Hyperlipidemia- Kearns
1/93
Earn XP
Description and Tags
These flashcards are easier than what Kearns is gonna ask.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
94 Terms
Hyperlipidemia = high ________________
cholesterol
Lipids are insoluble in plasma and are transported by _________________.
lipoproteins
What are the 4 major types of lipoproteins?
Chylomicrons
VLDL
LDL
HDL
What is the name of the genetic disorder where a mutation in lipoproteins causes lipids to be incorrectly metabolized?
hyperproteinlipidemia
If a pt had hyperproteinlipidemia and had problems with their VLDL lipoproteins, what would you expect to see?
lipids to stay in the cells
increase in bile
If a pt had hyperproteinlipidemia and had problems with their LDL lipoproteins, where would you expect lipids to accumulate?
in the blood
If I had a lipid panel, would it be a good idea to use my LDL-C value to diagnose?
no
Hyperproteinlipidemia is a disorder that may lead to the buildup of which of the following in the systemic circulation? SATA
a. LDL
b. HDL
c. triglycerides
d. cholesterol
ALL
What are some of the reasons we need cholesterol?
cell membrane component
hormone production
produce bile salts
synthesize Vit D
helps nervous system
mood/stress stabilizer
What are the 2 strategies for CV prevention dealing with cholesterol?
lower LDLs
increase HDLs
LDLs are mostly _________ and HDLs are mostly ___________.
LDLs are mostly lipids and HDLs are mostly protein.
VLDLs are the primary carriers of ________________.
triglycerides
What makes up the core of a lipoprotein?
cholesterol esters
triglycerides
What makes up the outer layer of the lipoprotein?
apolipoprotein
free cholesterol
phospholipids
What are examples of pro-atherogenic molecules?
chylomicron remnants
VLDL
LDL
What are examples of anti-atherogenic?
HDL
What are the functions of apolipoproteins?
structure
ligands
activators or inhibitors of enzymes in the metabolism of lipoproteins
A lipid blood test detected by measuring lipids in serum after a _____-hour fast.
10
Risk of Heart Disease increases with
_______-atherogenic lipoproteins
HDL <____ mg/dL
LDL >______mg/dL
triglycerides >_______mg/dL
pro-atherogenic lipoproteins
HDL <40 mg/dL
LDL >160 mg/dL
triglycerides >200 mg/dL
What is the optimal and high, Total Cholesterol (mg/dL)?
optimal <200
high >239
What is the optimal and high, LDL (mg/dL)?
optimal <130
high >159
What is the optimal and high, HDL (mg/dL)?
optimal >60
high <40
What is the optimal and high, triglycerides (mg/dL)?
optimal <150
high >199
What is the optimal and high, Non-HDL-C (mg/dL)?
optimal <130
high >159
(Think: same as LDL)
PRACTICE:
Would an LDL value of 129 mg/dL be considered high, intermediate, or optimal?
optimal
PRACTICE:
Would an HDL value of 50 mg/dL, would that be considered high, intermediate, or optimal?
intermediate (between 40-60)
PRACTICE:
If I had a triglyceride level of 201 mg/dL, would that be considered high, intermediate, or optimal?
high
Which pathway deals with dietary cholesterol? (endogenous or exogenous)
exogenous
Briefly explain how the exogenous pathway works:
dietary lipids—> chylomicrons—> chylomicron full of TG in circulation—> TG are metabolized by muscles and fat by LPL—> chylomicron remnants are transported to the liver
Briefly explain how the endogenous pathway works:
liver—> VLDL formation—> VLDL metabolized to release fatty acids—>IDL—>LDL—>LDL taken up by LDLRs
What lipoprotein is used in reverse cholesterol transport? (LDL,VLDL,HDL, Chylomicron)
HDL
Enterohepatic circulation of bile acids includes what 3 steps?
bile acids secreted by __________ to __________________.
bile acids are stored in the __________________.
after a meal, bile acids are secreted into the _________________ then either absorbed by the _______________ or transported back to the ____________.
bile acids secreted by liver to gallbladder
bile acids are stored in the gallbladder
after a meal, bile acids are secreted into the intestine then either absorbed by the enterocyte or transported back to the liver.
What would happen if the gallbladder was removed?
we wouldn’t be able to store bile
After a meal what is secreted by the duodenal mucosa?
Cholecystokinin (CCK)
Cholecystokinin stimulates what?
release of bile from the gallbladder
After bile is released, micelles are formed, what is released from the pancreas to hydrolyze the triglycerides in that micelle?
Lipase!!
The threshold cholesterol conc for micelle formation is _________mmol/L.
1.5
After a large meal the bile acid conc in the small intestine is between ____-_____mmol/L
5-10
Enterohepatic Recycling allows drugs to do what?
provides a secondary absorption phase
prolongs t1/2
produces multiple peaks in plasma conc time
What transporter allows micelles and cholesterol to enter the enterocyte from the intestinal lumen?
NPC1L1
What protein is attached to the chylomicron and is a sign of chylomicron metabolism?
Apo B-48
If we had a mutation in the NPC1L1 transporter, does that mean we have a 0% risk of hyperlipidemia?
NO- we still have the endogenous pathway that could be causing hyperlipidemia
What enzyme do Statins inhibit?
HMG-CoA Reductase
If I had diabetes, how would that affect my lipid metabolism?
increase in Acetyl CoA causes increase in HMG-CoA
result: extra cholesterol production
What are the names of the 2 PCSK9 inhibitors that are humanized Antibodies?
Alirocumab
Evolocumab
What is the name of the PCSK9 Inhibitor that is an siRNA?
Inclisiran
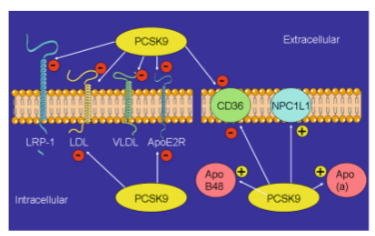
The BIG PICTURE of PCSK9 inhibitors is that it allows for ____________ to be recycled.
allows for RECEPTORS to be recycled
For intra and extra cellular PCSK9, out of EVERYTHING, the only mechanisms that are upregulated are what?
Apo B-48, NPC1L1, Apo-A
EVERYTHING ELSE IS DOWNREGULATED
Familial Hypercholesterolemia is what type of disorder?
a. autosomal recessive
b. sex-linked recessive
c. autosomal dominant
d. sex-linked dominant
c- AUTOSOMAL DOMINANT
For familial hypercholesterolemia, heterozygous (Cc) individuals have cholesterol levels between _______ to _______ mg/dL.
260 to 500 mg/dL
For familial hypercholesterolemia, homozygous (CC) individuals have cholesterol levels >_______mg/dL.
>1000 mg/dL
Does familial hypercholesterolemia, deal with the endogenous or exogenous pathway?
endogenous
If you have familial hypercholesterolemia, there is either a decreased or inability to produce __________.
a. HDLs
b. LDLRs
c. VLDLs
d. Lipase
b
List the brand name for each of the following statins:
Rosuvastatin
Atorvastatin
Simvastatin
Lovastatin
Pravastatin
Fluvastatin
Rosuvastatin- Crestor
Atorvastatin- Lipitor
Simvastatin- Zocor, Flolipid
Lovastatin- Mevacor, Altoprev
Pravastatin- Pravachol
Fluvastatin- Lescol
All statins are indicated in cases of…
primary hypercholesterolemia
mixed dyslipidemia
What is the pleiotropic (secondary) effect of Statins?
decrease vascular inflammation as atherosclerotic lesions stabilize
Do statins possess low or high systemic bioavailability?
low
A good counseling points of statins is to take them with __________.
water
Which of the statins are prodrugs?
Lovastatin
Simvastatin
Which of the statins are hydrophilic? What groups allow them to be hydrophilic?
Rosuvastatin- sulfonamide
Pravastatin- carboxylic acid/carboxylate
Which statins are non-lactone/fluorinated statins?
atorvastatin
fluvastatin
rosuvastatin
Lovastatin is converted to it’s active metabolite through what reaction? Additionally, what group is modified in that reaction?
converted through hydrolysis
lactone group is modified
Which of the statins are metabolized by CYP2C9?
fluvastatin
rosuvastatin
Which of the statins are metabolized by CYP3A4?
Atorvastatin
Lovastatin
Simvastatin
Which of the statins are not metabolized by any of the CYPs?
pravastatin
Each statin and their drug interactions:
just a helpful table I made for reference:
TIPS:
Look at the CYP of each drug- all CYP3A4’s have similar interactions
Cyclosporine interacts w/ everything but Fluvastatin
Fluvastatin doesn’t react with any of the drugs Kearns wants us to know, while Lovastatin reacts with everything
-Sarah Kiser, said she remembered they asked about antidepressants on her exam so make note of that-
Drug | Drug Interactions |
Atorvastatin (CYP3A4) | Azole Antifungals Non-DHPs (rare) Cyclosporine Antidepressants |
Fluvastatin (CYP2C9) | Nothing |
Lovastatin (CYP3A4) | Azole Antifungals Non-DHPs Cyclosporine Antidepressants Macrolide Antibiotics Warfarin |
Pravastatin (no CYP) | Cyclosporine |
Rosuvastatin (CYP2C9) | Cyclosporine Warfarin |
Simvastatin (CYP3A4) | Azole Antifungals Non-DHPs Cyclosporine Antidepressants Macrolide Antibiotics |
What are the Drug Interactions for Atorvastatin?
Specifically, does it interact with:
Azole antifungals
Non-DHPs
Cyclosporine
Macrolide Antibiotics (-mycin)
Warfarin
Antidepressants
azole antifungals
non-DHPs
Cyclosporine
Antidepressants
What are the Drug Interactions for Fluvastatin?
Specifically, does it interact with:
azole antifungals
Non-DHPs
Cyclosporine
Macrolide Antibiotics (-mycin)
Warfarin
Antidepressants
NONE OF THESE
What are the Drug Interactions for Lovastatin?
Specifically, does it interact with:
azole antifungals
Non-DHPs
Cyclosporine
Macrolide Antibiotics (-mycin)
Warfarin
Antidepressants
ALL OF THESE
What are the Drug Interactions for Pravastatin?
Specifically, does it interact with:
azole antifungals
Non-DHPs
Cyclosporine
Macrolide Antibiotics (-mycin)
Warfarin
Antidepressants
Cyclosporine
What are the Drug Interactions for Rosuvastatin?
Specifically, does it interact with:
azole antifungals
Non-DHPs
Cyclosporine
Macrolide Antibiotics (-mycin)
Warfarin
Antidepressants
Cyclosporine
Warfarin
What are the Drug Interactions for Simvastatin?
Specifically, does it interact with:
azole antifungals
Non-DHPs
Cyclosporine
Macrolide Antibiotics (-mycin)
Warfarin
Antidepressants
azole antifungals
non-DHPs
Cyclosporine
Antidepressants
Macrolide Antibiotics
PRACTICE:
Which of the following statins would interact with Warfarin? SATA
a. Crestor
b. Lipitor
c. Mevacor
d. Pravachol
a, c
What is the most common add-on tx with statins and why?
Ezetimibe (Zetia)
bc PCSK9 inhibitors are expensive
How does Niacin effect the…
endogenous pathway
exogenous pathway
and it’s overall goal
endogenous
decreases TG synthesis—> decreases VLDL formation—> decreases FFA and LDL—> increases HDL
exogenous
increases chylomicron removal from plasma
overall goal:
increase HDL
decrease LDL, TG
Fibrates are ligands for NFT PPAR-a and up-regulate what? Additionally, what is the goal of fibrates?
up-regulate LPL, apo A-I, and apo A-II
goal: decrease VLDL, Increase HDL
Which has a longer half-life… Gemfibrozil or Fenofibrate?
Fenofibrate
What are the warnings with fibrates?
avoid in hepatic/renal dysfunction
should not give with Ezetimibe or Statins
Fibrates could be combined with…
niacin or PSCK9 Inhibitor
What is the active metabolite of Fenofibrate?
Fenofibric acid (Trilipix)
What are the generic names of Bile acid sequestrants and when are they used?
Names: “The C’s” Colesevelam, Colestipol, Cholestyramine
Used: In isolated LDL increases
MOA of Bile acid sequestrants:
bind to bile acids in the intestinal lumen and prevent their reabsorption
effects exogenous
Bile acid sequestrants… pos or neg feedback?
negative feedback
Toxicity warning of bile acid sequestrants and what to do because of that:
absorption of certain drugs may be impaired
give those meds 1 hr before or 2 hrs after taking
Ezetimibe is a ________________ absorption inhibitor. The goal is to decrease _______.
cholesterol, LDL
What transporter does Ezetimibe block?
NPC1L1
PRACTICE:
If I wanted a statin that stayed in my plasma longer, which of the following would I chose?
a. Lipitor
b. Zocor
c. Mevacor
d. Lescol
d
Toxicity warning of Ezetimibe:
prior lipid lowering therapy in combo of sterol absorption inhibition has been associated w/ coronary events
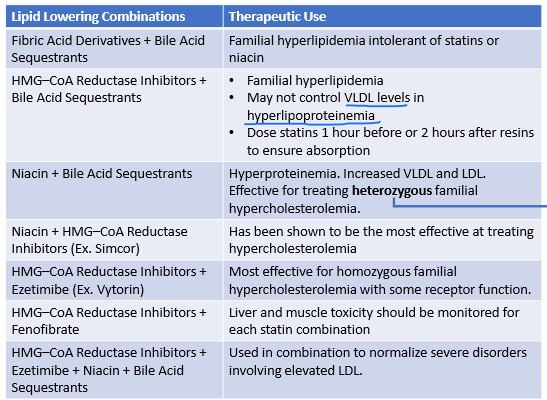
When are these 2 meds used in combo?
Fibrates + Bile acid sequestrants
familial hyperlipidemia
can’t use statins/niacin
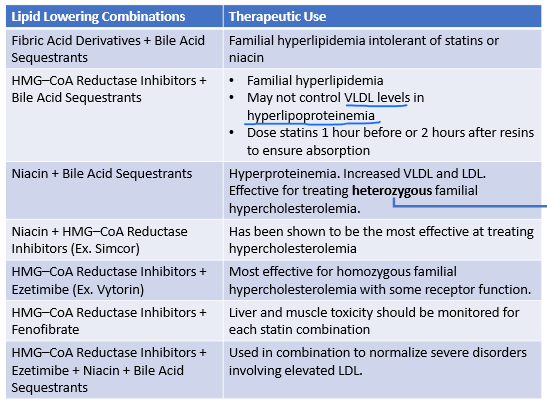
When are these 2 meds used in combo?
Statin + Bile acid sequesterants
familial hyperlipidemia
bc of bile acid seq. make sure you give 1 hr before or 2 hr after
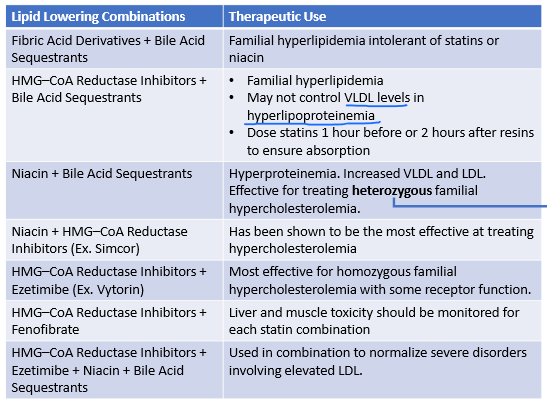
When are these 2 meds used in combo?
Niacin + Bile acid sequestrants
HETEROZYGOUS familial hypercholesterolemia
hyperproteinuria
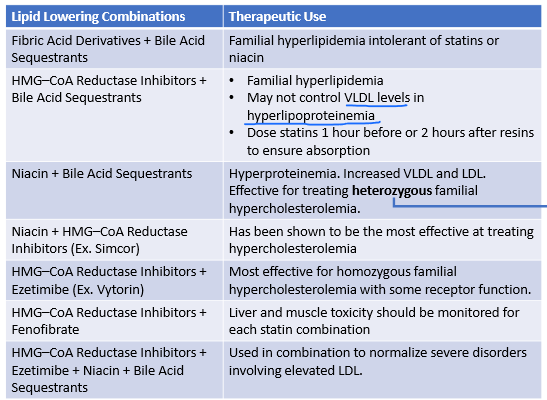
When are these 2 meds used in combo?
Niacin + Statin
hypercholesterolemia
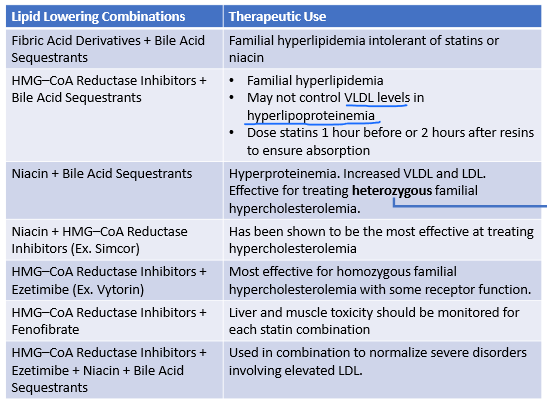
When are these 2 meds used in combo?
Statin + Ezetimibe
HOMOZYGOUS familial hypercholesterolemia
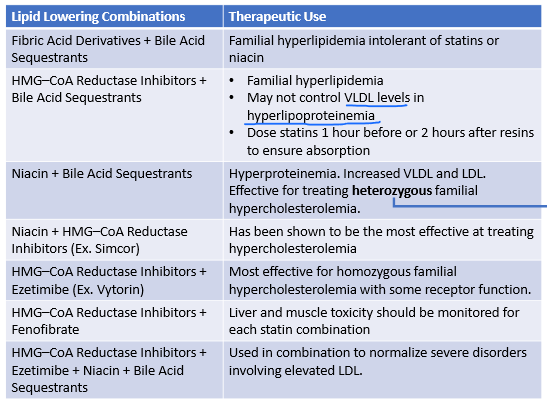
When are these 2 meds used in combo?
Statin + Ezetimibe + Niacin + Bile acid sequesterants
severe disorders involving high LDL