Week 7: childhood and adolescent disorders
1/29
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
30 Terms
externalising vs internalising
externalising disorders:
create problems for external world
breaking age-appropriate social rules/disobeying parents and teachers
anger and depression
impulsive
internalising disorders
create problems for internal world
anxiety
sadness
ADHD external
A: Persistent pattern of inattention and or hyperactivity-impulsivity
A1: inattention: 6 or < for at least 6 months
A2: hyperactivity and impulsivity: 6 or more symptoms for at least 6 months (for >17 5+ for 6 months
B: serveral symptoms present BEFORE 12 years old
C: symptoms present in 2 or more settings
D: interfere with functioning
E: no other better explanation
Inattention A1 symptoms
a) often fails to give close attention to details
b) often has difficulty sustaining attention
c) often not seem to listen when spoken directly to
d) often does not follow through on instructions and fails to finish
e) Often difficulty organising
f) Often avoids, dislikes or reluctant to sustain mental effort
g) Often loses things
h) often easily distracted
i) often forgetful
hyperactivity/impulsivity symptoms
a) often fidgets
b) often leaves seat when being seated is expected
c) often runs about or climbs excessively
d) often difficulty playing quietly
e) Often “on the go”
f) Often talks excessively
g) Often blurts out
h) Often difficulty waiting
i) often interrupts or intrudes
Type of ADHD
combined presentation ADHD-C: A1 and A2
predominantly inattentive presentation ADHD-PI: A1 but no A2 for past 6 months
predominately hyperactive-impulsive presentation (ADHD-HI): A2 but no A1 for past 6 months
Conduct disorder (CD)
A. a repetitive and persistent pattern of behaviour in which the basic rights of others or major age-appropriate societal norms or rules are violated, as manifested by the presence of three (or more) of the following 15 criteria in the past 12 months for any category
aggression to ppl and animals
destruction of property
deceitfulness or theft
serious violation of rules
B. causes clinically significant impairment in social/academic/occupation
C. if 18 or <, and not met for antisocial personality disorder
aggression to ppl or animals
often bullies, threaten or intimidate others
often intiate physical fights
has used a weapon that can cause serious harm to others
has been physically cruel to ppl
has been physically cruel to animals
has stolen while confronting victim
has forced someone into sexual acitvity
Destruction of property
has enageged in fire-setting to cause serious damage
has destroyed others property on purpose
Deceitfulness or theft
has broken into someone’s house, cat or building
often lies to obtain goods
has stolen items of non-trivial value without confronting victim
serious violations of rules
often stays out at night even if not allowed (before 13 yrs old)
has run away from home overnight at least twice
is often truant from school before age 13
Specify if: conduct disorder
with limited prosocial emotions
lack of remorse
callous - lack of empathy
unconcerned about performance
shallow or deficient affect
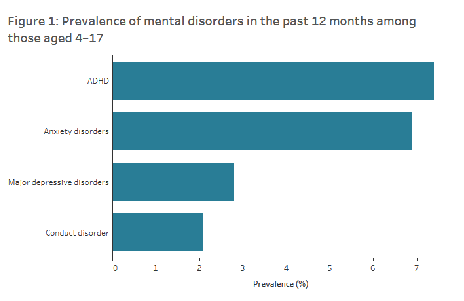
Prevalence and course
ADHD most common in children and adolescents
7.4% of all children in AUS have ADHD
most common in boys 12.9% of boys, 5.6% of girls
average 4:1 in children and adolescents. 6:1 adults
maybe because ADHD is different presenting in girls than boys
5.1% diagnosied with ODD*; 2.1% with CD**
higher in males than females
Course:
ADHD hyperactivity declines in adolescence
ADHD persists to adulthood 50-60%
ODD onset usually 2-3 years, CD late childhood or early adolescence
half of children with ODD or CD continue in adulthood
Aetiology of externalising disorders
genetic risk
temperamental risk
neurobiological risk
parenting factors
psychological factors
peers, neighbourhoods and media
Treatment of ADHD
preschool: 4-5 years
First-line treatment = behavioural interventions
One prescribes stimulants if no significant improvements and moderate to severe impairment (short-acting)
Primary school 6-11 years
First-line treatment = approved medication and or behavioural interventions - preferably both, stimulant tried first
adolescence 12-18 years
first-line treatment= approved medication
may include behavioural interventions
stimulants and non stimulants ADHD
psychostimulant e.g., ritalin:
increase norepinephrine and dopamine
side effects: decrease appetite, increased heart rate, sleep, motor tics
non-stimulants:
SSRI - selective serotonin reuptake (antidepressant)
SNRI - selective norepinephrine reuptake inhibitor
alpha-agonists
increase serotonin levels in brain
Behavioural interventions ADHD
parent education and support - most successful
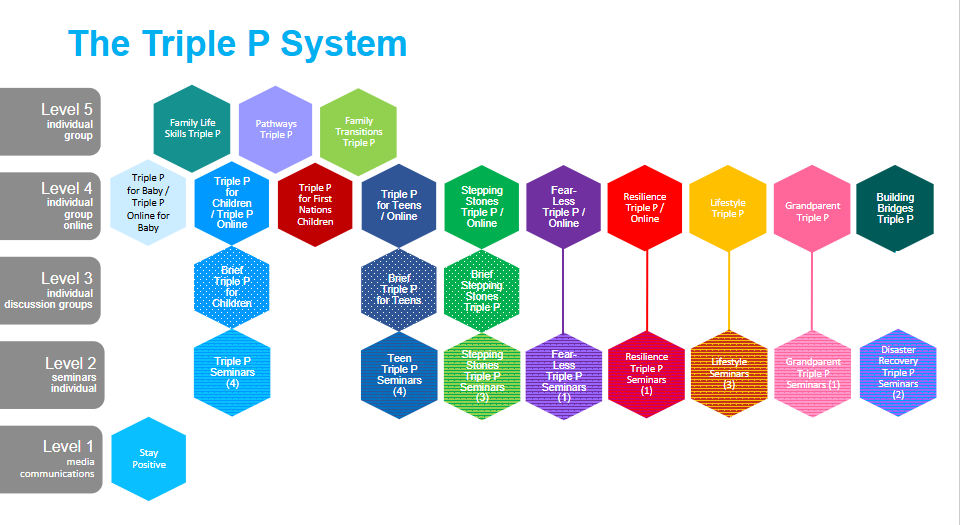
triple P - positive parenting program
strategies to strengthen relationship, communication etc
classroom accommodations
organisational supports
Personal coping skills ADHD
learn to compensate for executive function deficits
make mental info physical to compensate for lack of working memory (cues, to do lists)
make time physical eg clock
break up lengthy tasks
make motivation external - immediate reinforcement/consequence
make problem solving manual eg math tasks
refill self-regulation (i can do this, relax, meditate)
Treatment of ODD/CD
evidence-based parenting support e.g., triple P, PCIT, incredible years
individual skills development
multisystemic therapy
residential programs
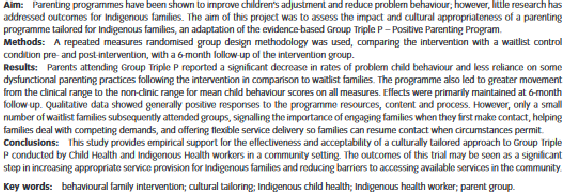
the triple P program
Pilot RCT
decrease in child behaviour concerns
improved parenting and adjustment (depression and stress)
good consumer satisfaction
reduction in barriers to mainstream services-
→ local health workers needed support
National think tank
tailored training to increase confidence e.g., more time, less texts
pre-accreditation workshops
dealing with logistical barriers
workplace support e.g., manager briefings
peer networking
clinical and cultural supervision
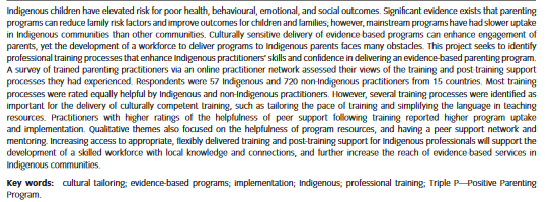
Practitioner support evaluation
peer networking and coaching
positive family outcomes
supportive coaching led to program sustainment 3 years later
→ first nations implementation consultants
→ first indigenous trainer
Remote community trial
38 local workers trained
positive training outcomes (knowledge, confidence)
positive family outcomes (child adjustment, parenting, self-efficacy, parental adjustment
worker and parent empowerment
community partnership: cherbourg positive parenting collaborative
tailoring:
community survey re parenting concerns and service needs
project scope developed
localised adaptations
results:
child adjustment - significant decrease in disruptive behaviours
parenting - significant decrease in inconsistent parenting and coercive parenting
parental adjustment - significant increase in parent self-efficacy
Internalising disorders
defines depressive and anxiety disorders same for children as adults
depressive symptoms
depression in children/adolescents often comorbid with both externalising problems and anxiety
depressed mood → may show as irritability
children’s fears and anxiety
often identity their anxiety but they are more aware of their fears
consider age-appropriate fears (distress, duration and interference)
DSM-5-TR Internalising disorder
depressive symptoms: 5 or < during the same 2 week period
depressed mood (irritability)
diminished interest or pleasure - in typically satisfying activities
significant weight loss or gain
insomnia or hypersomnia
psychomotor agitation or retardation
fatigue
feelings of worthlessness or excessive/inappropriate guilt
diminished ability to concentrate/indecisiveness
recurrent thoughts of death
separation anxiety disorder and selective mutism
developmentally inappropriate and excessive fear or anxiety concerning separation from home for 4+ weeks
distress when anticipating or experiencing separations
worry about losing an attachment figure
worry about experienced untoward events (getting lost, being kidnapped)
refusal to go out or sleep away from home without attachment figure
fear or reluctance about being alone
nightmares with separation themes
selective mutism
consistent failure to speak in certain social situations (when expected to)
speak to small number of people
prevalence and course
among AUS 1-17 years old:
3.2% diagnosed with MDD (higher for 12-17 years old 5%)
6.9% diagnosed with anxiety disorders (separation anxiety most common 4.3% selective mutism rate ,1%)
similar rates for male and female until age 12
higher in female 12-17
course:
some internalising problems persist into adulthood
linked to relationship difficulties, other anxiety disorders and mental health problems
functional impairment in social and personal life
childhood depression predicts 6-fold increase suicide in young adults
aetiology of internalising disorders
biological factors:
few behavioural genetic studies have been conducted
some indication to heritability
social factors
experience of life stress, loss or trauma
attachment issues
parental overprotectiveness
maltreatment
psychological factors
emotion regulation
rumination predicts future depression
caretaking children of depressed parents
unable to make depressed parents happy
feel guilty and responsible
programs may be able to prevent this
treatment of internalising disorders
depression:
individual psychotherapy
CBT
Family therapy
antidepressant medication not as effective as with adults
anxiety
child focussed CBT = gold standard
family therapy / child + parent interventions e.g., fear-less triple P
medication: selective serotonin reuptake inhibitors SSRIs most common
CBT components: psychoeducation, emotion regulation etc