Lecture 5- BMP and CMP
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
what is included in a BMP
kidney function:
BUN
creatinine
eGFR calc
endocrine
glucose
electrolytes:
calcium
sodium
potssium
chloride
blood gas/pH
CO2 (bicarb)
checking volume, acid/base, CHF, and kidney failure
components of CMP
all of BMP +
albumin
alkaline phosphate
alanine aminotransferaase
aspartate aminotransferase
bilirubin
checiing liver funvton adn nutritional status
when to order BMP vs CMP
BMP
routine screening
monitor electrolytes
renal function
acid base stsus
glucose
common in: ED, preop, medication monitoring (diuretics, ACE inhi, ARBs)
CMP
hepatic func also neeeded
common in : annual wellness exam, sus liver diseasem mutritional assessment
creatinine (Cr)
only excreted by kidney
produced by skeletal muscles as part o fmetabolic preocesses
released into circualtion at constant rate
freeely filtered acrss glomerulus
no reabsorbed by tubules→ secreted in minimal amnts
decreased filtration bu kidneys → ioncreased serum lvels
can be impacte dby muscle mass:
lw ,uscle mass an cause artificially low level → over estimating GFR and renal fucntion
high muscle mass can cause higher levels of creatinine → under estimarte GFR and renal function
acute kidney injury and Cr
increased serum Cr by 0.3mg/dL or 50% in 48 hrs → AKIN
factors that control for creatinine testing
age
ethnicity
gender
blood urea nitrogen (BUN)
reflects urea prod (liver) adn resabsoprtion/secretion (nephron)
azotemia= increase in BUN
more nitrous waste in blood than usual
dietary protein intake, muscle mass, asvanced preg
elevated BUN→ upper got it! bleedm protein overloas, corticosteroids
BUN: Cr
assess kidney ad nliver function
increase ith age and wirh decreasing muscle mass
ratio <20:1
prerenal causes- voluem depletion
ratio 20:1
intrinsic renal causes (glomeruloenohritis, CKD)
eGFR
assess kidney fiunction
calculated with CKD-EPI equation
glucose
assess blood glucose lvels; eval for diabetes
critical values: <50 and >450mg/dL (male); <40 and >450 (female)
sodium (Na+)
critical values <120 or >160mEq/L
assess fluid and electroplyte balance
primary extracellular cation
determine dby dietary AN uptake and renal excretion
fluid/voluem stasis
serum osmolality: measur o focnc of solutes in blood serum
hyponaturemia
low levels of Na+
impact both brain asndn nervous ystem
timing: acute (48 hours) vs chronic > 48 hours
sx hyponaturemia
weakness
headache
conusionm delerium
lethargy
stupor
coma
hyponaturemia- hypovolemic
diuretics
GI loss (vomit, diarrhea)
hyponaturemia- euvolemic
SIADH
med, pain, psychosism surgery
hyponaturemia- hypervolemic
HF
cirrhosis
nephrotic syndrome
CKD
acute kidney injury
hypernatremia
incrased morbidity and mortality
mvmt of water in adn out of cell→ demyelination
sx hypernatremia
orthostatis HTN
tachycardia
dry mucu smembranes
fagtigue, lethary
non speciifc weakness
seizures
coma
associations hypernatremia
increase Na intake
dietary, IV fluids
decraease Na loss
cushing syndrome - aldosterone like effect (increase serum Na)
hyperaldosteronism
increase free body water loss→ increase Na
GI loss
excesive sweating
diabetes insipidus - ADH deficiency
sectensive burns
osmostic iduesis
decreased fre body water loss
restrained
sedated
intubated
med:
steroids
estrogens and OCP
laxatives
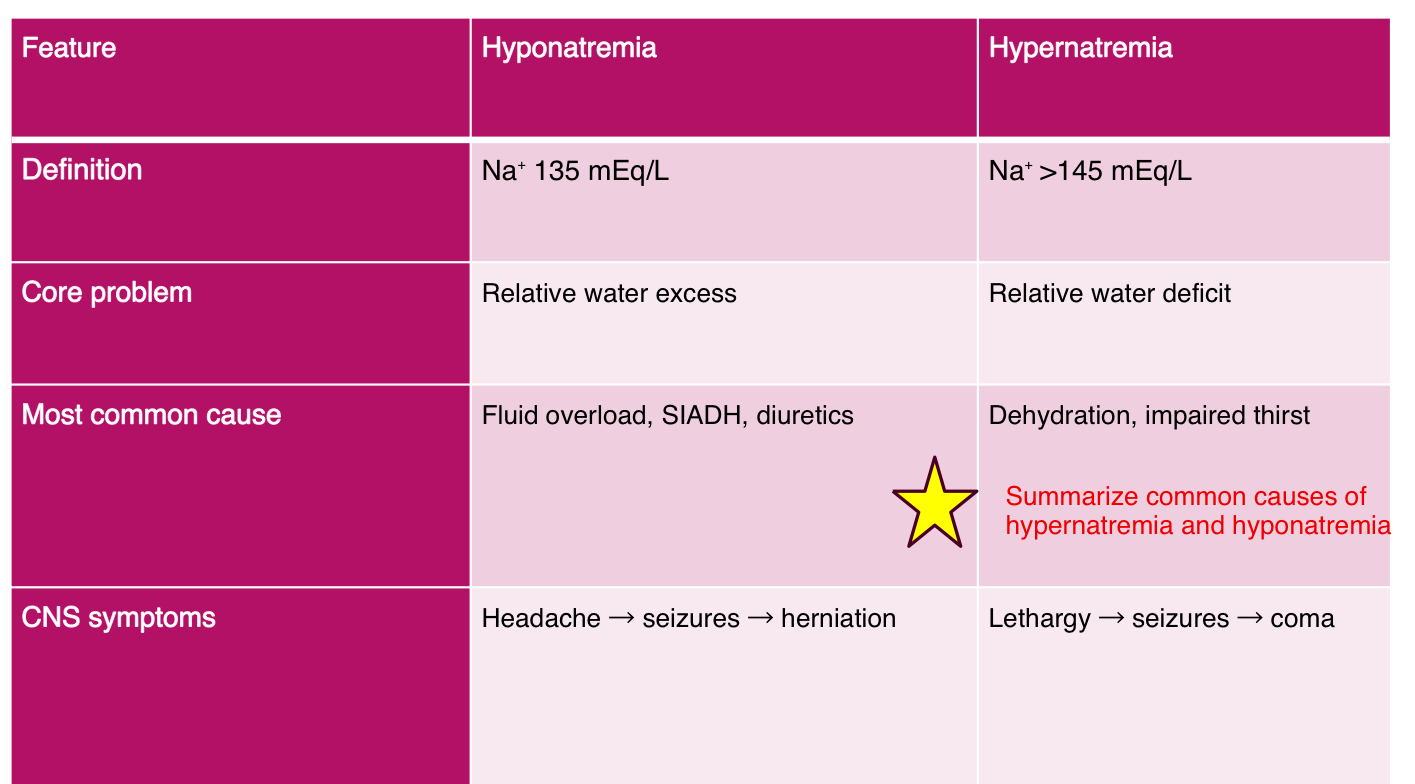
common causes of hypernatremia and hyponatremia
calcium (Ca)
use: neuromuscular disease, cardiac function, bone metabolism, eval PT function, renal diseases and some malignances
correct for hypoalbuminemia, pH status, prolonged torniquet time
hypercalcemia
hyperparathyroidism
malignancy
excessive vit D intake
thiazide diuretics
hypocalcemia
hypoparathyroidism
low vit D
renal failure
Mg deficiency
massive transfussion
potassium (K)
critical values: <3 or >6.1 mmol/L
important in caridiac function; maintenance of memebrane elcetrical potential (neuromuscular tissue) affecting heart rate and contractility
most abundant intracellular cation
excreted by kidneys with NO renal resorption
levels can drop if not adequte in diet or IV infusion
common factors affecting K
meds
dietary intake
renal dysfunction→ acid-base balance - alkalotic states lower serum K, acidotic states INCREASE serum K
hypokalemia
low levels <3.5 mEq/L
decrease contractility
ascending muscel weakness
paralysis
cardiac arrhythmias excentuated
ECG changes
causes of hypokalemia
decrease K intake
dietary and IV
insulin admin- pushes K and glucose into cel
diuretics→ need K supplementation
burns
GI
hyperaldoseteronism
sudhings
renal tuubular acidosis
renal artery stenosis
acites
alkalosis
ensure Mg is good→ or else wasting us eof K bd Mg in charge of K regrulation
hyperkalemia
high levels >5.5
symptoms:
irritability
nausea/vomiting
GI cramping/colic
diarrhea
signs:
ascending muscel weakness
paralysis
cardiac arrhythmias
ECG→ peaked T waves, widened QRS, depressed ST
hyperkalemia causees
increase K intake
dietary, IV
acute/chronic renal failure- inability of kidneys to excrete K
addisons disease
hypoaldosertonism
acidosis (diabetic ketoacidosis)
crush injury
dehydration
medications:
beta blockers
ACE inhibitors
aldosterone inhibiting diuretics
Chloride (Cl)
use: electrolyte, extra cellular anion
functions:
maintain electrical neutrality as salt with Na
affects water balance- water moves with sodium and chloride
buffer in acid-base - CO 2 cation increasem bicarb (anion) moves from intracellular space to extracellular space, Cl- will move back into cell to maintain electrical neutrality
carbon dioxide (CO2)
assess serum pH and electrolytes
major role in acid-base balance
CO2 on BMP actually measures total carbon dioxide in venous blood, which is predoinately composed of bicarb (HCO3-)
BMP CO2= serum bicarb
ABG PaCo- dissolved CO2 gas
respiratory component
Cl and CO2 relationship
inversely related
Cl often moves inversely with bicarb
CO2 reflects bicarb (main buffer against acid)
confounding factors : pseudohyperkalemia
hemolysis (hemolyze as drawn)
erythrocytosis (extrme)
thrombocytosis (K released from platelets durign clotting)
prolonged tourniquet time
fist clenching during blood drawn
confounding factors : pseudohyponaturemia
flasely low Na due to elevated lipids or proteins in serum
check serum osmolarity- its normal
confounding factors: psuedohypocalcemia
hypoalbuminemia- Ca is bound to albumin in serum
MUST calculate correct Ca
corrected Ca= measured Ca+ 0.8 x (4.0- albumin)
confounding factors
acid-base status affects
acidosis shifts K extracellualry (increase serum K)
alkalosis shifts K+ intracellulary (decrease serum K)
specimen handling:
delayed processing, pneumatic tube transport, adn temp extreme acan cause hemolysis→ false increase K
BUN elevation w/o renal dz
upper GI bleed, high protein diet, corticosteroids, catabolic states
Cr limitations:
affected by muscle mass (m=low in elderly→ overestimate GFR)
IV fluid contamination:
drawing bloof from lien running IV fluids can dilute or concentrate electrolytes