ANA 873 Anesthesia Complications & MH
1/84
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
85 Terms
mortality
•Timeframe 24 hours to 30 days post anesthesia
•Coroner reports, surveys, malpractice
ASA risk mortality
mortality ASA 1 is 0.04 per 10,000 (0.0004%) anesthetics.
ASA physical status 2 risk is 0.5 per 10,000 (0.005%) anesthetics,
ASA physical status 3 risk is 2.7 per 10,000 (0.027%) anesthetics
ASA physical status 4 risk is 5.5 per 10,000 (0.055%) anesthetics
Morbidity
indicative of disase, incorporating any complication, excluding death, occurring during the perioperative period
most common events leading to injury in anesthesia claims included regional blocks (20% of claims), respiratory problems (17% of claims), CV(13% of claims), and equipment problems (10% of claims)’
morbidity classification
Minor morbidity: Moderate distress without prolonging hospital stay. No permanent complications (PONV)
Intermediate morbidity: Serious distress prolonging hospital stay or both. No permanent complications (e.g., dental injury).
Major morbidity: Permanent disability or complication (SCI;anoxic brain injury).
The incidence of adverse outcomes with minor morbidity is 18%-22%).
hoarseness has been cited to occur in 14% to 50% of patients and may accompany a traumatic lesion in the larynx or hypopharynx in 6.3% of patients.
Drug errors (0.1%), equipment malfunction (0.23%), PONV (10%-79%), and accidental dural perforation (0.5%-0.6%)
complications of anesthesia identify by ASA
Aspiration of gastric contents
● Failed intubation
● Esophageal intubation
● Other problems with the induction of general anesthesia
● Inadequate ventilation
● Airway obstruction
● Respiratory failure
● High spinal or massive epidural
● Neuraxial cardiac arrest
● Local anesthetic toxicity
● Drug reaction
● Anaphylaxis
● Overdose of sedatives
● Prolonged hypotension or hypertension
● intraoperative cardiac arrest during anesthesia of undetermined etiology
anesthesia related death by types of complications
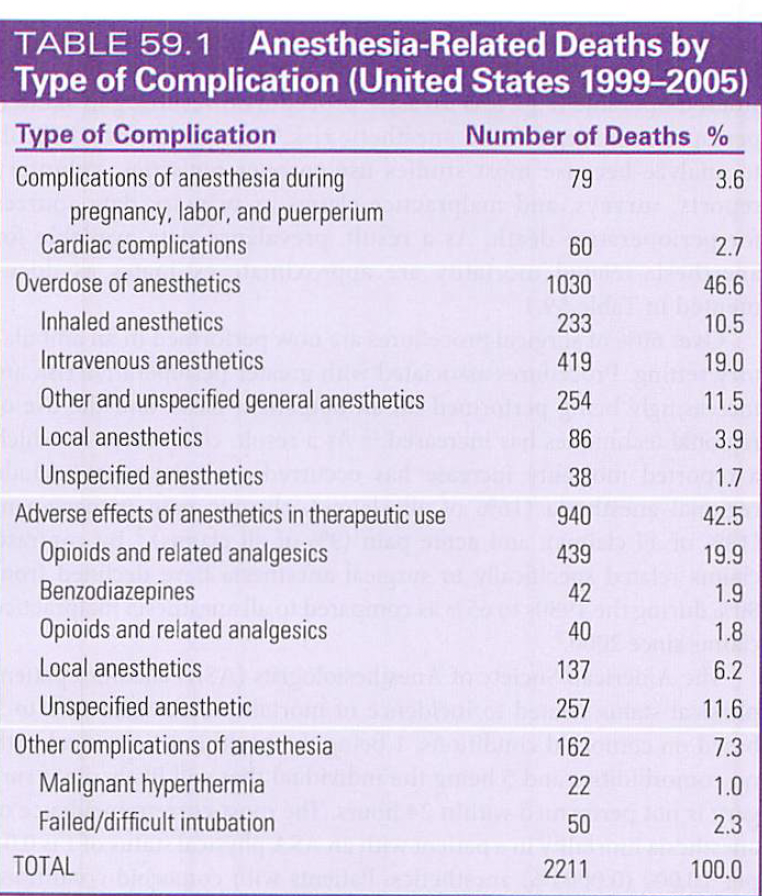
emerging areas of anesthesia M&M
perip hyman erro
partiureint and neonatla resusciation
acute and chronic pain
elderly >70 yrs
pediatric brain growth and development
Adults with CHD
intraop cardiac arrest
supraglotic device and ETT intubation
domains of frailty measurements 5
1. Unintentional weight loss
2. Exhaustion measured by assessing effort and motivation
3. Decreased grip strength
4. Slowed walking speed
5. Low physical activity
Common post op complications
laryngospasm/ bronchospasm
airway obstruction
desaturation
PNA
PE
Atelectasis
Reintubation/mechanical ventilation for >48 hrs
severe coughing
Stridor
pleural effusion
pneumothorax
resp infection/ aspiration pneumonitis
worsening of OSA
Acute or worsening resp failure
during induction- instrumentation phase
dental injury with largynoscopy
cerical (cornea) injury
Soft tissue trauam (OA)
bloody airway (laryngospasm)
lip injury
During induction- intubation
Esophageal (Unrecognized)
Right Main stem
Aspiration
Bronchospasm
Laryngeal spasm
airway managmenet complications- mask ventialtion
Mucosal, skin irritation, conjunctivitis caused by cleansing agents
● Soft tissue damage from excessive pressure
● Corneal abrasion, retinal artery occlusion, blindness
● Damage to mandibular branch of facial nerve causing transient facial nerve paralysis
● Damage to mental nerves causing lower lip numbness
● Broken teeth, mucosal tears
● Worsening obstruction from malposition of tongue
● Subtuxation of the temporomandibular joint
● Gastric distention increasing risk for aspiration
● Gastric rupture
● Subcutaneous emphysema
Airway management complications LMA
Folding of epiglottis tip causing labored breathing, coughing, laryngospasm, and obstruction
● Excess lubricant that causes coughing or laryngospasm
● Lack of protection from aspiration of gastric contents
● Laryngospasm. coughing
● Sore throat
● Increased intracuff pressures with prolonged procedures with NO and CO2
● Dysarthria
● Edema of epiglottis, uvula, posterior pharyngeal wall
● Hypoglossal nerve paralysis
● Postobstruction pulmonary edema
● Tongue cyanosis
Airway management complications- ETT 13
Damage to teeth
Mucosal/ Lip injuries
Swelling tongue
Sore throat
Trauma to larynx/vocal cords
Arytenoid dislocation/subluxation
Tracheobronchial trauma/ Barotrauma
Nerve injury
Cervical spine injury
Vocal cord paralysis
Temporomandibular joint injury
Laryngospasm/ Bronchospasm
Hemodynamic perturbations
Airway management complications- extubation
Hemodynamic perturbations
Laryngospasm
Laryngeal edema
Bronchospasm
Negative-pressure pulmonary edema
Aspiration
Airway compromise
Difficult/accidental extubation
intraop awareness
High-risk cases (e.g., trauma, obstetric, CV
tachycardia and hypertension
hearing unwanted conversations and remembered bright lights during their procedure inconsistent with their expectations, making them distraught.
could lead to complications of awareness, PTSD, future surgery apprehension, and enhanced medicolegal risks associated with anesthesia.
Postoperative sequelae reported related to PTSD include sleep disturbances (19%), nightmares (21%), fear of future anesthetics (20%), and daytime anxiety (17%).
assessing incidence of awareness
Modified Brice Interview
● What was the last thing you remember before going to sleep?
● What is the first thing you remember after waking up?
● Do you remember anything between going to sleep and waking up?
● Did you dream during your procedure?
● What was the worst thing about your operation?
Risk Factors for Awareness 9
Female sex
Age (younger adults, but not children)
Obesity
Clinician experience
Previous awareness
After normal hours of operation
Emergency procedures
Type of surgery (obstetric, cardiac, thoracic)
Use of nondepolarizing relaxants
What is bronchospasm and what are 3 causes
Spasmodic contraction of smooth muscle
Causes:
Histamine Release
Reflex bradycardia (PNS stimulation w airway manipulation)
medications:
Muscle relaxants (Sch, Rocuronium)
Non-selective BB- (block beta2) (Propranolol)
Anticholinesterases (neostigmine) counteract muscarinic choline receptor effects
Prostaglandin inhibitors
bronchospasm risk factors 4
Reactive Airway Disease (Asthma, COPD)
Pediatric
Recent URI
Atopy (eczema, hay fever)
Cigarette smoke
Bronchospasm clinical signs 7
Wheezing
Prolonged expiration
Reduced (or absent) lung sounds
Increased airway pressure during PPV
decreased pulmonary compliance
Decreased SPO2
Decreased ETCO2 or upsloping wave (obstructing pattern)
Hypotension
bronchospasm prevention
Delay 2 weeks after URI
Continue & consider: Preop inhaled beta agonist & inhaled corticosteroid
Adequate depth of anesthesia
IV induction preferred (Propofol & Ketamine bronchodilators)
IV Lidocaine MAY help
Avoid endotracheal intubation, if possible
LMA, mask ventilation, regional
bronchospasm treatment
Remova cause
#1 -Manual ventilate 100% FiO2
Auscultate, Confirm ETT placement / patency
r/o mucous plug, kink, tensions pneumo, PE
#2 -Deepen anesthesia
Volatile Agent
Bolus: Prop, Ketamine, Lidocaine
#3 -Albuterol (Beta 2-agonist) 8-10 puffs
#4 -Epinephrine IV
Magnesium or steroids
what is laryngospasm
Sustained & involuntary contraction of laryngeal muscles causing closure of vocal cords
Inadequate ventilation d/t airway obstruction
May involve false vocal cords / supraglottic soft tissue
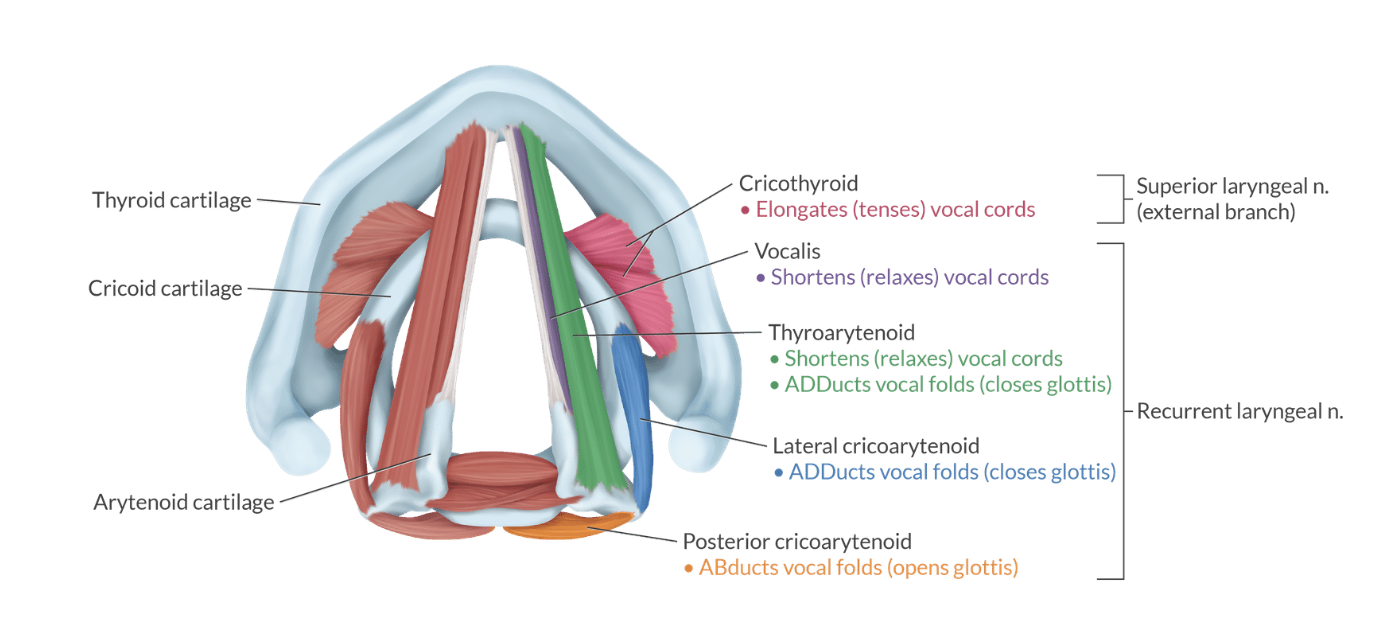
match intrinsic larynx muscle with fxn
thyroarytenoid= (shortens) “They Relax”
cricothyroid= tenses/ elongates “cords tense”
posterior cricoarytenoid= ABducts
lateral cricoarytenoid= ADDucts
laryngospasm reflex includes
Afferent limb:
Internal branch of the superior laryngeal nerve
Sensory only
Efferent branch consists of:
Recurrent laryngeal nerve
Innervates vocal cord adductors -
Lateral cricoarytenoid
Thyroarytenoid
Transverse (interarytenoid)
External branch of the superior laryngeal nerve
•innervates the cricothyroid muscle
•Adjusts cord tension (pitch) only
•Does not adduct cords
“Triggered by the internal SLN, executed by the RLN"
(RLN= Real reflex, Locks, No Air)
•Blocking the internal SLN decreases afferent stimulation so decreased laryngospasm risk
•Succinylcholine works because it relaxes RLN‑innervated intrinsic adductors
•Cricothyroid tension is not what closes the cords in laryngospasm
Larynospasm risk factors
Light anesthesia (induction / emergence)
Airway irritation [Manipulation (suction), Secretions, blood, bile, Volatile agents (des > sevo)]
Reactive airway (Asthma, URI, smoker)
Obesity / OSA
laryngospasm clinical signs
Inspiratory stridor (squeak)
No ETCO2 waveform
Paradoxical breathing movements
Supraclavicular retractions / rocking boat
Rapidly decreasing SPO2
NPPE
laryngospasm complications
airway obstruction
Negative Pressure Pulmonary Edema (NPPE) risk
Negative pulmonary pressure develops after spontaneous ventilation against a closed glottis, presenting with pink, frothy sputum and decreased oxygen saturation leading to acute respiratory failure.
aspiration of gastric contents
dysrhythmias
cardiac arrest
death
laryngospasm prevention 4
Propofol induction
Lidocaine before extubation (1-2mg/kg IV, 4mg/kg vocal cords)
Magnesium bolus (15mg/kg before extubation)
Removal of blood & secretions
laryngospasm treatment 3
#1 -FiO2- 1.0
remove noxious stsimuli
deepen anesthesia
#2 -Continuous PPV 5-10cmH2O, chin lift & Larson's maneuver
bilateral inward anterior pressure
#3 - Succinylcholine
adult and child IV= 1mg/kg
adult and child IM= 4 mg/kg
neonate/ infant IV= 2 mg/kg
neonate/infant IM= 5 mg/kg
if <5 yrs= give atropine 0.02 mg/kg
(0.2mg/kg IV or 4-5mg/kg IM) (Propofol 0.5mg/kg IV)
valsalva maneuver
exhalation against closed glottis or obstruction
pressure applired 3-5 seconds, released 5-10 sec
Ex. coughing, bucking, bearing down
risk= increased pressure in throax, abdomen, and brain
Muller’s maneuver
inhalaiton against closed glottis or obstru tion
Ex. patient bites down on ETT and takes deep breath
RIsk= substmospheric pressure in throax→ negative pressure pulmonary edema
CV complications during maintenance phase
MI
Oxygen carrying capacity
Blood pressure control
Factors that can cause hypotension: 4
Decreased contractility
Decreased SVR
Decreased preload
Dysrhythmias
Multisystem complications
Thermoregulation (Hyper & hypothermia)
Kidney perfusion
Position diligence
Intraop MI risk factors 5
70% mortality rate
Age: 51-70 years old
ASA 3 & 4
Males > Females
General > Regional
Excessive surgical bleeding in 70% procedure related deaths
Intraop anesthesia CV complications
Co-morbidities
MI, Angina, CHF pre-op predictors
Inadequate risk assessment
Inappropriate anesthetic management
Human error / misjudgment
What is the strongest predictors for increases risk for periop MI & increased risk of postop death
Ischemic heart disease (previous MI or angina) and CHF
Thermoregulation- hypothermia
Redistribution of heat from core to vasodilation
defined as temp <36 C
age extremes greatest risk of periop hypothermia
*1-1.5 C degree decrease in first hour
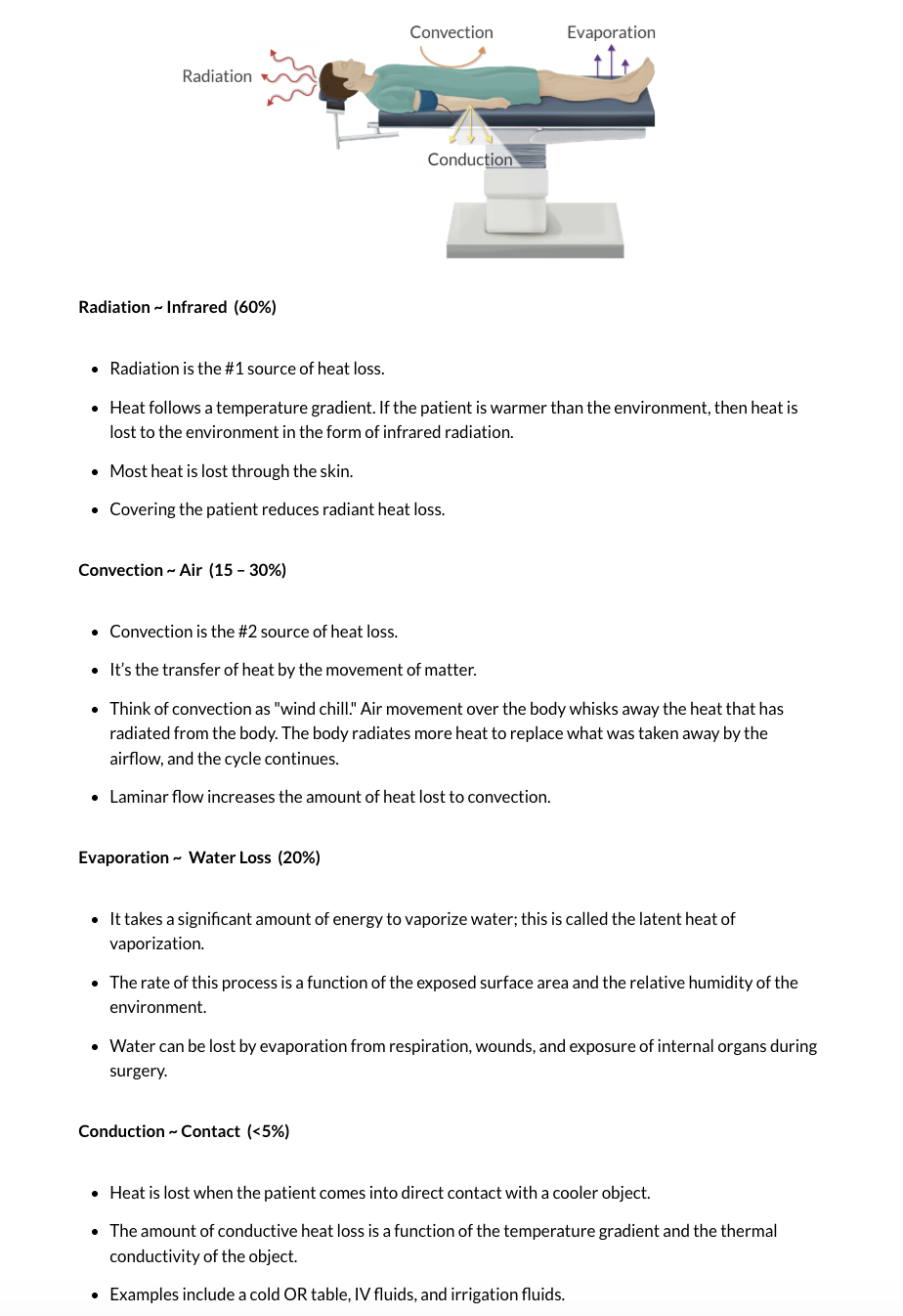
Radiation - Loss to environment through radiation - most significant
Convection – Loss to air currents 2nd most significant
Conduction – Loss from physical contact
Evaporation – Loss from transfer of liquid to gas
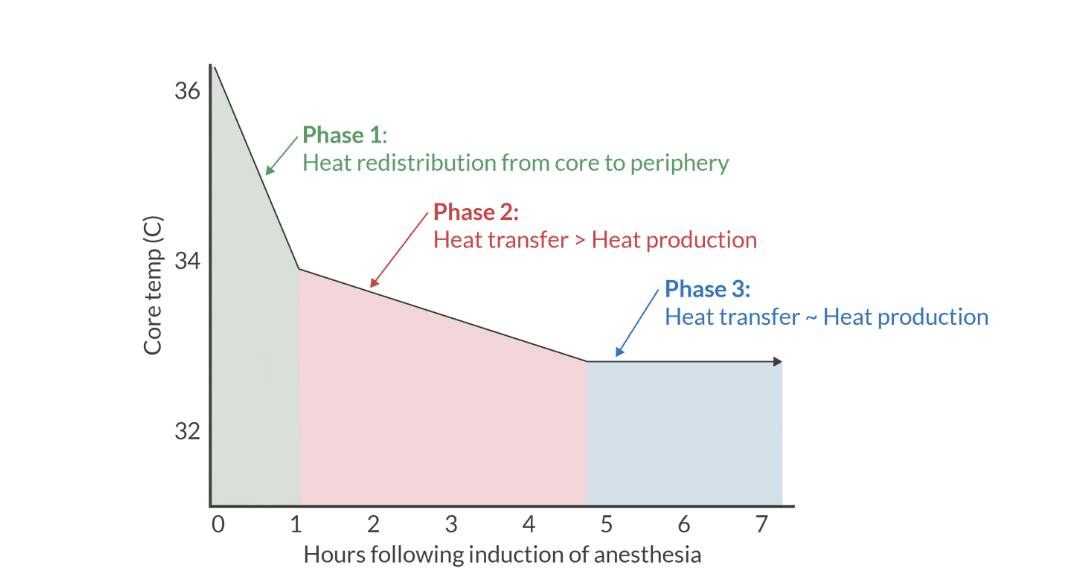
3 stages of intraop heat transfer
phase 1 heat redistribtuion from core to periphery
phase 2: heaat transfer? heat production
phase 3: heat tx- heat production
phase 1
with general, spinal, or epidural, there is redistribtion of heat fro central comparement (thorax, abdomen) to heripheral comparement (extremeities and skin)
anesthethic agensts impair thermoregulatory response in hypothalmauc, revnet shivering, and cause vasodilation
only nominal amount of heat loss to enviornemnt during phase 1. agai heat redistrubtion is way more importnat durign this phase
simple interventions, warm blanket on patient before OR, minimizes centrla to pheriapher temperature gradient and goes a long way towards preserving core temp
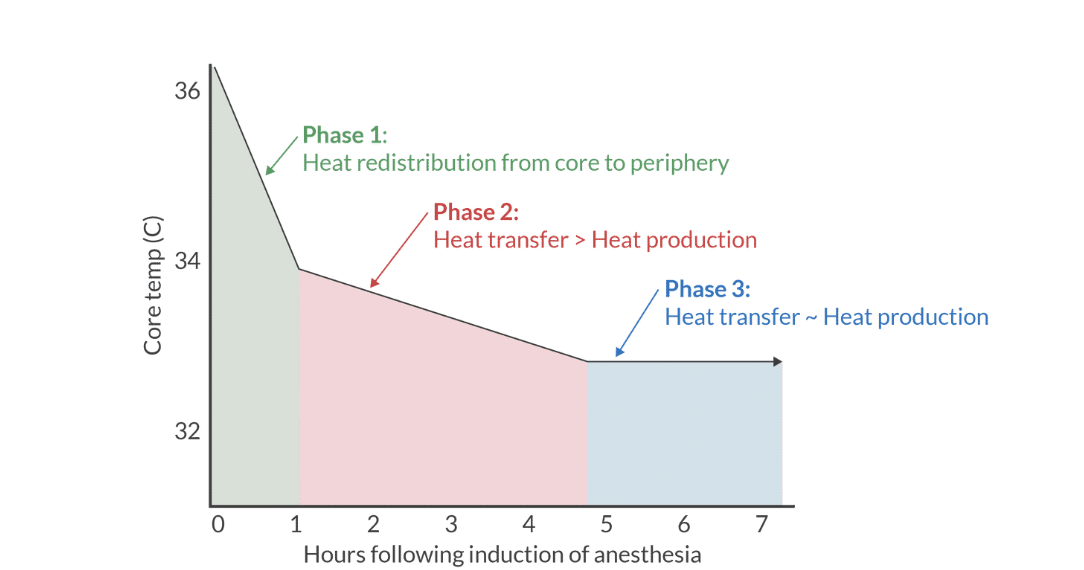
phase 2
heat loss ot evnrioenemnt exessed heat production
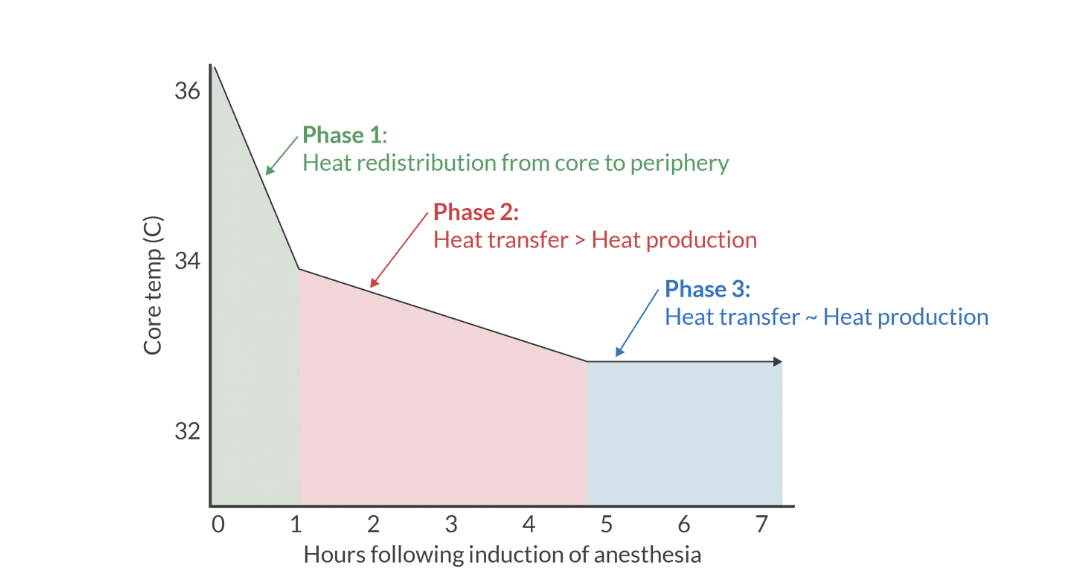
phase 3
an equilibrium develops between heat loss to environment and heat production
periop events contributing to heat loss
recalibration of hypothalamic set point
drug-induced vasodilation
impaired shivering
core to pheripahrl temp redistribution
cool ambient temp
cold OR table
amdin room temp fluids and cold blood products
Hypothermia adverse events
Coagulopathy
Impaired PLT aggregation
Reduced coagulation cascade enzyme activity
Prolonged drug effects (esp NDMR
Hypothermia complications
Delayed emergence
Myocardial ischemia
Sympathetic stimulation
Post operative Shivering
Increased oxygen demand —> Increases myocardial workload
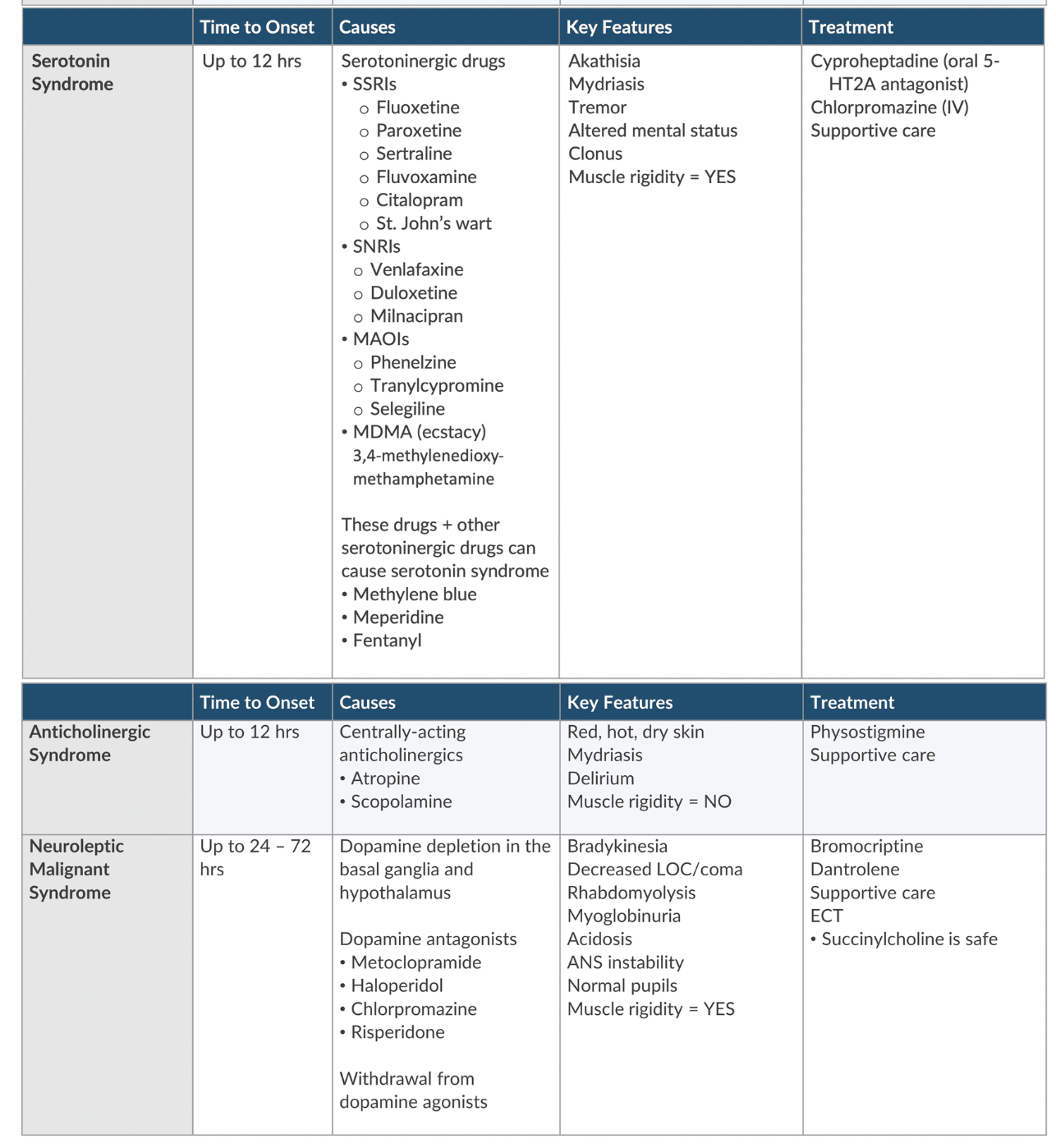
hyperthermia causes
Environmental (warming device)
Drug reactions
Neuroleptic malignant syndrome- dopamine depletion
Serotonin syndrome- excess 5HT activity
Anticholinergic toxicity- an excess Ach blockade
Thyroid Storm
Transfusion reaction/infection
Malignant Hyperthermia
Hyperthermic syndromes tx
Neuroleptic malignant syndrome- bromocriptine, drantrolene
Serotonin syndrome- cyproheptadine
Anticholinergic toxicity- physostigmine
hyperthermia complications
Increased metabolic rate
Increased myocardial oxygen consumption
Ocular injuries & postoperative blindness risk factors
•Intraoperative hypotension
•Male sex
•Obesity
•Anemia from blood loss greater than 1 liters
•Surgery greater than 5 hours in duration
•Use of a Wilson frame
•Decreased percent colloid administration.
ocular injuries are more common in
older adults. Most common in nose, neck, sinus, spine surgeries
corneal abrasions
•Eye pain
•Tearing / photophobia
•Foreign body sensation
•Pain increased with blinking and ocular movement
•Present immediately after emergence
Anterior ischemic optic neuropathy- know
•Sudden, painless vision loss, usually unilateral
•Typically post-op day #1
•Temporary reduction in blood flow to the vessels supplying anterior portion of optic nerve
•Shows optic disc swelling= EXAM
Posterior ischmeia optic neuropathy- know
•Reduction of oxygen supply to retrolaminar aspect of optic nerve
•Delayed, painfree vision loss (24-48 hrs, even weeks)
•Bilateral blindness common
•Less common than AION
bone cement implantation syndrome
There are several proposed mechanisms of bone cement implantation syndrome, including: Bone marrow debrisembolization during pressurization of the femoral canal Toxic effects of incompletely mixed methyl methacrylate, resulting in the release of the monomer Activation of inflammatory cytokines with femoral reaming, resulting in the release of microemboli.
The emboli move into the pulmonary circulation with the subsequent release of vasoactive mediators, causing an abrupt increase in pulmonary vascular resistance. This can lead to right heart failure and circulatory collapse
Bone cement implantation syndrome
After methyl methacrylate is injected into the femur:
•Acute hypotension
•Decreased oxygen levels
•Bronchospasm
•Decline in end-tidal carbon dioxide
•Cardiac dysrhythmias
•Increased pulmonary vascular resistance --> right failure and cardiac arrest
Initial indicators of bone cement implantation syndrome
• Awake (under spinal anesthesia), dyspnea and altered mental status are the initial indicators
General anesthesia, the first sign is a decrease in end-tidal carbon dioxide.
high risk for BCIS
hip arthroplasty is highest risk
other high risk: knee arthroplasty, vertebroplasty, and kyphoplasty
bone cement implantation syndrome tx
first line: 100% O2
Supportive
IV fluids
vasopressors- phenylephrine
adequate ventilation and oxygenation
bone cement implantation syndrome risk factors
presence of metastatic disease,
a previous femoral prosthesis
preexisting pulmonary hypertension or right heart failure,
and the use of large volumes of methyl methacrylate cement
Pneumoperitoneum Insufflation- resp implicatins
•Decreased Functional Residual Capacity (FRC)
•Decreased Respiratory Compliance
•Increased Peak Airway Pressure
•Increased V/Q mismatch
Pneumoperitoneum Insufflation- cardiac implications
•Increased SVR
•Increased Mean Arterial Pressure
•Vagal response = bradycardia
•Decreased Cardiac Output
Pneumoperitoneum Insufflation- tx
•Preop Volume loading
•Slow / lower insufflation pressures
Peritoneal insufflation
an increase in SVR and MAP due to compression of the abdominal aorta and increased afterload.
Hypotension response more profound with positive pressure ventilation or positioning such as reverse trendelenburg.
Tourniquet standards
1.Width minimum half the diameter of limb
2.Insufflate 50-100 mmHg above SBP
3.Increase risk of limb loss after 2 hours
4.Hypotension with deflation typical
tourniquet duration and safety
Insufflation safely for 2 hours
0-2 hrs increasing pain
2-3.5 hrs Nerve and Muscle injury
3.5 - 5 hrs Widespread muscle & Nerve damage
5+ hrs. Severe effects with systemic involvement
Cardiac – hypotension/arrhythmias
Renal – AKI from myoglobin proteins
when deflating tourniquet cuff
several physiological events occur,
transient metabolic acidosis
Increased carbon dioxide levels
drop in systemic blood pressure.
MH DX
unexpalined increased ETCO2
fever
tachycardia
cyanosis
rigity
failure of massesster musle to relax (trismus)
What elecrtrolytes effected in MH
increases
H
K
Ca2+
CO2
Decreased
O2
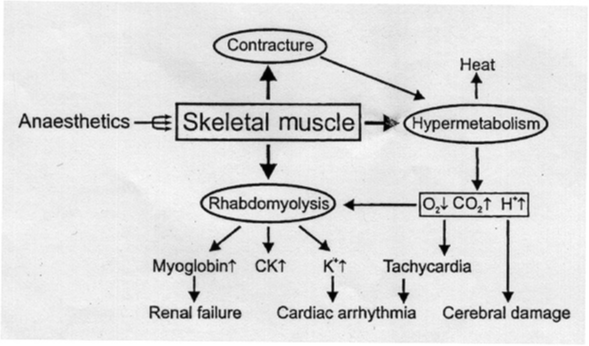
MH physiology
Ryanodine (RYR1) mutation
Autosomal dominant inherited trait= EXAM
Sometimes random mutation (Mayo Clinic,2022)
Skeletal Muscle Hypermetabolism
Excessive Calcium release from the Sarcoplasmic Reticulum—> Increased intracellular calcium leads to sustained contractions with increased metabolsim
MH triggers
Halogenated Anesthetics (Iso, des, halothane, enflurane, sevo)
Depolarizing muscle relaxants (Succs)
Physiological stressors
Extreme heat
Strenuous exercise
WHAT IS NOT A TRIGGER FOR MH
N2O
MH S/S 11
None until exposed to trigger
Trismus( masseter spasm) 50%
Whole body muscle rigidity 75%
High body temperature
Tachycardia & tachypnea
from SNS stimulation secondary to hypermetabolism & hypercarbia
tachycardia is 2nd sign
Increased ETCO2/ Decreased pH
Combined metabolic and respiratory acidosis
Cardiac arrhythmia
Renal Failure
HyperK
Cyanosis
what is earliest, most senstiive and specific sign of MH
elevated ETCO2
how fast can temp increase in MH
1-2 C q 5 min
know
MH risk factors
Family History of Malignant Hyperthermia (MHAUS, 2024)
autosomal dominant inheritance pattern
children and siblings of a patient with MH susceptibility usually have a 50% chance of inheriting a gene defect
Exposure to Succinylcholine or Inhaled Anesthetics
Associated susceptibility disorders (Watt & McAllister, 2023)
Central Core Disease (rare, non-progressive myopathy)
King-Denborough Syndrome (rare myotonia)
current safe anesthetic practice
First Case of the day
Fresh anesthetic circuit and 20 min 100% oxygen flush
Benzodiazepines and Nitrous Oxide are safe
TIVA Propofol anesthetic w BIS monitor
No Succinylcholine
No Halogenated Inhaled agents
current helath practice for dx
Contracture Caffeine – Halothane test
Gold Standard, controlled setting
Sensitivity: close to 100%
Specificity: 80%
Genetic testing only 50-86% of MH affected individuals
Very low sensitivity
Gene sequencing mutations from DNA (Yang et al., 2020)
RYR1 (48)
CACNA1s (2)
Triggering event
MH tx
Notify MH Hotline for help (1-800-MH-HYPER)
Dantrolene (Dantrium, Revonto, Ryanodex)
Suppresses the calcium release from SR
Only disease-specific drug available (Yang et al., 2020)
Mortality rate from 70% down to 9.5% after Dantrolene
Body Cooling interventions (Ice Packs, Cold IVF, Gastric Lavage)
Hyperventilate with 100% oxygen
Bicarbonate 1-2mg /kg as needed
Treat arrhythmias (no Calcium Channel blockers)
Mortality Rate 3-5% (Watt & McAllister, 2023)
8 initial management for MH
DC inahled anesthetic and succs
hyperventilate with 100%
admin dantrolene (dosing based on HR and temp)
tx acidosis with Na bicarb (1-2 mM/kg)
Lower body temp to 38 C with external ice packs, gastric lavage
replace anesthethic cirut and cannister
monsitor with capnography and ABG
tx hyperk and dysrythmias
If a pt experiences massteter msucle rigidity from sucs. what lab value may confirm dx of MH
elevation in creatine phosphokinase (CPK> 20,000)
how does dantrolene work
acts on ryanodine recpetor ot decrease Ca level in skeletal muscle by decreasing release of ca from SR. skeletal muscle relaxes when supply of calcium to contractile proteins is impaired
dantrolene dose
2.5 mg/kg q5 min until episode is terminated.
max 20 mg/kg
ppx dantrolene dose is 2.5 mcg/ml
each vial of dantrolene contains 20mg withh 3g mannitol- mix with 60ml warmed sterile water
½ life of dantrolee
10 hrs
so readmin q 10-15 hrs for at least one, but possible several doses