Human Physiology Midterm #3
1/147
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
148 Terms
Lecture 20
20
heart sounds
from turbulent blood flow from valves closing
first sound: softer, '“lubb”, AV valves closing simultaneously (diastole)
second sound: louder, “dubb”, semilunar valves closing simultaneously (systole)
blood flow
silent unless there is an obstruction where it becomes turbulent → most heart murmurs are valve issues
stenotic valve: stiff, narrowed valve that doesn’t open completely
incompetent valve: doesn’t close completely, backflow of blood & collides with forward flowing blood, or can happen from holes in the interventricular septum
blood vessel composition
as arteries divide into smaller arteries → walls become more muscular and less elastic
elastic systemic arteries are a pressure reservoir that maintain blood flow during ventricular relaxation
systemic veins→ expandable volume reservoir
arteriole walls have layers of smooth muscle → contracts/relaxes under chemical signaling
aortic blood pressure
blood pressure in the aorta
doesn’t stay elevated during diastole because blood stops flowing into aorta → lowers blood pressure
elevated pressure in arteries during diastole is because of elastic recoil property of arteries
systolic vs diastolic pressure
systolic pressure: max pressure during systole
diastolic pressure: minimum pressure during diastole
average arterial pressure during cardiac cycle: MAP
capillaries
have small and thin walls
veins vs arteries
veins: thinner muscle, fibrous, and endothelium tissue
arteries: has elastic tissue
pulse pressure
pressure increase generated by left ventricle ejecting blood creates pressure/pulse wave in arteries
measure of strength of pressure wave
pulse pressure= systolic pressure - diastolic pressure
venous blood flow is steady (not pulsatile)
Mean Arterial Pressure (MAP)
represents driving pressure created by pumping of heart
MAP= diastolic pressure + 1/3 pulse pressure
hypotension: blood pressure is too low (fainting)
hypertension: blood pressure is elevated (rupture vessels)
measuring blood pressure
arterial BP measured with a sphygmomanometer & stethoscope
sphygmomanometer has inflatable cuff, when inflates above systolic pressure arterial blood flow is stopped → no sound heard above brachial artery
when cuff pressure is btw systolic & diastolic pressure → turbulent blood flow (Korotkoff sounds) can be heard thru compressed artery
when cuff pressure is below diastolic pressure → artery is no longer compressed and blood flow is silent
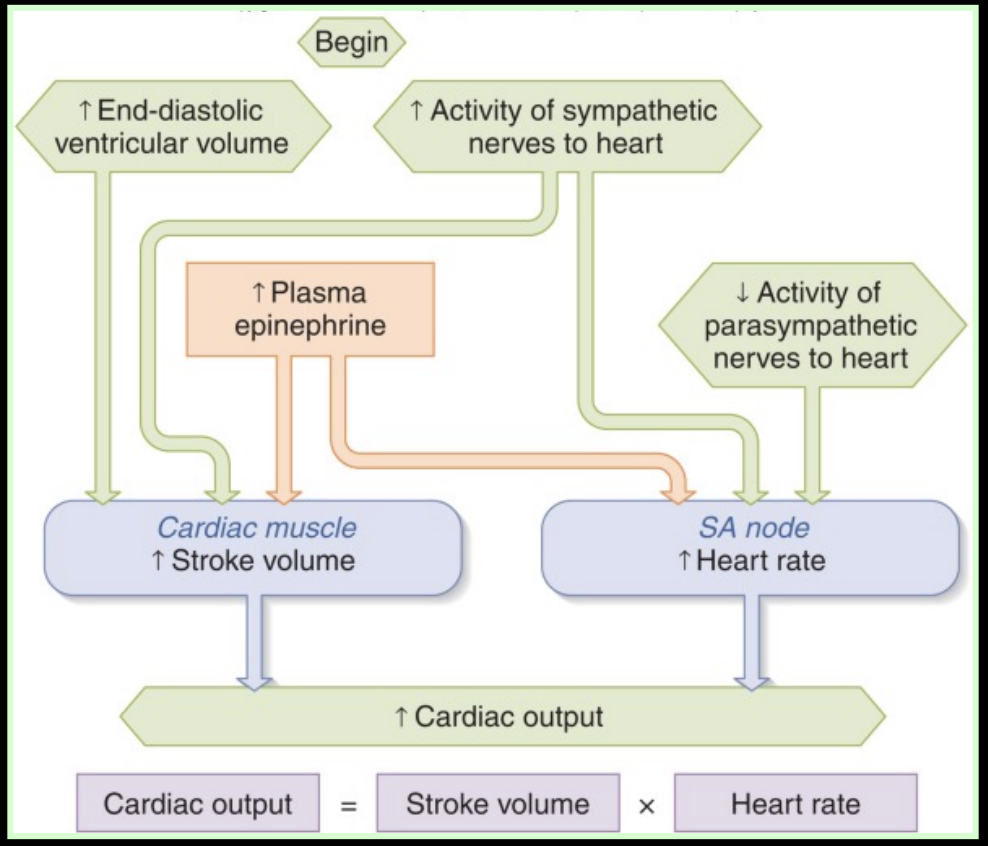
cardiac output (CO)
amount of blood pumped out of each ventricle in one minute
product of heart rate (HR) & stroke volume (SV)
CO= HR * SV
heart rate & parasym vs sym activity
HR is initiated by autorhythmic cells in SA node @ 100 bpm
@ resting state → more parasympathetic than sympathetic activity to heart → normal resting HR is lower (70 BPM)
sympathetic NS activity increases HR
sympathetic NS activity raises HR: epinephrine/nerves ↑ → B-adrenergic receptors in SA node activated by epi → increase open state of F-type Na & T-type Ca2+ channels → increases rate of spont depol → increase HR
parasympathetic NS activity decreases HR
increased parasympathetic activity (vagus nerve) → muscarinic cholinergic receptor in SA node → increased open state of K+ channels and closed state of Ca channels → decrease rate of spon depol & hyperpol cell → decreased HR
sympathetic NS
can increase the force of contraction at any given end-diastolic ventricular volume → which increases stroke volume
Frank-Starling principle
the heart will pump all the blood that returns to it → strength of contraction increases as the end-diastolic ventricular volume increases
increasing end-diastolic volume stretches muscle → brings fibers closer to optimum length → optimum length = greater strength of contraction → increased stroke volume and cardiac output
SV is increased by increase in end-diastolic volume & increase in contractility to due sym stimulation/epinephrine
factors determining cardiac output
MAP
regulated by homeostatic mechanisms, influences blood flow to all organs in systemic circuit
MAP = CO * TPR (total peripheral resistance)
Total peripheral Resistance (TPR): sum of resistances to flow by all systemic blood vessels
baroreceptor reflex
primary short-term reflex pathway for homeostatic control of MAP, increases MAP
sensory receptors of the baroreceptor reflex are in walls of carotid arteries and aorta → carotid baroreceptors in brain, aortic baroreceptors in body
baroreceptor reflex arc components
stimulus: change in BP
integrating center: medullary cardiovascular control center (CVCC) in medulla oblongata
initiates a rapid response→ changes in CO & TPR within 2 heartbeats of stimulus
output signals from CVCC are carried by sym & parasym neurons
peripheral resistance
under tonic sympathetic control → increased sym discharge causes vasoconstriction
baroreceptor firing frequency
changes w BP
high BP → stretches baroreceptor membranes → firing rate increases
low BP → firing rate of baroreceptors decreases
heart is regulated by
antagonistic control
increased sym activity → increases HR, shortens conduction time thru AV node, enhances force of myocardial contractions
increased parasym activity→ slows HR, small effect on ventricular contraction
arterial baroreceptor reflex
functions as a SHORT-term regulator of arterial BP, if BP changes for long time the baroreceptors simply adapt
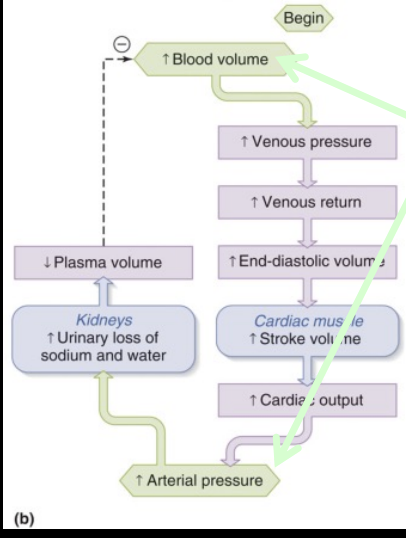
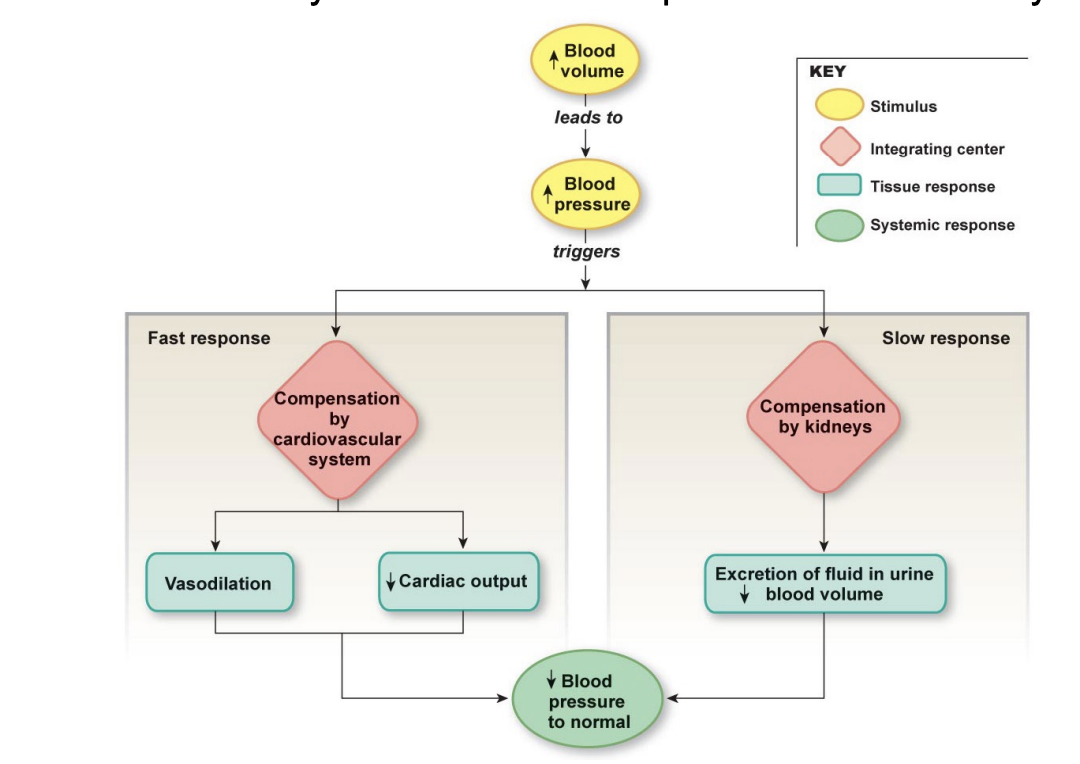
BP control includes rapid responses from cardiovascular system & slower responses from kidneys
if blood volume increases, BP increases
hard to compensate for decreased blood volume → kidneys can only conserve BV (blood volume) not restore it
increase in excretion of urine restores BV to normal
increased BV due to increased fluids → increase in arterial pressure
Lecture 21
21
respiratory function
pulmonary ventilation: movement of air into lungs (inspiration) & out (expiration) via bulk flow
exchange btw lung air spaces & blood via diffusion
transport O2 & CO2 btw tissues via blood
exchange O2 & CO2 btw blood & body tissues via diffusion
Fick’s Law
states that rate of diffusion of a gas depends on 5 parameters
solubility of gas in aqueous film lining gas exchange surface
temperature
surface area available for diffusion, A
difference in partial pressure of gas across surface, P2-P1
thickness of barrier to diffusion, D
respiratory epithelia are thin (D is small) and folded (A is large), large pressure gradient (P2-P1 is large)

K is diffusion constant, A is area for gas exchange
upper airways
air passages of head & neck → nasal cavities, oral cavities, pharynx
air enters thru the cavities which lead to pharynx → food enters esophagus & air enters larynx
respiratory tract
2 components→ upper conducting zone & lower respiratory zone
upper conducting zone:
conducts air from larynx to lungs
begins w the larynx (tube containing vocal cords)
lower respiratory zone:
contains sites of gas exchange within lungs
thinner walls
larnyx
opens into 2 main bronchi→ one of which enters each lung (right & left bronchi)
each bronchi divides into secondary bronchi→ right side into 3, left side into 2 → continues to branch out (millions)
alveoli
major sites of gas exchange btw each other and blood
attached to walls of respiratory bronchioles, increases in amount near alveolar ducts
terminate in clusters called alveolar sacs
alveolar sac
surrounded by elastic fibers & network of capillaries
type I alveolar cells
thickly covers the air-facing surface of 1 alveolar wall, all flat
permits gas-exchange
type II alveolar cells
secretes surfactant that reduces surface tension in alveoli → allows better expansion
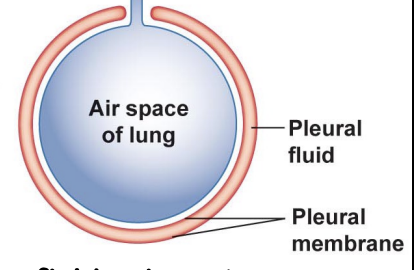
pleural sac
fluid that surrounds each lung
double membrane→ parietal pleural side lines chest wall, visceral pleural membrane lines the lung
like a fluid filled balloon surrounding an air-filled balloon
ventilation
air moves down a pressure gradient from pressure of atmosphere to alveoli
inspiration happens when alveoli pressure is less than atmosphere pressure
expiration happens when atmosphere pressure is less than alveoli pressure
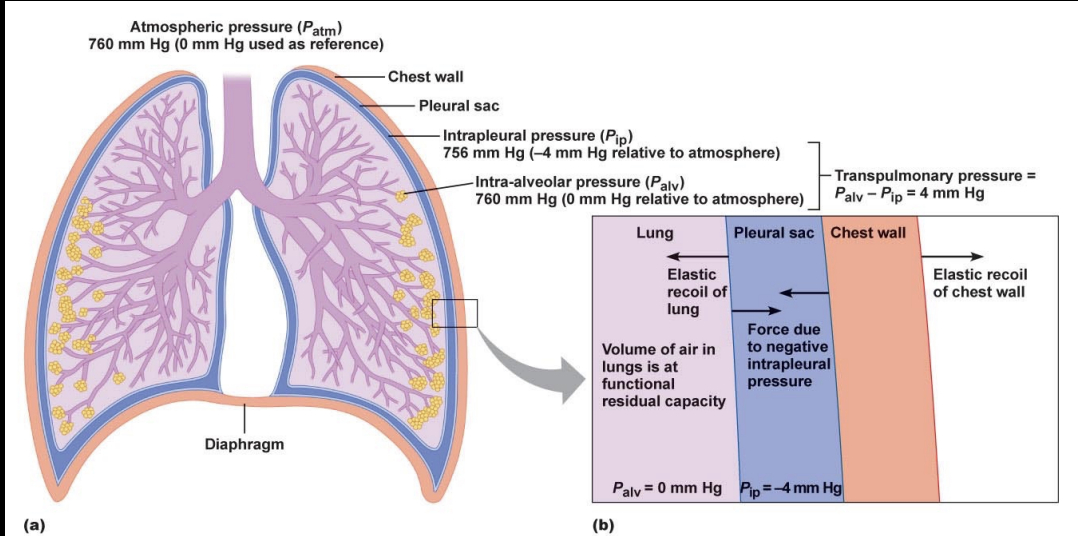
4 pressures in lungs
atmospheric pressure
intra-alveolar pressure
intra-plural pressure
transpulmonary pressure
atmospheric pressure
Patm
pressure of outside air
constant, 0 mmHg
intra-alveolar pressure
Palv
pressure of air in alveoli
varies w phase of respiration → during inspiration it is negative (less than Patm) & during expiration it is positive
ventilation is driven by Palv-Patm
intra-plural pressure
Pip
pressure inside the pleural sac
always negative because of elasticity in lungs & chest wall → opp forces pull on intra-pleural space (chest wall outward, lungs inward)
surface tension of intrapleural fluid hold wall & lungs tg
always less than Palv
-4mmHg
transpulmonary pressure
Palv - Pip
distending pressure across lung wall
increase in transpulmonary pressure creates a larger distending pressure
wound to pleural sac
pleural sac must be airtight → if punctured then negative Pip is lost → lungs recoil and collapse while chest wall expands → pneumothorax
air flow mechanism & Boyle’s Law
air flow is driven by pressure gradients that respiratory muscles create by changing the volume of the lungs
Boyle’s Law: pressure in inversely related to volume → can change alveolar pressure by changing volume
inspiration to expiration & pressure
start of inspiration: lungs expand from contraction of inspiratory muscles → lowers Palv so air is drawn into lungs
next: Palv falls at first but then rises because of increase of air molecules flowing in, when Palv=Patm air flow inward stops
finally: lung volume decreases, Palv increases → air flows out, amount of airflow in alveoli decreases which lowers pressure to 0
inspiration initiation (active expiration)
by neural stimulation of inspiratory muscles → ACh is released → causes contraction of the diaphragm → diaphragm flattens and moves down → contraction of external intercostals make ribs go up and out to expand chest wall
as chest expands it pulls out on intrapleural fluid → makes Pip decrease → causes increase in transpulmonary pressure → causes larger distending pressure across lungs → inflation of lungs Palv < Patm
quiet breathing expiration
passive process, no muscle contraction
when motor neurons stop firing → inspiratory muscles relax → lungs/chest wall recoil to OG positions → volume of thoracic cavity decreases Palv > Patm → air flows out until Palv = Patm
2 factors affecting pulmonary ventilation
lung compliance: measure of ease which they can be stretch, lungs are elastic and recoil after being stretched
elasticity & surface tension
airway resistance: resistance of the entire system of airways in the respiratory tract
lung compliance
change in lung volume that results from transpulmonary pressure change
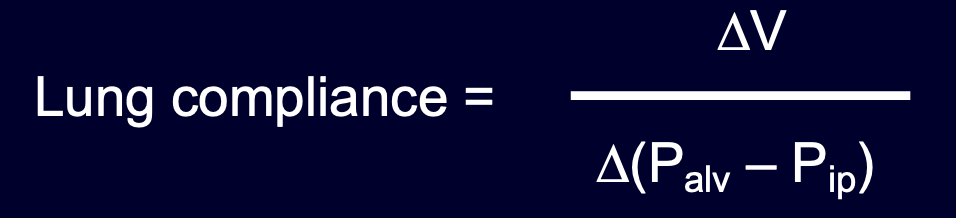
big lungs = better → smaller change in transpulmonary pressure needed to bring in air, less muscle contraction
elasticity
elastic fibers oppose lung expansion → lungs stretch, fibers recoil
emphysema results in destruction of elastin fibers in lung tissue → lungs have high compliance and stretch easily but don’t recoil back to resting position for expiration
surface tension
the greater the ST the more work needed to spread the fluid out
created in lungs by thin layer of fluid lining the internal surface of the alveoli → as lungs expand work is required to stretch elastic tissue but to increase SA of fluid layer
big ST = less compliant
Laplace’s Law
P = 2T/r
pressure = 2*surface tension / radius
air pressure is directly proportional to surface tension & inversely proportional to alveolar radius
pulmonary surfactant
decrease ST in alveoli, secreted by type II alveolar cells
increases lung compliance
stabilizes alveoli of diff sizes (r) by differentially altering surface tension to allow them to have same pressure
Newborn Respiratory Distress Syndrome (NRDS)
risk for premature babies, develops by 34th week
lungs have low-compliance (stiff) low surfactant → alveoli collapse completely and must completely re-inflate → waste energy → use steroids that increase surfactant production to treat
airway resistance
when resistance increases → large pressure gradient required to make air flow
determines how much air flows into lungs at any given pressure (major determinant)
Lecture 22
22
gas exchange
involves diffusion of O2 & CO2 from regions of higher to lower partial pressure
gases are expressed as partial pressures because gas is mixture of more than 1 molecule
Dalton’s Law
Ptotal= P1 + P2 + P3 + P4 + Pn
total pressure of such a gas is the sum of the pressure of individual gases that make up the mixture
partial pressure: proportion of the pressure of the entire gas that is due to the presence of the individual gas
atmosphere is 79% N2 & 21% O2
solubilities of gasses in liquids
when a gas is in contact w water → pressure gradient, gas molecules move from gas to water IF gas pressure is higher than water pressure → continues until equilibrium
oxygen has low solubility in aqueous solution, CO2 is more soluble
carbonation
water in contact w normal air has negligible carbonation
when cool water and combine w high pressure CO2 → gas moves into water → carbonation
normal alveolar Po2
100 mmHg while deoxygenated venous blood is 40mmHg
Pco2
of arterial blood is 40mmHg
it’s lower than Pco2 of cells (46mmHg) → CO2 diffuses out of cells into capillaries
Po2 of aterial blood
leaving lungs is 100mmHg
when arterial blood reaches capillaries → gradient is reversed → intracellular Po2 partial pressure is lower than 40mmHg → O2 travels down pressure gradient
oxygen solubility
per 1 liter of arterial blood has 200ml of O2
only 3ml dissolves in 1 Liter of blood & 197 ml of O2 is transported in RBCs combined w hemoglobin
hemoglobin (Hb)
protein made of 4 subunits → each subunit consists of heme & polypeptide attached
each heme group has 1 Fe+ ion which O2 binds to
O2 + Hb (deoxyhemoglobin) →← HbO2 (oxyhemoglobin)
percent Hb saturation = (O2 bound to Hb/max capacity of Hb to bind O2) × 100
O2-Hb dissociation curve
relationship btw Po2 & % hemoglobin saturation → shape reflects properties of Hb molecule and affinity for O2
at normal Po2 (100mmHg) 98% of Hb is bound to O2
as blood passes thru lungs under normal conditions Hb picks up almost max O2
at Po2 above 100mmHg → only minor changes in % of Hb saturation
alveolar Po2 can be <100mmHg w/o lowering % Hb sat significantly
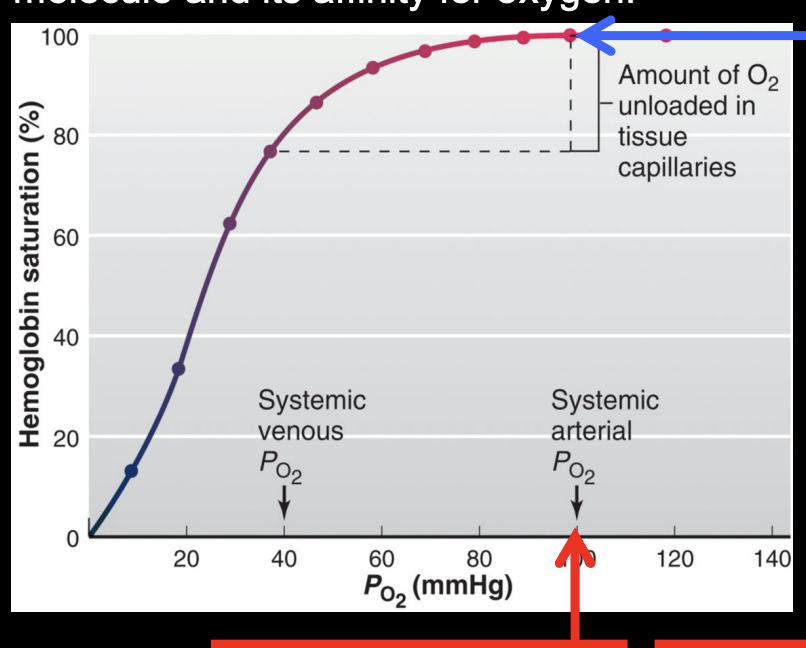
more about O2-Hb dissociation curve
once Po2 falls from 100 to 60 the % Hb sat becomes steeper → small decrease in Po2 causes large release of O2
in blood leaving systemic capillaries w a Po2 of 40 → Hb is still 75% sat → cells release only 25% of its O2 → remaining O2 stays bound to serve as a reservoir
O2 affinity to hemoglobin
each subunit combines w 1 O2 molecule → rxns of 4 subunits are sequential, each combo facilitates the next
DeoxyHb subunits are tightly held by electrostatic bonds in conformation w low affinity for O2
binding of O2 breaks bonds → conformational change → remaining O2 binding sites more exposed → binding of 1 O2 increases affinity of other sites
O2 affinity hemoglobin chart
if shifts left → more loading of O2, less unloading
if shifts right → less loading of O2, more unloading
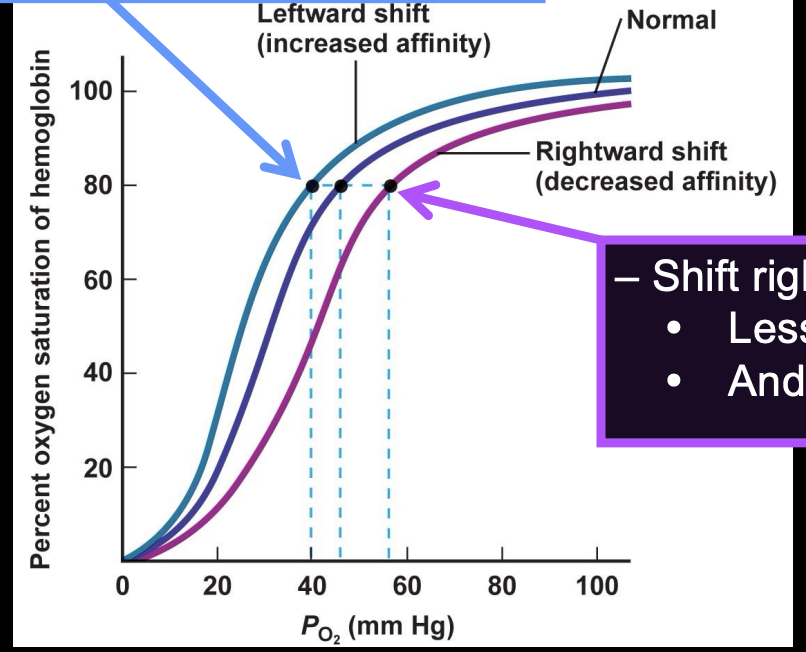
factors that affect Hb sat
temp, acidity, blood DPG (makes Hb have less affinity, releases more O2 to cells)
increase in these causes a shift to the right (decrease affinity)
decreases causes a shift to the left (increase affinity)
molecules w greater affinity facilitate O2 delivery
fetal Hb→ high affinity for O2 than adult Hb → fetus can steal O2 from mom’s blood
myoglobin→ high affinity for O2
Hb has a higher affinity for CO than O2 → makes it v toxic
CO2 is transported in blood in 3 ways
First way is:
only 7% of CO2 carried by venous blood is dissolved in blood, other 93% diffuses into RBCs → 70% is converted to bicarbonate & 23% binds to hemoglobin
2nd way CO2 is transported in blood
conversion of CO2 to bicarbonate (HCO3-) depends on carbonic anhydrase (CA) enzyme in RBC
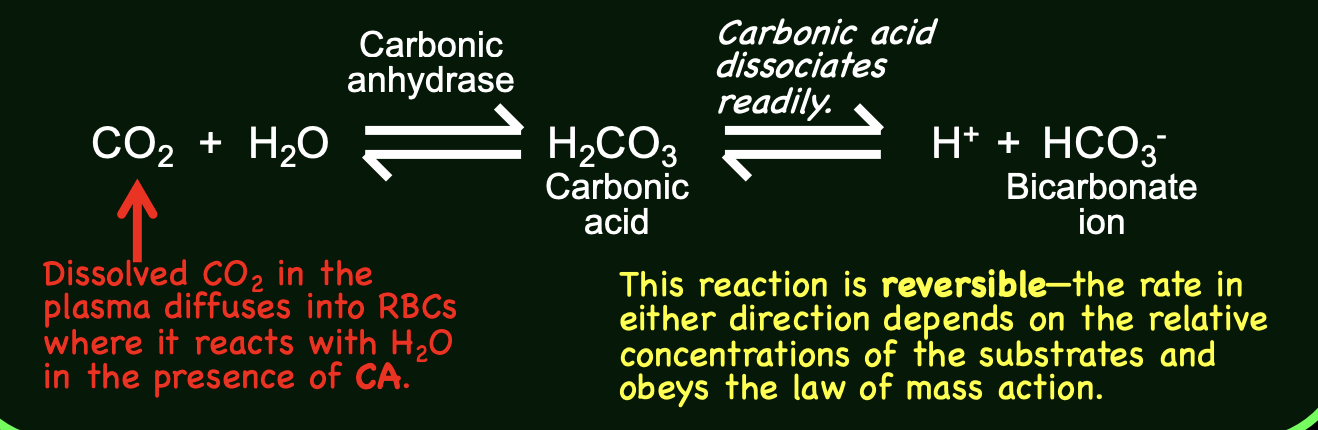
products (bicarbonate) must be removed from cytoplasm of RBC → 2 mechanisms remove H+ and bicarbonate
antiport protein exchanges HCO3- for Cl- → chloride shift
deoxyhemoglobin in RBC bind H+ → has a greater affinity for H+ than oxyHb
3rd way CO2 is transported in blood
about 23% of CO2 in venous blood binds directly to Hb → when O2 leaves binding sites on Hb, Co2 binds w free Hb at amino groups → forms carbaminohemoglobin

CO2 transport summary
CO2 diffuses out of cells into systemic capillaries
7% of Co2 is dissolved in plasma
23% of CO2 binds to Hb to form carbaminoHb
70% of Co2 is converted into bicarbonate & H+, Hb buffers H+
HCO3- enters plasma in exchange for Cl- (chloride shift) → transported to lungs → @ lungs dissolved CO2 diffuses out of plasma → CO2 unbinds from Hb and diffuses out of RBC → carbonic acid rxn reverses, pulls HCO3- back into RBC and converts to CO2
Lecture 23
23
spirometer
device that measures volumes of inspired and expired air
breathe into tube that converts air into electrical signal
3 of 4 non-overlapping lung volumes make total lung capacity, including tidal volume, inspiratory volume, and expiratory reserve volume
4 non-overlapping lung volumes
inspiratory reserve volume
tidal volume
residual volume
expiratory reserve volume
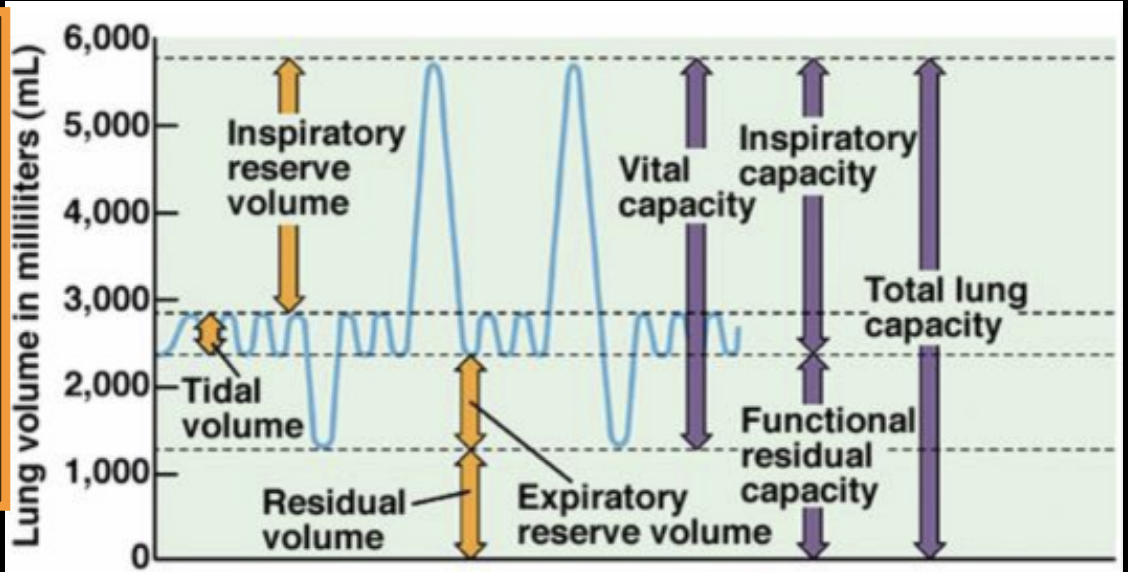
inspiratory reserve volume (IRV)
max volume of air that can be inspired from end of normal inspiration
tidal volume (Vt)
volume of air that moves in & out of lungs during a single unforced breath
residual volume (RV)
volume of air remaining in lungs after max expiration
expiratory reserve volume (ERV)
max volume of air that can be expired from end of normal expiration
lung capacities are sums
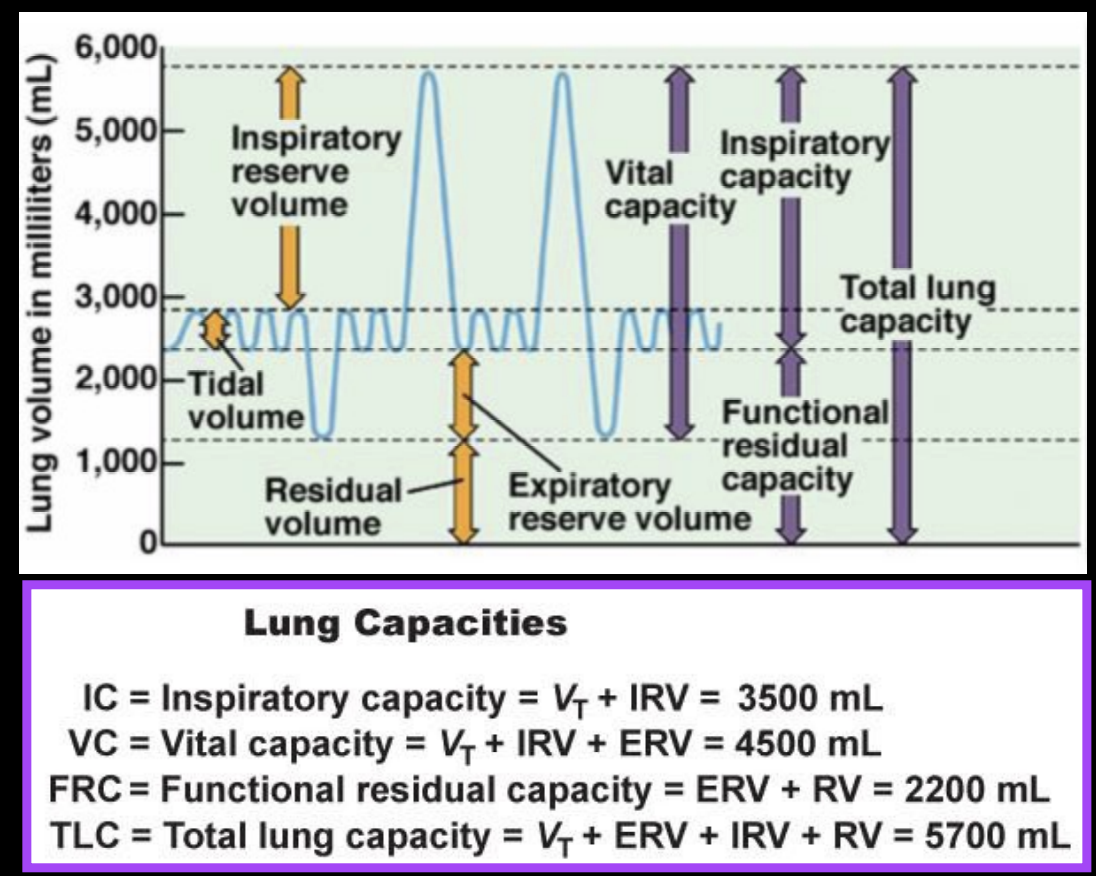
vital capacity is sum of?
tidal volume, inspiratory reserve volume, and expiratory reserve volume
minute ventilation
minute ventilation = tidal volume * respiratory rate
total amount of air inhaled or exhaled in a minute
minute ventilation > alveolar ventilation → because of dead space
air that remains in upper airways does not get to alveoli→ dead space
alveolar ventilation = (tidal volume -anatomical dead space) * respiratory rate
end of inspiration & dead space
end of inspiration → first exhale air comes out of dead space → at end of expiration, dead space filled w stale air from alveoli → inhale fresh air
diaphragm and intercostal muscles
both skeletal muscles, do not contract w/o stim by motor neurons
breathing depends on cyclical respiratory muscle excitation by motor nerves → inhibit nerves = no breathing
inspiratory spinal motor neurons
when AP stops → inspiratory muscles relax → expiration occurs
inspiration initiated by burst of AP in spinal motor nerves to diaphragm
medulla oblongata
holds the Pre-Botzinger complex in the reticular formation
integration center that controls breathing
Pre-Botzinger complex: consists of pacemaker cells which create the rhythm of breathing, on either side of medulla oblongata
PreBotC fires APs to the Phrenic Motor Neurons (lead to diaphragm, tells to contract)
if separate PreBotC & Phrenic Motor Neurons→ breathing stops
Medulla also has:
dorsal respiratory groups: inspiration
ventral respiratory groups: forced/heavy breathing
medulla oblongata regulates contraction of insp & exp muscles
thru reciprocal inhibition→ motor neurons of exp muscles are inhibited when insp muscles are active & vise versa
Pontine Respiratory Group (PRG) & medulla oblongata
both regulated by cortex
PRG fine tunes transition btw insp & exp
peripheral arterial & central chemoreceptors regulate medullary insp neurons
peripheral chemoreceptors:
near baroreceptors controlling BP
sense changes in Po2 levels, increased H+, & pH of plasma
2 types:
carotid bodies: strategically located to monitor O2 supply to brain
aortic bodies: monitor rest of body O2 supply
central chemoreceptors:
in medulla
stimulated by increase in H+ conc in brain ECF (from carbonic acid rxn) or in blood Pco2
give excitatory synaptic input to medullary insp neurons
glomus cells
trigger reflex in ventilation
in carotid & aortic bodies, activated by decrease in Po2, increase in Pco2, or pH change
ventilation stimulated when arterial Po2 is less than 60mmHg OR when plasma pH lowers OR Pco2 increases
glomus cells pathway
stimulus(change in Po2/Pco2/pH) inactivates K+ channels causing glomus cell depolarization → depol opens VG Ca+ channels → Ca+ entry leads to exocytosis of NT onto sensory neuron → AP in sensory neuron leads to brain stem resp network → increase ventilation
central chemoreceptors
located on ventral surface of medulla oblongata (brainstem)
respond to pH changes in CSF, not directly responsive to CO2
increased CO2 decreases pH
central chemoreceptors set the respiratory pace
arterial Pco2 increases → CO2 crosses the BBB → CO2 in CSF is converted into carbonic acid → carbonic acid dissociates into bicarbonate & H+ → central chemoreceptors activated by H+ → receptors signal the control network to increase ventilation rate & depth → CO2 is removed from blood
ventilation stimulated by chemoreceptors by:
a LARGE decrease in arterial Po2
arterial Pco2 increases A LITTLE
Lecture 24
24
central chemoreceptors
located on ventral surface of the medulla
sets the respiratory pace by providing continuous input into control network
respond to pH changes in CSF, not directly responsive to CO2
increased CO2 decreases pH
negative feedback loop for central chemoreceptors & CO2
arterial Pco2 increases → Co2 crosses BBB → Co2 in CSF is converted to carbonic acid → carbonic acid readily dissociates into bicarbonate and H+ → central chemoreceptors are activated by H+ → receptors signal the control network to increase rate and depth of ventilation → CO2 is removed from blood