Lecture 5- Relines and rebases
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
What is reline used for?
To only solve the problem of the fit
If a patient has ridge resorption, relining can be used to
Close the gap between existing denture and ridge
What is relining?
Resin is added to the existing denture base
What is rebasing?
All the denture base is replaced (all pink acrylic)

Why might relining be necessary?
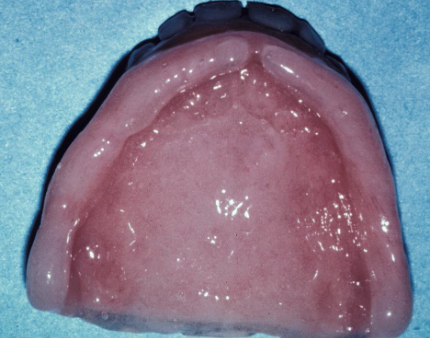
Residual ridge resorption
Ill-fitting denture causes tissue problems (conventional)
More cost effective than making a whole new denture

What are the two types of relines
Direct- intraorally
Indirect- done in lab
What are some indications for direct (intraoral) relines?
To improve denture fit
For immediate dentures during healing
To aid in healing tissue (tissue conditioning)
Used for RPDs
What is a CON for direct intraoral relines?
Technique sensitive so not used in every case, must be precise
What is a PRO for direct intraoral relines?
Soft relines have a limited life span, it is temporary so easy to adjust
What is a contraindication for a direct (intraoral) reline?
Denture problem is not related to the fit
What is an indication for using soft reline material for an interim denture?
If it’s still in the early stages <2 months and there are rapid changes in the fit, use lynal. This is because majority of the absorption occurs during this tie
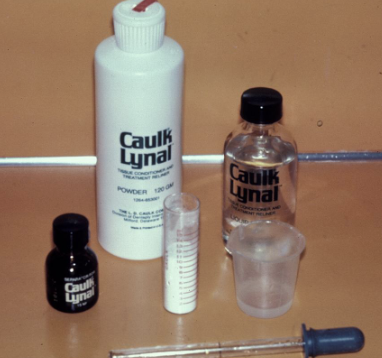
You can use a tissue condition and treatment reliner called
Caulk Lynal. It is a powder and a liquid, you want to create a peanut butter consistency
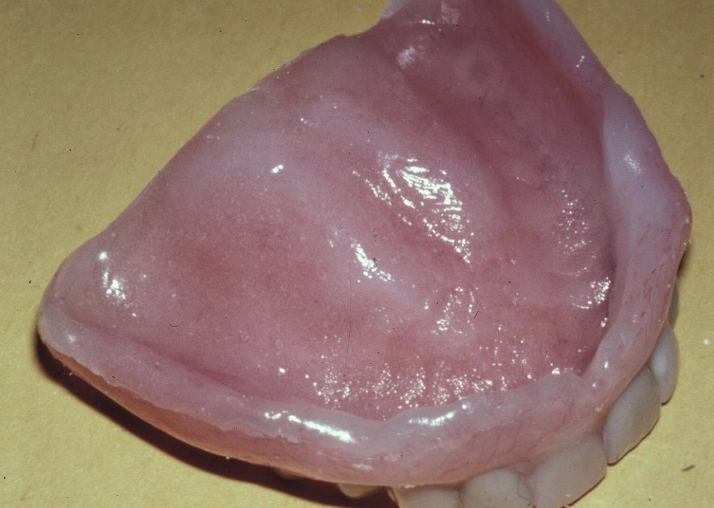
What do you do during the relining appointment?
Place the lynal in the intaglio 7-10 min, trim the rough areas. The whole appointment should take ~30 min
Lynal hardens over time and starts to chip. This varies with each patient. You want to ensure what?
You cleanse the oral flora well

What are some indications for direct hard relines?
Reline for RPD
Interim dentures after ridge has matured
New denture if lack of fit
Direct hard relines material that mixes just like lynal
Astron- requires light cure


Apply astron and let it set for ~10min. If you like it, cure it! If you don’t like it?
You can peel/remove it and redo. It is convenient for a hard denture
What are some indications for indirect (lab) RELINES?
Recently made dentures that require better extensions
Refitting immediate dentures
Refitting older dentures
What are some indications for indirect (lab) REBASE?
This is where you are replacing the whole acrylic.
Lack of proper fit, otherwise denture okay
Discolored base material
Fractured base material with previous repairs
What are some components to check if the fit is okay regarding an indirect rebase?
Adequate VDO
Acceptable occlusion
Acceptable esthetics
What are some contraindications for indirect (lab) RELINES & REBASES?
If you need to modify tooth position
There is a major occlusal discrepancy
If you need to alter the VDO
You have severely inadequate/deficient extensions
Unrealistic expectation of patient regarding outcome
Should you be selective or indiscriminative when relining dentures?
Selective

What impression material should you use for the border molding
Impregum

What impression material should you use for the final impression on the upper?
Light body permadyne

What impression material should you use for the final impression on the lower? Why?
2/3 light body permadyne
1/3 impregum
This will help increase its viscosity
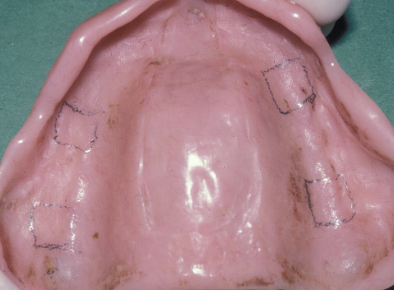
How do you take the final impression for the reline or rebase?
Use the denture as the impression tray, remove any undercuts from intaglio, and provide 1mm of relief inside denture to create room for the impression material
If your denture is underseated, what does that mean?
You need to increase the vertical dimension
If your denture is overseated, what does that mean?
You need to decrease the vertical dimension
What are some problems that can happen with relines?
It can change the VDO or the position of the anterior teeth
How can you solve the problems that occur with the relines?
Try in the final impression
If incorrect, redo the impression
Making a new denture if the reline is incorrect costs

What are your reline options for removable partial dentures?
Do them directly with light cured resin (astron hard) and use only the framework to seat the prosthesis
A 71-year-old edentulous patient presents with maxillary and mandibular complete dentures that are 10 years olf and complains that “my dentures are too loose, I am having difficultly chewing my food and my dentures ahve been relined about 2 years ago".” After your examination and diagnosis, you confirmed that the dentures are ill-fitting, presence of generalized tissue inflammation on edentulous ridges, IPH on the palate, the VDO is not correct, and the denture teeth are worm. What is your treatment plan for this patient?
Direct soft reline followed by new maxillary and mandibular dentures
The disadvantages of direct soft liners include:
Both being hard to polish and they are temporary
T/F: Rebasing of the denture is indicated in situations where the entire base of the denture needs to be replaced
True
When treatment planning for a reline or rebase, direct or indirect reline, the following important criteria of the existing dentures needs to be evaulated.
Retention
Stability
Support
Esthetics
Extensions and
?
?
VDO and occlusion
The following is/are indications of a direct reline (hard or soft)
All of the options