Case 2: Lan Chen - Depression
1/31
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
32 Terms
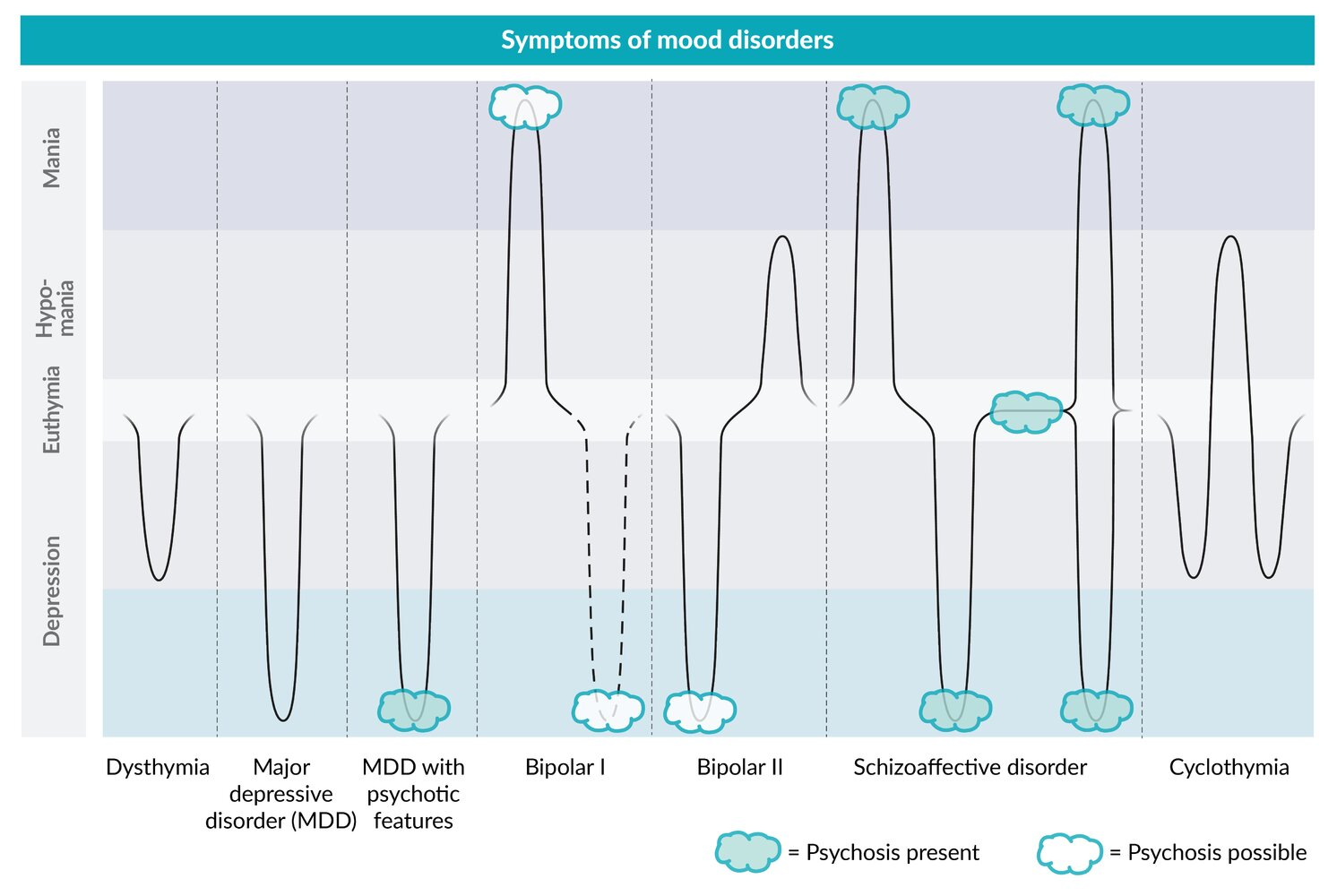
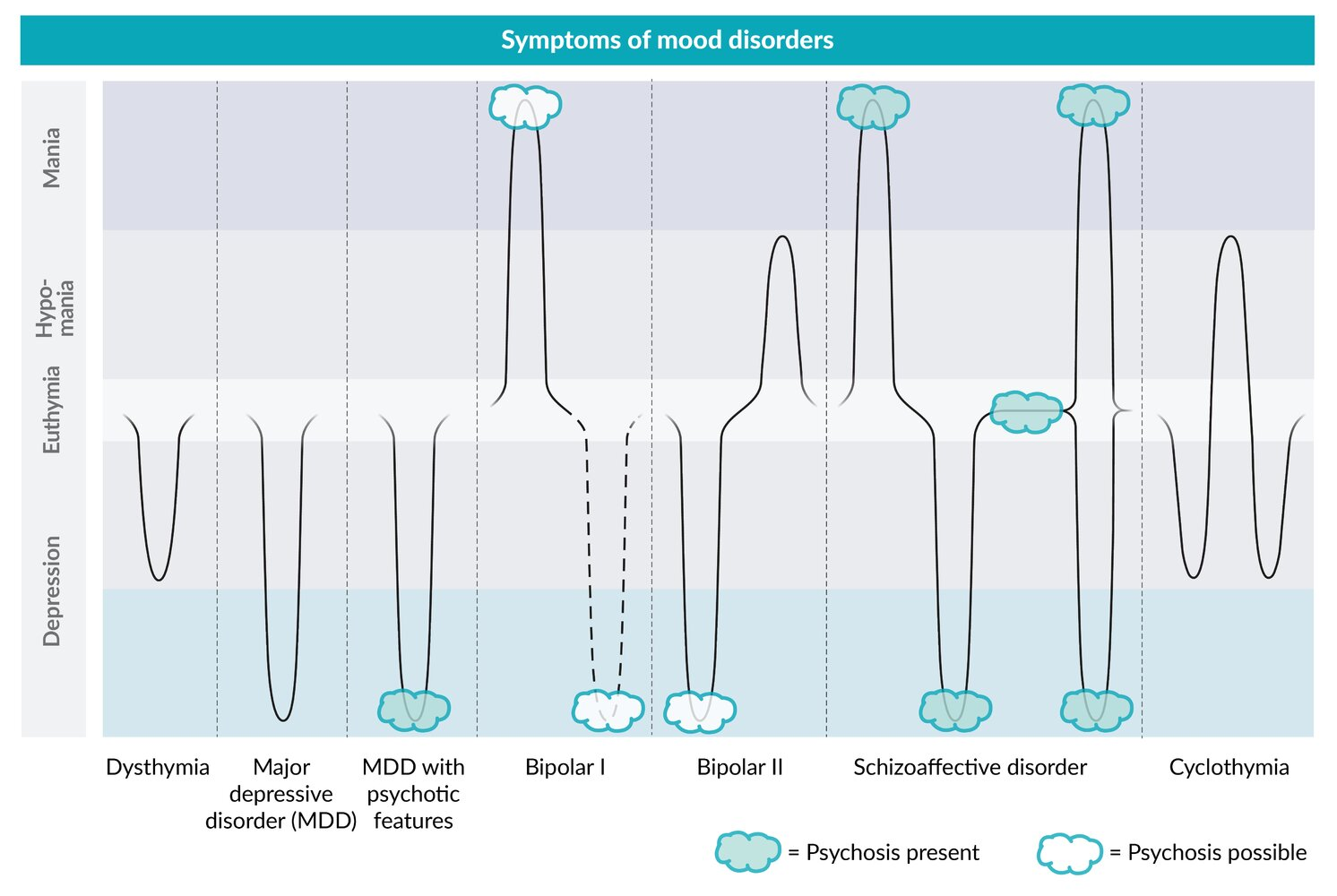
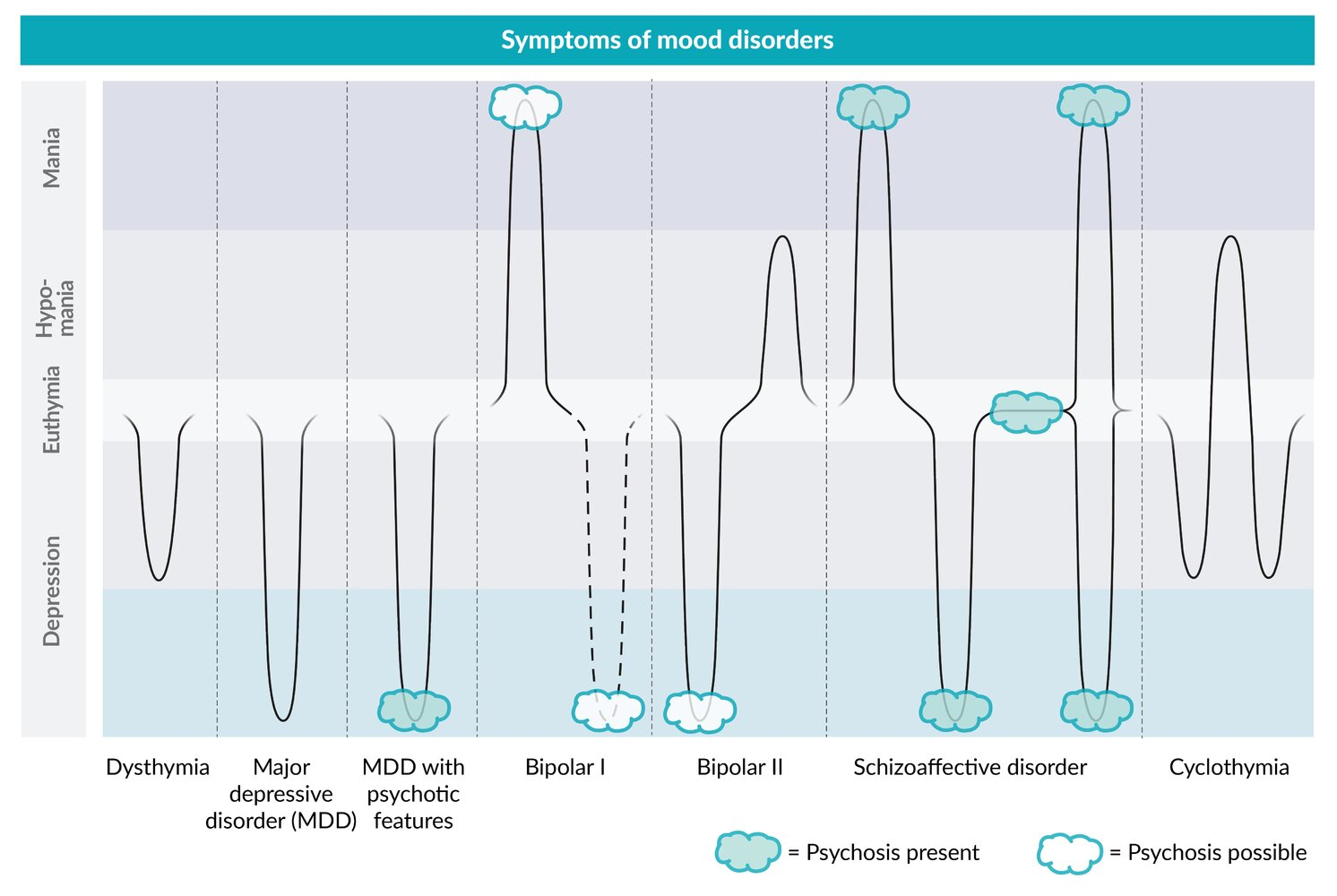
Depressive Disorders: Description
Conditions with symptoms of depression impairing ability to function
Depressive Disorders: Types
Major depressive disorder (MDD)
Premenstrual dysphoric disorder (PMDD)
Disruptive mood dysregulation disorder (DMDD)
Persistent depressive diosrder (Dysthymia)
MDD
Episodic mood disorder
Depressed mood + anhedonia ≥ 2 weeks
Atypical Features: Mood reactivity
Mood brightening in response to positive events
Psychotic Features: Congruent with mood
Seasonal Pattern: Episodes only in winter
PMDD
Affective + somatic symptoms during luteal phase
Resolve with menstruation
DMDD
Extreme irritability + recurrent anger outbursts
> 3/weeks for > 12 months
Dysthymia
Chronic depression ≥ 2 years
MDD: Description
Episodic mood disorder with depressed mood + anhedonia ≥ 2 weeks
MDD: Epidemiology
Risk factors…
Poor sleep hygiene
Sleep apnea → Intermittent cerebral hypoxia
Alcohol use
Childhood trauma
Family history
Women
MDD: Etiology
Biological
Psychological
Comorbidities
MDD: Biological Etiology
NT + hormone dysregulation
Genetics: Increased risk with 1º relatives with depression
MDD: Psychological Etiology
Increased stress/trauma
Stress-Diathesis Model: Combination of predisposition (diathesis) + external stressors = Mental/physical disorder development
Behavioural factors
Learned helplessness
MDD: Comorbidities Etiology
Neurodegenerative diseases
Chronic inflammatory disease
Psychiatric disorders
MDD: Pathophysiology
Monoamine hypothesis
HPA axis dysfunction
Cognitive model
MDD Pathophysiology: Monoamine Hypothesis
Monoamine NT deficiency (serotonin + tryptophan (precursor), norepinephrine, dopamine) = Impaired mood circuit regulation = Depressive symptoms
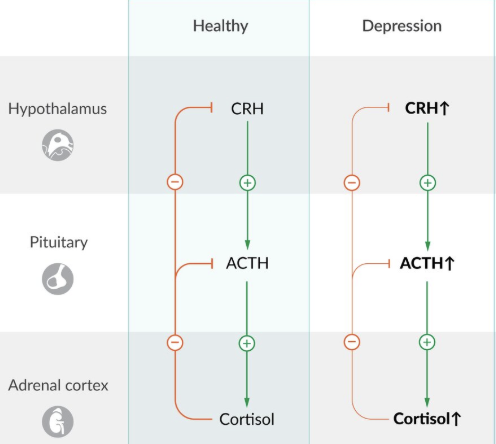
MDD Pathophysiology: HPA Axis Dysfunction
Stress = Activate HPA axis
Increase CRH (hypothalamus) → Increase ACTH (anterior pituitary) → Increase cortisol (adrenal cortex)
Negative feedback = Inhibit hypothalamus + anterior pituitary
Chronic stress = Decrease glucocorticoid receptors in hypothalamus + anterior pituitary (resistance) = No negative feedback from glucocorticoids (cortisol)
Continued CRH release = Cause…
Hippocampal damage = Mood dysregulation + cognitive dysfunction
Neuroinflammation
Frontolimbic disconnection
MDD Pathophysiology: Cognitive Model
Repeated negative experiences = Learned helplessness = Negative view of self (internal), world (external environment), and future (uncontrollable hopelessness)
MDD: Clinical Presentation
MSIGECAPS
M: Mood changes
Depressed mood
Irritability
S: Sleep disturbances
Insomnia
Hypersomnia
I: Interest
Anhedonia: Lack of interest in enjoyable activities
G: Guilt
Feelings of guilt, worthlessness, hopelessness
E: Energy
Low energy
Fatigue
C: Concentration (Pseudodementia)
Difficulty concentrating
Decreased cognition
Difficulty making decisions
A: Appetite
Changes in appetite/weight
P: Psychomotor
Agitation
Retardation
S: Suicide
Ideation/thoughts
MDD: Diagnostic Criteria
DSM-5
A-C: Episode
A-E: MDD
Criteria:
A: 5+ MSIGECAPS for ≥ 2 weeks
≥ 1 must be depressed mood or anhedonia
B: Cause…
Distress
Impaired function in work/school
C: Not caused by substances/organic disease
D: Not caused by schizoaffective/psychotic disorder
E: No mania/hypomania episodes
MDD: Screening
Pt health questionnaire-2 (PHQ-2)
Assess depressed mood + anhedonia
Suicide risk
MDD: Investigations
Physical exam
Lab tests
TFTs
Serum + urine toxicology
HIV testing
Neuroimaging
Cognitive testing
Polysomnography: Not routine
Sleep study assessing sleep hygiene
R/O sleep disturbances
MDD: Treatment/Management
Nonpharmacological
Pharmacological
MDD Management: Nonpharmacological
Lifestyle modifications
Sleep hygiene
Decrease substance use
Stress reduction + mindfulness
Increase social support
Regular exercise
Improve nutrition
Psychotherapy
CBT:
Mild: First-line
Moderate-Severe: Combine with antidepressants
MDD Management: Pharmacological
Antidepressants
≥ 4 weeks for effects
Antidepressants
Selective serotonin reuptake inhibitors (SSRIs)
Serotonin norepinephrine reuptake inhibitors (SNRIs)
Atypical
Tricyclic antidepressants (TCAs)
Monoamine oxidase inhibitors (MAOIs)
Antidepressants: SSRIs
Ex: Fluoxetine, sertraline, citalopram
MOA: Inhibit serotonin reuptake
Indications: First-line
Adverse Effects:
Headache
GI symptoms
Activating effects
Agitation
Anxiety
Insomnia
Sexual dysfunction
SIADH
Serotonin syndrome (SS)
Neuromuscular excitability → Hyperthermia, autonomic dysfunction, altered mental status
Antidepressants: SNRIs
Ex: Venlafazine, duloxetine
MOA: Inhibit serotonin + norepinephrine reuptake
Indications: Second-line
Adverse Effects:
Increase BP
Increase cholesterol + TAG
Sleep disturbances
SS
Antidepressants: Atypical
Bupropion
Mirtazapine
Atypical Antidepressant: Bupropion
MOA: Decrease dopamine + norepinephrine reuptake
Indications:
Seasonal depression
Weight concerns + sexual dysfunction
Adverse Effects:
Tachycardia + palpitations
Weight loss
Decrease seizure threshold
NOT for ED pt
SS
Atypical Antidepressant: Mirtazapine
MOA:
A2-adrenergic antagonist = Increase serotonin + norepinephrine release
5-HT1/3 receptor antagonist = Increase serotonin effects on 5-HT1
H1 antagonists
Indications: Underweight + insomnia
Adverse Effects:
Increase appetite + weight
Sedation
Increase cholesterol + TAG
SS
Antidepressants: TCAs
Ex: Amitryptyline, nortriptyline
MOA: Inhibit serotonin + norepinephrine reuptake
Indications: Third/fourth-line
Adverse Effects:
Orthostatic hypotension
Cardiotoxicity
Tachycardia
Arrhythmias
Prolonged QT interval → Torsades de pointes
Wide QRS
Anticholinergic symptoms
Confusion + hallucinations
Constipation
Urinary retention
Dry skin
SS
Antidepressants: MAOIs
Ex: Selegiline, phenelzine
MOA: Inhibit MAO = Decrease epinephrine, norepinephrine, serotonin, dopamine breakdown
Selegiline: Selective MAO-B inhibition = Decrease dopamine breakdown
Indications: Atypical MDD
Adverse Effects:
Sexual dysfunction
Orthostatic hypotension
Weight gain
+ Tyramine = HTN crisis
SS
MDD: Complications
SI
Cognitive deficits
Increased with severity
Decreased executive function, memory, attention, learning
CVD