Types of breast cancer
1/14
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
15 Terms
Breast cancer
•Multiple molecular mechanisms:
1.Hormone receptor positive (~80%)
•oestrogen + Progesterone + (65%)
•oestrogen + Progesterone – (~13% )
2.HER2 overexpression (~30%)
3.Inherited (e.g. BRCA1 and BRCA2) commonly “triple negative” breast cancer (~15% of cases)
•Treatment is directed by risk of reoccurrence and hormonal status e.g. high risk - radiotherapy, cytotoxic chemotherapy and adjuvant hormonal chemotherapy
•Risk is determined by the presence of biomarkers e.g. Use of the Oncotype Dx test for ER-positive, HER2-negative invasive breast cancer to determine if chemotherapy should be used alongside adjuvant therapy (see the biomarker signature sceencast from term 1)
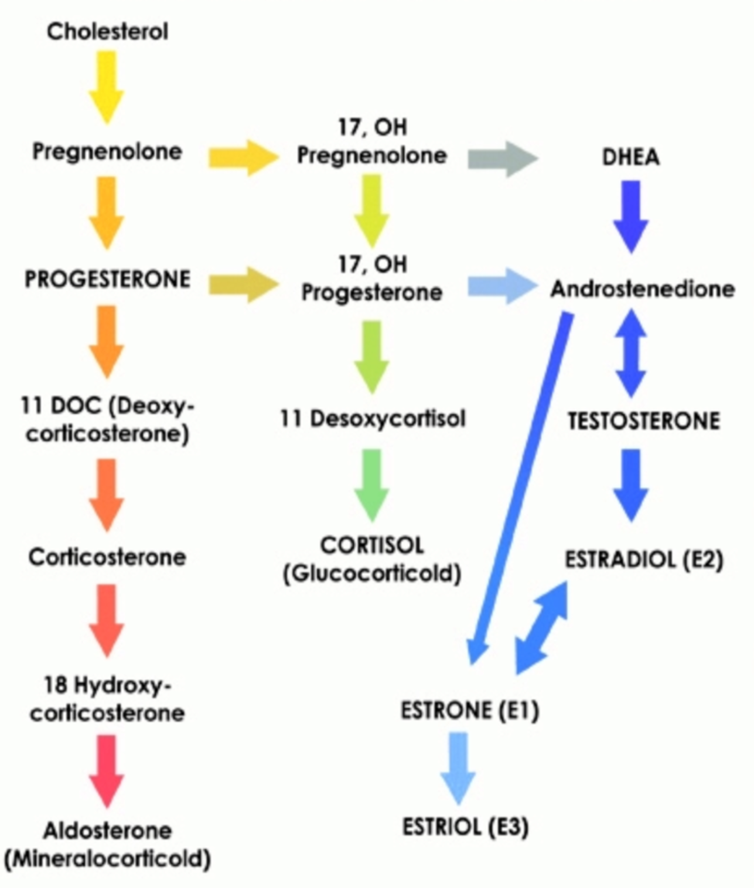
Synthesis of progesterone and
oestrogens
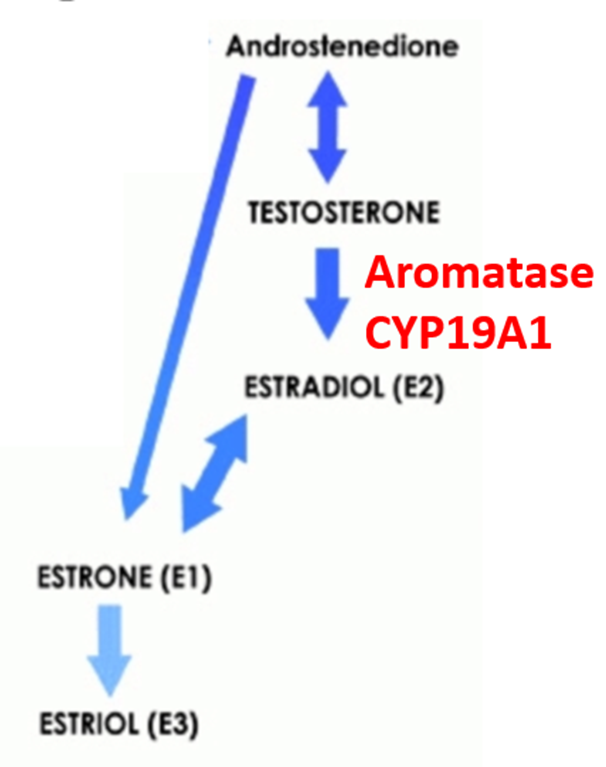
•There are 3 types of oestrogen
•Estrone (E1) is produced from Estradiol in the liver and the small intestines.
•Estradiol (E2) is synthesised in relatively large amounts in the ovaries (urogenital tract) & the female breast. Small amounts in the brain, cardiovascular system, bone, gastrointestinal tract, liver.
•Estriol (E3) is the shortest-acting oestrogen and has the weakest effect on the oestrogen receptor
•Rank order of potency at the receptor:
estradiol >> estrone > estriol
Oestrogen and Progesterone receptors
•Two types of receptor
•Cell surface receptors (not associated with breast cancer)
•Intracellular hormone receptors that act as transcription factor (same family as the glucocorticoid receptors).
•There are 2 oestrogen receptor subtypes ERa and ERβ.
•ERa is involved in breast cancer.
Structure of the ERa and ERβ receptors
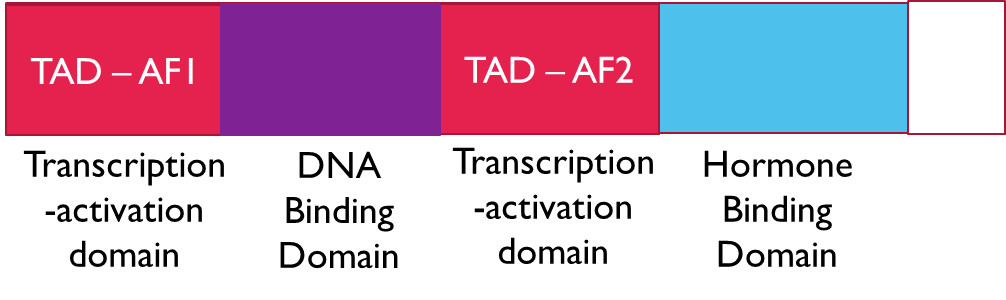
•The receptors contain 3 types of domains:
•Transcription activation domains (TAD) x 2 that can bind to the basic transcriptional machinery via co-activator proteins to stimulate transcription
•DNA binding domain
•Hormone binding domain
Oestrogen – physiological roles
•Oestrogen is a transcriptional activator, it stimulates entry into the cell cycle from G0
•The oestrogen receptor is present in the urogenital tract (cervix/uterus/ovaries), breast, brain, cardiovascular system, bone, gastrointestinal tract, liver
•In men it plays a role in spermatogenesis, sexual maturation, cholesterol metabolism and bone strength
•High levels in females from puberty to menopause. It:
•Stimulates growth of the endometrium
•Reduces bone resorption and increase bone formation
•Increases HDL cholesterol and reduce LDL
•Is elevates mood, low levels of oestrogen are associated with depression in women
Treatment of oestrogen dependant (positive) breast cancer
•There are three different types of antihormonal therapy:
1.Selective oestrogen receptor modulators e.g. tamoxifen
2.Aromatase inhibitors e.g. Anastrozole
3.Oestrogen receptor downregulators / antagonist e.g. Fulvestrant
●
•Pre / post menopausal status determines treatment choice.
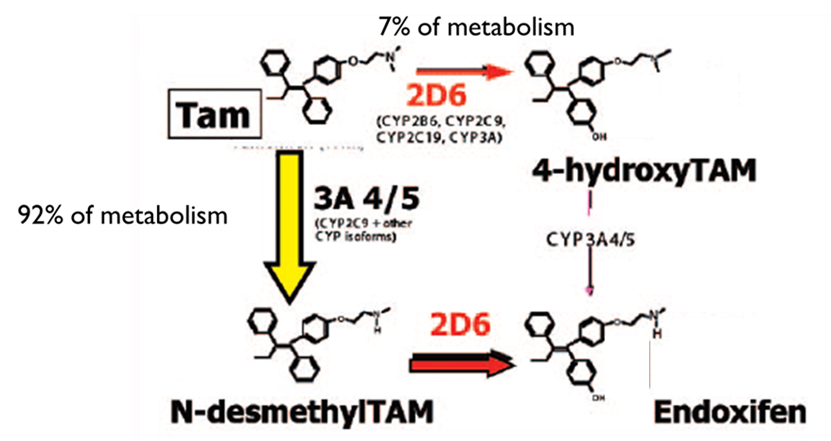
Tamoxifen – a selective oestrogen receptor modulator (SERM)
•There is variability in clinical efficacy and toxicity (2-3 fold greater risk of adverse effects in some individuals)
•Tamoxifen can be considered a prodrug
•It is activated by CYP metabolism
•4-hydroxytamoxifen and endoxifen have 30 to100 x the biological activity of tamoxifen at the oestrogen receptor
•Endoxifen has a 10 fold higher plasma conc than 4- hydroxytamoxifen
•Glucuronidation plays a major role in tamoxifen metabolites inactivation and elimination
•Multiple UDP glucuronosyltransferase family members are thought to be involved which have allele with normal, low or no activity phenotypes’
Tamoxifen – mechanism of action
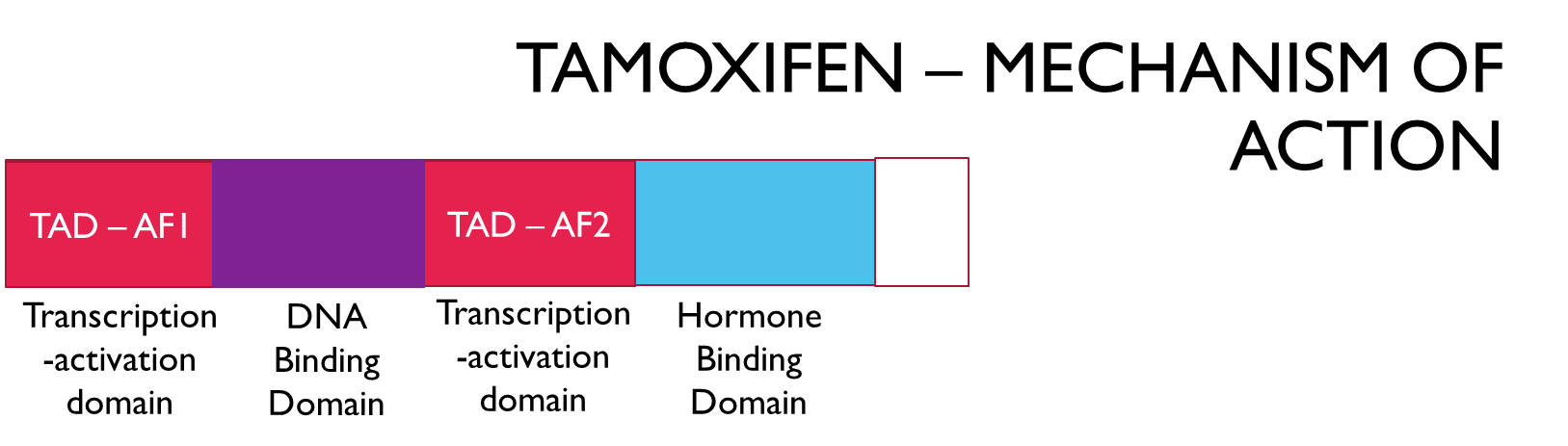
•Tamoxifen and its metabolite bind to the breast oestrogen receptor (ERa)
•Permits the AF1 transcription activation domain to bind to the basic transcriptional machinery via adaptor (co-activator) proteins
•Prevents the AF2 transcription activation domain from binding to the basic transcriptional machinery via adaptor (co-activator) proteins
•This maintains some of the functions of oestrogen via AF1 binding
•eg. enables bone cell division (It does not cause bone destruction as an oestrogen receptors antagonists would)
Tamoxifen - ADRS
•Tamoxifen also binds to the ERβ receptor and acts as an agonist enabling both AF1 and AF2 binding to adaptor proteins leading to increased gene expression
•Results in:
•Hot flushes, fluid retention and menstrual irregularities
•And risk of:
•Endometrial cancer (due to uterine cell proliferation)
•Deep vein thrombosis
•Stroke
Anastrozole - an aromatase inhibitor
•Aromatase (CYP19A1) catalyses the synthesis of estradiol from testosterone (the main source of oestrogen in post menopausal women)
•Aromatase inhibitors block the synthesis of ALL oestrogens from testosterone
•Anastrozole is a reversible inhibitor of CYP19A1
•Blocks oestrogen dependant cell division
•ADRs associated with low oestrogen i.e. menopausal symptoms
•BUT decreased risk of endometrial cancer, thrombosis and stroke.
Fulvestrant –
an oestrogen receptor downregulator / antagonist
•This binds to the receptor resulting in
•Receptor downregulation and
•Antagonises the ability of the receptor to bind to DNA
•May also inhibit aromatase
•No beneficial oestrogenic effects
•Similar adverse effects to tamoxifen
HER2 positive Breast Cancer
•Overexpression of HER2, a member of the epidermal growth factor receptor family
•Amplification of the HER2 gene
•Targeted treatment of HER2+ Breast cancer
•Trastuzumab
•Prevents HER2 homodimer formation
•It can be conjugated with mertansine (a microtubule inhibitor).
•Pertuzumab
•Prevents HER2 heterodimer formation with HER3
Treatment of HER2 positive Breast Cancer
•Neoajuvant treatment of HER2‑positive breast cancer (locally advanced, inflammatory or early‑stage at high risk of recurrence)
•Pertuzumab
•Trastuzumab
•Chemotherapy (typically a taxane e.g. paclitaxel and an anthracycline e.g. Doxorubicin)
•Adjuvant therapy
•Trastuzumab (+/- chemotherapy / radiotherapy depending on personal profile)
BRCA – linked to inherited breast cancer
•BRCA1 and BRCA2 are tumour suppressor genes
•Mutation in both copies of the gene is required for inactivity, mutation is the second copy is normally acquired by a somatic mutation
•BRCA1
•Involved in double strand break repair
•Increases risk of breast cancer and ovarian cancer
•Increase risk of prostate cancer
•BRCA2
•Involved in homologous recombination
•Increased risk of gall bladder, bile duct, stomach cancer and melanoma
Treatment of BRCA breast cancer
•Typically triple negative: ER –ve / PR –ve / HER2 -ve
•Treated with cytotoxic combination chemotherapy e.g.
•Fluorouracil (anti-metabolite)
•Epirubicin (topoisomerase inhibitor)
•Cyclophosphamide (DNA crosslinker)
•Docetaxel (microtubule inhibitor)
•Advanced cancer treated with a PARP inhibitor and chemotherapy