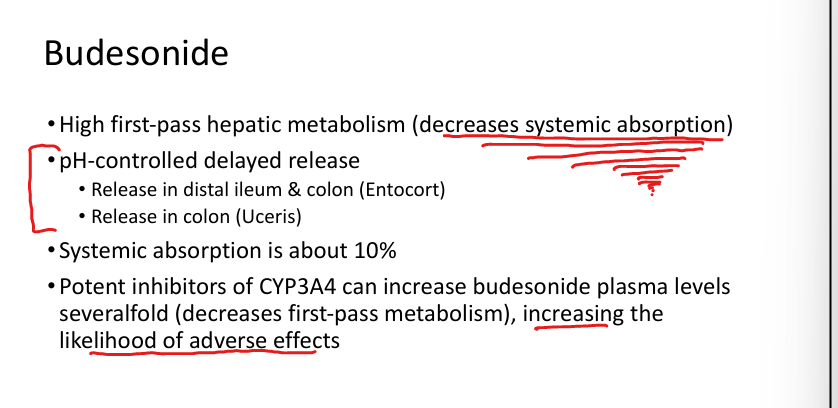
Budesonide uses
Mild–moderate Crohn’s (ileum/proximal colon), UC (Uceris)
Budesonide adverse effects
Increased toxicity with CYP3A4 inhibitors
Azathioprine/6‑MP MOA
Purine antimetabolites → inhibit DNA/RNA synthesis → suppress T‑cells
Azathioprine/6‑MP uses
Crohn’s, UC, autoimmune hepatitis, transplant, rheum diseases
Tofacitinib MOA
JAK inhibitor → blocks JAK‑STAT cytokine signaling; dec inflammation
Tofacitinib uses
Moderate–severe UC
Tofacitinib adverse effects
Infections, TB reactivation, shingles, ↑ cardiac events, DVT, cancer (You dont know Fact Jak)
Ozanimod MOA
S1P receptor modulator → prevents lymphocyte egress from lymph nodes> reduced immune response
Ozanimod uses
Moderate–severe UC, multiple sclerosis
Ozanimod adverse effects
Cardiac conduction issues, liver injury, skin cancers, infections, PML
Ozanimod contraindications
Cardiac disease, untreated sleep apnea, MAOIs
Etrasimod MOA
S1P receptor modulator → decreases circulating lymphocytes>dec inflammatory response (Mod think modulator)
Etrasimod uses
Moderate–severe UC
Etrasimod adverse effects
Cardiac issues, liver injury, skin cancers, infections, PML
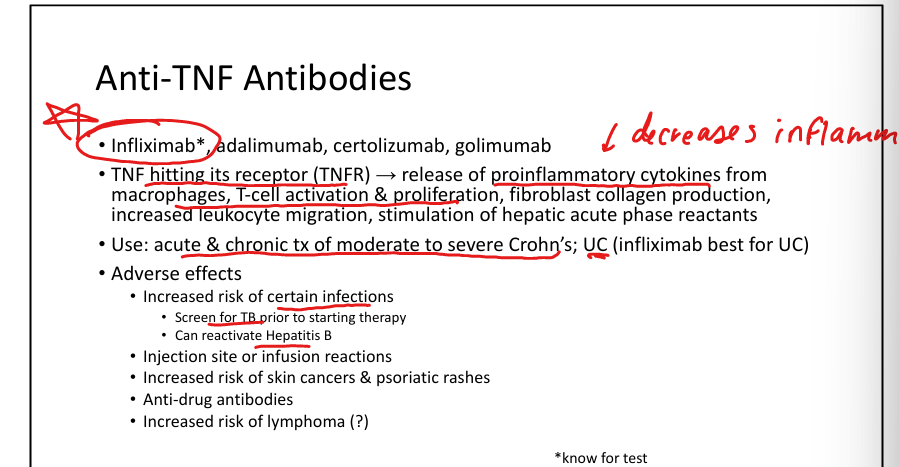
Anti‑TNF MOA
Bind TNF‑α → block pro‑inflammatory signaling
Anti‑TNF drugs
Infliximab*, adalimumab, certolizumab, golimumab
Anti‑TNF (infliximab) uses
Moderate–severe Crohn’s & UC
Anti‑TNF (Inflixamab) adverse effects
TB reactivation, Hep B reactivation, infections, infusion reactions, skin cancers, lymphoma
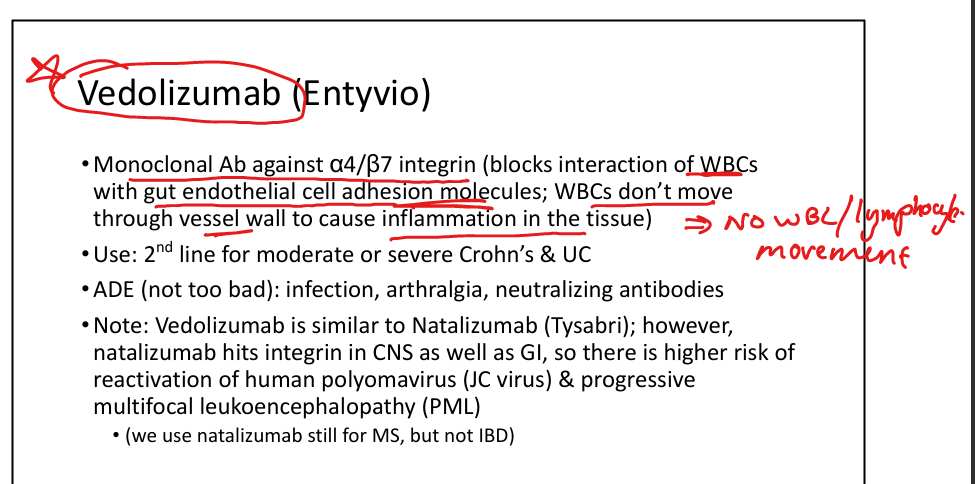
Vedolizumab MOA
Blocks α4β7 integrin → prevents WBC migration into GI tissue>less inflammation (a4b7»no WBC into GI tissue so they get VEDOed)
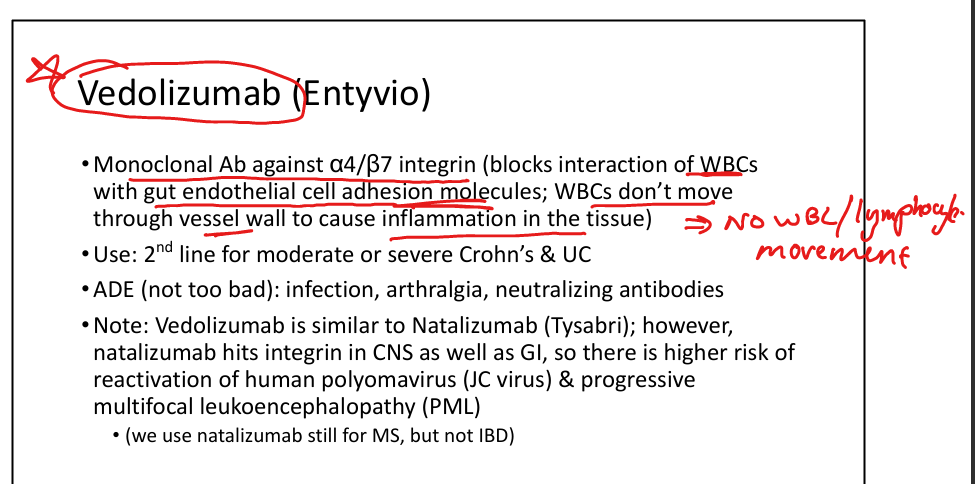
Vedolizumab uses
Moderate–severe Crohn’s & UC (2nd line)
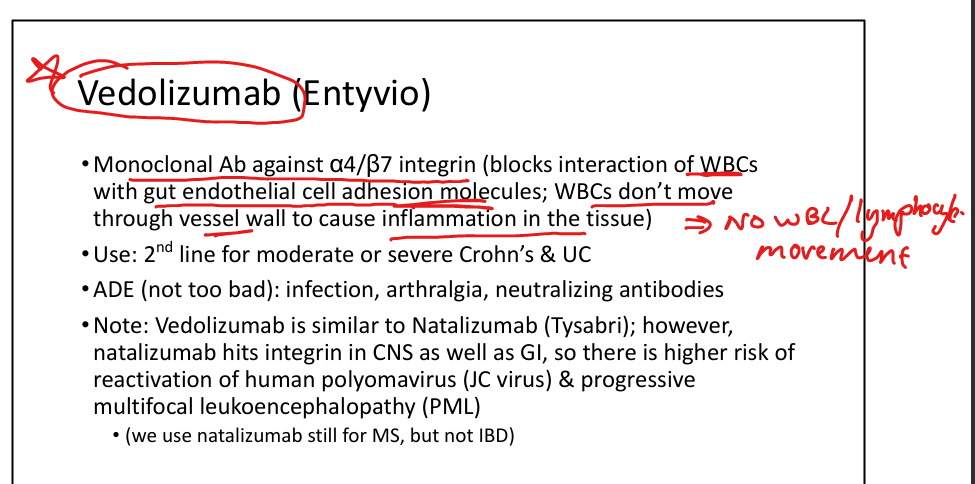
Vedolizumab adverse effects
Infections, arthralgia, neutralizing antibodies
Ustekinumab MOA
Blocks IL‑12 & IL‑23 → inhibits cell‑mediated inflammation (Tom Brady (12) and MJ (23) are kin goats)
Ustekinumab uses
Moderate–severe Crohn’s & UC
Ustekinumab adverse effects
Infections, headache, allergic reactions, slight ↑ cancer risk
Guselkumab(Tremfya) and Risankizumab(Skyrizi); MOA, Uses, ADE
Block IL‑23 p19 → reduce pro‑inflammatory cytokines. Used for Moderate–severe Crohn’s & UC. ADE: Infections, hypersensitivity, headache, liver injury (The goats as well IL23>)
Bulk‑forming laxatives MOA + Ex
Psyllium; Hydrophilic colloids → increase stool bulk → stimulate peristalsis
Osmotic laxatives
Mg salts, sorbitol, lactulose, PEG
Stimulant laxatives MOA
Senna, bisacodyl; Direct enteric nerve stimulation → increased motility
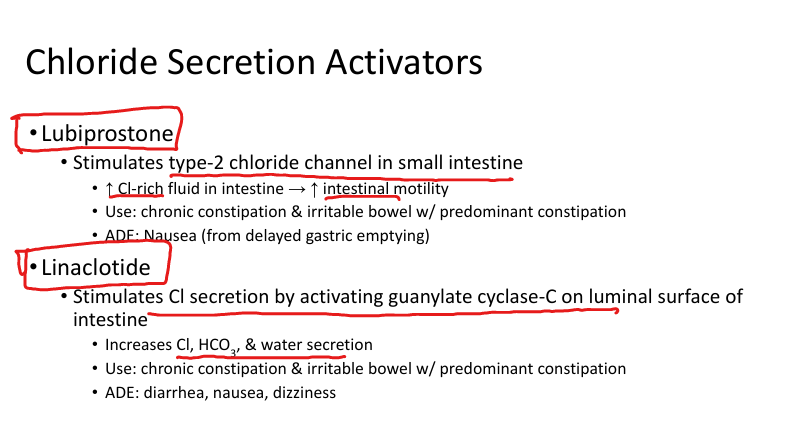
Lubiprostone MOA +uses
Activates type‑2 chloride channels → ↑ fluid secretion; Chronic constipation, IBS‑C (Lube up with Cl)
Linaclotide MOA + Uses
Activates guanylate cyclase‑C → ↑ Cl⁻, HCO₃⁻, water secretion. Used for Chronic constipation, IBS‑C
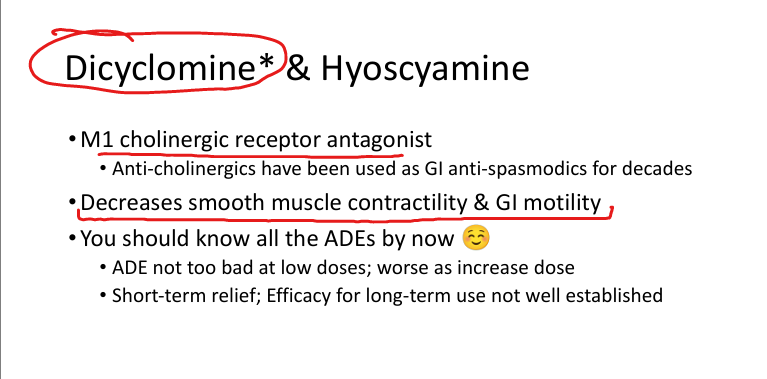
Dicyclomine/Hyoscyamine MOA
M1 anticholinergic → ↓ GI motility & spasm (Clo like cholinergic; DIe cholinergic=anti)
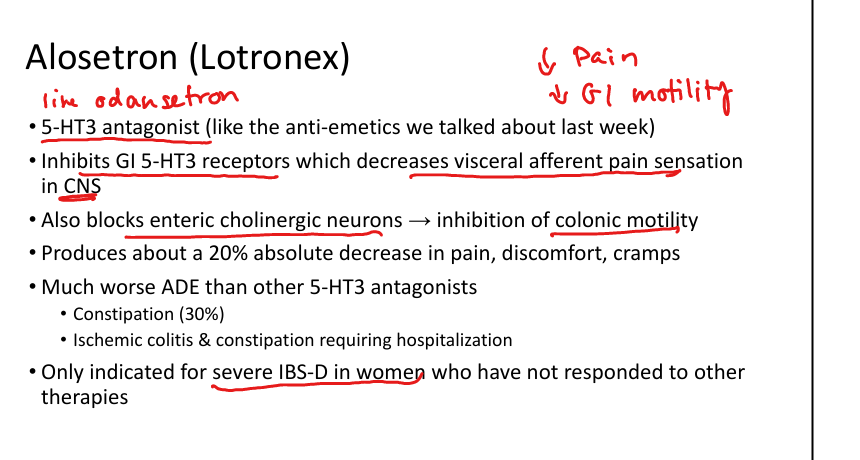
Alosetron MOA
5‑HT3 antagonist → ↓ visceral pain, ↓ colonic motility. Used for Severe IBS‑D in women
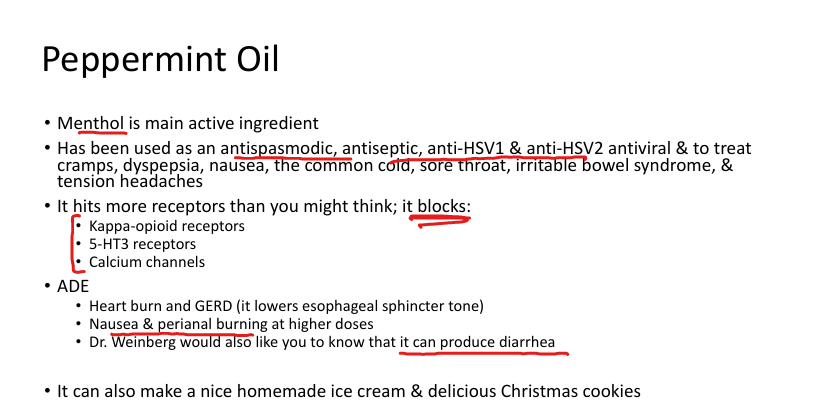
Peppermint oil MOA
Blocks kappa‑opioid, 5‑HT3, and Ca²⁺ channels; Used for IBS-D
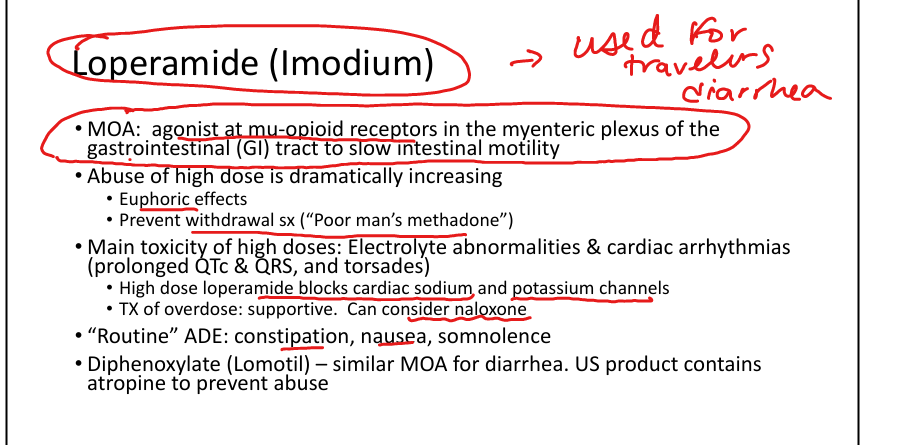
Loperamide MOA
Peripheral μ‑opioid agonist → slows motility. Used for Diarrhea. ADES: QT prolongation, QRS widening, torsades
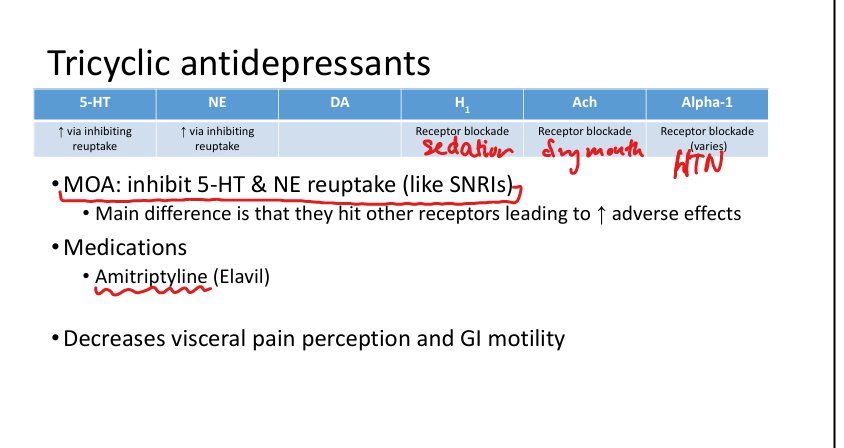
Amitriptyline MOA + Use
Inhibits 5‑HT & NE reuptake; Used for IBS‑D, neuropathic pain, migraine prophylaxis
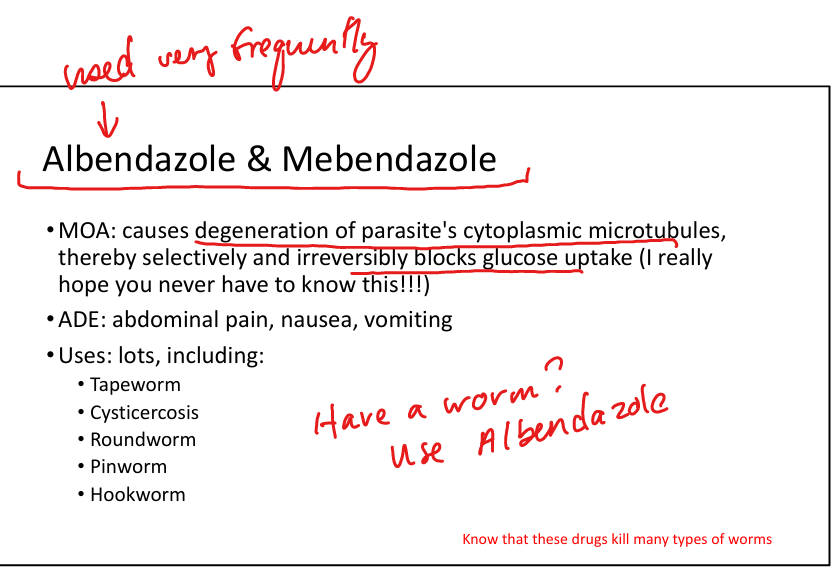
Albendazole/Mebendazole MOA + Use
Inhibit microtubules → block glucose uptake in parasites. Used for worms (Worms are tubes>inbhibit microtubules youre good)
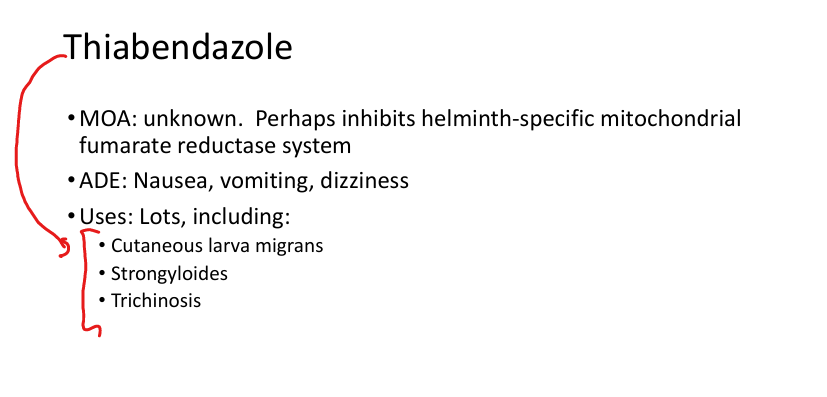
Thiabendazole use
Cutaneous larva migrans, strongyloides, trichinosis
Ivermectin MOA + Use
Opens glutamate‑gated Cl⁻ channels → paralysis of parasite. Strongyloides, scabies
Nitazoxanide MOA
Inhibits pyruvate:ferredoxin oxidoreductase. Used for Cryptosporidiosis, giardiasis
TMP‑SMX MOA + Use
Blocks folate synthesis. Used UTI, MRSA, PCP, Listeria (if pen‑allergic), Stenotrophomonas, Cyclospora
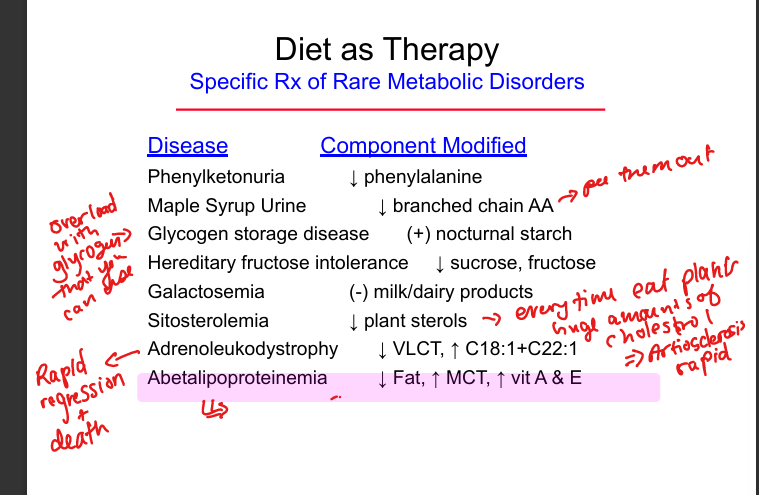
Phenylketonuria dietary treatment
Restrict phenylalanine
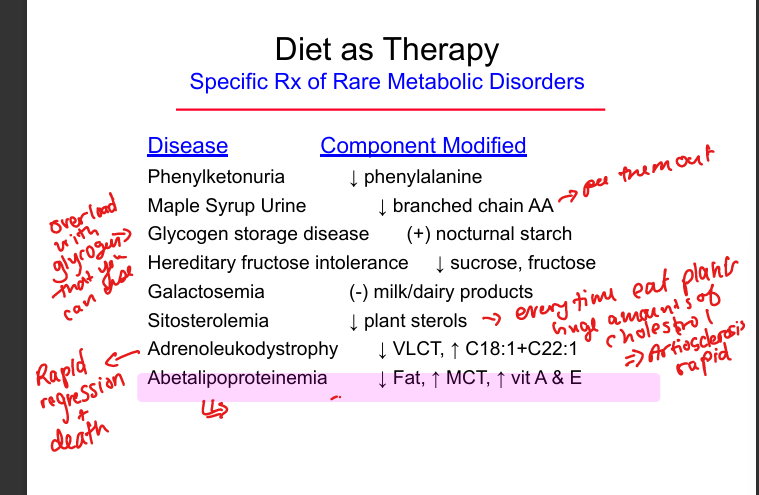
Maple syrup urine disease dietary treatment
Restrict branched‑chain amino acids
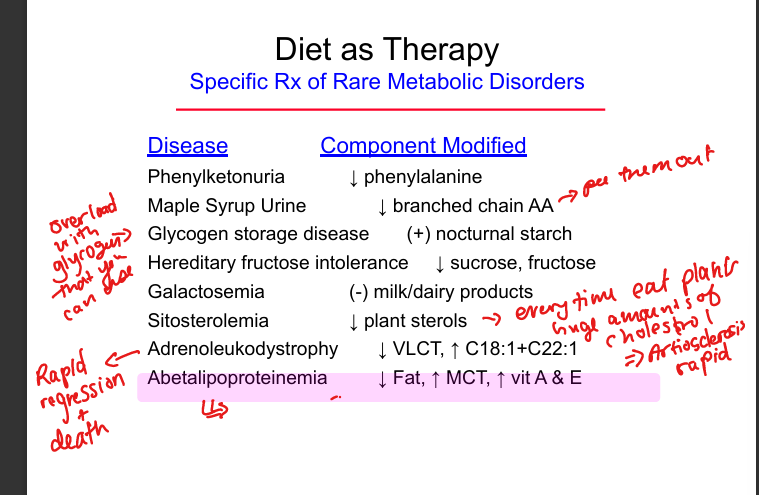
Glycogen storage disease dietary treatment
Provide nocturnal cornstarch
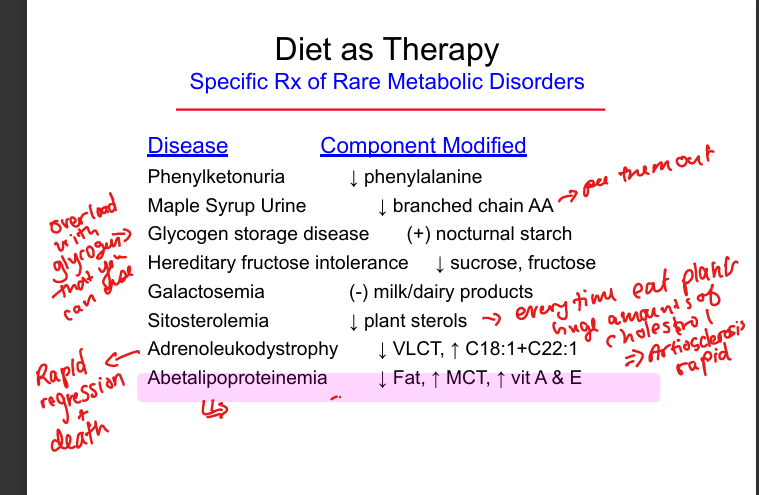
Hereditary fructose intolerance dietary treatment
Avoid fructose and sucrose
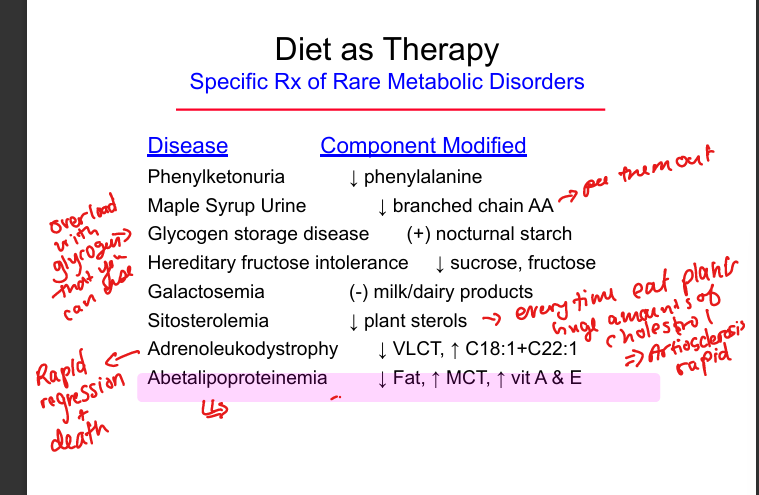
Galactosemia dietary treatment
Eliminate milk and dairy products
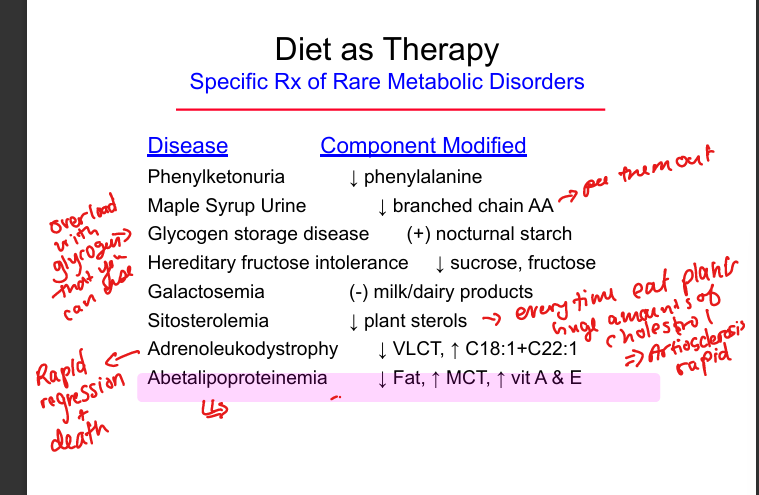
Sitosterolemia dietary treatment
Restrict plant sterols
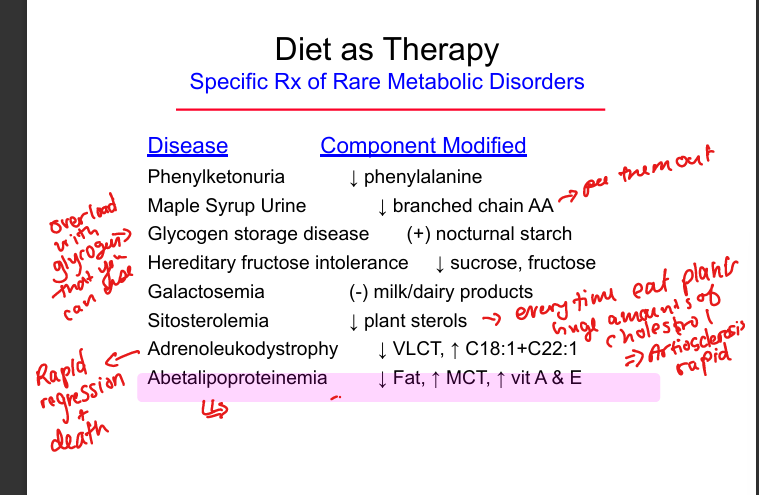
Adrenoleukodystrophy dietary treatment
Restrict very‑long‑chain fatty acids
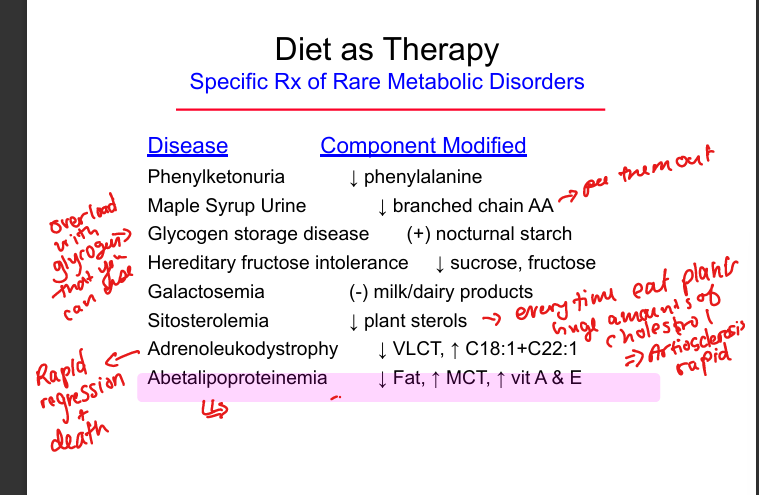
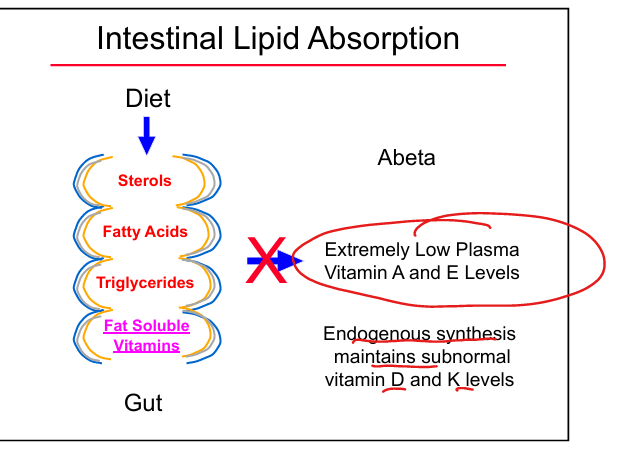
Abetalipoproteinemia dietary treatment
Low‑fat diet, high MCT intake, high‑dose vitamins A and E
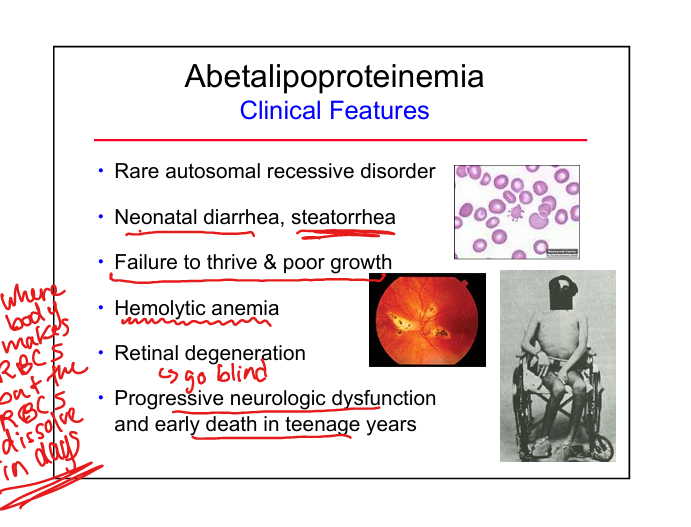
Abetalipoproteinemia clinical features
Neonatal diarrhea, steatorrhea, Failure to thrive, hemolytic anemia, retinal degeneration, neurologic decline
Abetalipoproteinemia biochemical defect
Absent chylomicrons, VLDL, LDL due to MTP mutation»cannot get fat into body
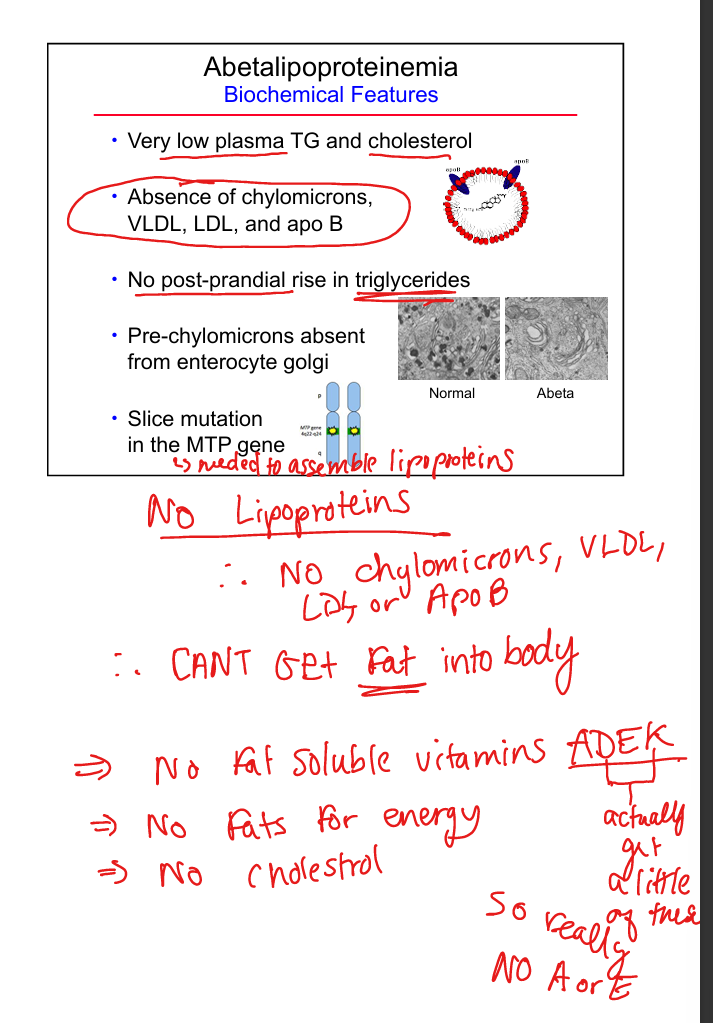
Why abetalipoproteinemia causes vitamin deficiency
Cannot absorb fat‑soluble vitamins (A, D, E, K) A and E particularly because D and K get small endogenous synthesis
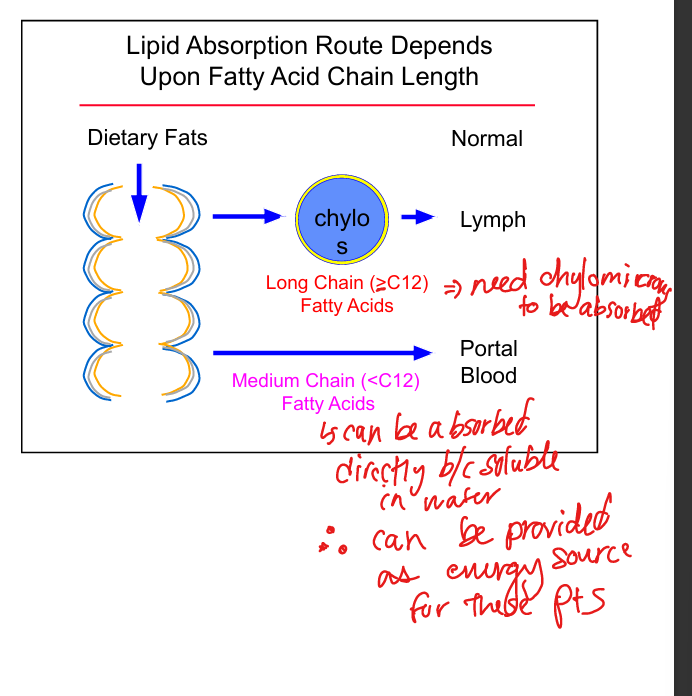
Why MCTs help in abetalipoproteinemia
MCTs are absorbed directly into portal blood without chylomicrons
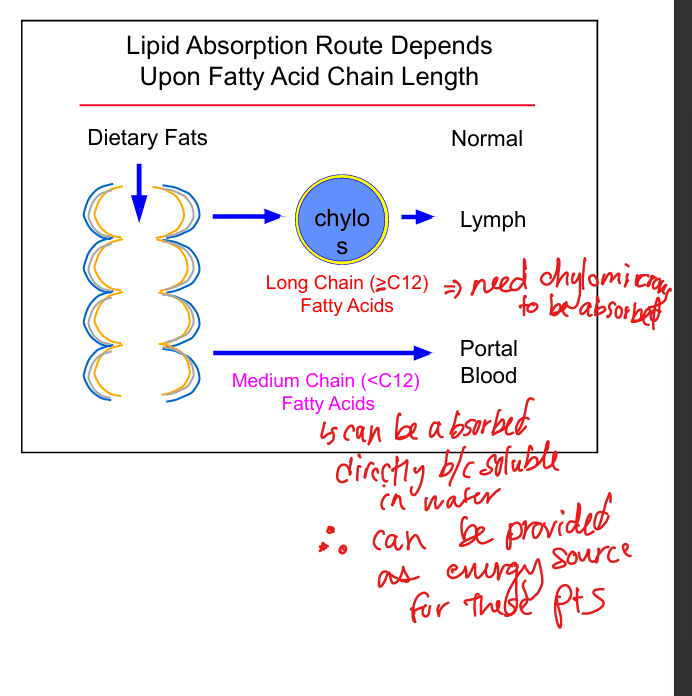
Long‑chain fatty acid absorption
Requires chylomicrons and lymphatic transport
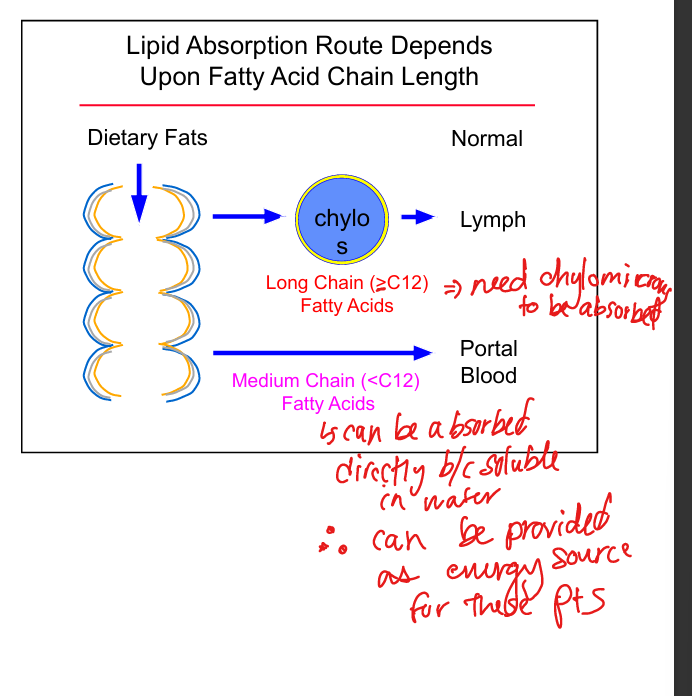
Medium‑chain fatty acid absorption
Directly absorbed into portal circulation
Post‑gastrectomy dietary needs
Increase iron and vitamin B12
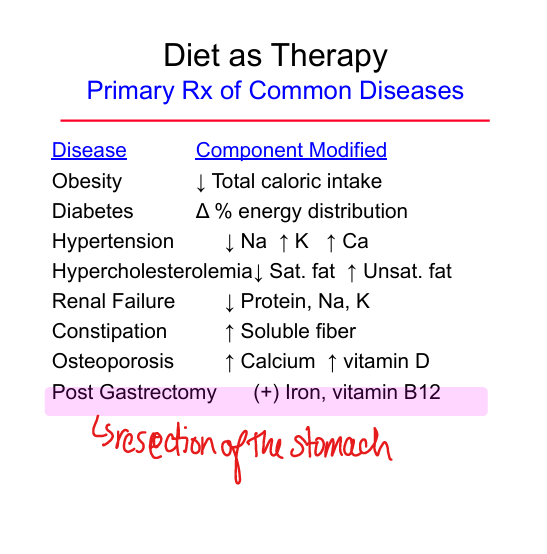
Post‑gastrectomy(removal of stomach) clinical features
Early satiety, dumping syndrome, diarrhea, vomiting, iron deficiency, B12 deficiency
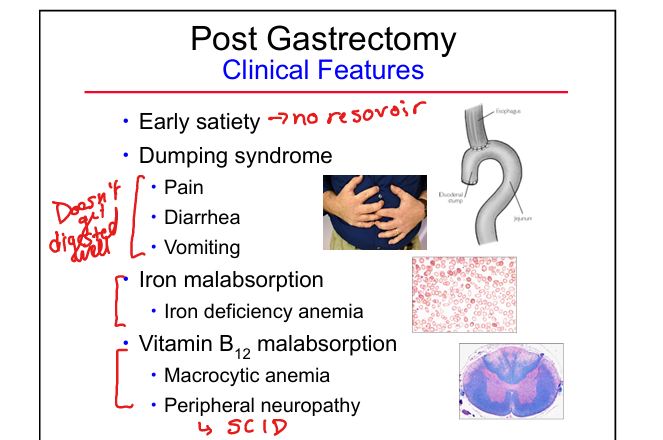
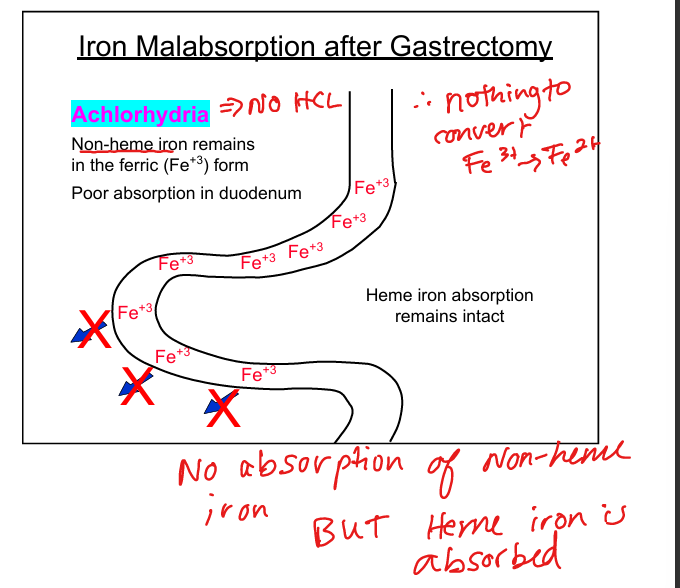
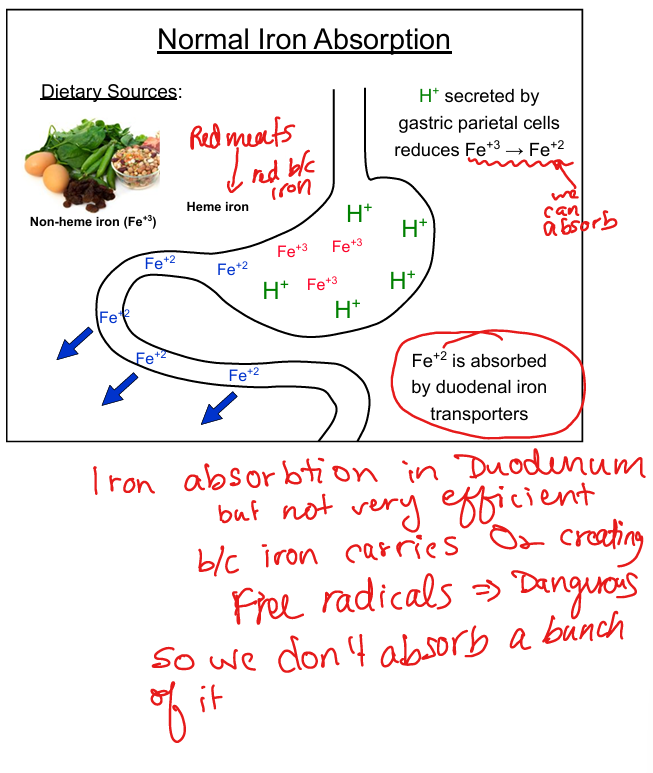
Why gastrectomy causes iron deficiency
Loss of gastric acid prevents Fe³⁺ → Fe²⁺ conversion needed for absorption
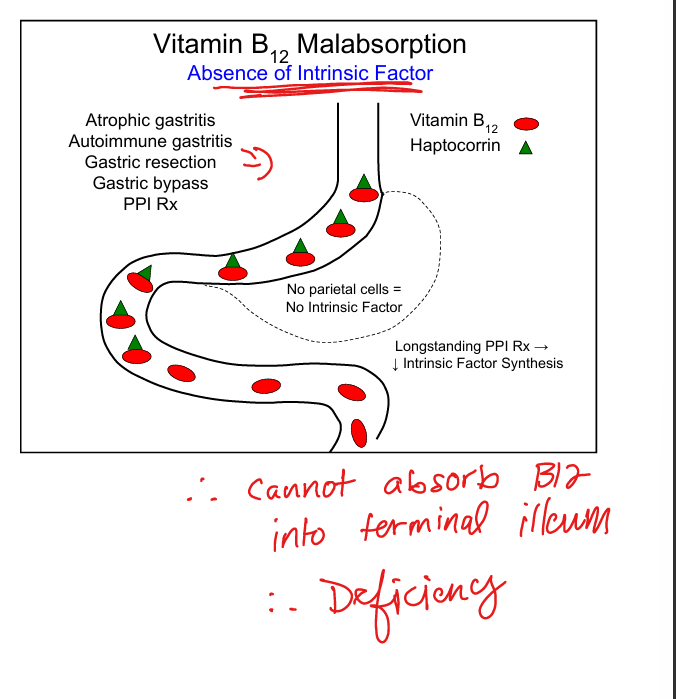
Why gastrectomy causes B12 deficiency
Loss of intrinsic factor from parietal cells prevents ileal absorption
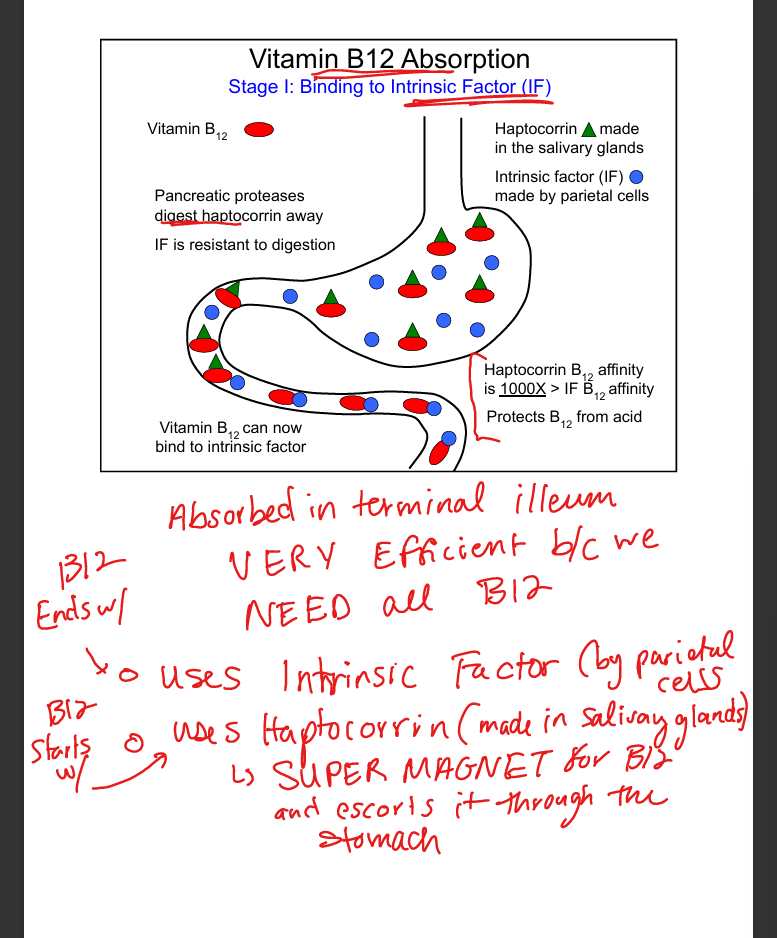
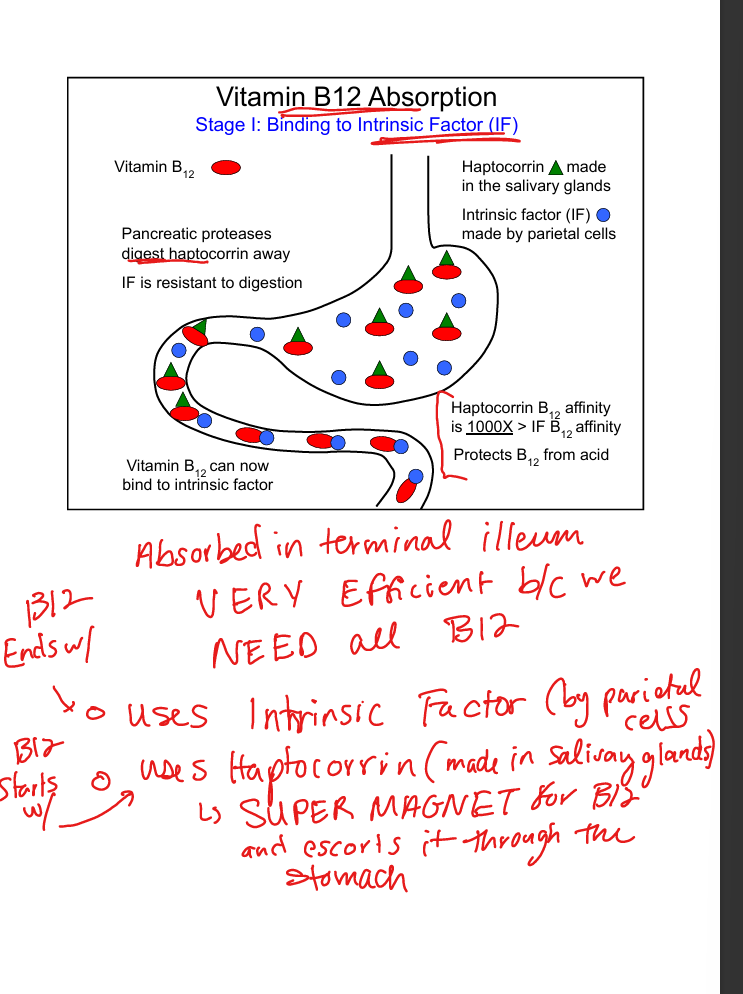
Vitamin B12 absorption step 1
B12 binds haptocorrin in stomach, then intrinsic factor in duodenum
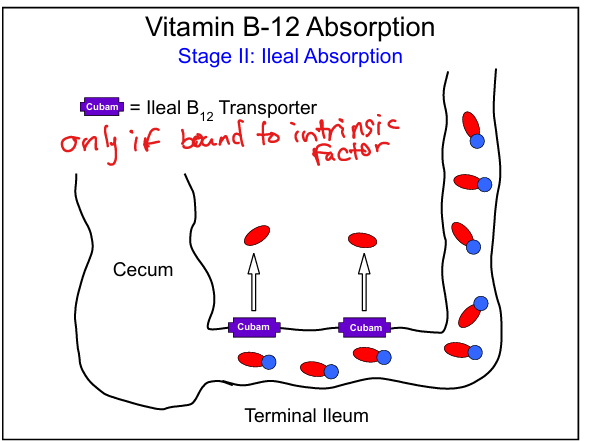
Vitamin B12 absorption step 2
B12‑IF complex absorbed in terminal ileum via Cubam receptor
Causes of B12 malabsorption
Atrophic gastritis, autoimmune gastritis, gastrectomy, gastric bypass, chronic PPI use
Post‑gastrectomy treatment
Small frequent meals, moderate fat restriction, oral iron, parenteral B12
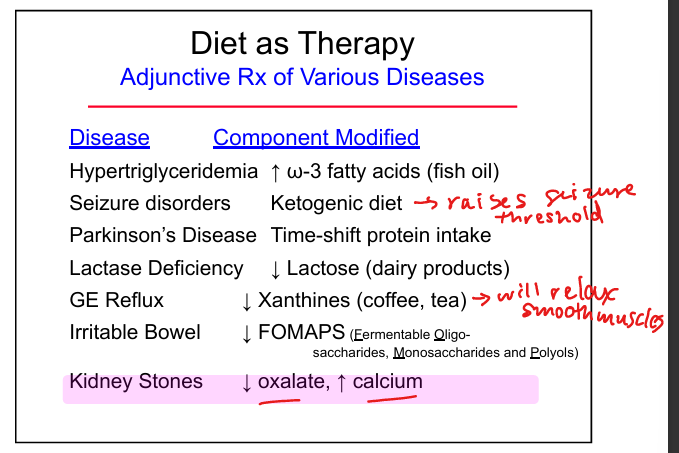
Diet therapy for kidney stones
Reduce oxalate, increase calcium
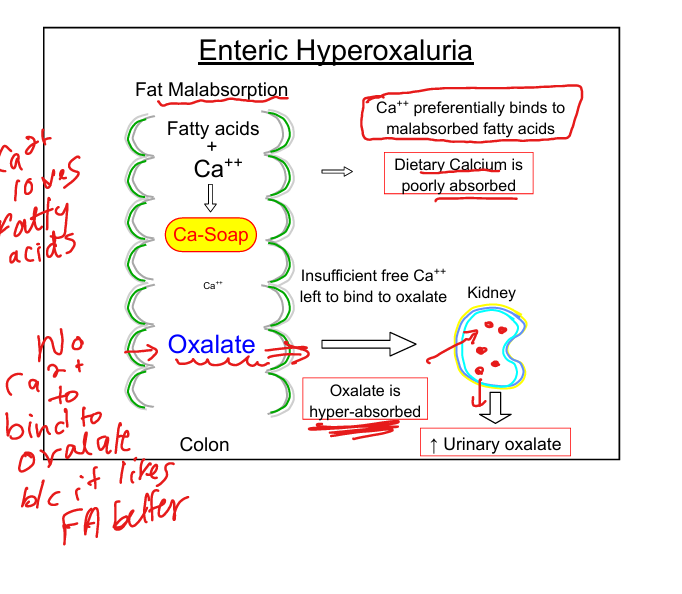
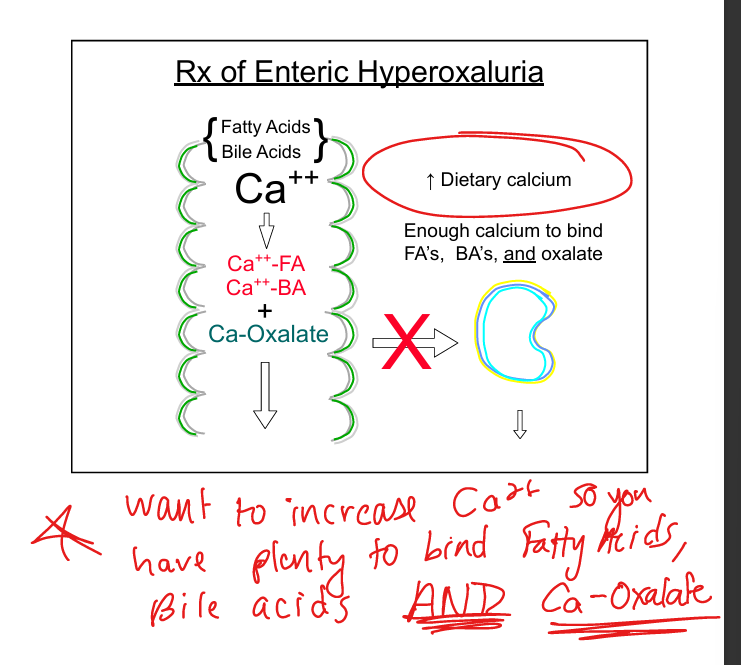
Enteric hyperoxaluria mechanism
Fat malabsorption → calcium preferentially binds fatty acids → free oxalate absorbed → kidney stones
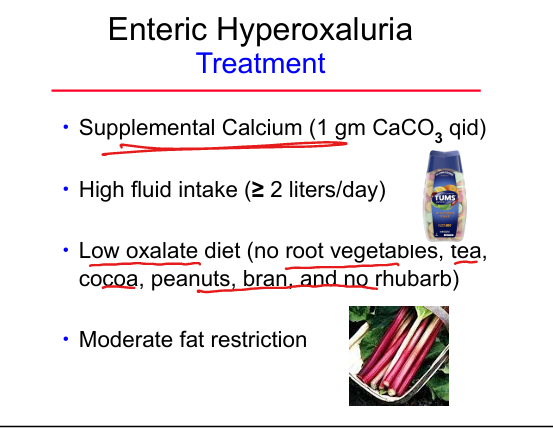
Foods high in oxalate
Root vegetables, tea, cocoa, peanuts, bran, rhubarb
Treatment of enteric hyperoxaluria
Increase calcium intake, high fluids, low‑oxalate diet, moderate fat restriction
Key components of nutrition assessment
Diet history, weight history, symptoms, physical exam, body composition, nutrient stores, daily requirements
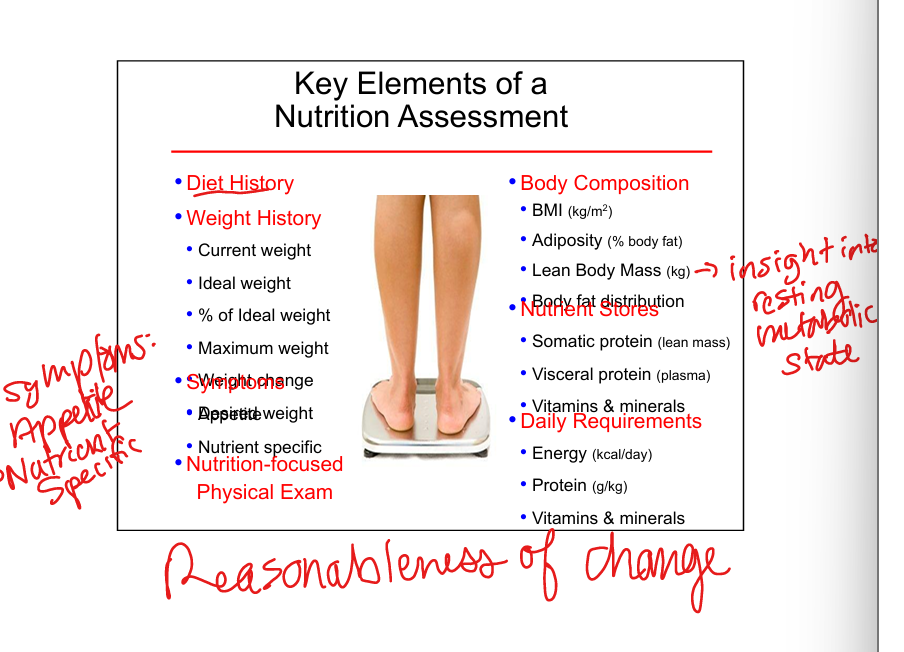
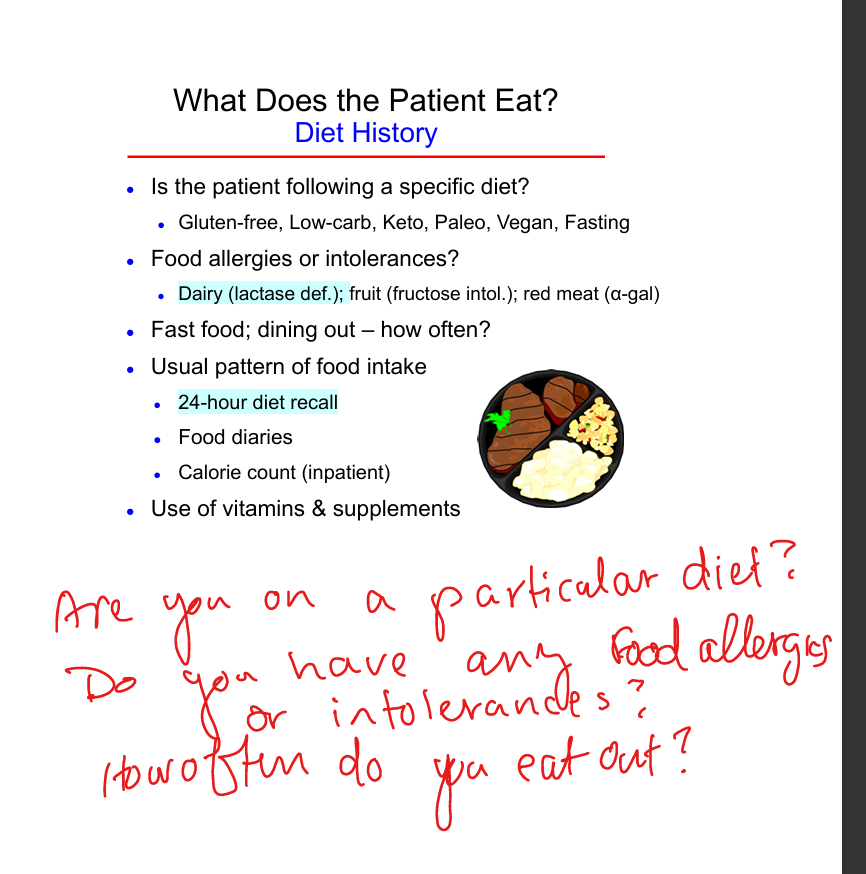
Elements of diet history
Specific diet patterns, allergies, intolerances, fast food frequency, 24‑hour recall, food diaries, supplements
GI conditions affecting nutrition
Dysphagia, gastroparesis, PUD, chronic nausea, diarrhea, celiac disease, Crohn disease
Surgical history affecting nutrition
Gastric bypass, ulcer surgery, bowel resections, cholecystectomy
Chronic illnesses affecting nutrition
DM, CHF, CKD, cirrhosis, cancer, AIDS, TB, SLE
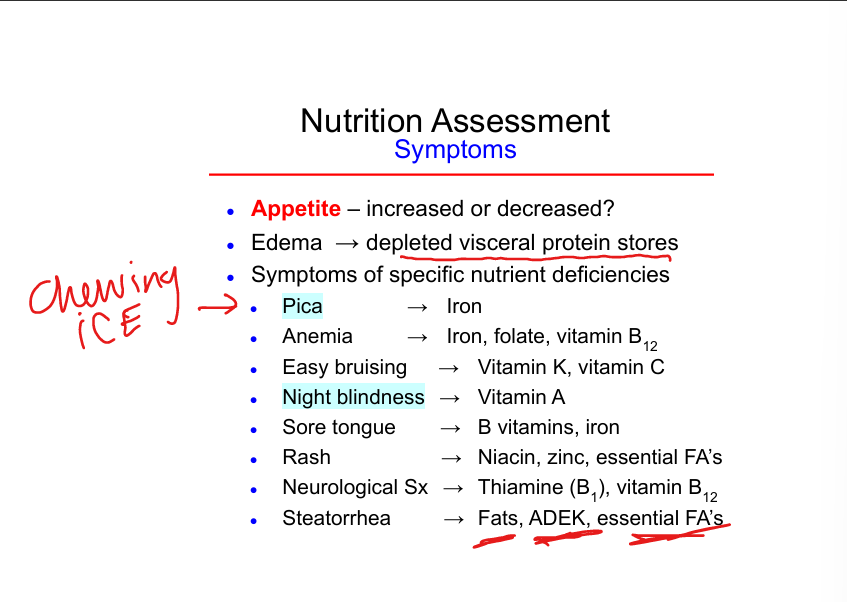
Symptoms of nutrient deficiencies
Pica (iron), anemia (iron/folate/B12), bruising (vit K/C), night blindness (vit A), sore tongue (B vitamins), rash (niacin/zinc), neuropathy (B1/B12)
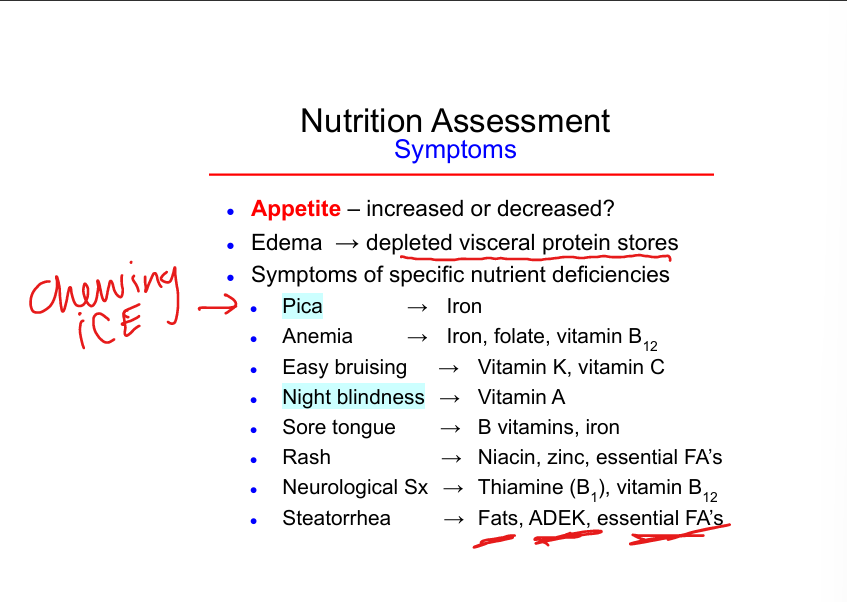
Symptoms of fat malabsorption
Steatorrhea, ADEK deficiency, essential fatty acid deficiency
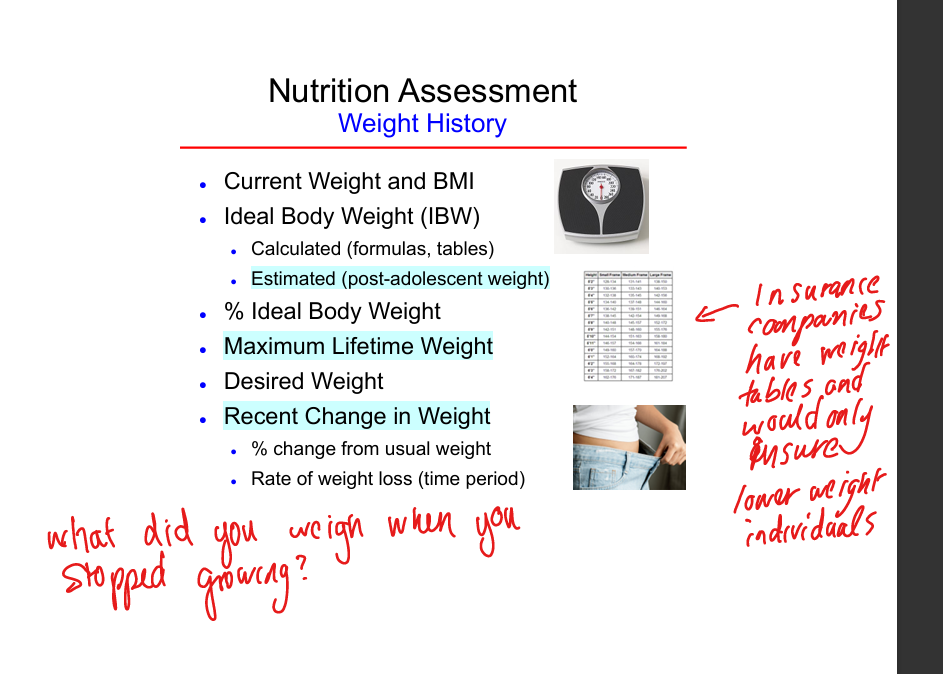
Weight history components
Current weight, ideal weight, % ideal weight, max lifetime weight, desired weight, recent weight change
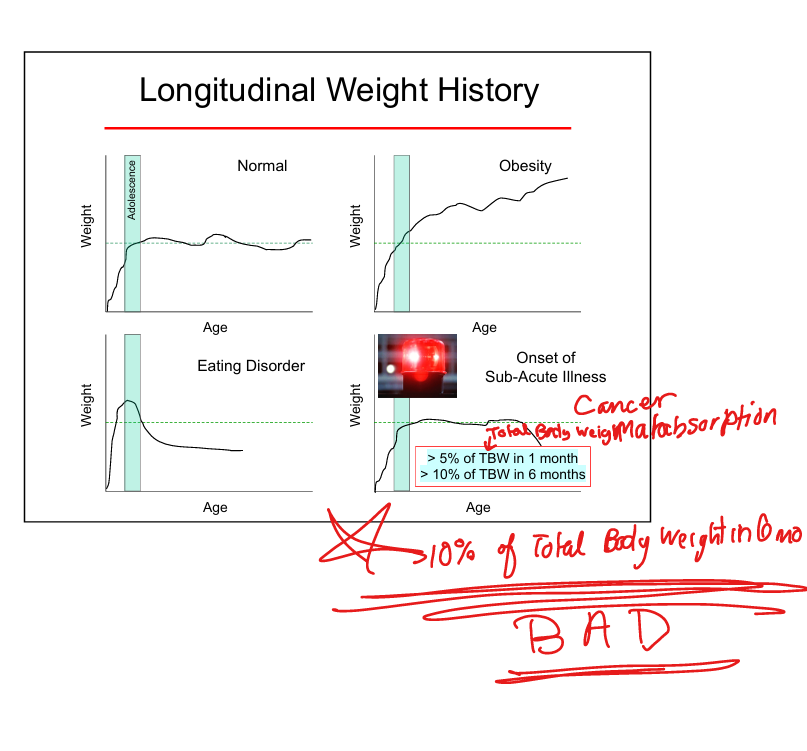
Significant weight loss thresholds
5% in 1 month or >10% in 6 months
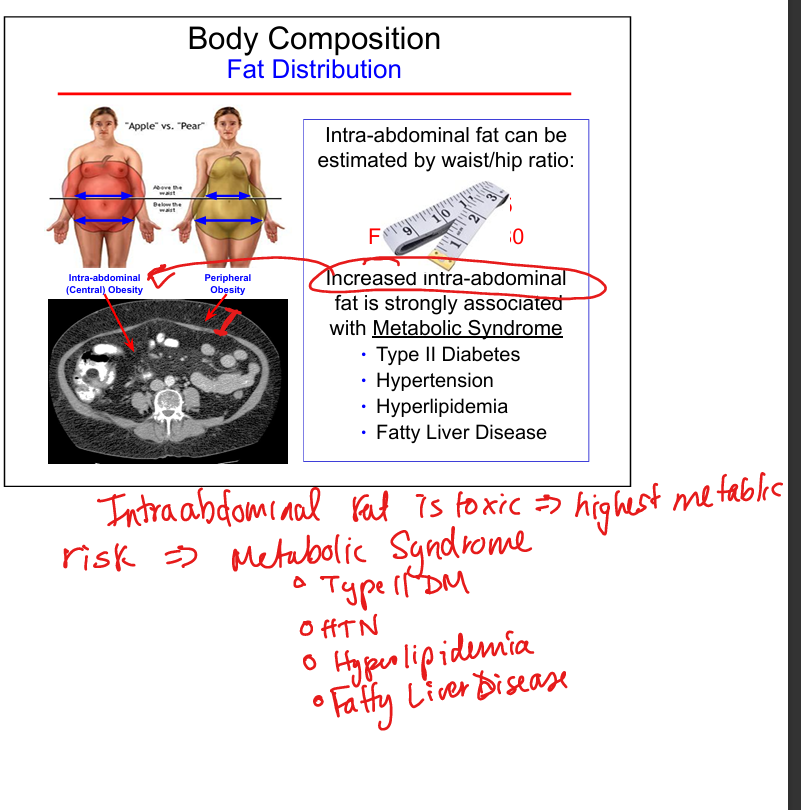
Central vs peripheral obesity
Central obesity(intraabdominal) linked to metabolic syndrome and higher cardiometabolic risk
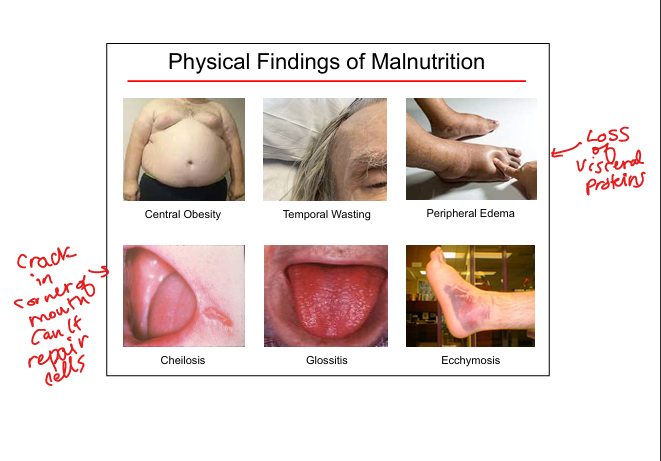
Physical signs of malnutrition
Temporal wasting, glossitis, cheilosis, peripheral edema, ecchymoses
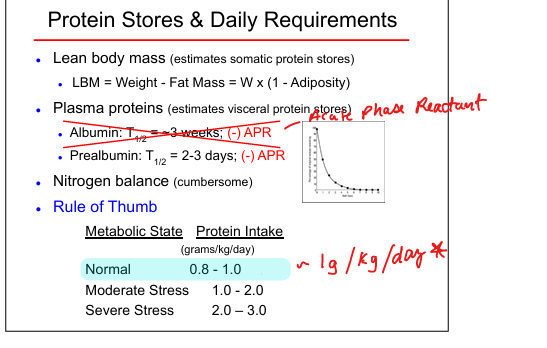
Protein requirement rule‑of‑thumb
Normal 0.8–1 g/kg/day
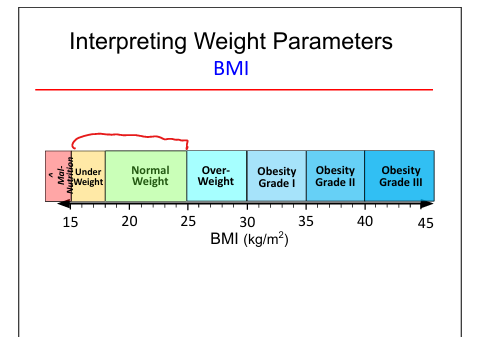
BMI Parameters
<15 manourished;15-25 Normal; 25-30=overweight; 30-35 Obesity 1; 35-40 Obestity 2; 40-45 Obesity 3
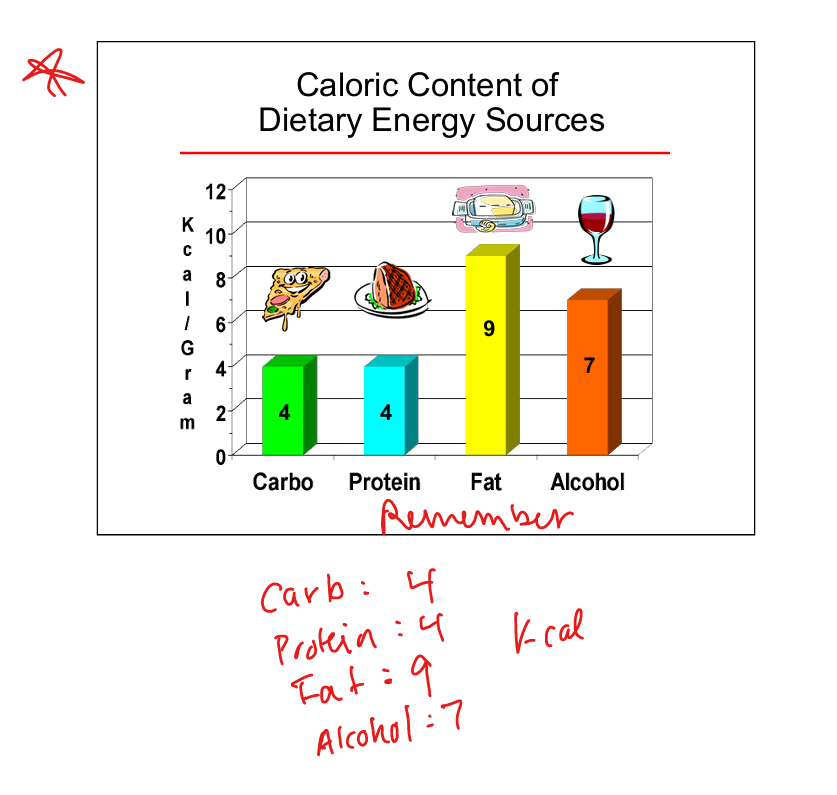
Caloric value of carbohydrates
4 kcal per gram
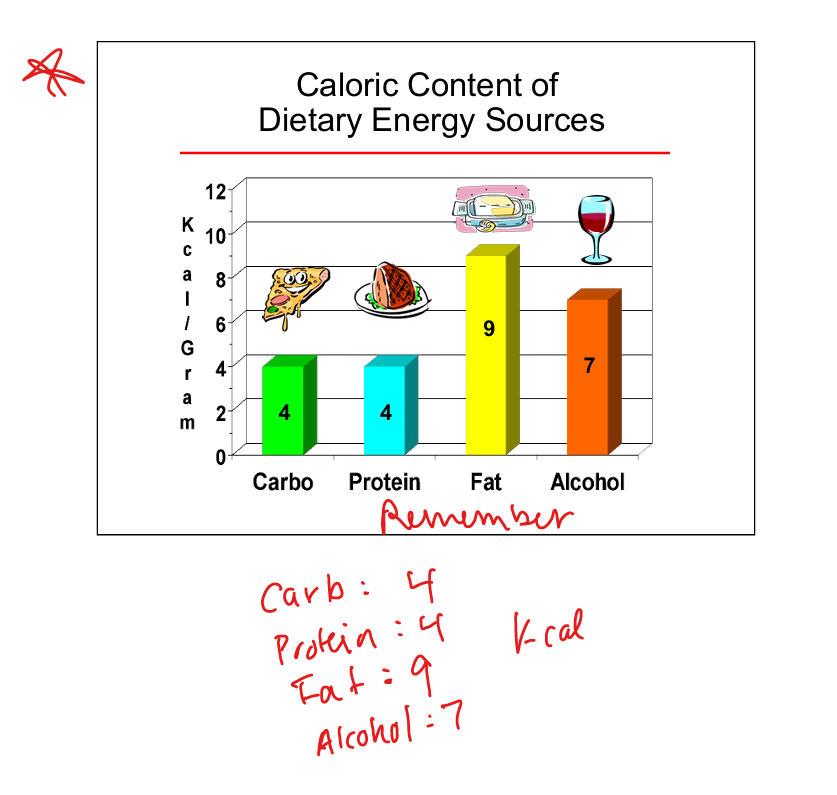
Caloric value of protein
4 kcal per gram
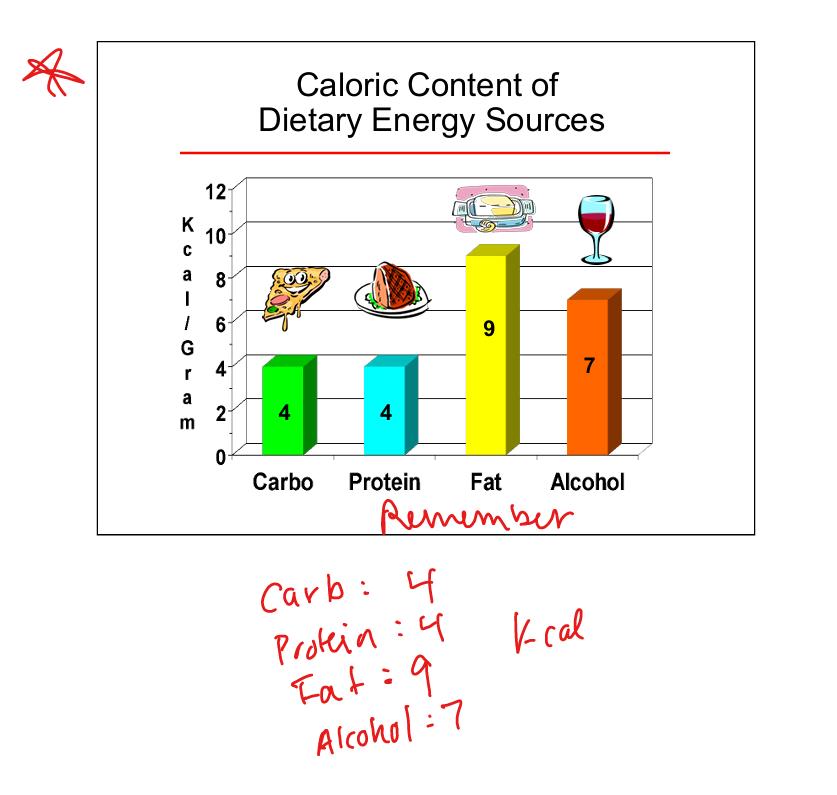
Caloric value of fat
9 kcal per gram
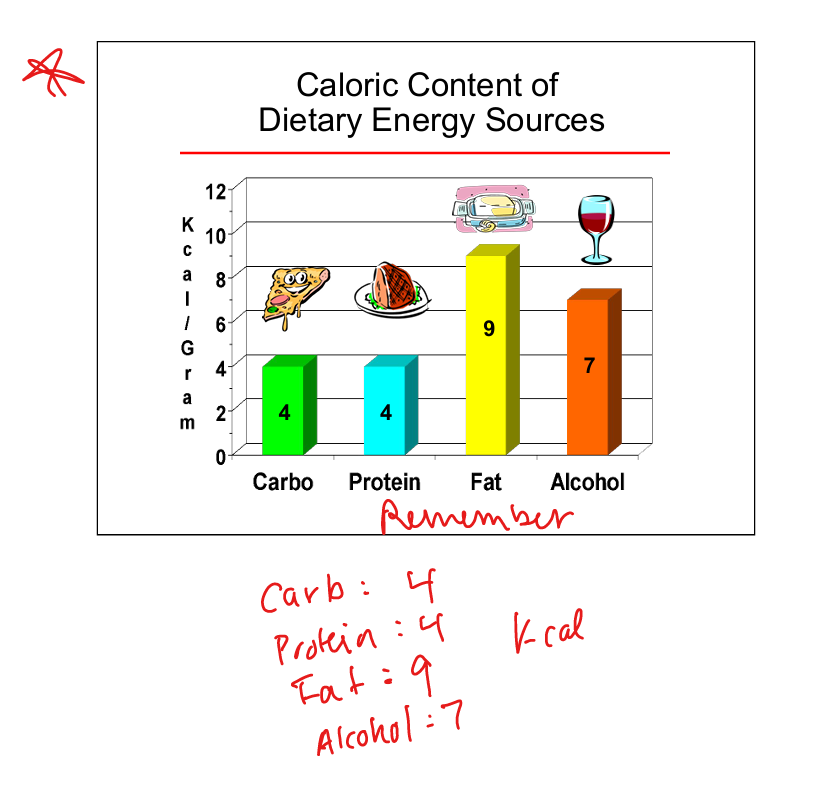
Caloric value of alcohol
7 kcal per gram
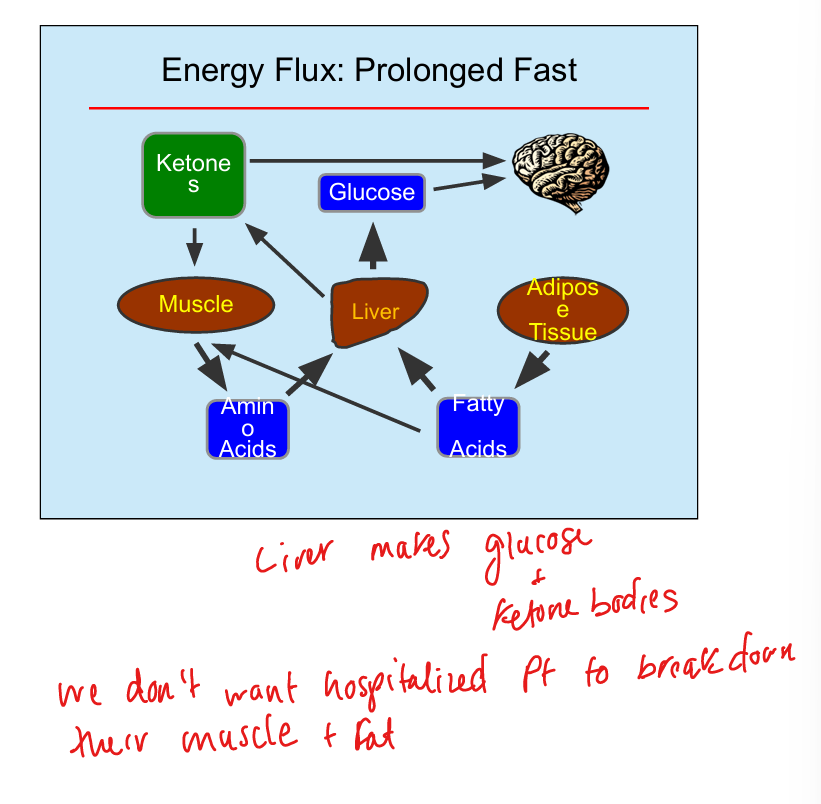
Prolonged fast energy state
Ketone production increases
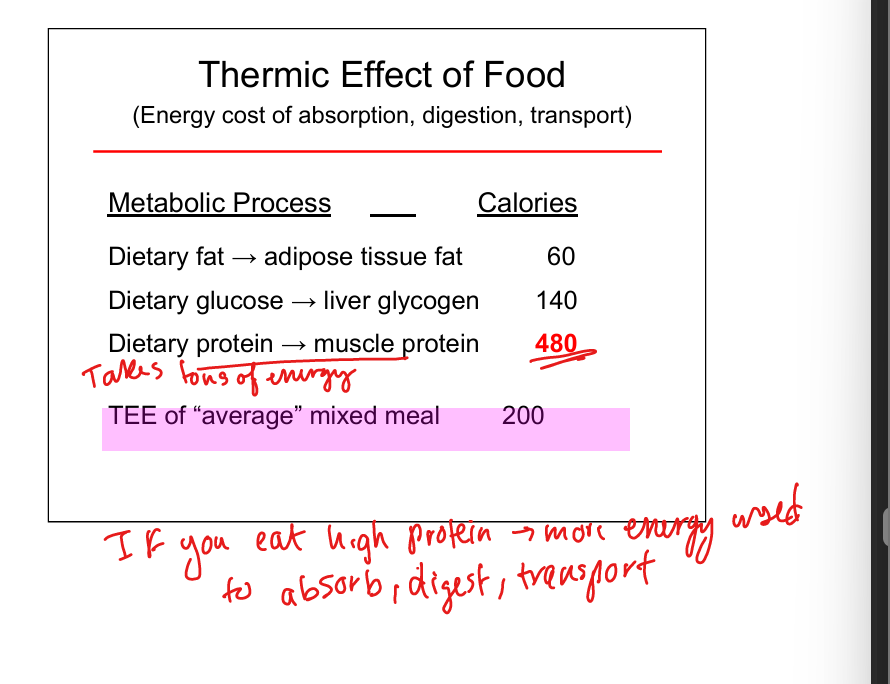
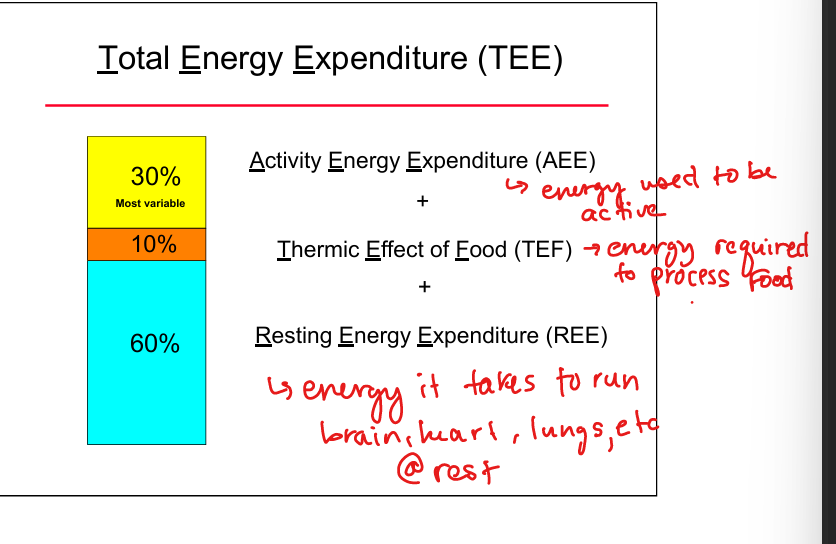
Components of total energy expenditure
Resting energy expenditure (REE), thermic effect of food (TEF), activity energy expenditure (AEE)
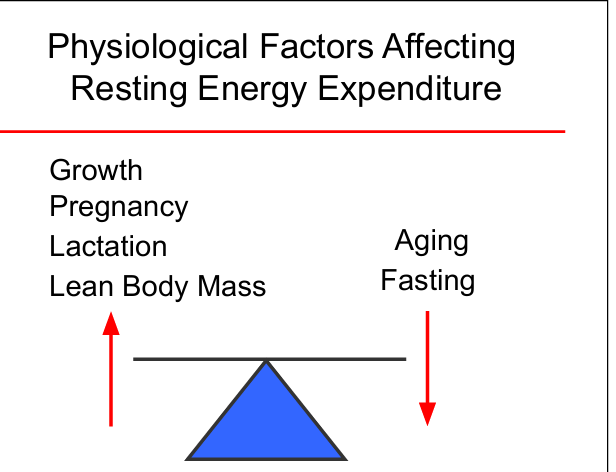
Factors increasing Resting Energy Expenditure
Growth, pregnancy, lactation, fever, sepsis, hyperthyroidism
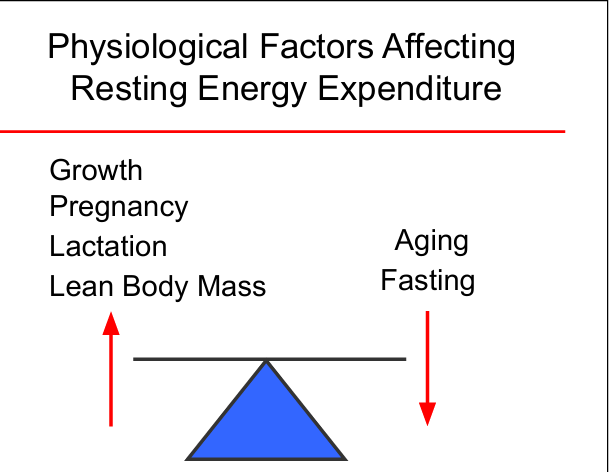
Factors decreasing Resting Energy Expenditure
Aging, fasting, hypothermia, hypothyroidism
High‑protein diet effect on Thermic Effect of Food
Increases energy expenditure due to higher digestion cost