Fetal Urogenital System Abnormalities
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
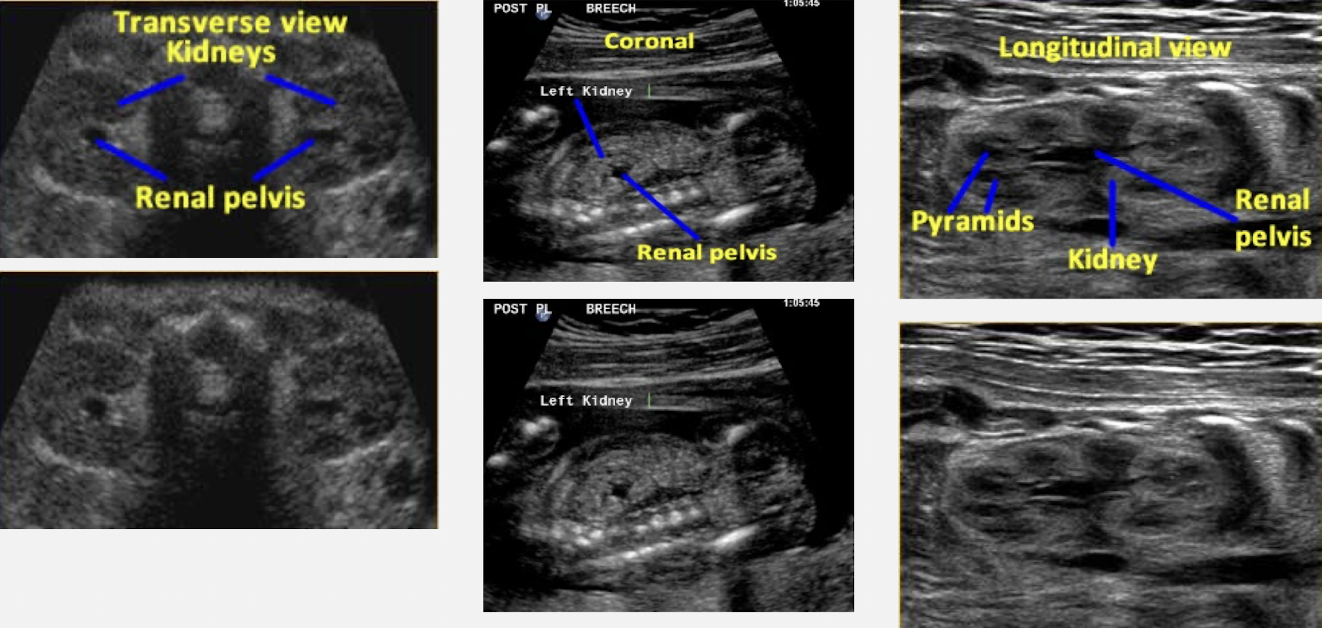
SONO: normal fetal kidneys
homogeneous corte
moderately hypoechoic cortex
hypoechoic pyramids and anechoic collecting system
kidneys are evaluated for:
size
collecting system dilation
appearance (texture and echogenicity)

renal agenesis (unilateral and bilateral)
complete absence of one or both kidneys due to failure of development
associated with genital anomalies and 2VC
unilateral agenesis:
MC than bilateral
excellent prognosis
bilateral agenesis:
lethal prognosis
exhibit classic Potter’s syndrome
oligohydramnios
pulmonary hypoplasia
associated with cardiac defects and MSK disorders
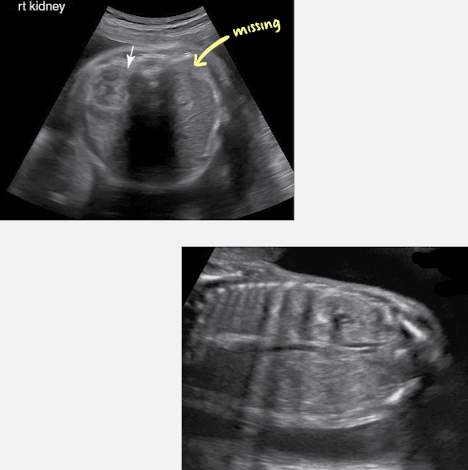
SONO: unilateral renal agenesis
absent kidney on one side
contralateral kidney → compensatory hypertrophy
ipsilateral adrenal: flattened; occupies renal fossa
absent ipsilateral renal artery branch
normal AFI
normal bladder
**sweep from chest to bladder to check for ectopic
SONO: bilateral renal agenesis
absent kidneys
adrenals: flattened within renal fossa
absent renal artery branches
bladder: not visualized; no urine (observe for 1 hours)
AFI: oligo- or anhydramnios
renal ectopia
kidney not positioned within renal fossa
usually lies in area of pelvis
crossed ectopia: both kidneys may be fused or appear to be fused
located on same side (usually right)
considered form of horseshoe kidney
prognosis: depends on presence of additional anomalies; generally good
associated with:
skeletal, GYN, GI, and cardiovascular anomalies

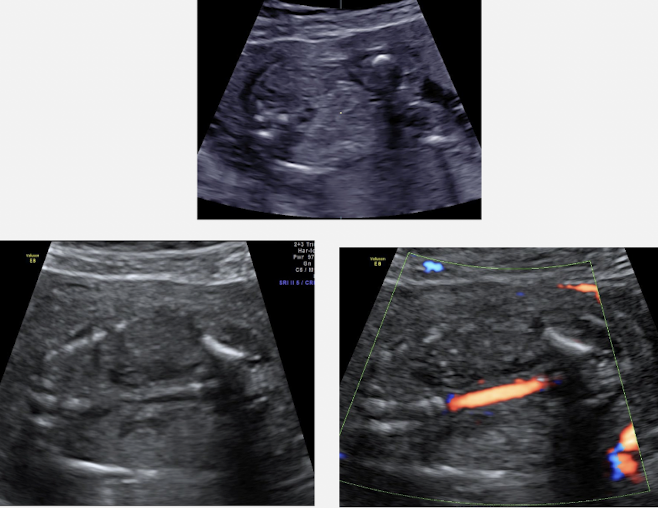
SONO: renal ectopia
absence of kidney in its normal position
ipsilateral adrenal gland flattening
ectopic kidney is usually in pelvis and may be malrotated
crossed ectopia and cross-fused ectopia is possible
horseshoe kidneys
inferior poles of kidney fuse while in pelvis
may be found as isolated anomaly or be associated with other anomalies or syndromes
isolated horseshoe kidneys carry good prognosis
incidence of trisomy 18 and 45, X
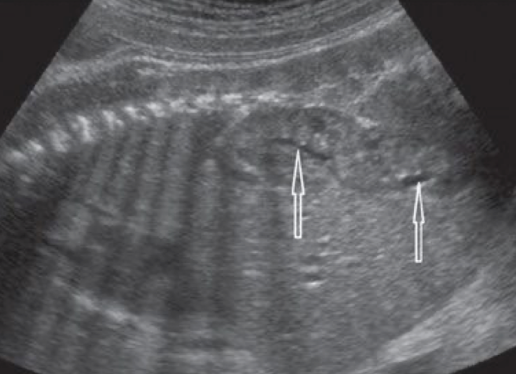
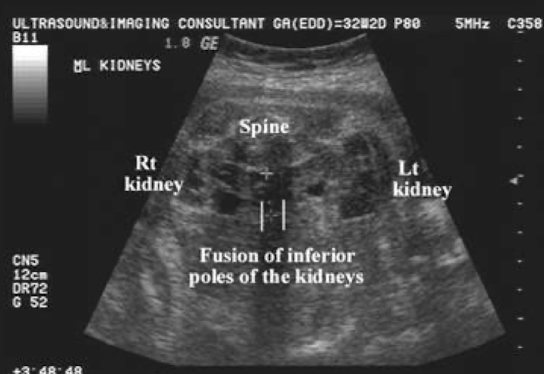
SONO: horseshoe kidneys
bridge of tissue connecting the lower poles
if spine down, connecting isthmus may be seen anterior to AO
**coronal view is ideal
autosomal recessive polycystic kidney disease
aka infantile PKD
autosomal recessive congenital disorder that affects both fetal kidneys and liver
characterized by:
numerous small cysts in both kidneys and liver
enlarged, nonfunctioning collecting tubules within the kidneys=renal failure
may be part of genetic syndrome—such as Meckel-Gruber or T13
prognosis: poor; decreased renal function and hypertension; death at an early age
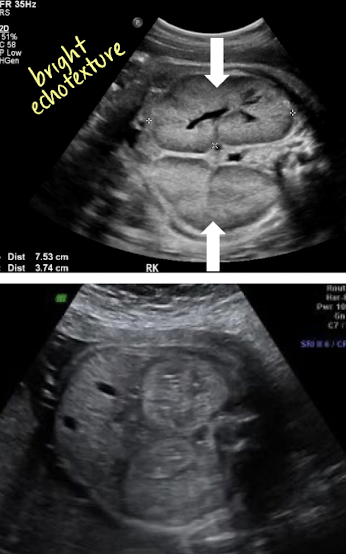
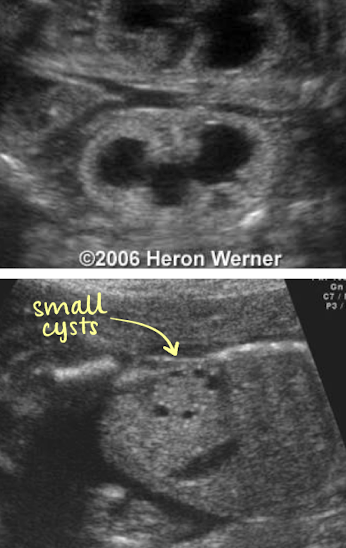
SONO: autosomal recessive polycystic kidney disease
bilateral, enlarged, echogenic kidneys
individual cysts not identified
kidneys are symmetrically enlarged
3-10x normal renal size for GA
AC will be large
bladder may be present or small
oligohydramnios
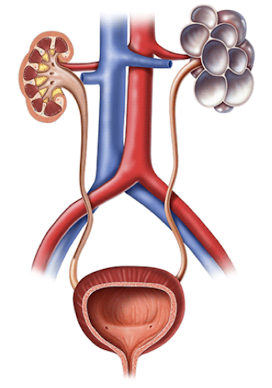
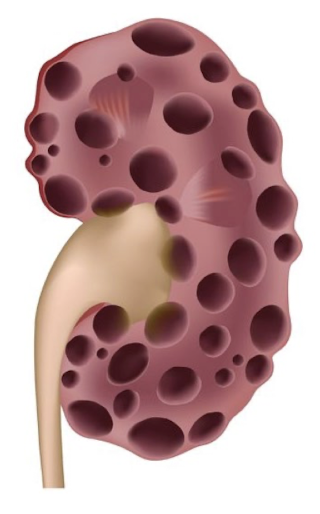
multicystic dysplastic kidney
characterized by:
cystic lesions that correspond primarily to dilated collecting tubules
cysts replace renal tissue (kidney doesn’t function)
cysts are nonfunctioning and noncommunicating
usually unilateral; can be bilateral
MC form of renal cystic disease in childhood
associated with Meckel-Gruber; CNS, GI, cardiac, and limb anomalies
prognosis
unilateral=excellent
bilateral=lethal
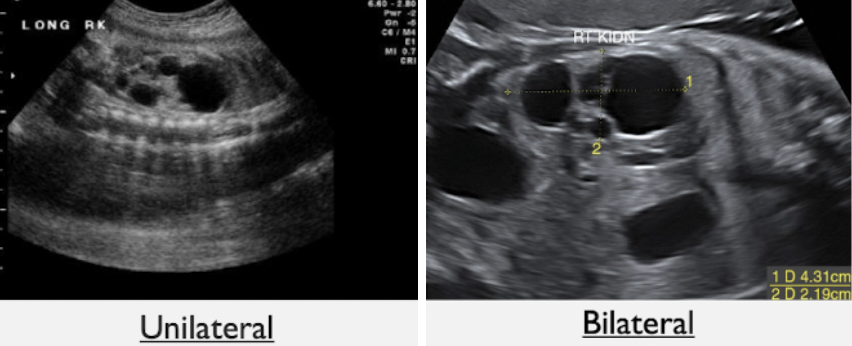
SONO: multicystic dysplastic kidney (unilateral vs bilateral)
unilateral
multiple, smooth-walled cysts of varying sizes
cysts do not communicate with each other
normal appearing contralateral kidney
bladder is visible
normal AFI
bilateral
multiple, noncommunicating renal cysts within both kidneys
failure to visualize bladder
severe oligohydramnios
autosomal dominant polycystic kidney disease
aka adult PKD
autosomal dominant congenital disorder that causes cystic dilation of nephrons and collecting tubules
macrocysts in kidneys, liver, and pancreas
may not be detected antenatally since it does not usually manifest until later in life
prognosis: variable when found in child
SONO: autosomal dominant polycystic kidney disease
bilateral (rare unilateral)
similar to ARPKD
symmetrically enlarged echogenic kidneys
amniotic fluid may be normal
unlike ARPKD, which has oligohydramnios
visible bladder
kidneys may look normal in 2nd trimester; follow up if family hx of ADPKD

obstructive cystic dysplasia
renal dysplasia occurs secondary to long standing kidney obstruction in the 1st/early 2nd trimester
leads to fibrosis and cystic replacement of renal tissue
if unilateral disease:
from UPJ or UVJ obstruction
variable prognosis: depends on additional anomalies
if bilateral disease:
from bladder outlet obstruction
poor prognosis b/c no AFI → renal failure and pulmonary hypoplasia
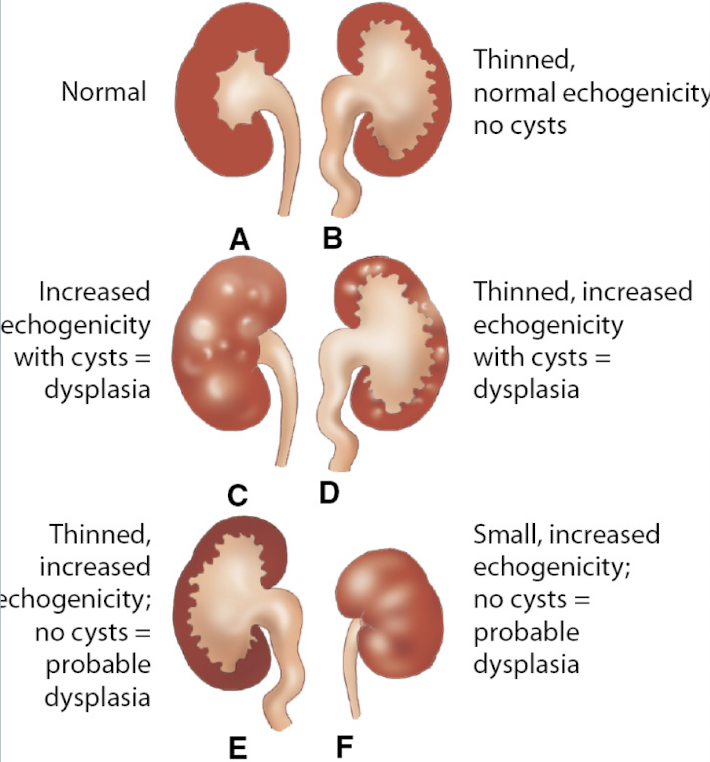
SONO: obstructive cystic dysplasia
echogenic kidneys containing peripheral cortical cysts
variable number/size of cysts
renal size can be small or enlarged
if bilateral disease from bladder outlet obstruction
thick-walled bladder; severe oligohydramnios
early disease may show hydronephrosis/hydroureter
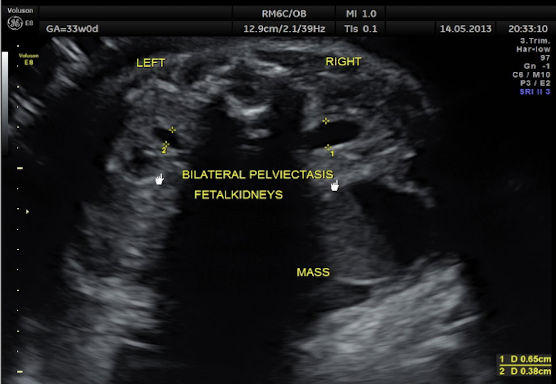
hydronephrosis
dilation of the renal pelvis in response to urine blockage
blockage in the ureter, bladder, or urethra
fluid-filled renal pelvis and calyces
MC fetal anomaly
unilateral or bilateral
associated with numerous conditions
prognosis depends on severity and underlying cause
SONO: hydronephrosis
dilated anechoic renal pelvis
measurement criteria:
measure renal pelvis in AP (TRV image, spine anterior)
<7mm=mild hydro
7-10mm=moderate hydro
>15mm=severe hydro
**sweep up and down in TRV to prove its kidney
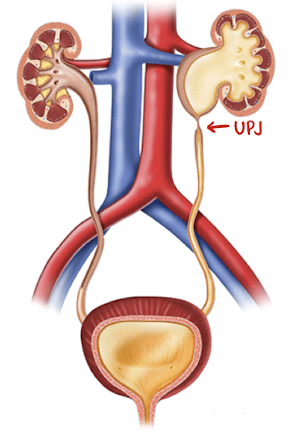
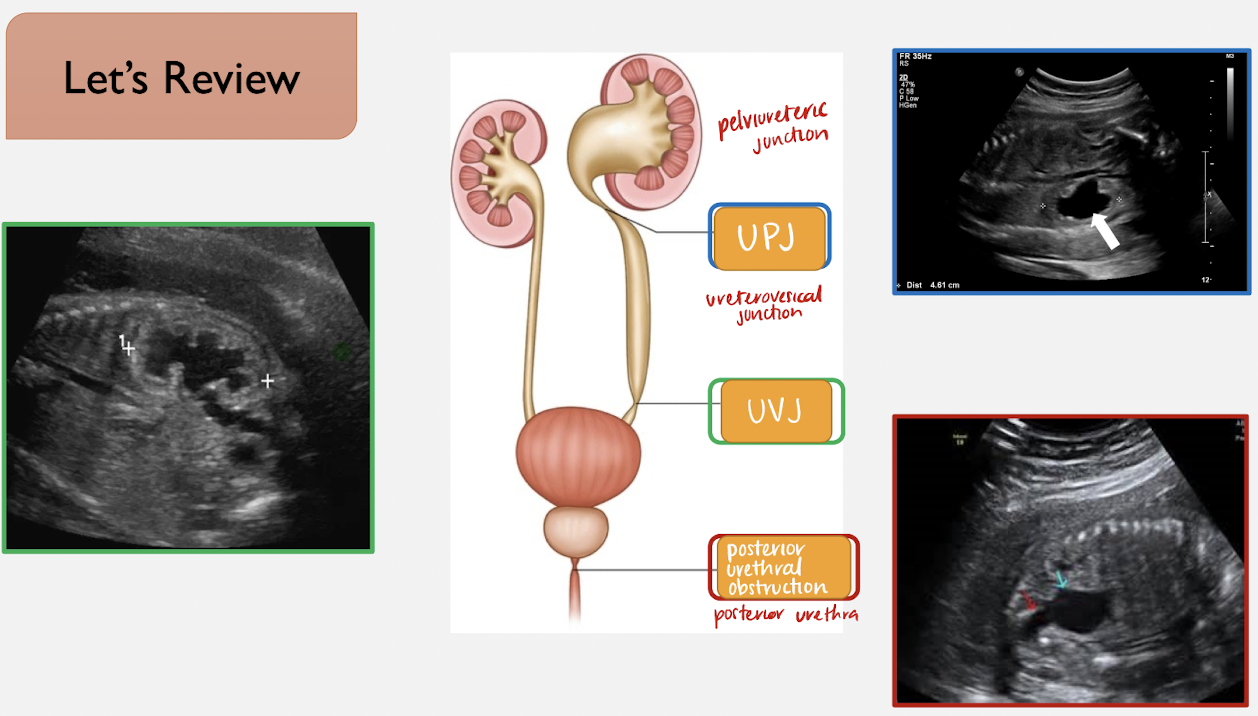
ureteropelvic junction obstruction (UPJ)
obstruction at the junction b/w renal pelvis and ureter
MC location for renal obstruction
MC cause of hydro in neonate
considered congenital hydronephrosis
MC male
usually unilateral
SONO: ureteropelvic junction obstruction (UPJ)
medial anechoic urine collection within renal pelvis that communicates with calyces (caliectasis)
moderate to severe hydronephrosis without hydroureter or bladder dilation
distended renal calyces connect with renal pelvis
enlarged kidney
if unilateral, bladder and AFI are normal
if bilateral, bladder will be empty and may have oligohydramnios
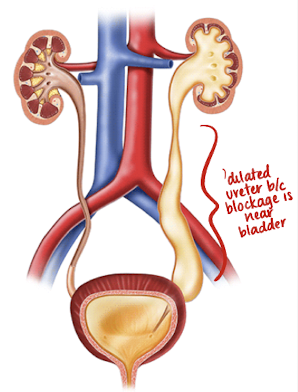
ureterovesical junction obstruction (UVJ)
obstruction at the junction of the ureter and bladder
hydronephrosis occurs secondary to obstruction
dilated ureter also forms: megaureter
possibly from ectopic ureterocele within bladder causing obstruction of upper pole of kidney
males?females (biological)
may be unilateral or bilateral
definitive diagnosis is made with VCUG or ceVUS
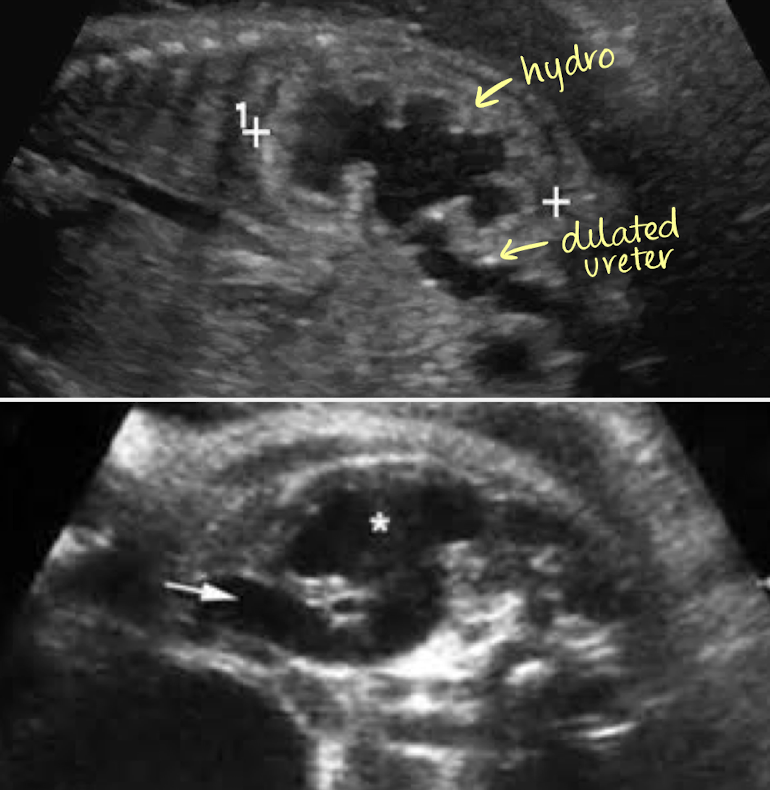
SONO: ureterovesical junction obstruction (UVJ)
affected kidney will have dilation of renal pelvis and ureter
ureter will appear tortuous
if unilateral, bladder and AFI are normal
if bilateral, bladder will be empty and may have oligohydramnios
posterior urethral valve obstruction
obstruction produced by abnormal congenital membrane within posterior urethra
leads to hydronephrosis, hydroureter, bladder dilation, and dilated proximal urethra
degree of obstruction can be complete, partial, or intermittent
MC urethral anomaly
occurs only in males (biological)
prognosis depends on severity of obstruction
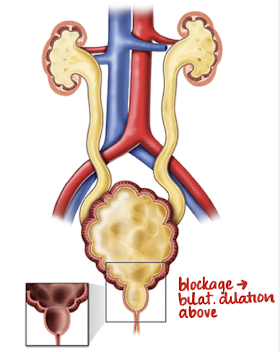
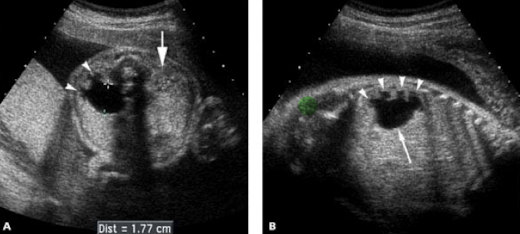
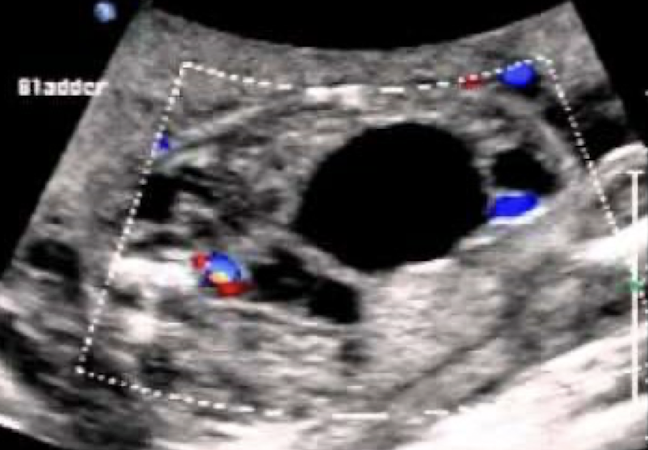
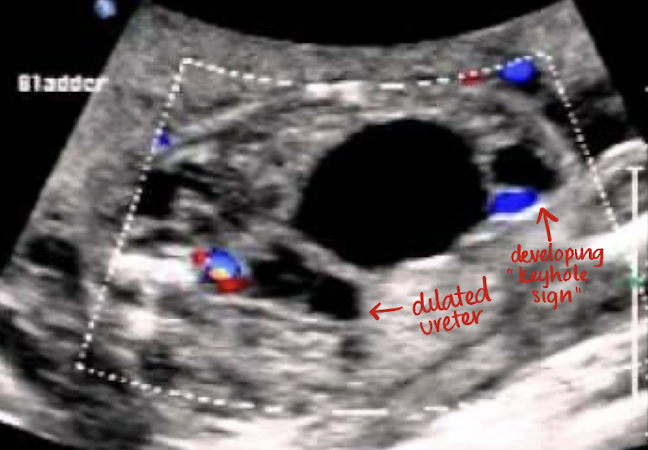
posterior urethral valve obstruction
bladder wall severely thickened with dilated posterior urethra
“keyhole sign”
bladder wall thickening
marked bilateral hydronephrosis and dilated tortuous ureters
occurs only in male fetuses
diminishing AFI

what do you see?
prune belly syndrome
aka Eagle-Barrett Syndrome
rare congenital disorder characterized by:
dilation of collecting system, cryptorchidism, and agenesis/hypoplasia of abdominal wall muscles
seen mostly in male fetuses
associated with megacystitis and posterior urethral valves
prognosis depends on severity and renal function
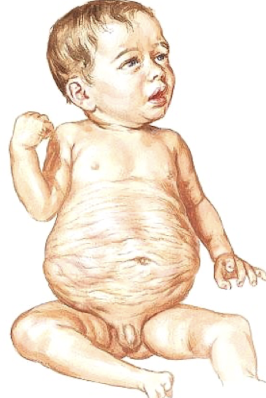
SONO: prune belly syndrome
hypoplastic/absent anterior abdominal muscles
protrusion of anterior abdominal wall
massively distended bladder
dilated, tortuous ureters
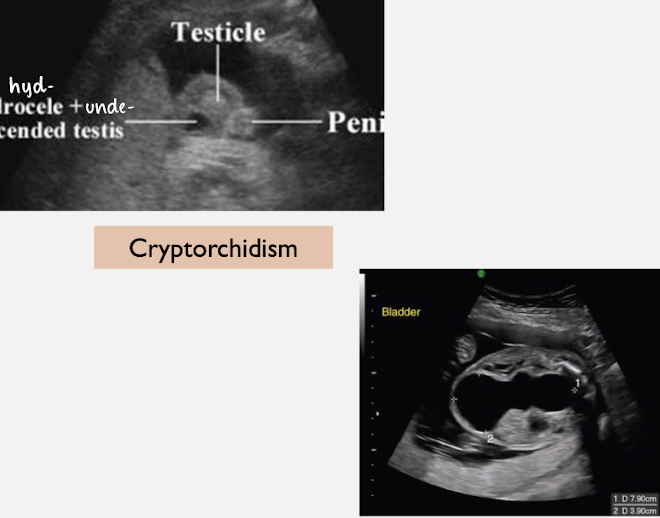
cryptorchidism
dilated prostatic urethra
kidneys may be normal, hydronephrotic, or dysplastic
ureterocele
cystic dilation of intravesical (bladder) segment of distal ureter
often found in duplex collecting systems
ureter attached to ureterocele in duplex collecting system drains upper pole of kidney as it enters bladder in more medial and caudal position (ectopic ureter)
females are more likely to present with ureteroceles
unilateral or bilateral
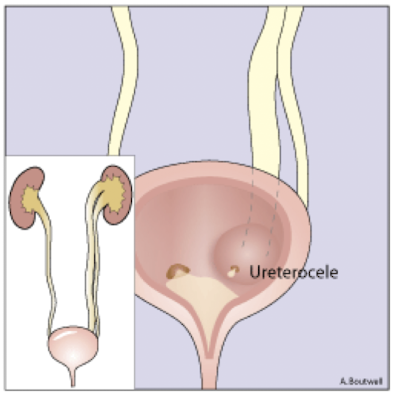
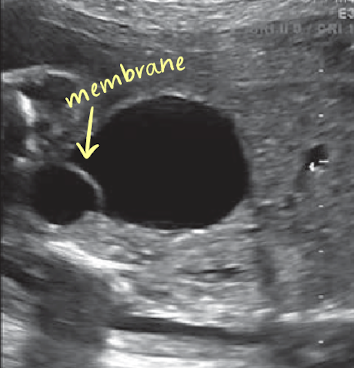
SONO: ureterocele
best visualized when the bladder is somewhat full
anechoic cystic surrounding by a thin echogenic membrane within the bladder
if bladder empty, ureterocele may be mistaken for small bladder
if bladder too full, ureterocele may be compressed
bladder should be evaluated multiple times through examination
possible renal duplication
fetal renal tumors
tumors of the fetal kidneys are rare
MC fetal renal tumor is mesoblastic nephroma (hamartoma)
benign tumor
composed of oddly arranged indigenous tissue
Wilms’ tumor is malignant renal tumor; MC in females
neuroblastoma is a malignant adrenal tumor

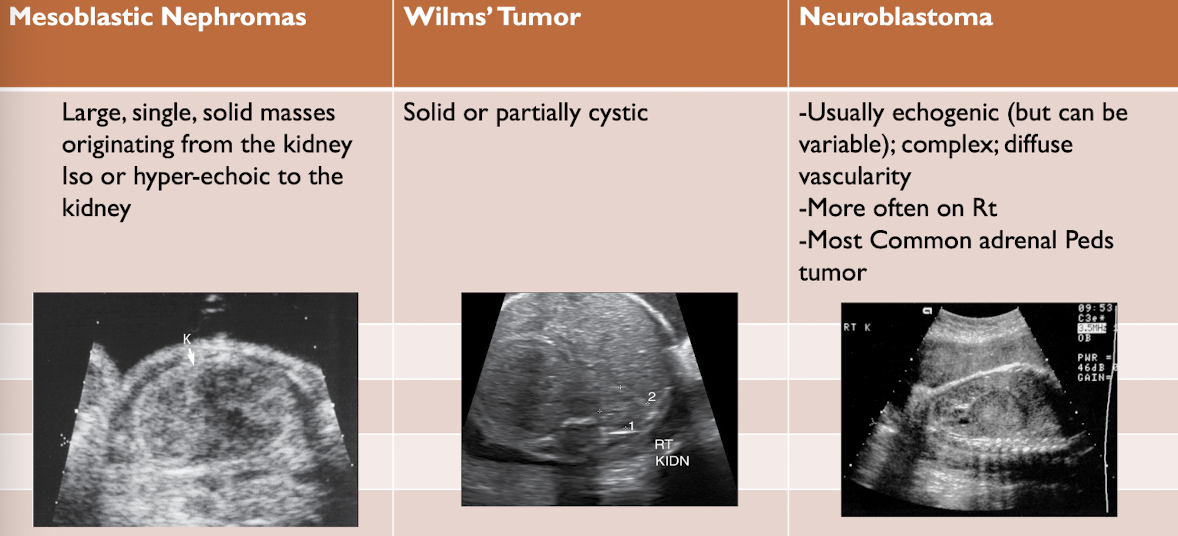
renal tumors
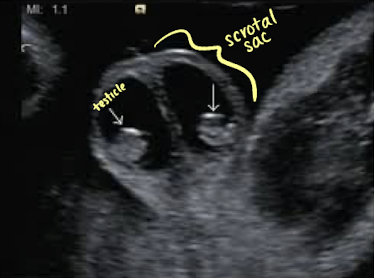
hydrocele
accumulation of serous fluid surrounding testicle, resulting from communication with peritoneal cavity
SONO: simple or complex
cryptorchidism (undescended testicle)
if descent interrupted or stopped testes will remain located within inguinal canal
referred to as undescended testes, or cryptorchidism
risk of torsion and development of cancer
scrotal sac with no testicular tissue
SONO: anechoic fluid seen in scrotum

hydrometrocolpos
obstruction of uterus and vagina resulting in collections of fluid (hydrometrocolpos)
from atresia/blockage of vagina or cervix, imperforate hymen, or abnormal membranes within vaginal lumen
masses may be predominantly cystic, may contain midlevel echoes, or may be fluid-debris levels
SONO: hypoechoic “cyst-like” ovoid mass posterior to bladder in area of uterus

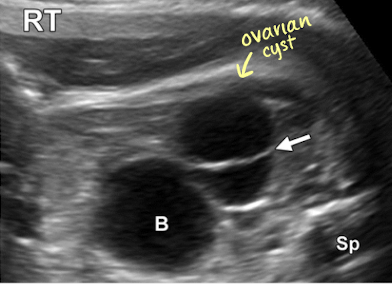
ovarian cyst
ovarian cyst that results from maternal hormonal stimulation
usually benign
typically represent normal functional ovarian cysts
MC cystic mass in female fetuses
can be unilateral or bilateral
most regress in utero or postnatally
have the potential to lead to ovarian torsion or rupture