Accommodation Basics - Diagnosis and Management of Common Ocular Conditions Spring 2026
1/94
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
95 Terms
Will accommodation affect most of the tests that optometrists perform?
yes
What is the definition of accommodation?
the eye's ability to bring objects located at different distances into focus by changing the shape of the lens
Is there a clinical simplification of accommodation?
yes
Accommodation from the spectacle plane used in the clinical simplification of accommodation
spectacle accommodation
What does spectacle accommodation ignore?
ignores differences in accommodative demand between correcting at the spectacle plane vs CL
Is spectacle accommodation the adequate way of thinking for a vast majority of clinical situations?
yes
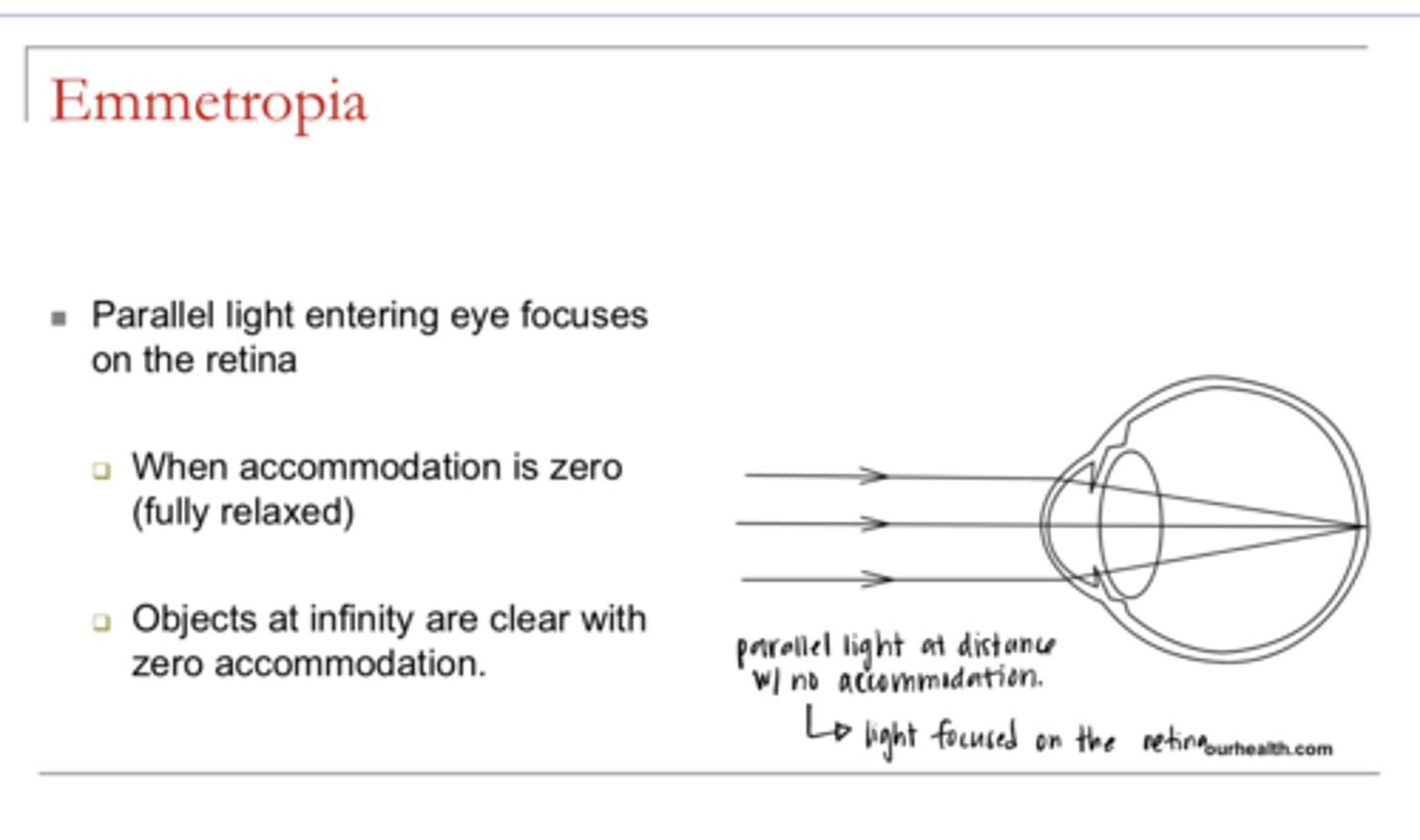
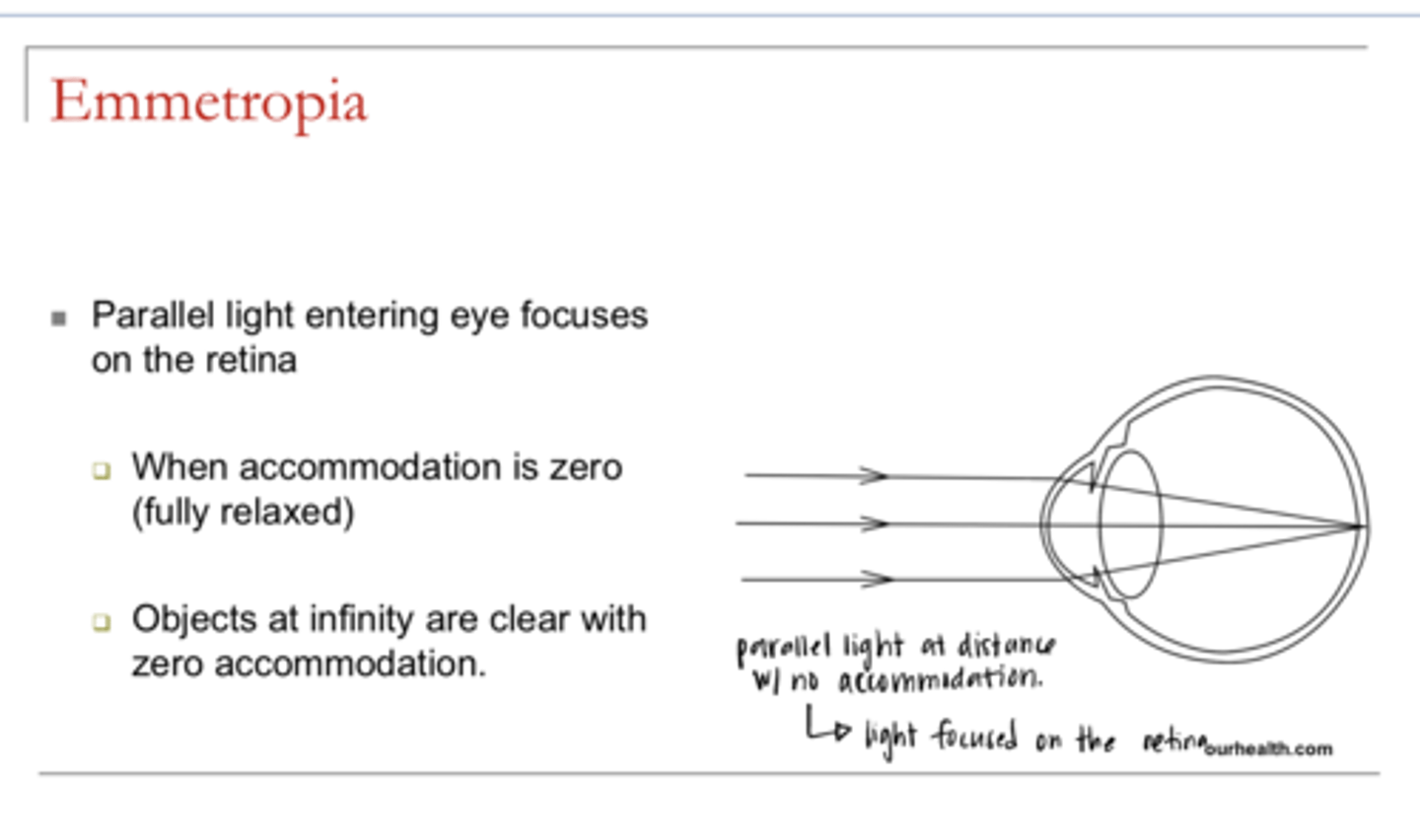
What is emmetropia?
parallel light entering eye focuses on the retina when there is zero accommodation in place
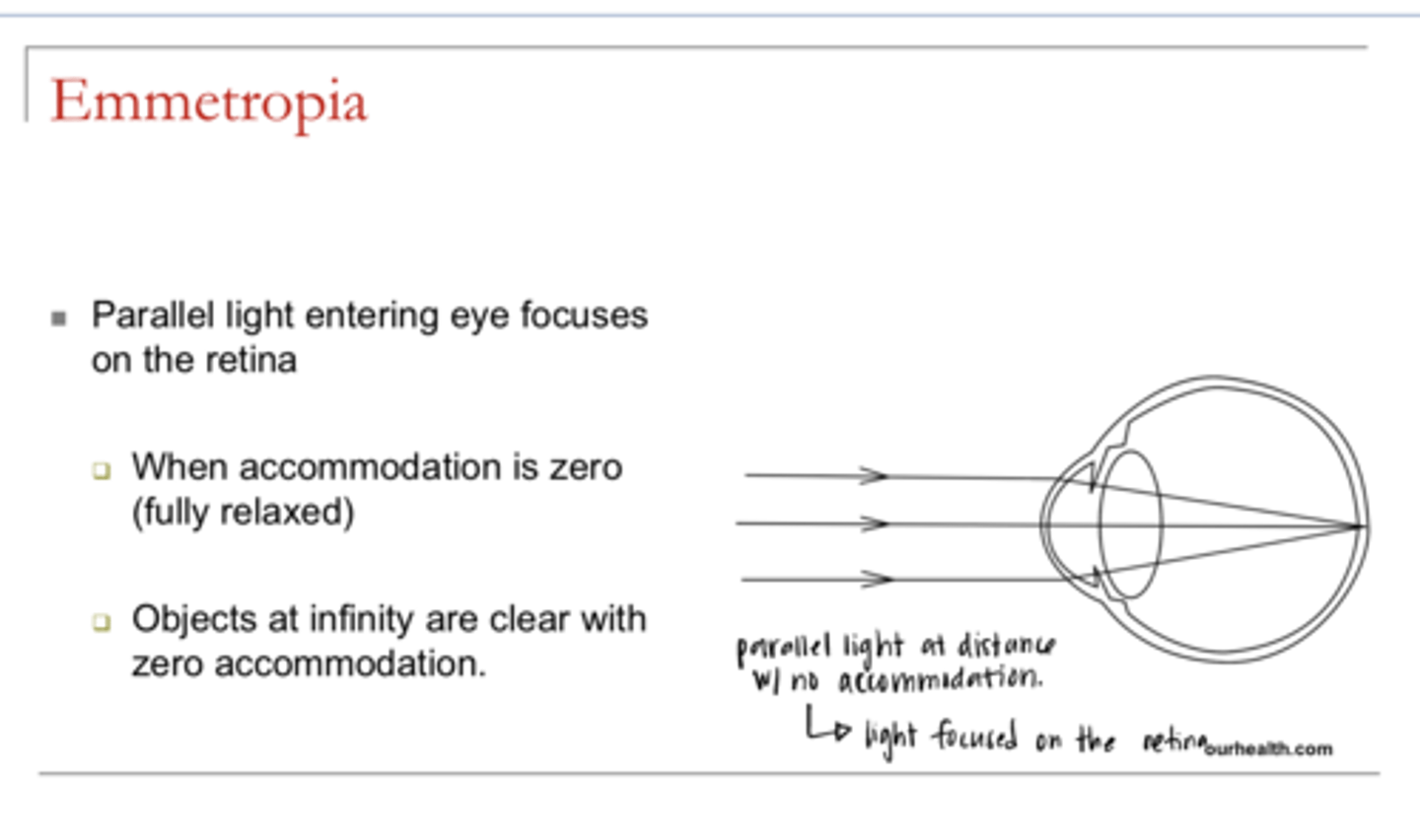
Do emmetropes have to accommodate to see clearly at distance?
no -- accommodation will be fully relaxed
True or False:
For emmetropes, objects at optical infinity are clear with zero accommodation in place
true
What is the role of accommodation?
Adds more plus power to the eye and focuses nearer objects
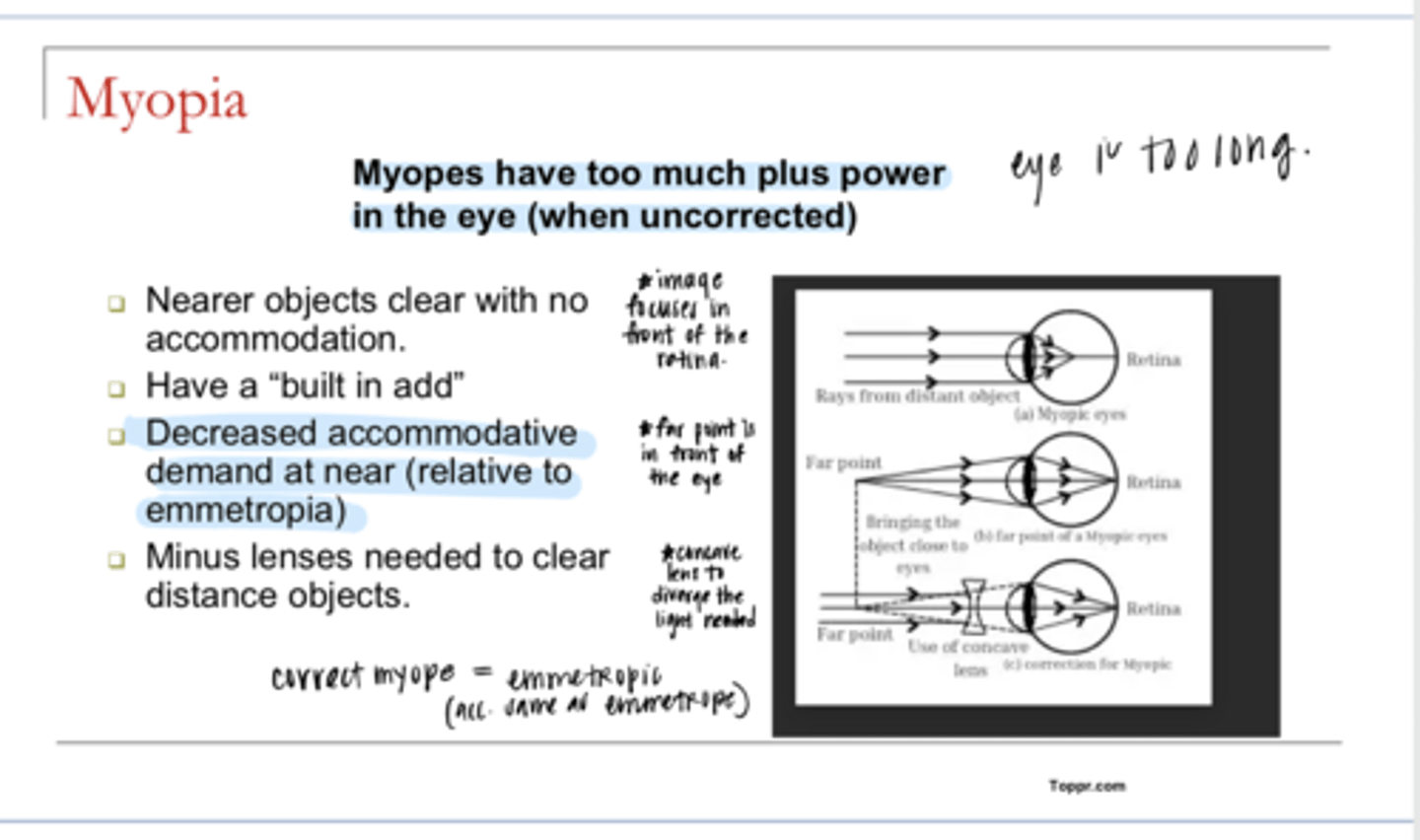
Myopes have too much what?
plus power in the eye (when uncorrected) -- eye is too long
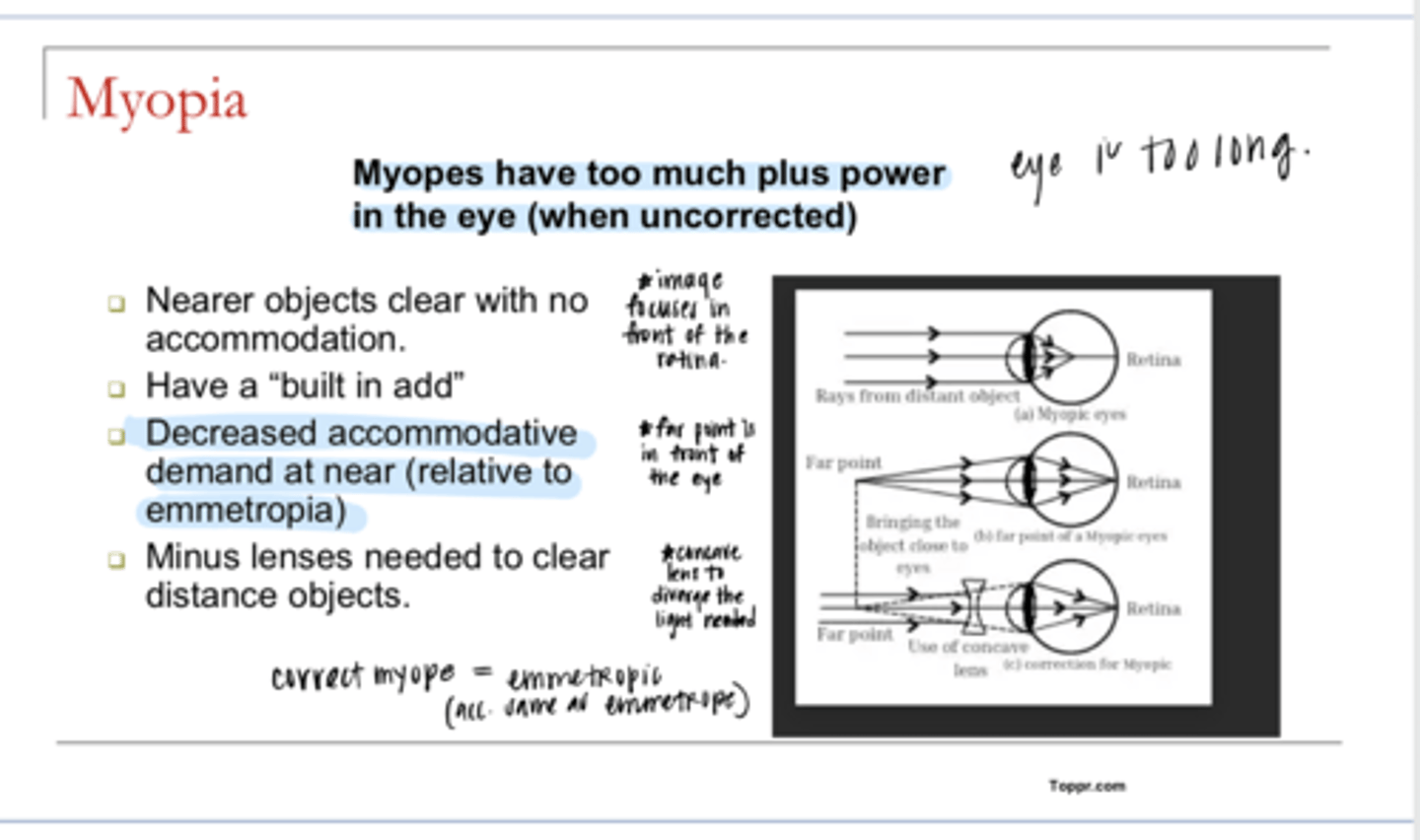
Where is the far point for a myope?
in front of the eye
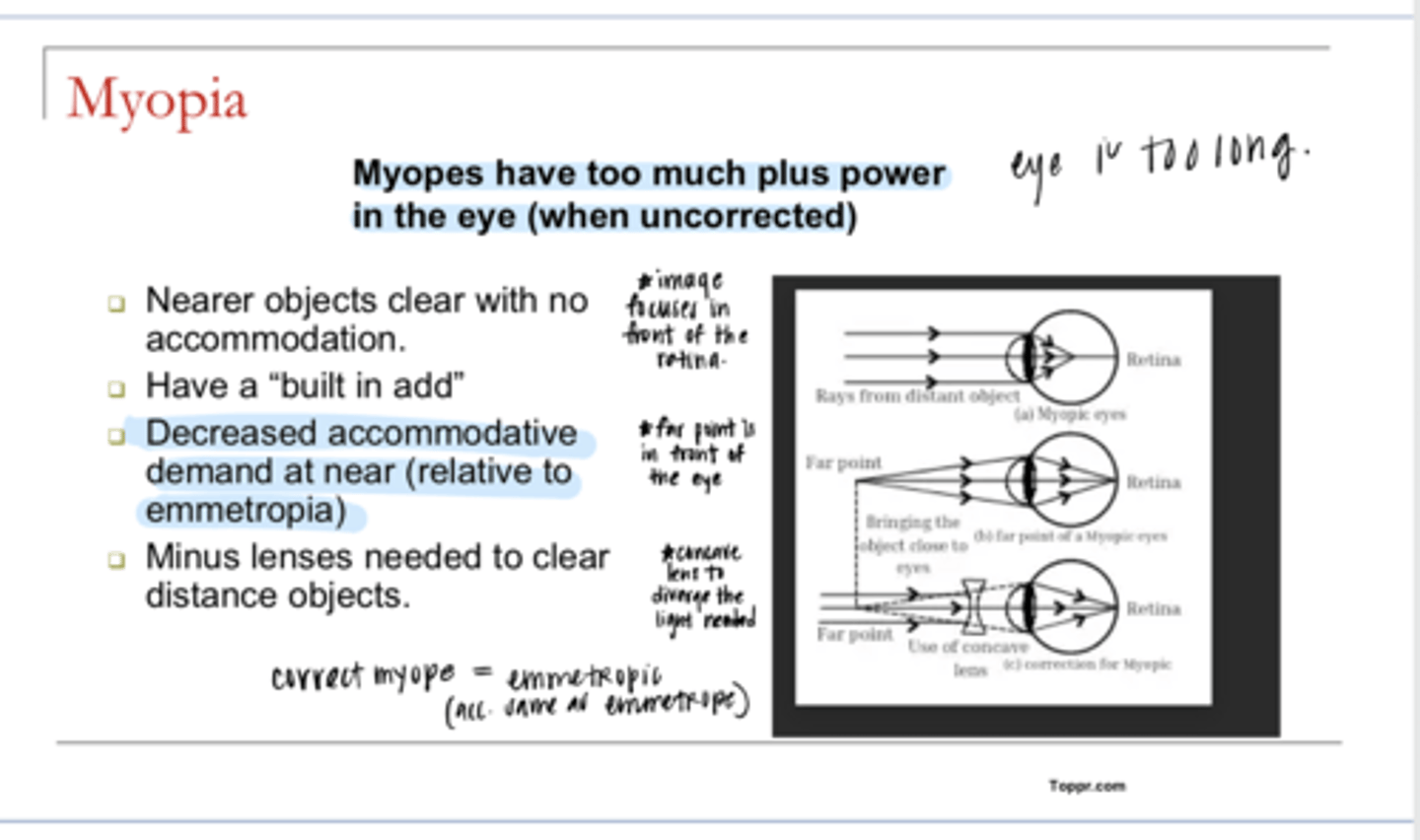
In a myope, which will be clearer with no accommodation?
Near or distant objects
near objects with no accommodation
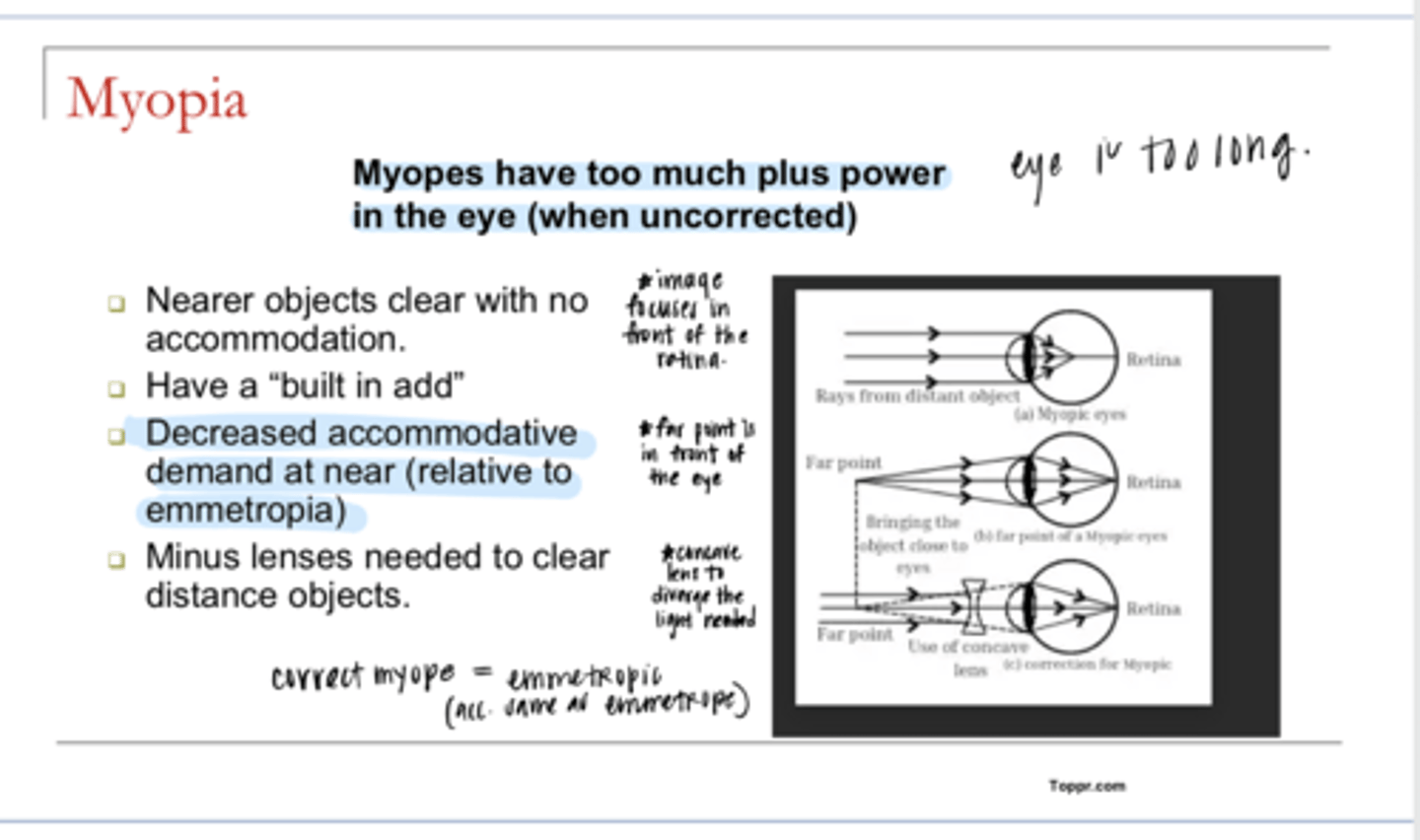
Myopes have what?
a built in add
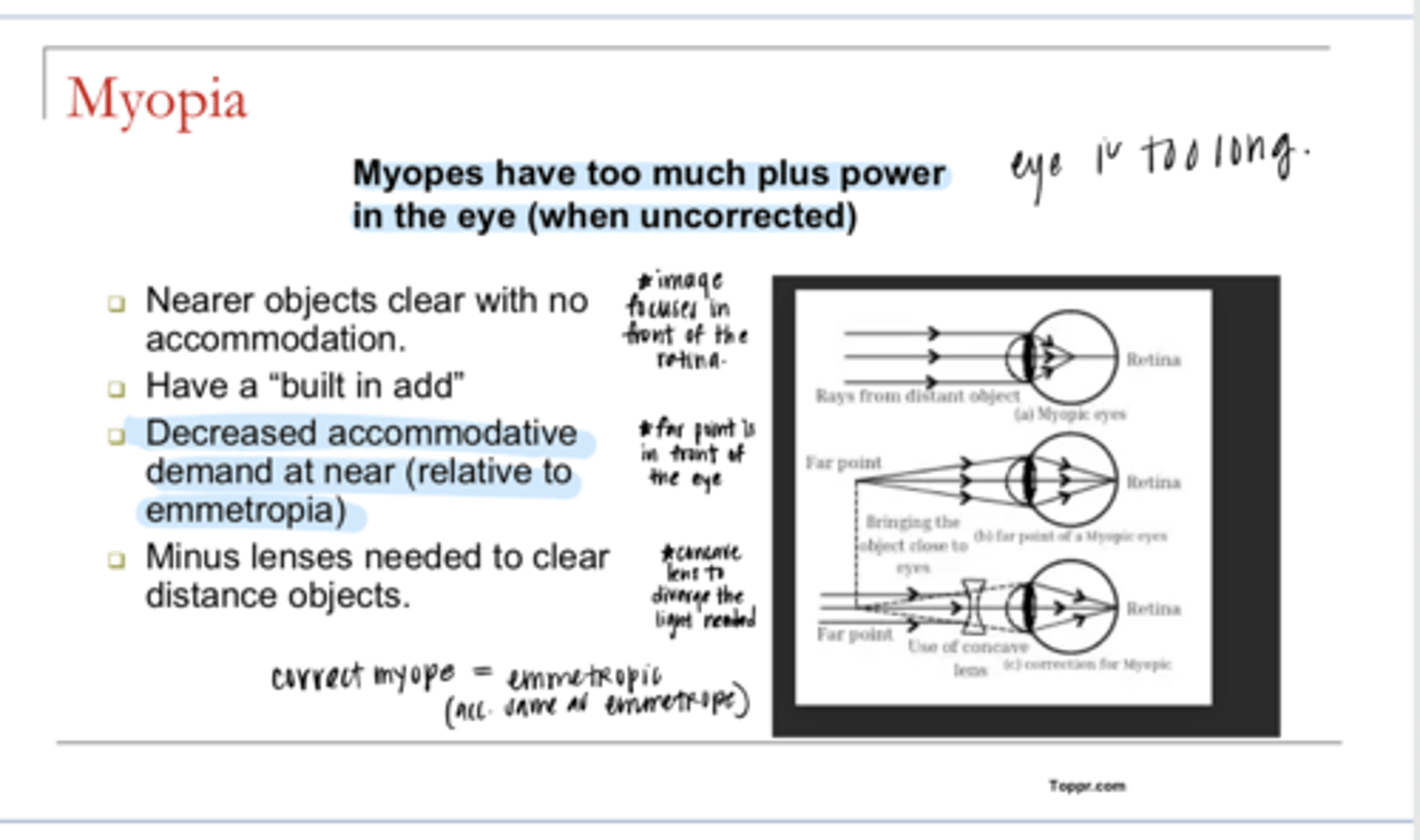
Myopes have a(n) (decreased/increased) accommodative demand at near relative to emmetropia?
decreased
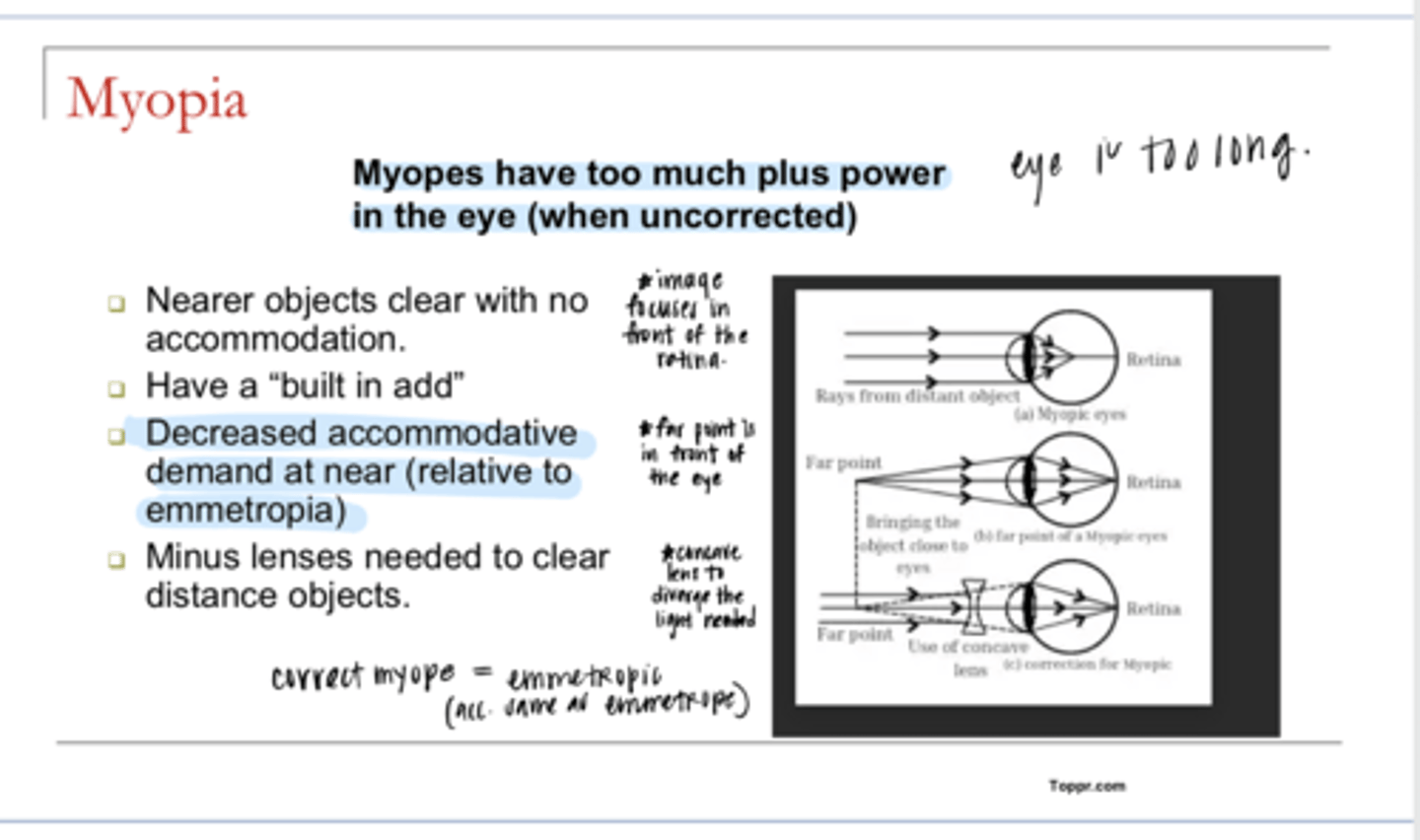
____ lenses are needed to clear distant objects for myopes
minus (concave) -- used to diverge light
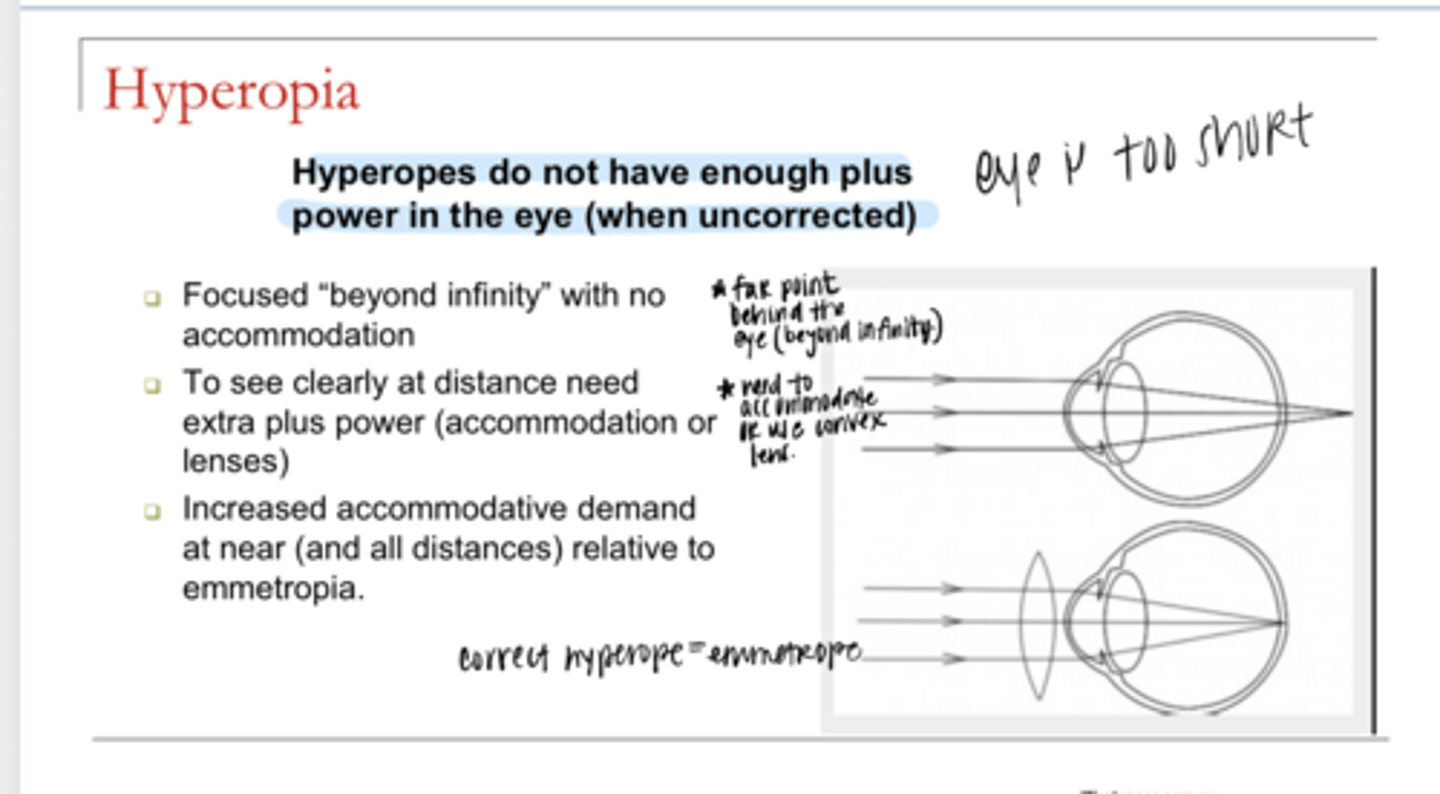
Hyperopes do not have enough what?
enough plus power in the eye (when uncorrected) -- eye is too short
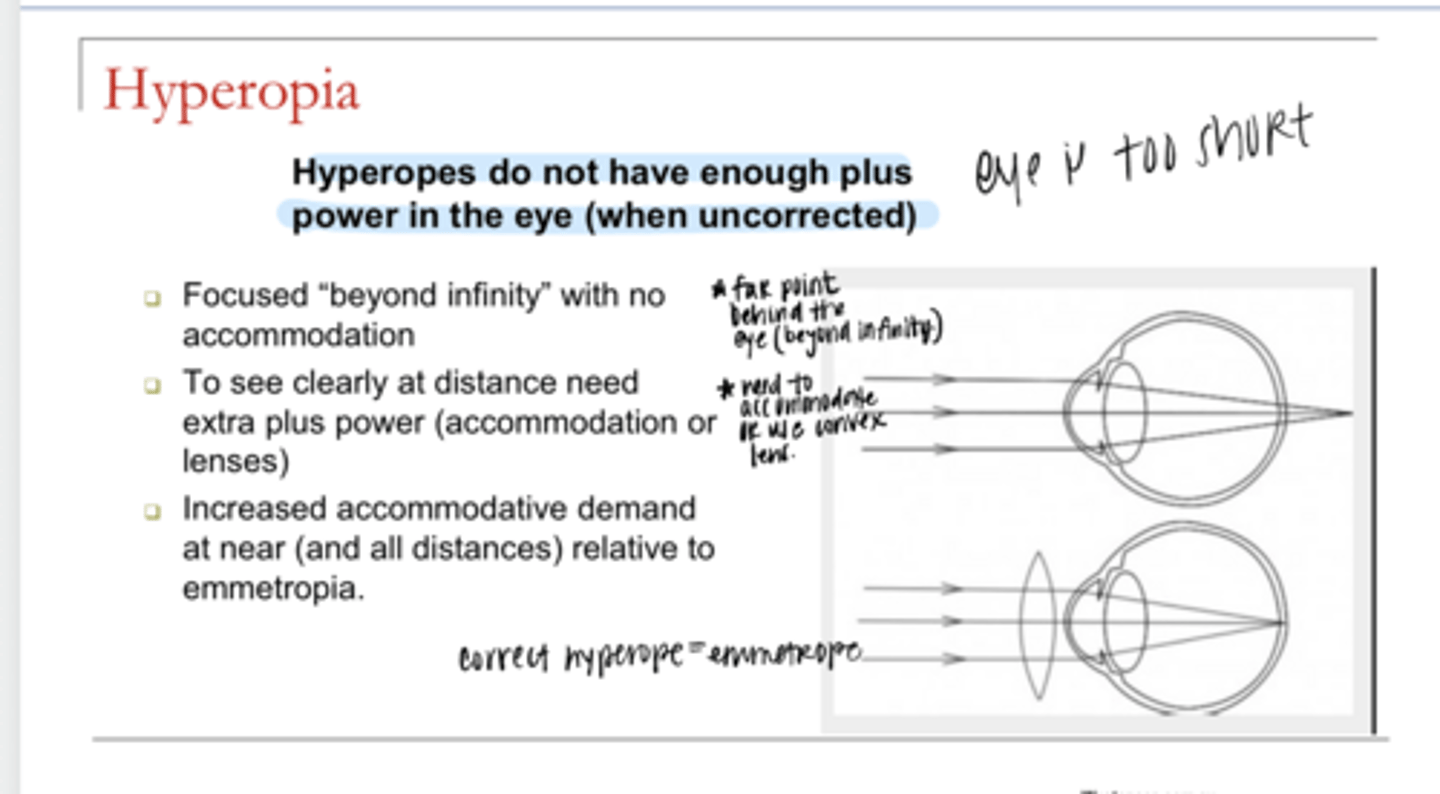
Where are hyperopes focused without correction?
beyond infinity (far point is behind the eye)
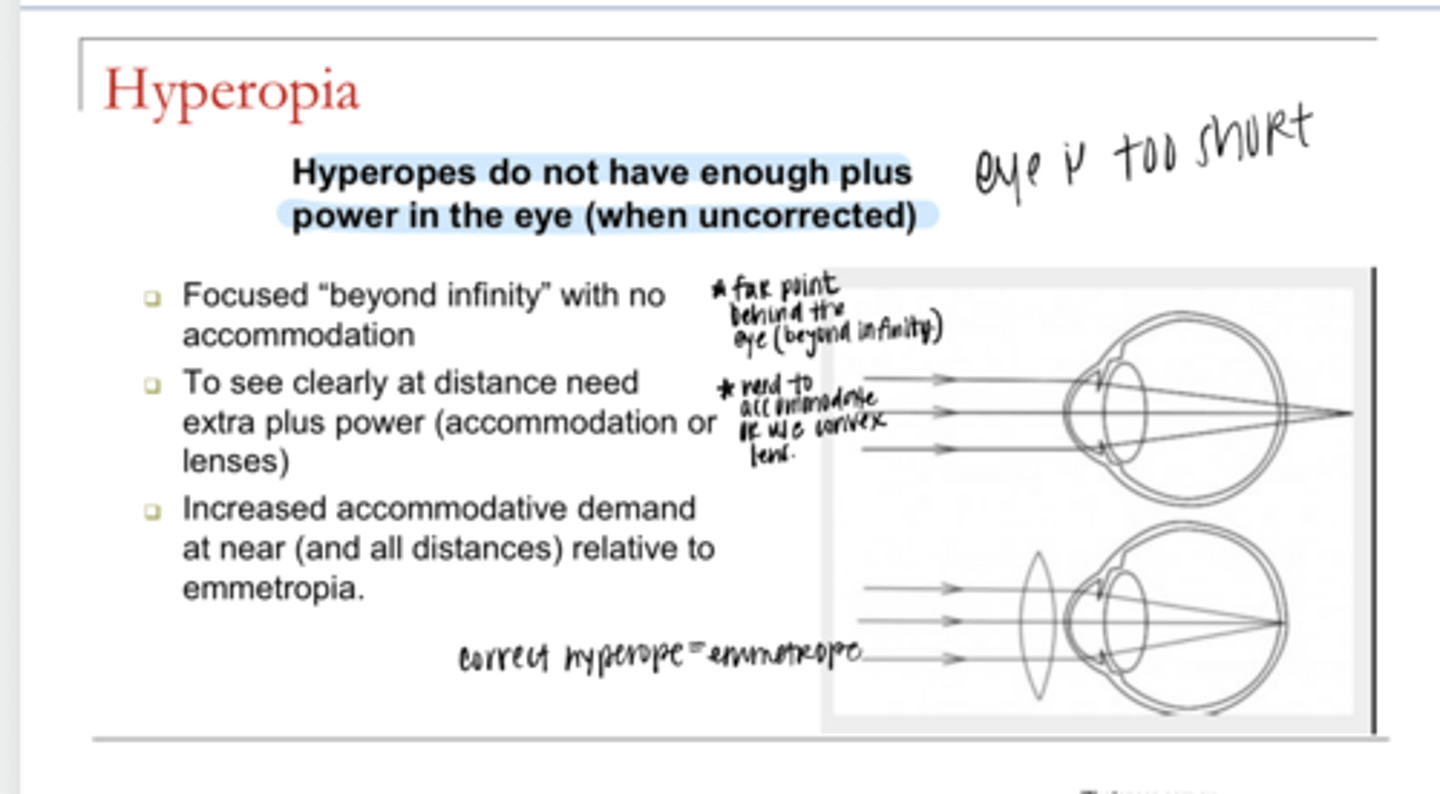
To see clearly at distance, what do hyperopes have to do?
they have to accommodate to see clearly at distance (they need extra plus power)
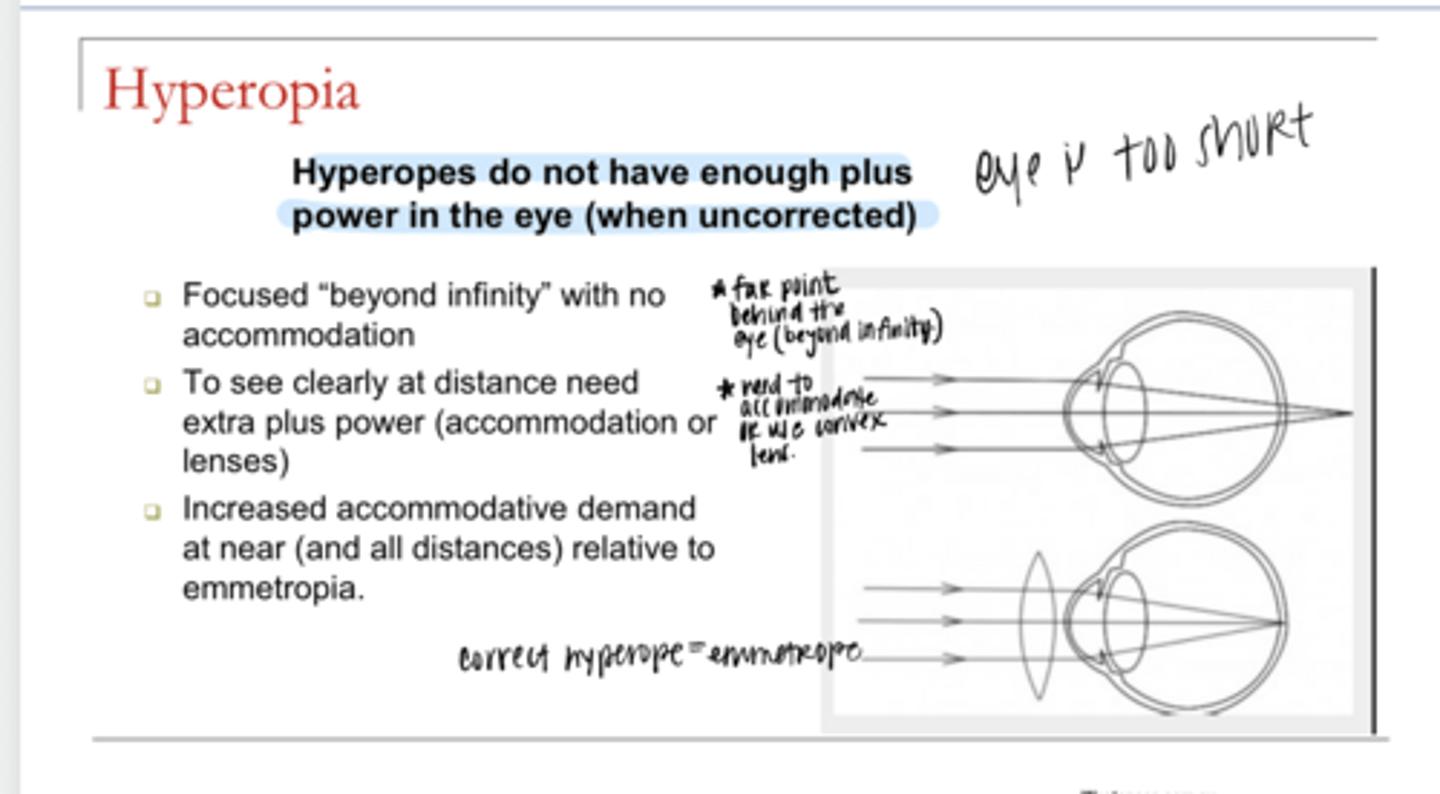
Hyperopes have a(n) (decreased/increased) accommodative demand at near relative to emmetropia?
increased
What does fully correcting ammetropes do?
puts them on an even playing field with emmetropes
Can accommodative demands be considered the same for a fully corrected ammetrope and emmetropes?
yes
What is the equation for accommodative demand?
Accommodative Demand = 1 / distance
What is accommodative demand measured in?
diopters
What is the standard working distance for an adult?
40cm
What is the standard working distance for a child?
33cm
What is the standard accommodative demand for a far away target?
0
Is the equation for accommodative demand a generalization?
yes
Does the equation for accommodative demand describe the accommodative demand for an object for a given patient?
no
What needs to be factored into the accommodative demand equation in order for it to be more accurate?
1) Refractive error
2) Refractive correction
What is the equation for TRUE Accommodative Demand? (TAD)
TAD = AD + RE - lens
What is the accommodative demand for an object at 25 cm for a 2D myope wearing -1.00 glasses?
TAD = AD + RE - lens
TAD = 1/0.25 + -2 - (-1)
TAD = 3
Being an undercorrected myope has a 1D built in add
What is a good way to think about accommodative demand clinically?
1) Type of RE relative to the correction
2) Lens power relative to the refractive error
If your patient is a fully corrected myope, what is the accommodative demand? (standard, increased or decreased)
standard
If your patient is an over-corrected myope, what is the accommodative demand? (standard, increased or decreased)
increased
If your patient is an under-corrected myope, what is the accommodative demand? (standard, increased or decreased)
decreased -- built in add present
If your patient is a fully corrected hyperope, what is the accommodative demand? (standard, increased or decreased)
standard
If your patient is an over-corrected hyperope, what is the accommodative demand? (standard, increased or decreased)
decreased (over plussed) -- built in add present
If your patient is an under-corrected hyperope, what is the accommodative demand? (standard, increased or decreased)
increased (under plussed)
EX: What is the accommodative demand at distance and near for a 2D myope wearing -1.00 glasses?
-Patient is -1.00D undercorrected
-Accommodative demand at distance: 0D
-Accommodative demand at near: 1.5D
EX: What is the accommodative demand at distance and near for a 4D hyperope wearing +2.00 glasses?
-Patient is +2.00D undercorrected
-Accommodative demand at distance: 2D
-Accommodative demand at near: 4.5D
What is the absolute limit to fully relaxing accommodation?
0 -- we cannot accommodate LESS than 0D
What is our goal when doing a refraction?
Find the least minus power for maximum VA. Or find the lens power that brings distance target into focus when all accommodation is relaxed.
True or False:
Sometimes the spec Rx that is given to a patient DOES NOT match the refraction
true
Why does the spec RX that is given to the patient sometimes NOT match the refraction?
-aniseikonia
-usually d/t accommodation
CLINICAL ASSUMPTION: Accommodative response will match the _______ when possible
accommodative demand
EXAMPLE: What is the accommodative response and amount of blur at distance and 40cm for an emmetrope wearing no Rx?
-Accommodative Response at Distance: 0
-Amount of Blur at Distance = Clear
-Accommodative Response at Near: +2.50
-Amount of Blur at Near = Clear
EXAMPLE: What is the accommodative response and amount of blur at distance and 40cm for a 2D hyperope wearing +2.00D glasses?
-Accommodative Response at Distance: 0
-Amount of Blur at Distance = Clear
-Accommodative Response at Near: +2.50
-Amount of Blur at Near = Clear
EXAMPLE: What is the accommodative response and amount of blur at distance and 40cm for a 1D hyperope wearing no RX?
-Accommodative Response at Distance: 1
-Amount of Blur at Distance = Clear
-Accommodative Response at Near: +3.50
-Amount of Blur at Near = Clear
EXAMPLE: What is the accommodative response and amount of blur at distance and 40cm for a 1D myope wearing -2.00 glasses?
-Accommodative Response at Distance: 1
-Amount of Blur at Distance = Clear
-Accommodative Response at Near: +3.50
-Amount of Blur at Near = Clear
EXAMPLE: What is the accommodative response and amount of blur at distance and 40cm for a 1D myope wearing no RX?
-Accommodative Response at Distance: 0
-Amount of Blur at Distance = 1D
-Accommodative Response at Near: 1.50
-Amount of Blur at Near = Clear
EXAMPLE: What is the accommodative response and amount of blur at distance and 40cm for a 3D myope wearing no RX?
-Accommodative Response at Distance: 0
-Amount of Blur at Distance = 3D
-Accommodative Response at Near: 0
-Amount of Blur at Near = 0.50D
EXAMPLE: What is the accommodative response and amount of blur at distance and 40cm for a 3D myope wearing -2.00 glasses?
-Accommodative Response at Distance: 0
-Amount of Blur at Distance = 1D
-Accommodative Response at Near: 1.5
-Amount of Blur at Near = Clear
EXAMPLE: What is the accommodative response and amount of blur at distance and 40cm for an emmetrope wearing +2.00 glasses?
-Accommodative Response at Distance: 0
-Amount of Blur at Distance = 2D
-Accommodative Response at Near: 0.50
-Amount of Blur at Near = Clear
EXAMPLE: What is the accommodative response and amount of blur at distance and 40cm for a +0.50 hyperope wearing -5.00 glasses?
-Accommodative Response at Distance: 5.5
-Amount of Blur at Distance = Clear
-Accommodative Response at Near: 8
-Amount of Blur at Near = Clear? Hard to sustain this
True or False:
Considering accommodation becomes more complicated when there is astigmatic blur. Why?
true -- the response will be more variable and may be target independent
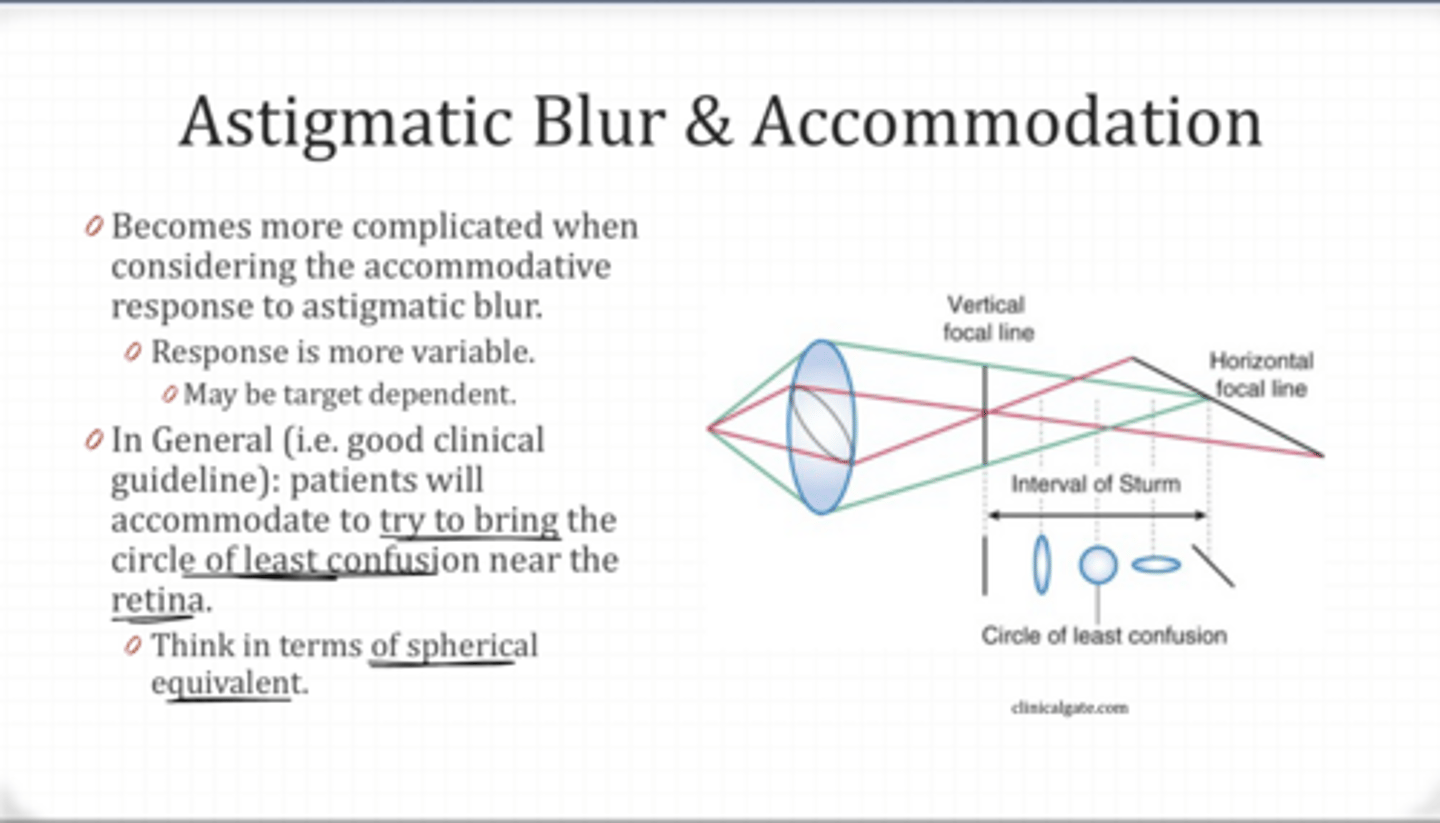
In general, patients will accommodate to try to do what?
in order to bring the circle of least confusion near the retina
When uncorrected, how much do you expect this patient to accommodate when looking in the distance? At 40cm?
+2.00-3.00x180
-SE = +0.50
-Accommodation at Distance: 0.50D
-Accommodation at Near: 3D
True or False:
Sometimes we do not fully correct hyperopes
true
If you wanted to cut the plus for this patient, what is the most that you would be willing to cut?
+2.00-3.00x180
-SE = +0.50
-Most you would be willing to cut is 0.50D of plus
What is the Spherical Equivalent?
+1.00-1.50x075
+0.25D
What is the Spherical Equivalent?
-1.25-1.00x004
-1.75D
What is the Spherical Equivalent?
-6.25-3.25x080
-7.88D
When is SE often used in clinic?
-Patient with increasing myopia
-Patient currently overminused
-Patient with anisometropia
-Patient with undercorrected hyperopia
How can a change in spec Rx be demonstrated?
-By holding a trial lens over the current gls
-Trial frame if large cyl power or axis
How much more plus is the Refraction than Current Rx?
Current: +1.00-1.00x180
Ref: +1.50-0.50x180
-SE Current: +0.50
-SE Ref: +1.25
-Ref is +0.75D more plus than the current rx
You want to demonstrate the SE change in refraction over your patient's current gls. What lens would you hold over the gls?
Current: -4.75-3.25x084
Ref: -5.00-3.75x087
-SE Current: -6.37
-SE Ref: -6.87
-Ref is -0.50 more minus than current rx
-Hold -0.50 lens in front of patients current gls to demo
How much do you expect this patient to accommodate when UNCORRECTED and viewing target at 40cm?
+1.00-2.00x180
-SE: 0
-Accommodation at near= 2.5D
How much do you expect this patient to accommodate when UNCORRECTED and viewing target at 40cm?
-1.00-4.00x180
-SE: -3
-Accommodation at near = 0
How much do you expect this patient to accommodate when UNCORRECTED and viewing target at 40cm?
+2.00-1.25x180
-SE: 1.375
-Accommodation at near = 3.875
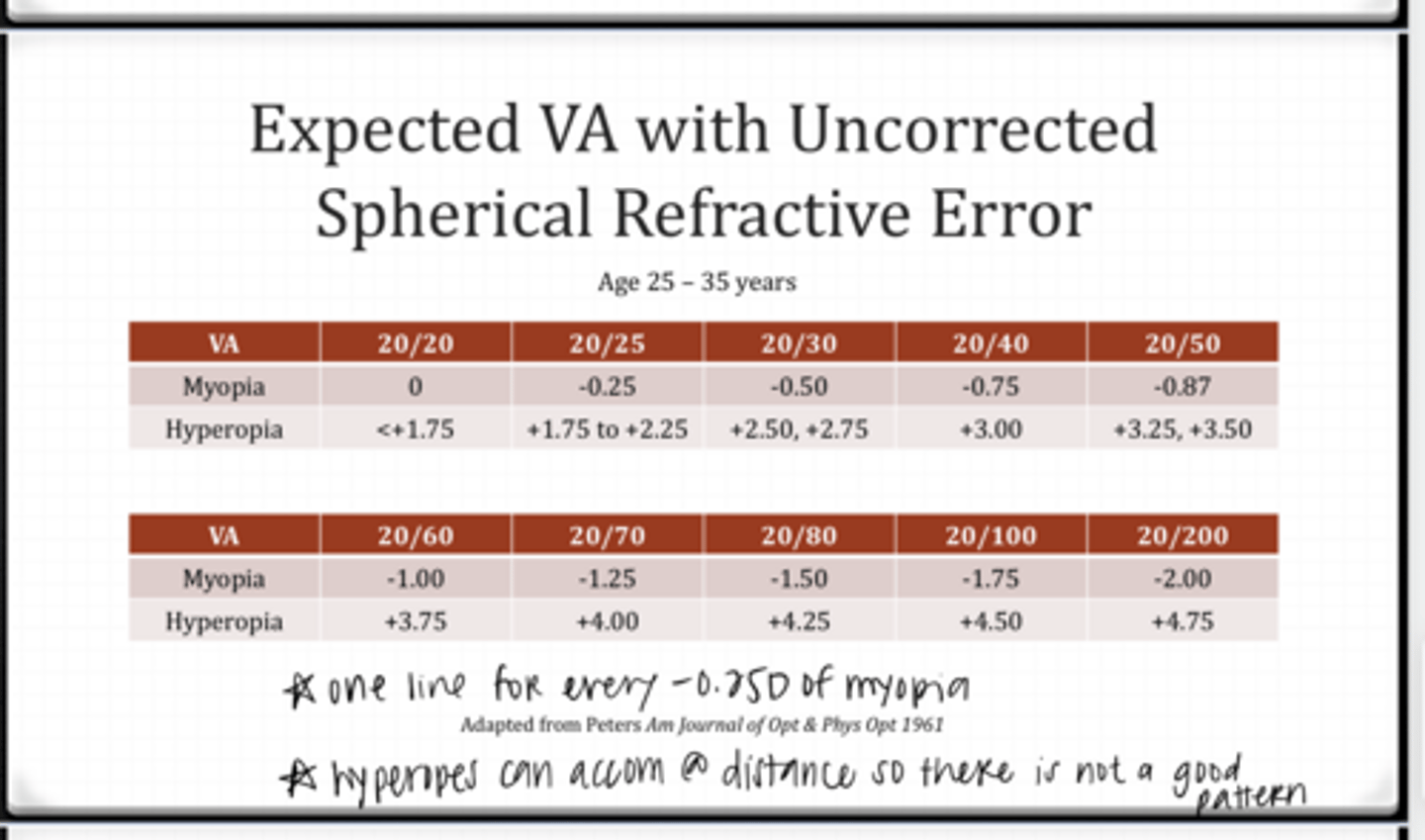
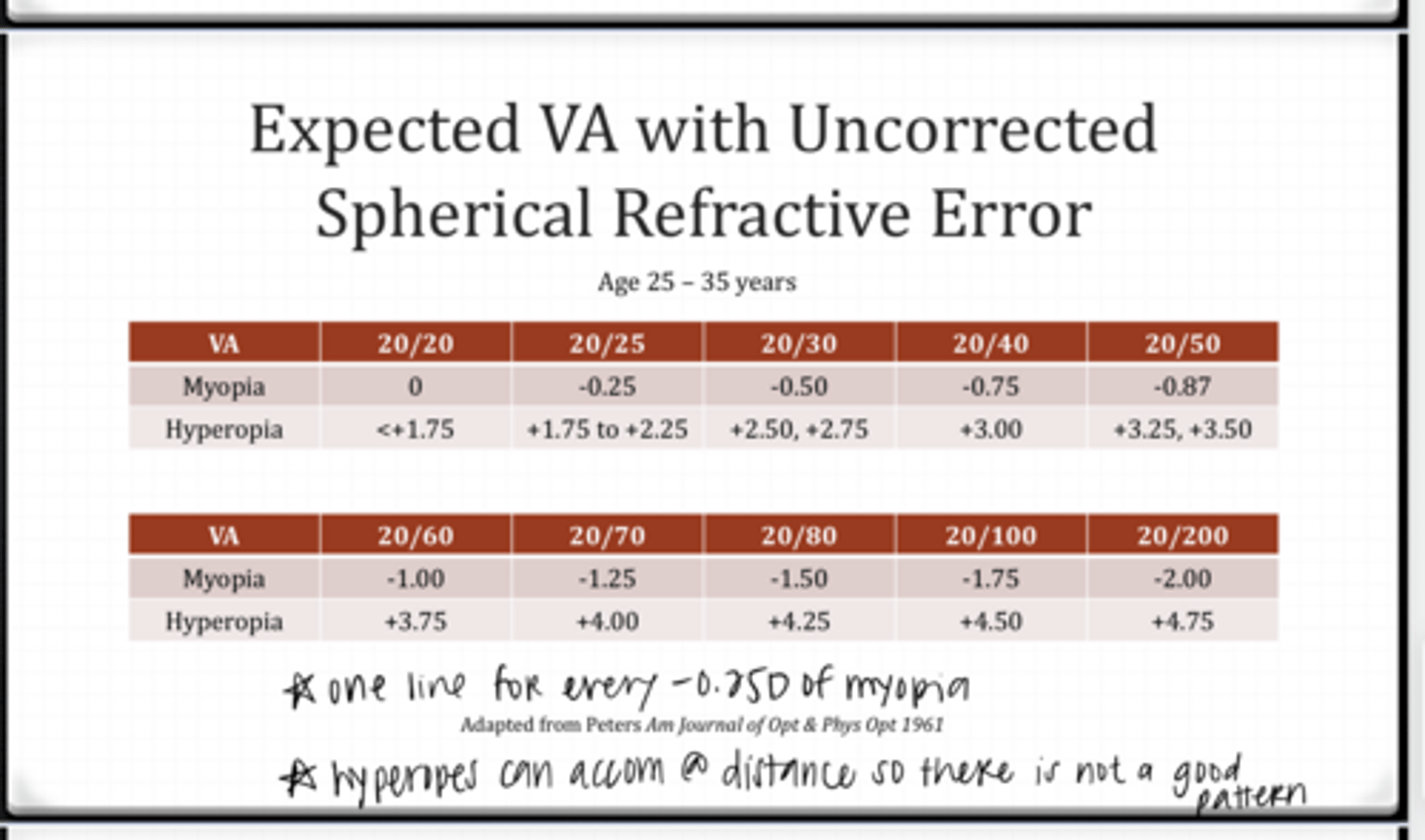
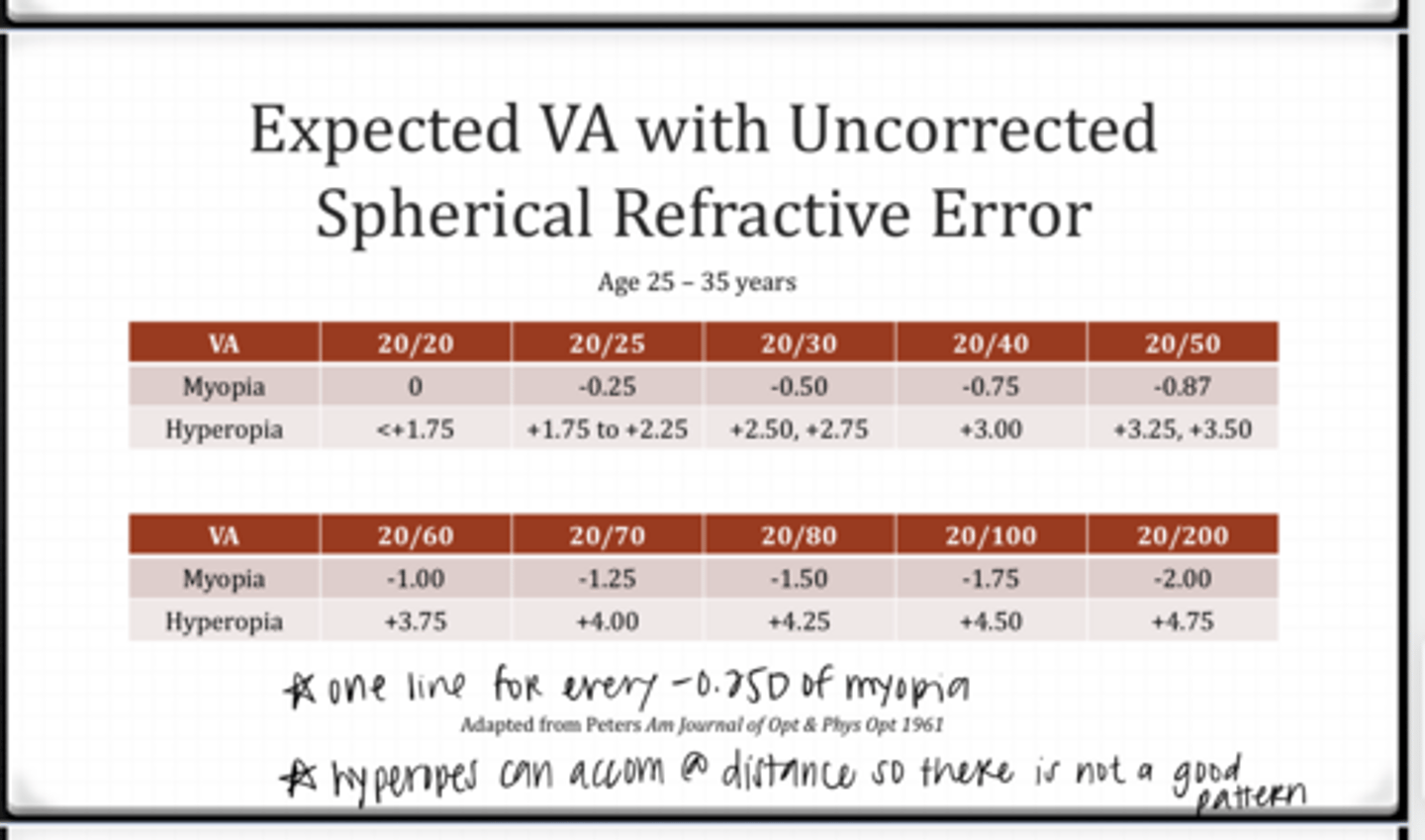
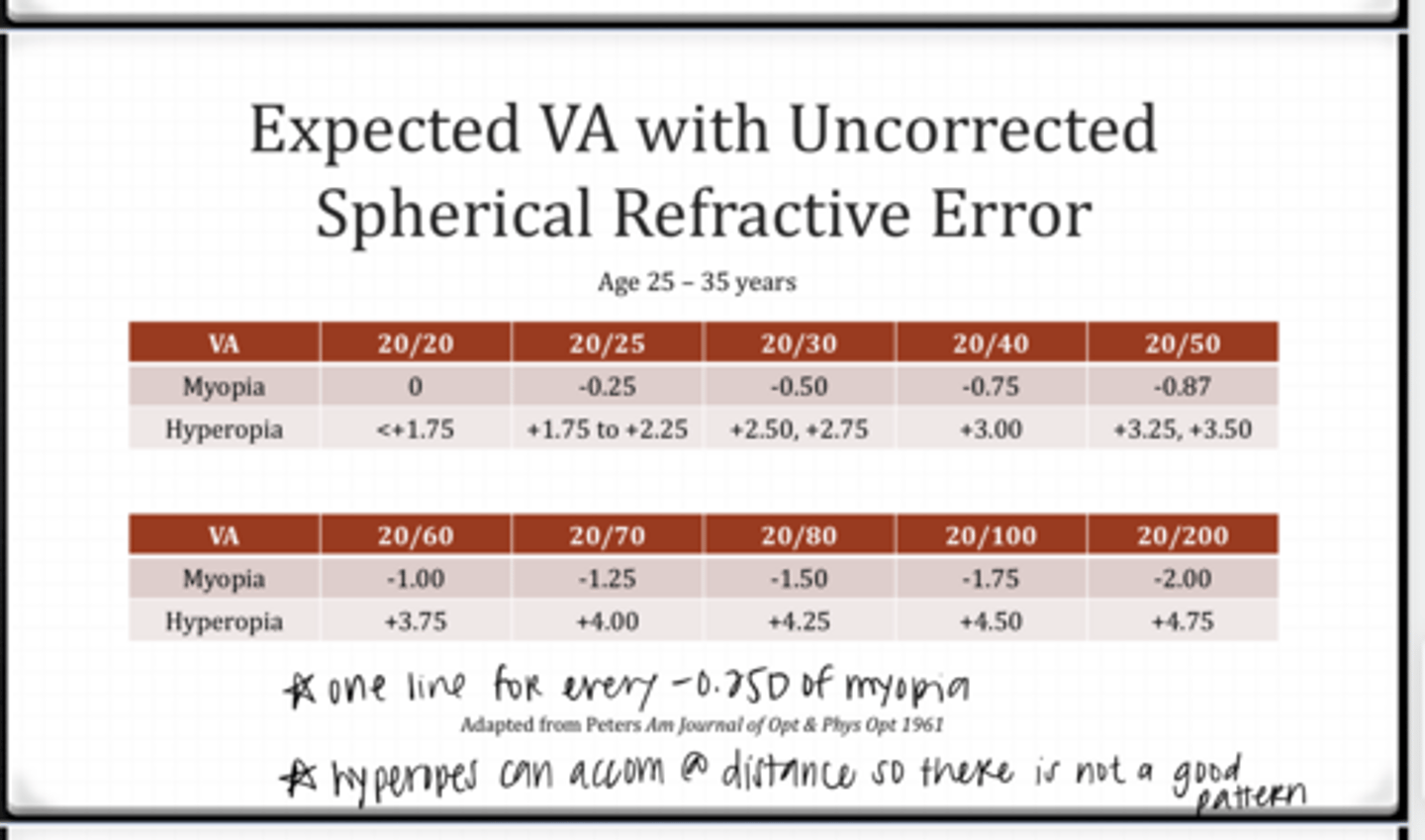
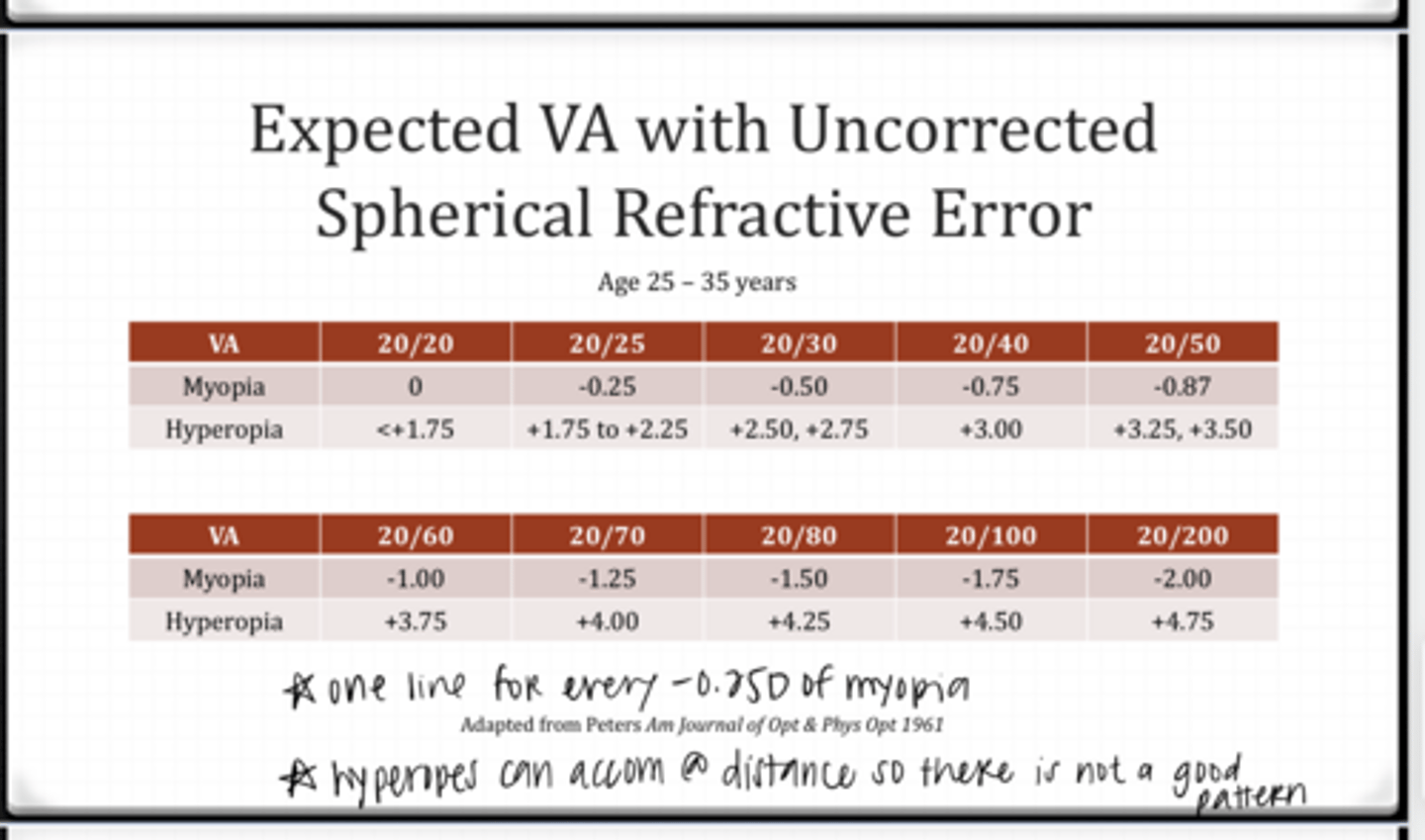
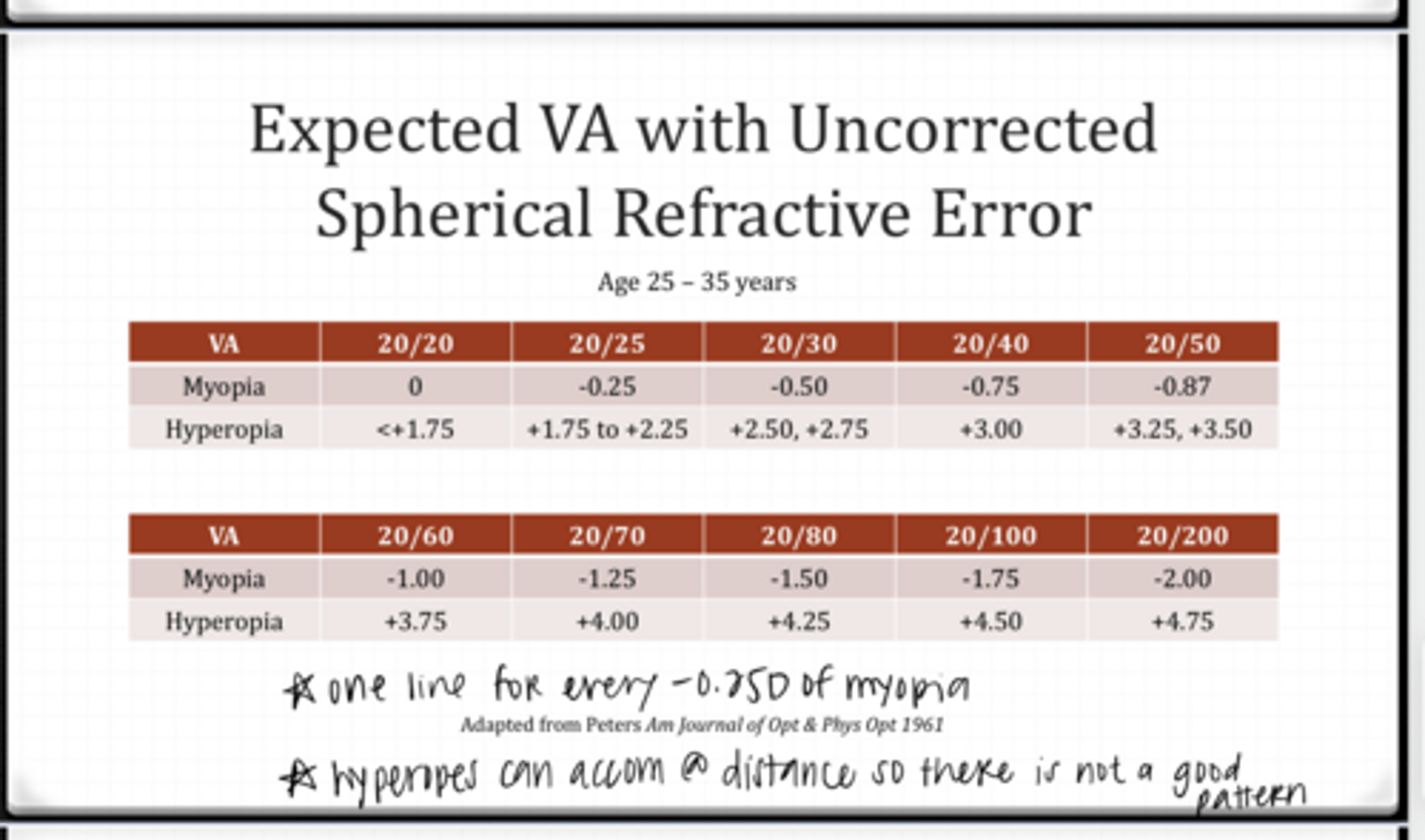
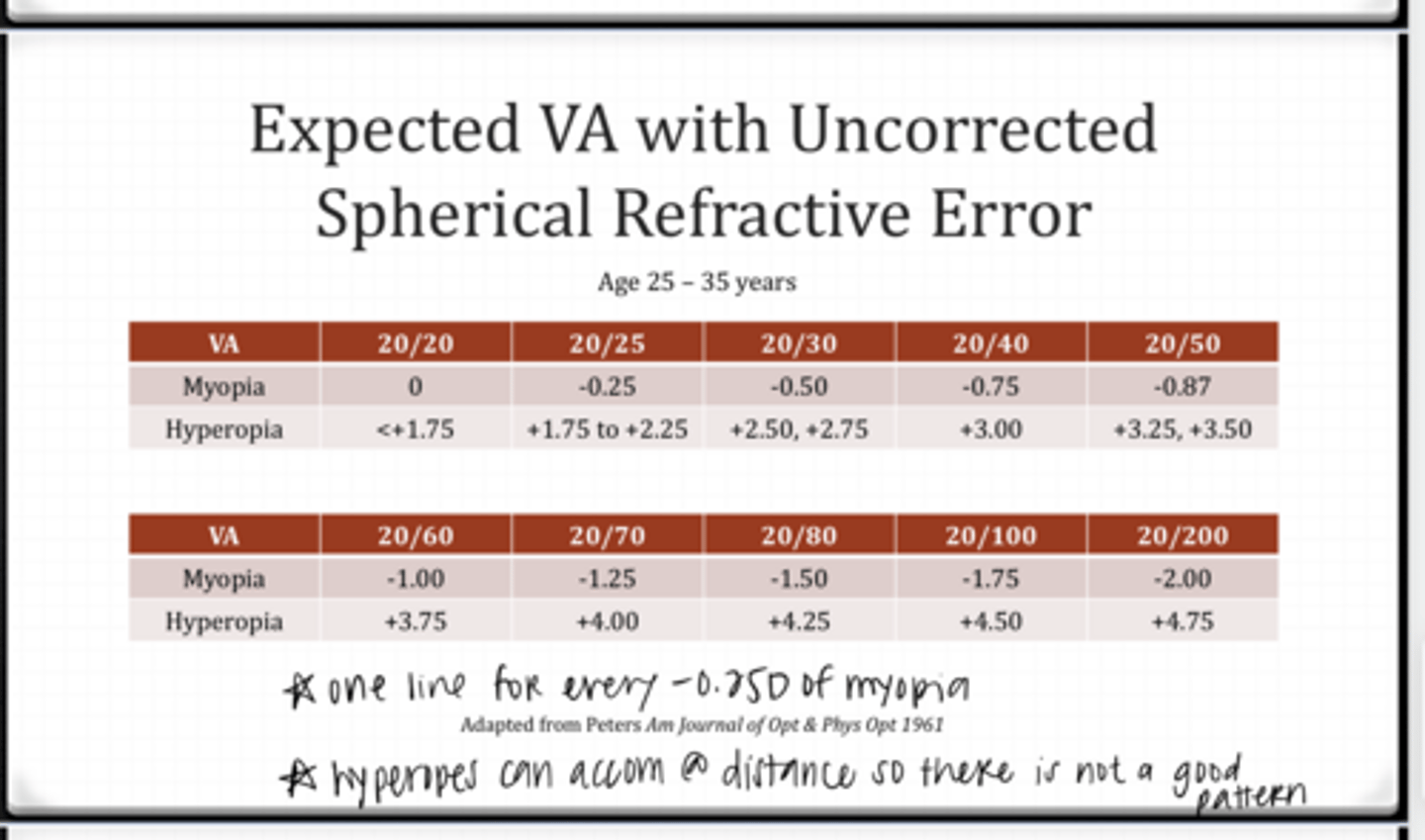
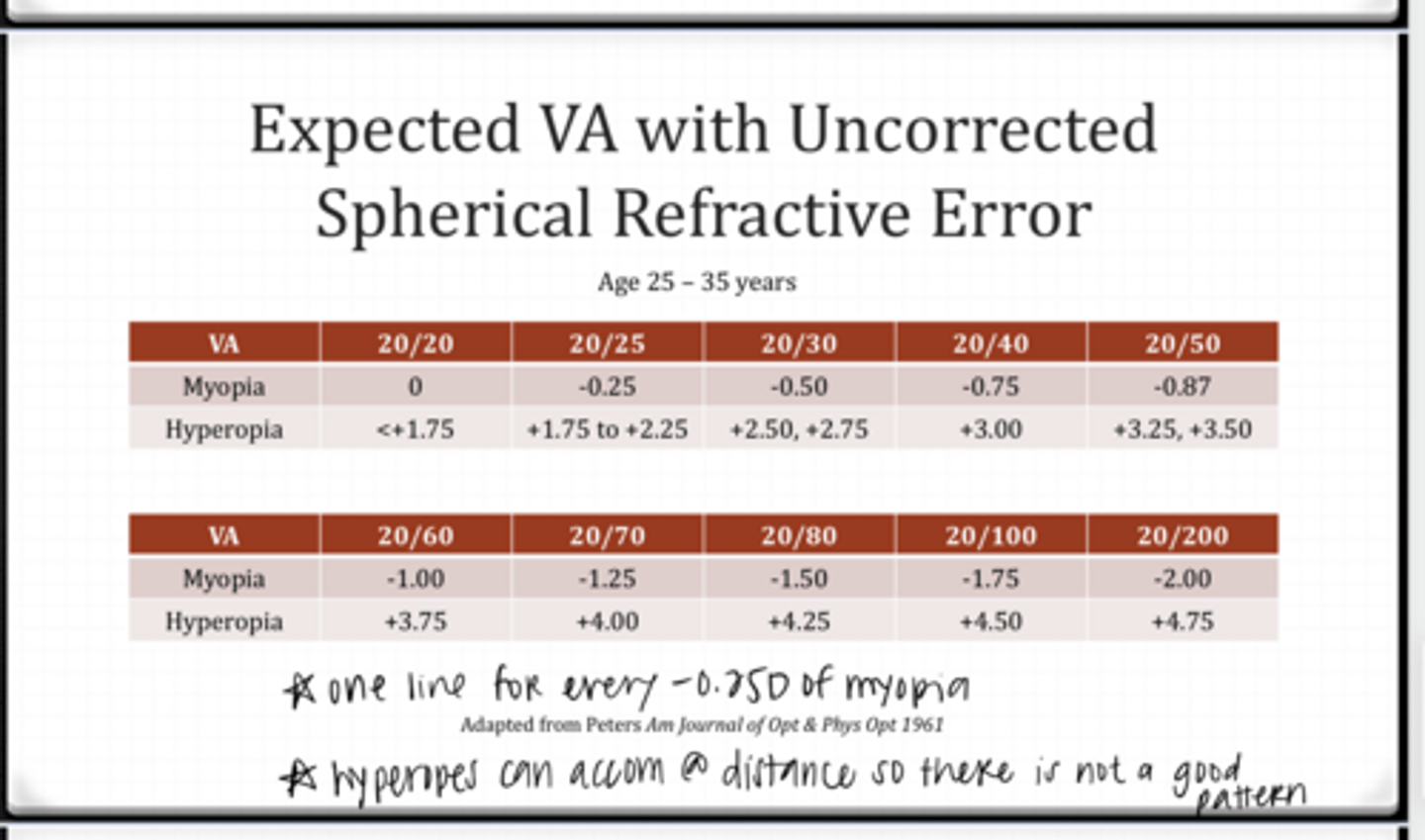
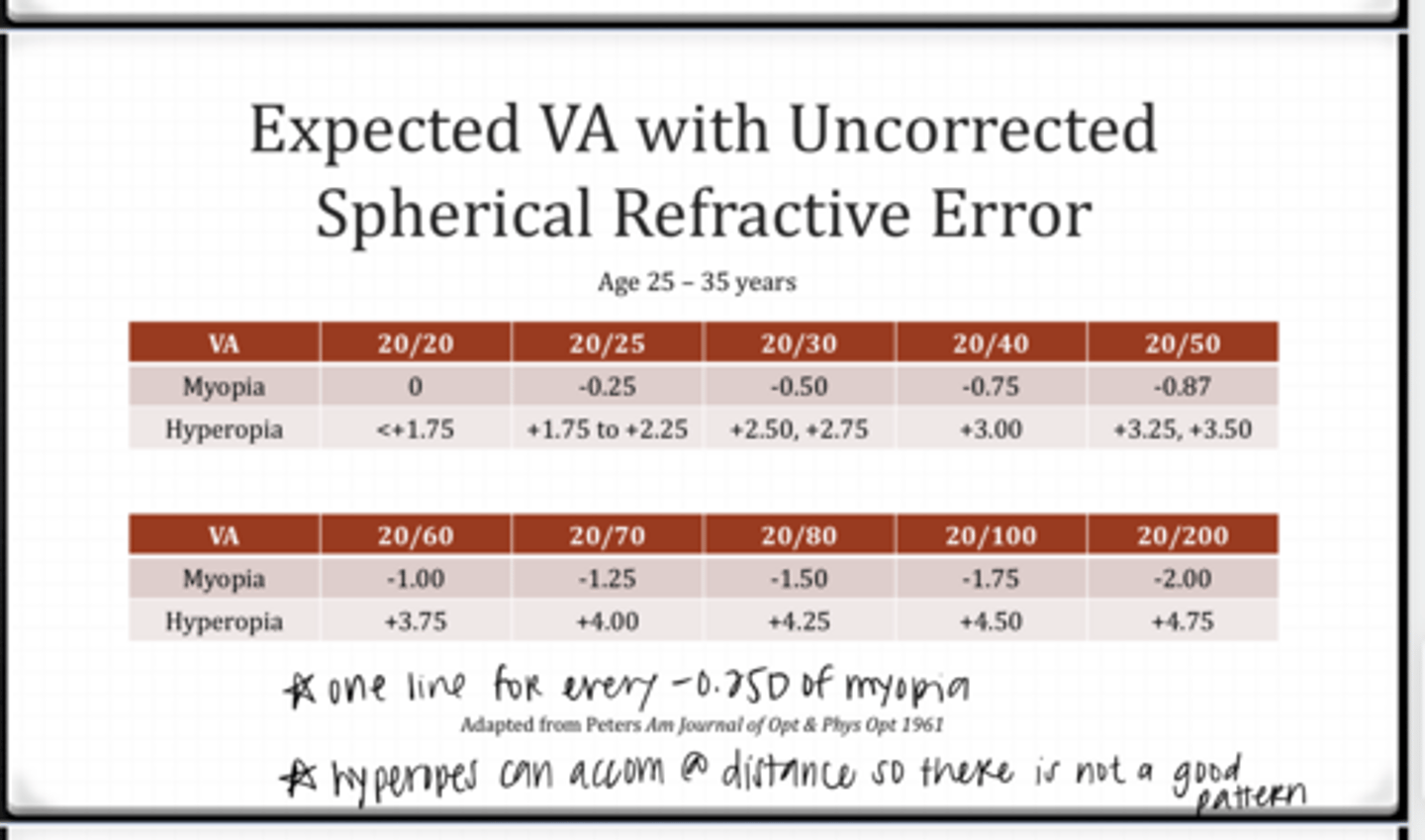
Expected VA with Uncorrected Spherical Refractive Error Chart (See Pic)
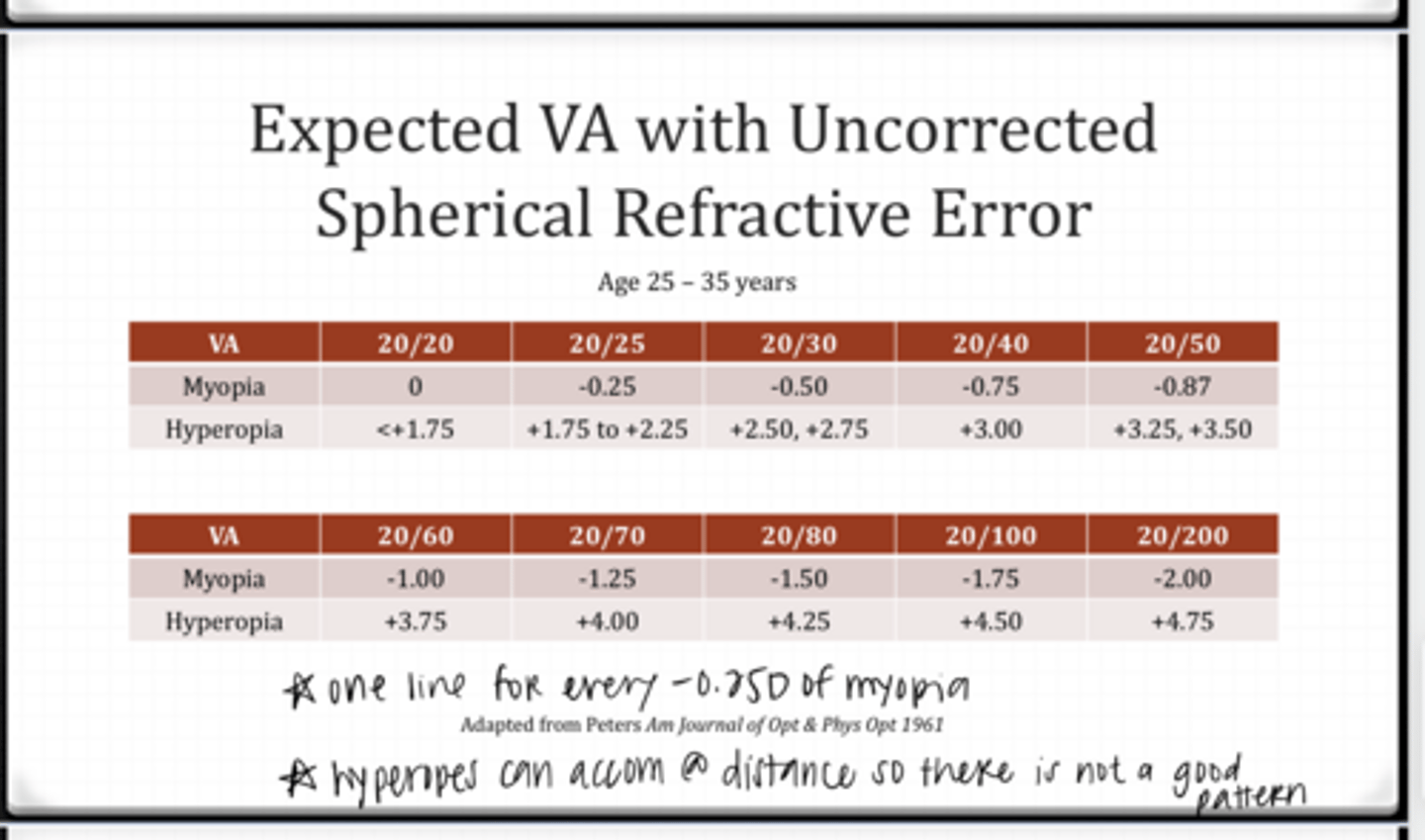
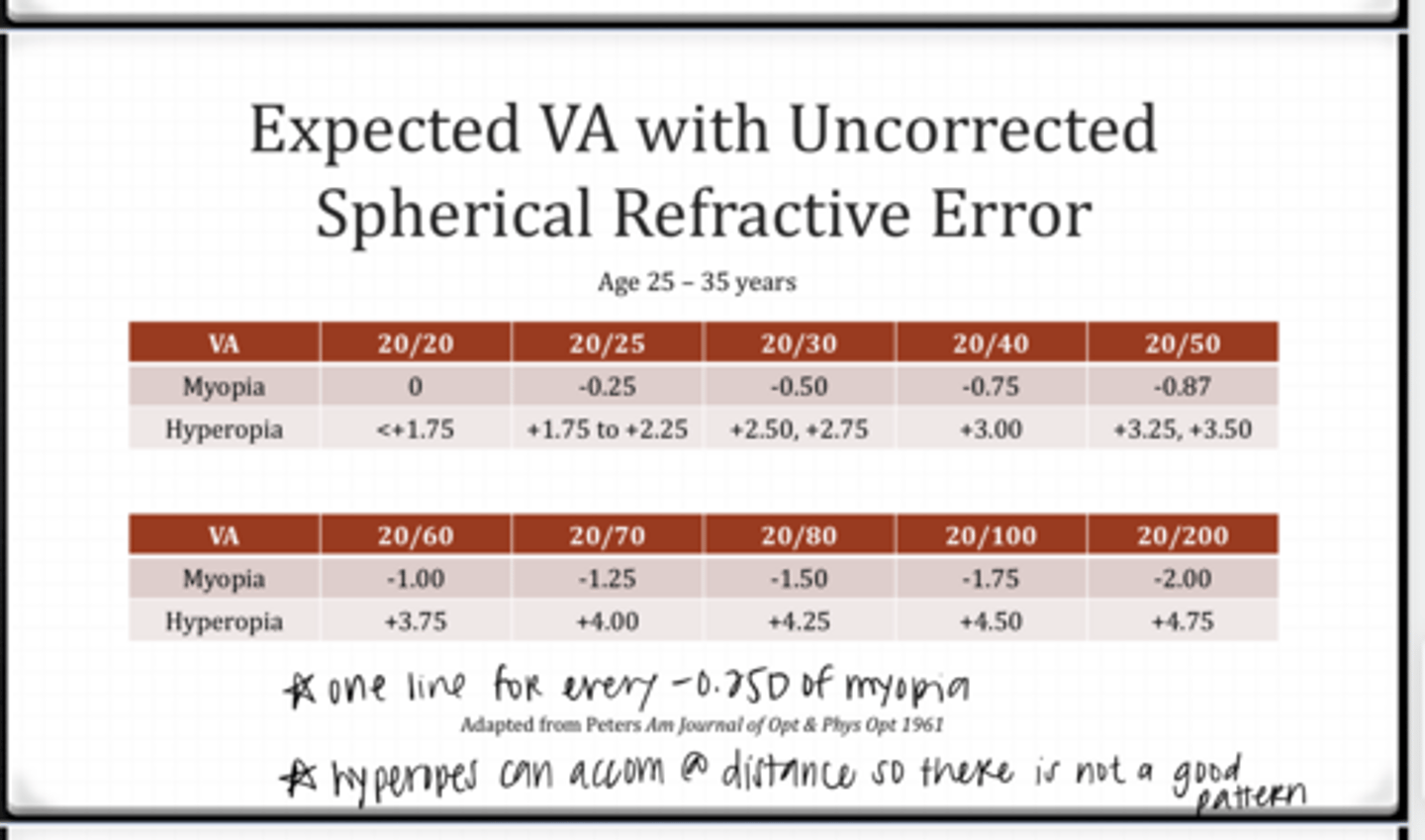
Expected VA with Uncorrected Spherical Refractive Error Chart (See Pic)
True or False:
For low amounts of uncorrected astigmatism (0.50-0.75D), you can use the SE table to determine expected VA
true
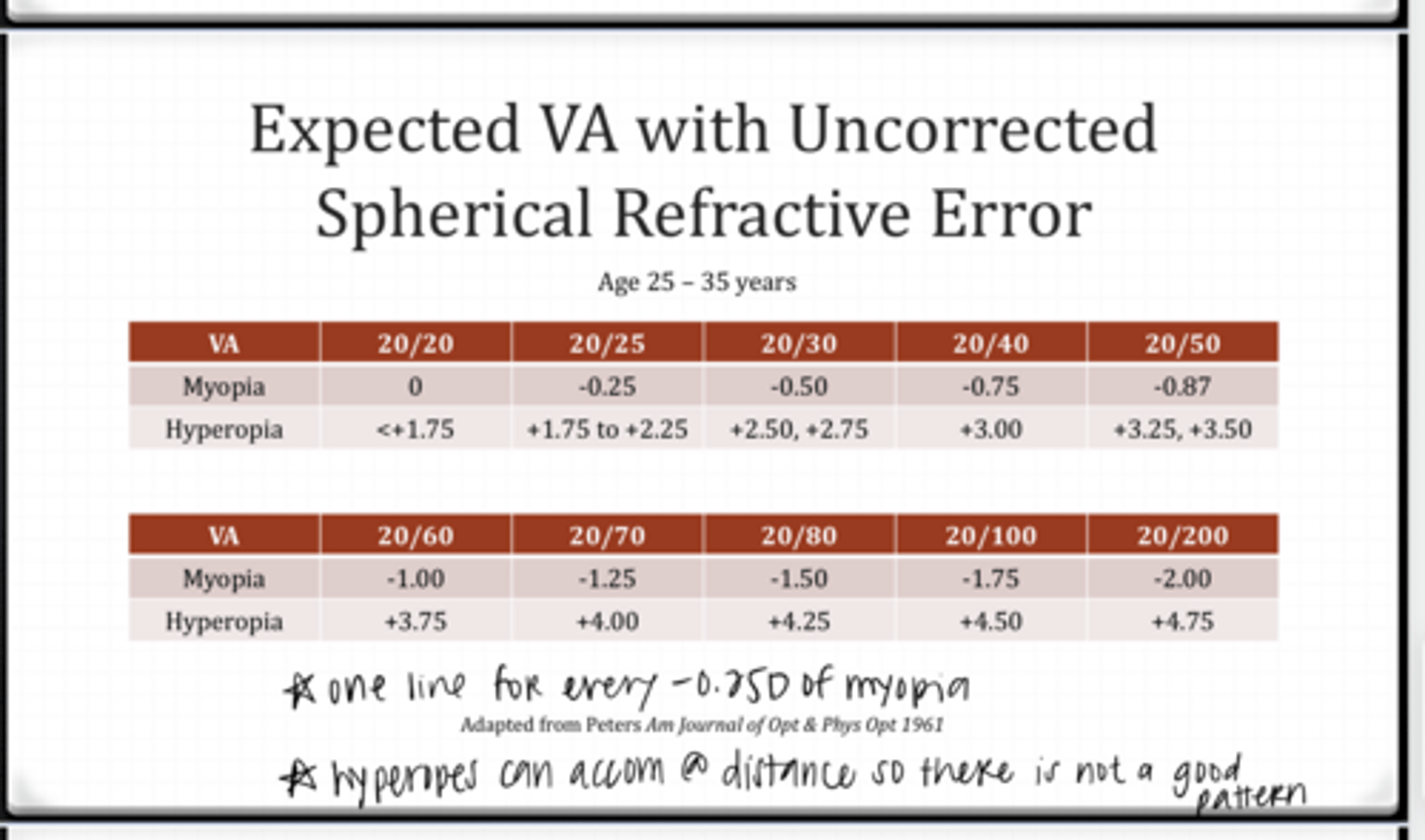
True or False:
For higher amounts of uncorrected astigmatism you can use the SE table to determine expected VA
false -- VA will be poorer than the predicted SE VA
What is the expected uncorrected VA for the following 30yo patient?
0.50D myope
20/30
What is the expected uncorrected VA for the following 30yo patient?
1.25D hyperope
20/20
What is the expected uncorrected VA for the following 30yo patient?
-0.50-0.50x145
-SE: -0.75
-Expect 20/40 VA
What is the expected uncorrected VA for the following 30yo patient?
Lenso: -3.25
Ref: -3.75
-myopia is -0.50 undercorrected
-You would expect VAs to be around 20/30
What is the expected uncorrected VA for the following 30yo patient?
Lenso: -3.75
Ref: -3.25
-myopia is +0.50 overcorrected
-You would expect VAs to be around 20/20
-Patient is able to accommodate 0.50D at distance
Does the following data make sense?
Entering VA with current Rx: 20/20
Lenso: -3.75-0.75x026
Ref: -4.25-1.25x019
-This does not make sense
-SE Lenso: -4.125
-SE Ref: -4.875
-Patient is -0.75 undercorrected and this would account for 20/40 VAs expected
Does the following data make sense?
20 yo patient
Entering VA with current Rx: 20/20
Lenso: +3.75-0.75x026
Ref: +4.50-0.25x019
Yes -- young hyperopes will have good VA when undercorrected by 1.00D
Does the following data make sense?
60 yo patient
Entering VA with current Rx: 20/20
Lenso: +3.75-0.75x026
Ref: +4.50-0.25x019
No -- 60yo would NOT be able to accommodate for the 1.00D undercorrected hyperopia that is present. VA should be reduced.
Does the following data make sense?
27 yo patient
Entering VA with current Rx: 20/25
Lenso: +3.75-0.75x026
Ref: +3.00-1.25x019
No -- if hyperopes are over-corrected by 1.00D SE then distance VA should be more reduced than 20/20. Would expect 20/60ish VAs
What are the 4 components to ocular accommodation? Total accommodation will equal the sum of these components...
1) blur (defocus) accommodation
2) convergence accommodation
3) proximal accommodation
4) tonic accommodation
What is the stimulus for blur (defocus) accommodation?
retinal image defocus
What is blur (defocus) accommodation driven by?
feedback loop -- continually evaluating the amount of defocus and updating blur accommmodation
In accommodative dysfunction, symptoms are thought to be d/t what?
strain on blur (defocus) accommodation
What is convergence accommodation?
accommodation that is driven by the act of convergence
What is the rate of convergence accommodation d/t?
convergence accommodation / convergence (CA/C)
What is the typical units of convergence accommodation?
diopters/prism diopters of convergence
What is a normal CA/C ratio?
0.1-0.4D / prism diopter
Is convergence accommodation and thus CA/A ratios usually measured clinically?
No
What is proximal accommodation?
accommodation that is driven by the perceived nearness of a target
Can proximal accommodation effect clinical testing?
yes -- mirrored room and instrument accommodation can effect
What is tonic accommodation?
base-line value in absence of any stimulus to accommodation
When performing minus lens tromboning, which type of accommodation is being trained?
blur accommodation