J Clin Med Gyn (Detailed)
1/321
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
322 Terms
menarche definition
onset of menstruation (lasts avg 28 days)
normal = 11-13.75 yrs, correlates w/ obesity
Day 1 = first day of bleeding
occurs 2-3 years after thelarche (tanner stage IV breast dev)
occurs anywhere from stage II-stage V for either breast/pubic hair dev (usually stage IV)
menopause definition
cessation of menses >1 year d/t loss of ovarian function
→ decreased estrogen + progesterone production
hormones in menstruation
hypothalmus releases GnRH to anterior pituitary
FSH and LH is released = growth of follicle and ovulation
→ release of progesterone during luteal phase of menstrual cycle
→ release of estrogen in follicular (before ovulation) AND luteal phase (after ovulation, when follicle → corpus luteum)
corpus luteum
white body in the ovary that secretes progesterone
formed from follicle following ovulation
progesterone role
increases blood flow/makes blood vessels
estrogen needs _, otherwise → lining w/o blood flow sloughs off → period
estrogen role
thickens the endometrial lining of uterus
replication of cells
amenorrhea definition
lack of menstrual period
dysmenorrhea definition
painful menstrual periods
polymenorrhea
cycles of < 21 days = happening often
menorrhagia definition
regular but very heavy periods or lasting for long time
→ anemia if chronic
ovulatory
metrorrhagia definition
uterine bleeding at irregular intervals
(esp between expected menstrual periods)
ovulatory or anovulatory
menometrorrhagia definition
prolonged/excessive uterine bleeding is irregular and more frequent than normal
puberty definition
developmental stage where secondary sexual characteristics appear
precocious puberty definition
onset of puberty an abnormally early age
<8 yo girls or <9 yo boys
thelarche definition
onset of female breast dev
adrenarche definition
first step in puberty!
onset of androgen-dependent body changes
(growth of axillary/pubic hair, body order, acne)
what do tanner stages correlate more with*
MSK maturity > chronological age
catamenia definition*
hx of a given female’s menstrual cycles
age of onset X # of days in cycle X duration of flow
ex: catamenia 13×28×5
PMS and neurotransmitter involved in PMS*
characterized by physical and behavioral symptoms
lack of serotonin
beta-endorphin, GABA, and ANS
luteal phase only
premenstrual dysphoric disorder (PMDD) refers to ONLY
behavioral components of premenstrual period
sx assoc. w significant distress/interference w activities
PMS/PMDD non-pharm tx
Avoid caffeine + alcohol, cigarettes, salt reduction
Get enough sleep
regular exercise
stress management (yoga, massage, etc)
NSAIDs
Vitamin B6 + E
Cognitive behavioral therapy
effective pharm tx of PMS/PMDD*
SSRIs
benzos
OCPs
agents that suppress ovulation: GnRH agonists, danazol
possible/ineffective tx of PMS/PMDD
possible: diuretics, calcium, vit b6
ineffective: progesterone, vit supps, TCAs, dietary restrictions, lithium
primary dysmenorrhea definition
painful menstruation with NO pelvic pathology
recurrent, crampy lower abdominal pain occurs during menstruation in absence of pelvic pathology
primary dysmenorrhea summary*
most common gyn complaint among adolescent females
cause: prod of of endometrial prostaglandin PGF2a AKA too much prostaglandins
dx: labs/images unnecessary unless possible pelvic dz, laparoscopy if unresponsive to 3 cycles of initial tx
tx: 1st line = NSAIDs (non steroidal anti-inflammatory drug)
2nd line: OCPs
heat compress, vit B and E, exercise
primary dysmenorrhea - cause
too much prostaglandins (PGF2a)
primary dysmenorrhea - dx
labs/imaging unnecessary UNLESS pelvic dz or unresponsive to meds → laparoscopy
primary dysmenorrhea - 1st line tx
NSAIDs
carboprost tromethamine (hemabate) is what
analog of PGF2a (prostaglandin) used to treat pp uterine atony
(makes uterine blood vessels + muscle constrict)
secondary dysmenorrhea definition
painful menstruation in presence of pelvic pathology
secondary dysmenorrhea summary*
more common among women in 4th/5th decades of life
dx: transvaginal U/S initial imaging of choice
tx the underlying factor
secondary dysmenorrhea causes (painful period w/ pelvic pathology)
gynecologic
endometriosis
adenomyosis
fibroids
ovarian cysts
intrauterine or pelvic adhesions
PID
obstructive endometrial polyps
congenital malformations
cervical stenosis
imperforate hymen
use of IUD
non-gynecologic
IBD/IBS
ureteropelvic junction obstruction
psych issues
primary amenorrhea definition
no menses by 13 yo with NO normal growth/2nd sex chars
OR no menses by 16 yo WITH normal growth/2nd sex chars
secondary amenorrhea definition
cessation of REGULAR menses for 3 months
or cessation of IRREGULAR menses for 6 months
prolonged amenorrhea can be the earliest sign of?
decline in general health
signal underlying condition ie hypothyroidism
primary amenorrhea causes
turner syndrome**, (anatomic) - gonadal dysgenesis/chromosome abnormality
androgen insensitivity, (endocrine) - disorder of HPA
constitutional delay of puberty,
abnormalities of outflow tract
turner syndrome (45 XO) stigmata**
Short stature
Low hairline
Shield-shaped thorax
Shortened 4th metacarpal
Small fingernails
Brown Nevi
Coarctation of the aorta
Nuchal fold (webbed neck with fold at base of neck)*
Elbow deformity
Rudimentary ovaries (gonadal streaks)
No menstruation
mullerian agenesis description
mullerian duct does not grow
→ agenesis/underdev of vagina/uterus
ovaries are normal! (separate embryologic source)
#1 cause of secondary amenorrhea**
pregnancy (1st step is to exclude pregnancy/preg test!)
#2: menstruation
others (either primary/secondary): ovary, hypothalamus, pituitary, meds, thyroid, celiac dz
ovarian causes of amenorrhea
PCOS (INC androgen and estrogen = ovary dysfx)
premature ovarian failure
sole uterine cause of secondary amenorrhea
asherman’s syndrome
(presence of adhesions/synechiae that prevent endometrium from responding to estradiol)
amenorrhea is more likely with _ _ compared to ?
severe hyperthyroidism
mild hyperthyroidism/hypothyroidism
menopause occurrence
d/t genetically programmed loss of ovarian follicles → complete ovarian follicular depletion
follicle role
egg maturation
hormone production
menopause s/sx*
irregular bleeding patterns, (anovulation → progesterone def)
hot flashes, (common at night)
vaginal dryness → itching, sexual dysfunction, atrophic urethritis, (recurrent UTI)
depression,
mastodynia, (breast pain)
migraines,
insomnia,
skin changes,
joint pain,
impaired balance
how to confirm menopause
no menses for 12 months
FSH level (very high)
when ovary fx declines, FSH goes UP. estrogen is present but no ovulation = low progesterone → irregular bleeding
ovary still secretes androgens
sources of estrogen after menopause
adipose tissue
zona reticularis of adrenal gland
perimenopause
ovulatory and anovulatory cycles
1st a lengthening of interval between normal menstruation → eventually cycles are skipped
chronic anovulation → unopposed estrogen (no progesterone)
if endometrium <4 mm, good! if higher = sus b/c estrogen only can’t cause thicker endometrial layer → biopsy
T/F: once menopause starts, no amount of bleeding is acceptable
T
menopause tx*
hormone replacement therapy (HRT) - short-term
^ must be estrogen/progesterone combo HRT if they have uterus d/t risk of hyperplasia and cancer (which can occur in 6 months of unopposed estrogen therapy = no sloughing)
nonhormonal for hot flash: relaxation not effective, SSRIs/SNRIs, GABA
HRT risks for menopause*
long-term not recommended
estrogen HRT: mixed results for breast cancer, INC stroke, MI, TEP (DVT/PE), + colon cancer <70
E+P HRT: INC of breast cancer, MI, TEP, LOWER risk of colon cancer
less risk of fractures after 4-5 yrs
high risk of CV (MI/stroke) in 1st year
causes of abnormal uterine bleeding*
pregnancy*
structural uterine pathology (fibroids/polyps/adenomyosis)
anovulation
hemostasis disorder
neoplasia
trauma/infx
normal menstrual flow*
change pads >/3 hrs
fewer than 21 pads/tampons per cycle
do not change pads during night
clots <1 in in diameter
mildly/not anemic
causes of menorrhagia
distortion of endometrium (leiomyoma, polyp, adenomyosis)
menopausal transition (anovulatory cycles)
VWD or other clotting factor/def
causes of intermenstrual bleeding (metrorrhagia)
breakthrough bleeding (esp OCPs)
non-progesterone IUD
polyps or cancer
bloody discharge (d/t endometritis, cervicitis, vaginitis)
ovulatory abnormal uterine bleeding (AUB) summary*
regular intervals + excessive flow/duration (menorrhagia)
breast tenderness, bloating, mood changes, vaginal secretions
cause: anatomic/physical lesion (ie polyp, adenomyosis, cancer, fibroid, FB), hemostatic defect (starts menarche, d/t coagulopathy), infx, trauma
anovulatory abnormal uterine bleeding (AUB) summary*
unpredictable (metrorrhagia) w variable flow/duration
(unopposed estrogen → endometrial proliferation)
causes: HPA (menarche, menopause, stress, lactation, excessive exercise, eating disorders) PCOS, thyroid disorders, drugs (OC’s, progestins, antidepressants + antipsychotics, steroid)
(teens, >40 yo)
menorrhagia definition
excessively heavy periods (>1 pad/tampon q1-2 hr) or excessively long periods (more than 7 days)
bleeding associated with IUDs follows a pattern of _ _ BUT they tend to what?*
anovulatory bleeding
continue to ovulate
in adults, when should you do endometrial sampling when abnormal uterine bleeding (AUB)?
hx of unopposed estrogen exposure (chronic anovulation, obesity, PCOS)
persistent AUB
med management failure
other risks (ie fh or tamoxifen)
tx for AUB
tx underlying cause
if anovulatory bleeding:
preg test, TSH, PLN
COC drugs (cause regular cycle)
cyclic progestins / progestin IUD
NSAIDs (reduce blood loss / dec prostaglandin:thromboxane ratio → hemostasis [vasodilation:vasoconstriction]
refractory = estrogen therapy, endometrial sampling again
last resort: hysterectomy, endometrial ablation (good w/ no polyps/fibroids)
endometrial hyperplasia cause
unopposed estrogen
proliferation of endometrial glands → thickened endometrium and AUB
simple → atypia (complex w atypia = INC risk of endometrial cancer)
cause of unopposed estrogen (endometrial hyperplasia)
pharm (HRT, tamoxifen)
endogenous = chronic anovulation (PCOS, perimenopause), obesity (adipose tissue makes estrogen), estrogen secreting tumors
indications of endometrial biopsy*
presence of atypical glandular cells* (AGUS) on cervical cytology (those come from the uterus)
>45 yo AUB or <45 yo AUB w RF (chronic anovulation, obesity, tamoxifen, DM, FH of cancer)
no response to tx
women w uterus w unopposed ERT
presence of endometrial cells on cervical cytology if >/40 yo (perimenopausal)
women w lynch syndrome (hereditary nonpolyposis colorectal cancer)
peutz-jehgers syndrome
lynch syndrome definition
genetic condition that INC your risk of developing cancer esp colorectal and endometrial cancer

peutz-jehgers syndrome definition
dev of hamartomatous growth in stomach and intestine
uterine cancer risk
small/dark colored spots on lips/hands/feet/mouth/anus
endometrial hyperplasia dx/tx
dilation & curettage (D&C) (b/c high coexistence with endometrial carcinoma)
no atypia = cyclic progestins / progestin IUD
f/u biopsy 3-6 mos
most common GYN malignancy in US*
endometrial carcinoma
RF of endometrial cancer*
nulliparity
early menarche + late menopause
chronic anovulation
obesity (endogenous estrogens), DM (IGFs), HTN (metabolic syndrome)
exogenous unopposed estrogens; tamoxifen
FH of colon, breast, ovarian, uterine cancer
hx of endometrial hyperplasia
increasing age
endometrial carcinoma protective factors*
smoking*
OC’s and combined postmenopausal HRT
physical activity
presentation of endometrial cancer*
Abnormal uterine bleeding – (bleeding after pre/menopause) (menorrhagia or metrorrhagia)
(one drop of blood in postmenopausal women NOT on HRT is NOT NORMAL)
dx: transvaginal U/S = thickened endometrial stripe >4 mm
endometrial cancer tx*
Hysterectomy is necessary w/ BSO (bilateral salpingo-oophorectomy) + pelvic node dissection
Stage 1 – total abdominal hysterectomy w/ BSO. May need post-op radiation
Stage 2,3 – TAH-BSO + lymph node excision w/ or w/o post-op radiation
Stage 4 – systemic chemo
Recurrence – high-dose progestin or antiestrogens
endometriosis definition
presence of endometrial glands and stroma at extrauterine sites
estrogen-dependent disorder
usually pelvis (#1 = ovaries, endometriomas = chocolate cysts - filled with old/dark/sludgy brown blood)
endometriosis presentation and progression
presentation: cyclic pelvic pain (1-2 wks before), severe dysmenorrhea, dyspareunia, infertility
1/3s: 1/3 better, 1/3 same, 1/3 worse
endometriosis RF*
nulliparity,
early menarche/late menopause,
short/long menstrual cycles,
FH,
mullerian anomalies,
taller/thinner/low BMI
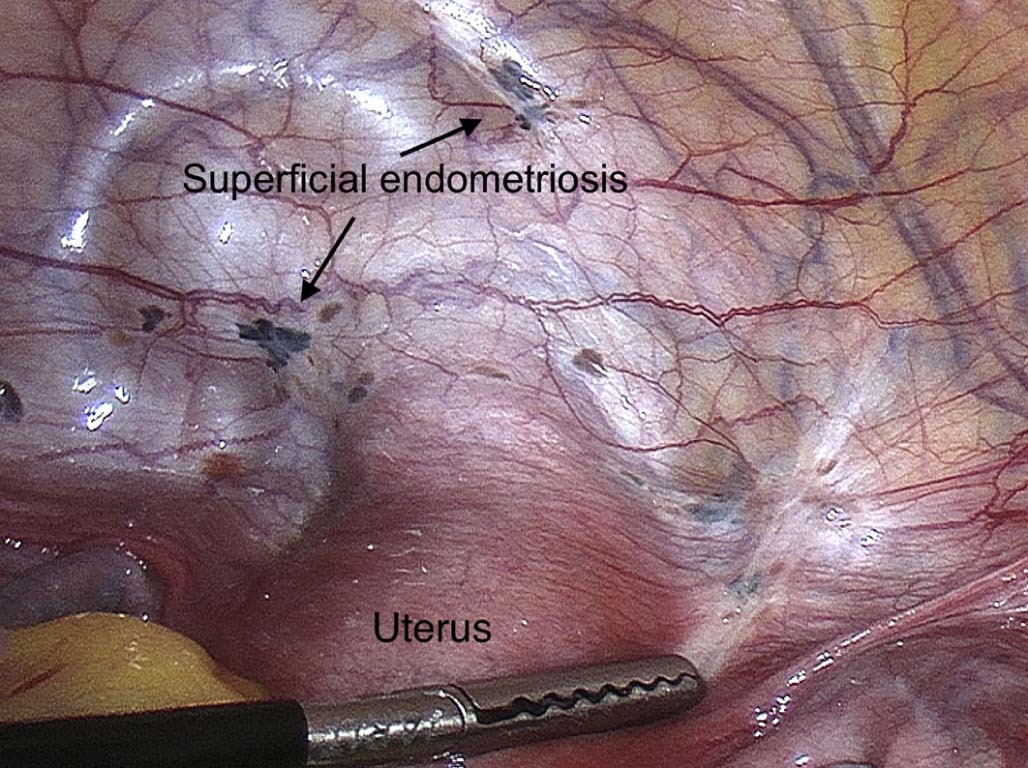
endometriosis appearance*
laparoscopy = reddish irregularly shaped, raised patches of thickened scarring or “powder burn”,
best diagnosed by direct visualization,
elevated CA-125 if PE consistent
there is an association with endometriosis with?*
ovarian cancer
first line tx for endometriosis
analgesia
others: hormonal therapy, surgery (if severe, won’t resolve, advanced)
adenomyosis summary
endometrial glands and stroma present within uterine musculature
dx: hysterectomy, MRI
heavy period, dysmenorrhea, pelvic pain
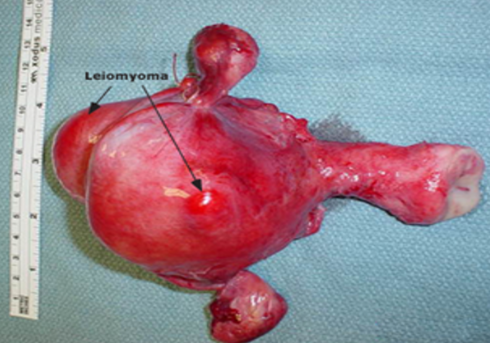
most common pelvic tumor in women and what does it NOT turn into
leiomyoma
do NOT often turn into leiomyosarcoma
sx of leimyoma*
abnormal uterine bleeding (heavy or long menses, NOT inter-menstrual or postmenopausal)
pelvic pressure + pain (bulk, dysmenorrhea, dyspareunia, torsion/degeneration)
reproductive dysfx (infertility, placental abruption, fetal growth restriction, preterm labor)
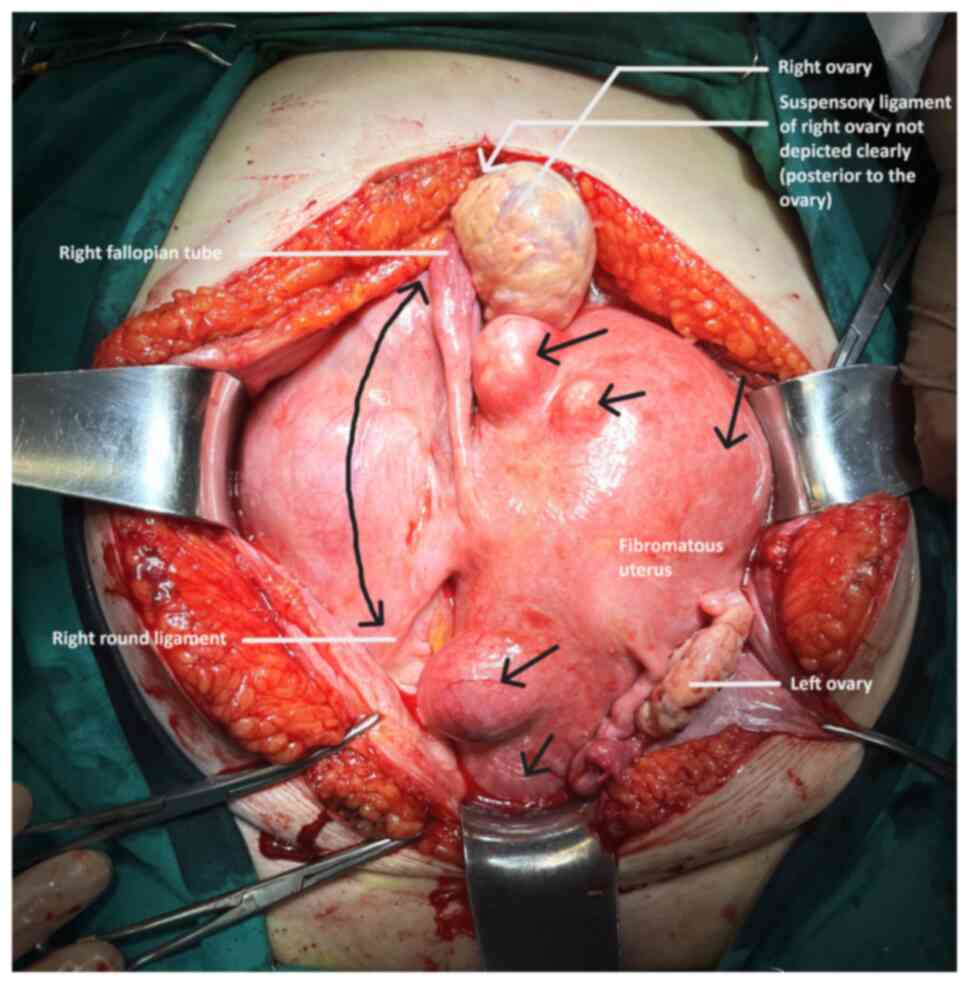
leiomyoma appearance*
pelvic exam = enlarged, mobile uterus w/ irregular contour, mobile mass
transvaginal U/S: focal heterogenic hypoechoic mass w shadowing
histology: whorled pattern of smooth muscle
RF for leiomyoma*
early menarche
nulliparity
black women
red meat/beer
OC’s do NOT promote growth of fibroids
fibroid location
submucosal - in the uterus
intramural fibroid - on top of the uterus
subserosal fibroid - “stalks” , attached to fibroid
leiomyoma tx*
no sx = no intervention
hormonal tx
gnRH agonist (pre-op to tx anemia + shrink fibroids)
surgery indicated for anemia, bulk sx, fertility problems (hysterectomy, myomectomy [preserves fertility], uterine artery embolization [no fertility])
PID definition
acute infx of upper genital tract structures
→ inflammation of uterus, ovaries, and infertility
pelvic inflammatory disease (PID) pathogens*
POLYMICROBIAL
chlamydia trachomatis
n. gonorrhea
gardnerella vaginalis
mycoplasma genitalium
poststrep
bacteroides
PID sx*
variable amounts of lower abd + pelvis, b/l
abnormal uterine bleeding, esp during/after intercourse
abnormal/heavy vaginal discharge w/ unpleasant odor
urethritis
proctitis
fever/chills
dyspareunia
painful/difficult urination
ASCENDING infx = cervicitis → endometritis → salping/oophor/ovarian → peritonitis
ascending infx for ob/gyn 2n1s
pelvic inflammatory dz (PID)
RF for PID*
adolescence
hx of PID
gonorrhea/chlamydia
male partners w gonorrhea/chlamydia
multiple partners
douching
IUD
OCPs
sequelae of PID*
ectopic pregnancy
infertility
chronic pelvic pain
leiomyoma
diagnostic criteria for PID*
at risk for STI, pelvic/lower abd pain, no other cause AND 1 more of the following:
cervical motion, uterine, or adnexal tenderness
lab tests NOT required but INC specificity
if you have uterine/adnexal/cervical motion tenderness → empiric abx therapy
more specific: high temp, abnormal cervical discharge, WBC on salin wet prep, elevated ESR or CRP, pos gonorrhea or chlamydia
PID tx
initiate fast → hospital
should improve within 72 hrs
outpatient: ceftriaxone + doxy
inpatient: 2nd gen ceph (cefoxitin/cefotetan) + IV doxy
screen + treat for chlamydia (>25 high risk, 1st tri preg)
tx partner for both c. trachomatis and n. gonorrhoeae
endometritis summary*
inflammation of endometrium
cause: PID from STD, invasive procedure, pp, FB, uterine issues, post-abortion
tx: clinda + genta OR ampicillin OR metro
beware of toxic shock sx! (cause: s. aureus or clostridium, clos = VERY LETHAL) = hypotension, high fever, multi organ involvement
causes of adnexal masses*
ovarian causes: endometrioma,
cysts (follicular, corpus luteum),
neoplasms,
carcinoma
non-ovary: ectopic pregnancy, hydrosalpinx, tuboovarian/diverticular/appendiceal abscess, fallopian tube cancer, IBD, pedunculated fibroid, pelvic kidney
FH breast, ovarian or colon cancer increases risk of
ovarian cancer
adnexal mass + mid-cycle pain suggests?
follicular cyst
→ U/S + pregnancy test → CA-125 and laparoscopy
adnexal mass + dysmenorrhea, dysparuenia = ?
endometriosis
→ U/S + pregnancy test → CA-125 and laparoscopy
adnexal mass + pain w/ fever suggests?
infx (PID, appendicitis, diverticulitis)
→ U/S + pregnancy test → CA-125 and laparoscopy