Unit V - The Nervous System II
1/69
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
70 Terms
Anatomy of a Nerve
Epineurium covers the nerves
Perineurium surrounds a fascicle
Endoneurium separates individual nerve fibers
Blood vessels only penetrate the perineurium
Ganglia
Clusters of nerve cell bodies
Rami
Branches of spinal nerves that split after exiting the spine
Plexuses
Networks where rami intermix and reorganize before serving the limbs
Spinal Nerves and Plexuses

The Spinal Nerves
31 pairs of spinal nerves (1st cervical above C1)
Mixed nerves exiting at intervertebral foramen
Proximal Branches
Dorsal root is sensory input to spinal cord
Ventral root is motor output of spinal cord
Cauda Equina is roots from L2 to C0 of the cord
Distal branches
Dorsal ramus supplies dorsal body muscle and skin
Ventral ramus to ventral skin and muscles and limbs
Meningeal branch to meninges, vertebrae and ligaments
Branches of a Spinal Nerve
Spinal nerves:
8 Cervical
12 Thoracic
5 Lumbar
5 Sacral
1 Coccygeal
Each has dorsal and ventral ramus
Shingles
Skin eruptions along path of nerve
Varicella-zoster virus (chicken pox) remains for life in dorsal root ganglia
“Occurs after age 50 if immune system is compromised”
Not true! Can occur at any age with re-exposure to Varicella
No special treatment
Nerve Plexuses
Ventral rami branch and anastomose repeatedly to form 5 nerve plexuses
Cervical in the neck, C1 to C5
supplies the neck and phrenic nerve to the diaphragm
Brachial in the armpit, C5 to T1
supplies the upper limb and some of the shoulder and neck
Lumbar in the low back, L1 to L4
supplies the abdominal wall, the anterior thigh, and the genitalia
Sacral in the pelvis, L4, L5 and S1 to S4
supplies the remainder of the lower trunk and lower limb
Coccygeal, S4, S5 and C0
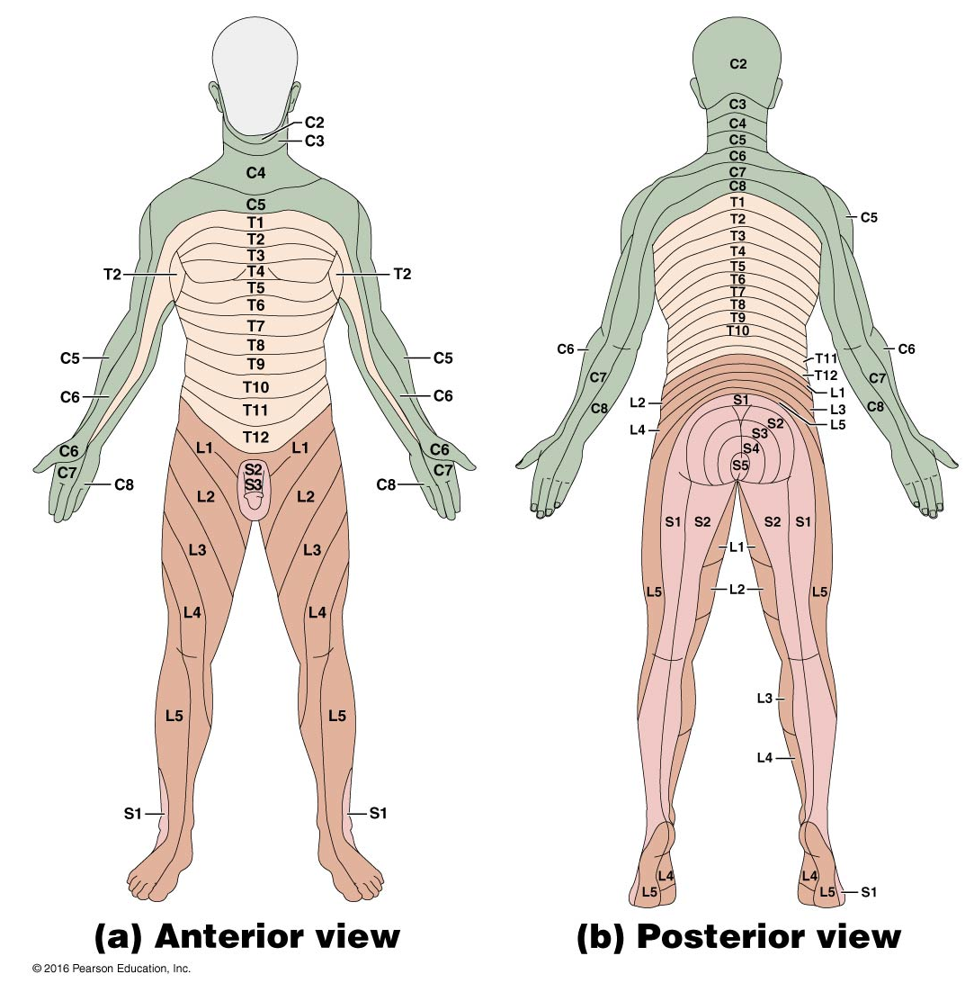
Cutaneous Innervation and Dermatomes
Each spinal nerve receives sensory input from a specific area of skin called a dermatome
Overlap at edges by 50%
A total loss of sensation requires anesthesia of 3 successive spinal nerves
Sensory Input
Vital to the integrity of personality and intellectual function
Sensory Deprivation
Withholding sensory stimulation
Sensory Receptor
A structure specialized to detect a stimulus
Bare nerve ending
Sense organs - nerve tissue surrounded by other tissues that enhance response to a certain type of stimulus
Added epithelium, muscle, or connective tissue
General Properties of Receptors
Transduction – the conversion of one form of energy to another
Fundamental purpose of any sensory receptor
Conversion of stimulus energy (light, heat, touch, sound, etc.) into nerve signals
Receptor Potential – small, local electrical change on a receptor cell induced by an initial stimulus
Results in release of neurotransmitter or a volley of action potentials that generates nerve signals to the CNS
Sensation – a subjective awareness of the stimulus
Most sensory signals delivered to the CNS produce no conscious sensation
Filtered out in the brainstem
Visceral stimuli do not require conscious awareness (pH and body temperature)
Receptors Transmit Four Kinds of Information
Modality
Location
Intensity
Duration
Modality
Type of stimulus or the sensation it produces
Vision, hearing, taste
Labeled Line Code
All action potentials are identical
Each nerve pathway from sensory cells to the brain is labeled to identify its origin, and the brain uses these labels to interpret what modality the signal represents
Location
Encoded by the nerve fibers that issue signals to the brain
Receptive Field – area that detects stimuli for a sensory neuron
Receptive fields vary in size – fingertip versus skin on the back
Two-point touch discrimination
Sensory Projection - the brain identifies the site of stimulation
Projection Pathways – the pathways followed by sensory signals to their ultimate destination in the CNS
Intensity
Encoded in 3 ways:
The brain can distinguish intensity by:
Which fibers are sending signals
How many fibers are doing so
How fast are these fibers firing
Duration
How long does the stimulus last
Change in firing frequency over time
Sensory adaptation – prolonged stimulation → firing of the neuron gets slower over time → less aware of the stimulus
Phasic Receptor –burst of action potentials on stimulation, quick adaptation & sharply reduce or stop signaling even though the stimulus continues
Smell, hair movement, and cutaneous pressure
Tonic receptor - adapts slowly, generates nerve signals more steadily
Proprioceptors - body position, muscle tension, and joint motion
Adaptation to Stimulation
Tonic: AP frequency determined by the amplitude of the stimulus
Phasic: AP frequency determined by the rate of change of the amplitude of the stimulus
Slowly adapting approaches, Tonic
Rapidly adapting, similar to Phasic
Receptor Level Processing
Receptor Potentials
Generator Potential:
The receptor region is part of a sensory neuron
Include free dendrites or encapsulated receptors of most general sense receptors
Graded potential that generates action potentials
Receptor Potential:
The receptor is a separate cell
Graded potential occurs in separate receptor cells and changes the amount of neurotransmitter released by the receptor cell
Most special senses
Classification of Receptors
By Modality:
Thermoreceptors, photoreceptors, nociceptors, chemoreceptors, and mechanoreceptors
By Origin of Stimuli
Exteroceptors - detect external stimuli
Interoceptors - detect internal stimuli
Proprioceptors - sense body position and movements
By Distribution
General (somesthetic) senses - widely distributed
Special senses - limited to the head
Vision, hearing, equilibrium, taste, and smell
General Senses
Structurally simple receptors
One or a few sensory fibers and a little connective tissue
Unencapsulated nerve endings
Encapsulated nerve endings
Physiologically simple receptors
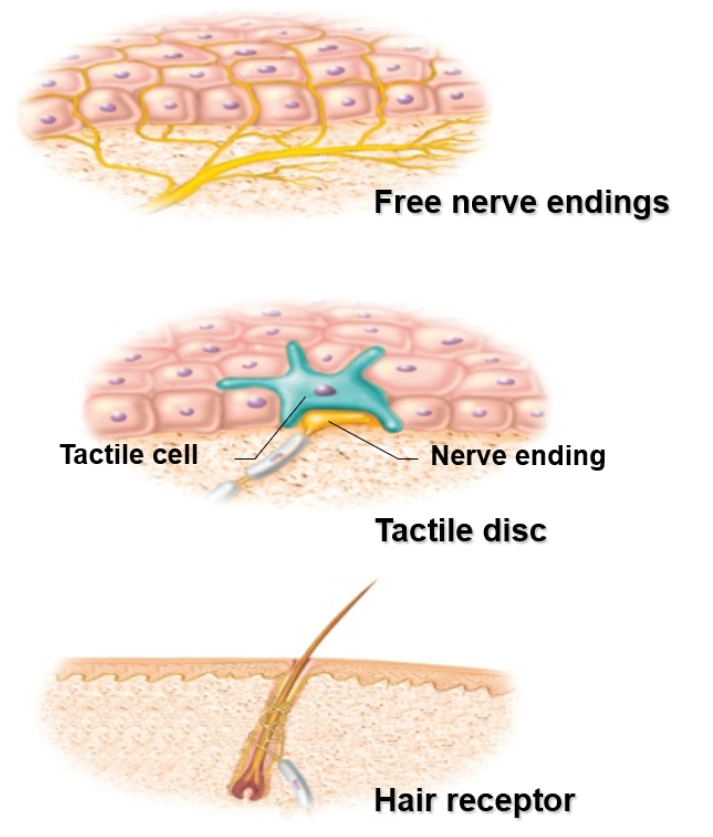
Unencapsulated Nerve Endings
Dendrites are not wrapped in connective tissue
Free Nerve Endings
For pain and temperature
Skin and mucous membrane
Tactile (Merkel) Discs
For light touch and texture
Associated with Merkel cells at the base of epidermis
Hair Receptors (Peritrichial Endings)
Wrap around the base of the hair follicle
Monitor the movement of hair
Encapsulated Nerve Endings
Tactile (Meissner) Corpuscles
Light touch and texture
Dermal papillae of hairless skin
Krause End Bulbs
Tactile
In mucous membranes
Bulbous (Ruffini) Corpuscles
Heavy touch, pressure, joint movements, and skin stretching
Lamellar (Pacinian) Corpuscles
Deep pressure, stretch, tickle, and vibration
Periosteum of bone, and deep dermis of skin
Muscle Spindles
Golgi Tendon Organs
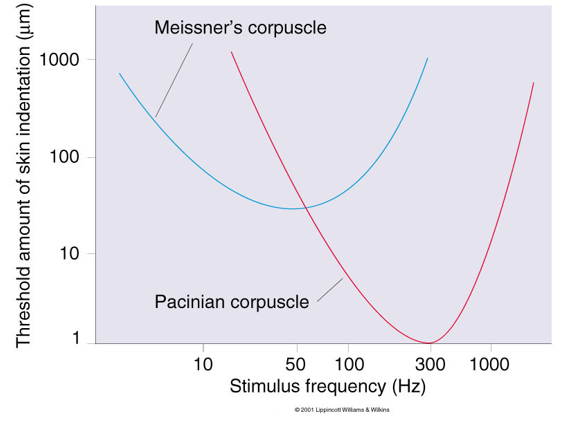
Vibration Sense
Texture sense and pitch sense vary according to the frequency of vibration
Tuning Curves measure sensitivity to varying frequency of stimulation
Meissner’s is more broadly tuned, less sensitive, and less rapidly adapting compared to Pacinian
Somesthetic Projection Pathways
From receptor to final destination in the brain, most somesthetic signals travel by way of three neurons
1st order neuron (afferent neuron)
From the body, enter the dorsal horn of the spinal cord via the spinal nerves
From the head, enter the pons and medulla via the cranial nerves
Touch, pressure, and proprioception on large, fast, myelinated axons
Heat and cold on small, unmyelinated, slow fibers
2nd order neuron
Decussation to the opposite side in the spinal cord, medulla, or pons
Ends in the thalamus, except for proprioception, which ends in the cerebellum
3rd order neuron
The thalamus to the primary somesthetic cortex of the cerebrum
Peripheral Nerves Undergo Regeneration
Undergo regeneration through Schwann Cells
Mature neurons do not divide, but they can regenerate in the PNS if the cell body remains intact
CNS regrowth is inhibited by oligodendrocytes and astrocyte-derived scar tissue
Three Levels of Motor Control
Cerebellum and basal nuclei (ganglia) plan and coordinate complex motor behaviors.
Motor control at lower levels is mediated by reflex arcs or governed by complex motor patterns
Three Levels:
Precommand Level (Highest)
Projection Level (Middle)
Segmental Level (Lowest)
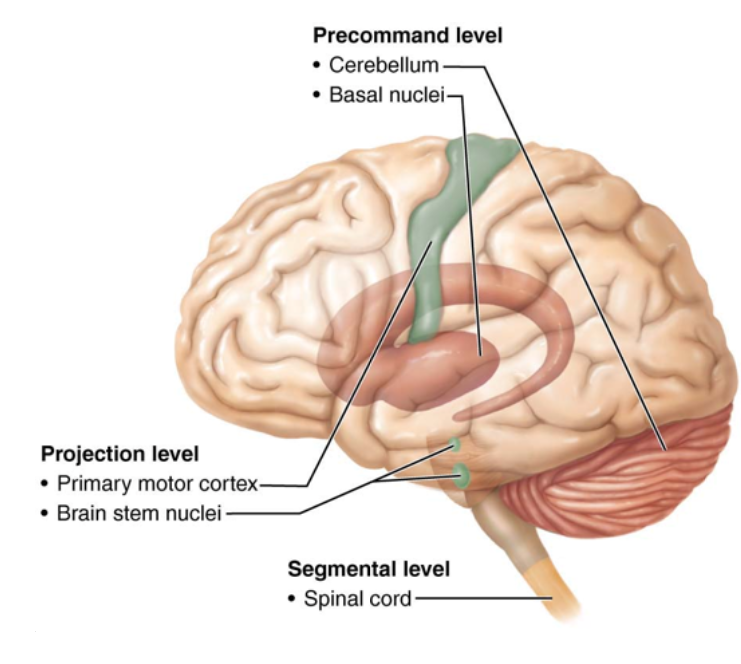
Segmental Level
Contains the reflexes and spinal cord circuits
Proximate executor of movement: direct connection to myofibers
Mediates automatic reflex movements
Segmental circuits
Activate ventral horn motor neurons in a group of segments
Stimulate specific groups of muscles
Central pattern generators
Circuits that control repeated motor activities
Inhibitory and excitatory neurons with rhythmic patterns of activity
Projection Level
Contains descending projection fibers
Convey information to lower motor neurons (LMNs)
Provide feedback to precommand level
Direct (pyramidal) pathways
Indirect pathways
Precommand Level
Contains the cerebellum and the basal nuclei
Unconscious planning—acts in advance of willed movements to control outputs of motor cortex
Precisely start/stop movements, coordinate them with posture, block unwanted movements
Cerebellum:
Integration of motor and sensory feedback: compares intentions to actions
“Fine tunes” motor activity by projecting to cortex (via thalamus) and brainstem
Basal nuclei:
Receives inputs from all cortical areas
Output to premotor and prefrontal cortex via the thalamus
Inhibits motor centers at rest, activation leads to motor initiation
Nature of Somatic Reflexes
Quick, involuntary, stereotyped reactions of glands or muscles to sensory stimulation
Automatic responses to sensory input that occur without our intent or often even our awareness
Functions by means of a somatic reflex arc
Stimulation of somatic receptors
Afferent fibers carry a signal to the dorsal horn of the spinal cord
One or more interneurons integrate the information
Efferent fibers carry impulses to skeletal muscles
Skeletal muscles respond
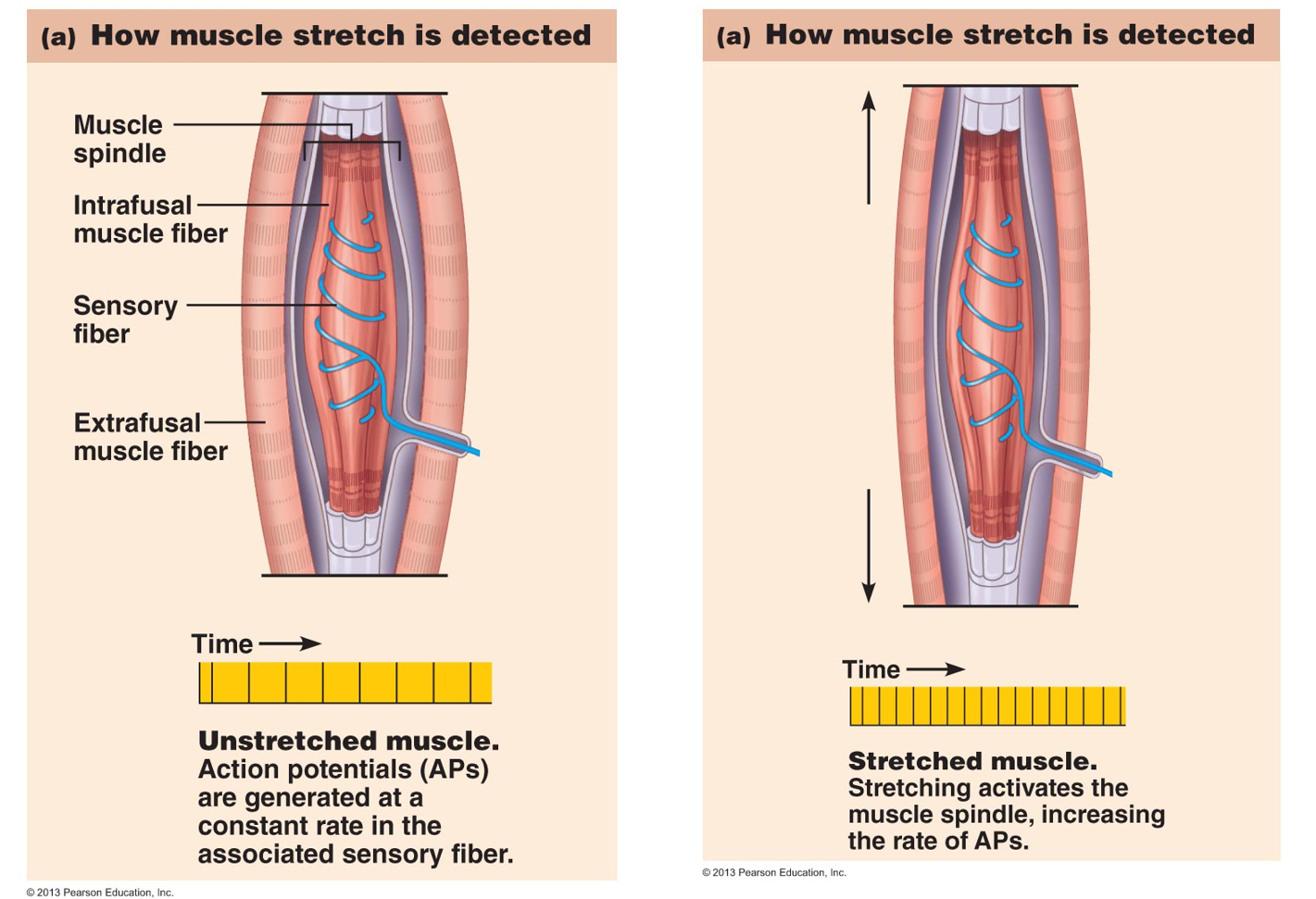
The Muscle Spindle
Sense organ (proprioceptor) that monitors length of muscle and how fast muscles change in length
Composed of intrafusal muscle fibers, afferent fibers and gamma motor neurons
The Stretch (Myostatic) Reflex
When a muscle is stretched, it contracts and maintains increased tonus (stretch reflex)
Helps maintain equilibrium and posture
Head starts to tip forward as you fall asleep
Muscles contract to raise the head
Stabilize joints by balancing tension in extensors and flexors, smoothing muscle actions
A very sudden muscle stretch causes a tendon reflex
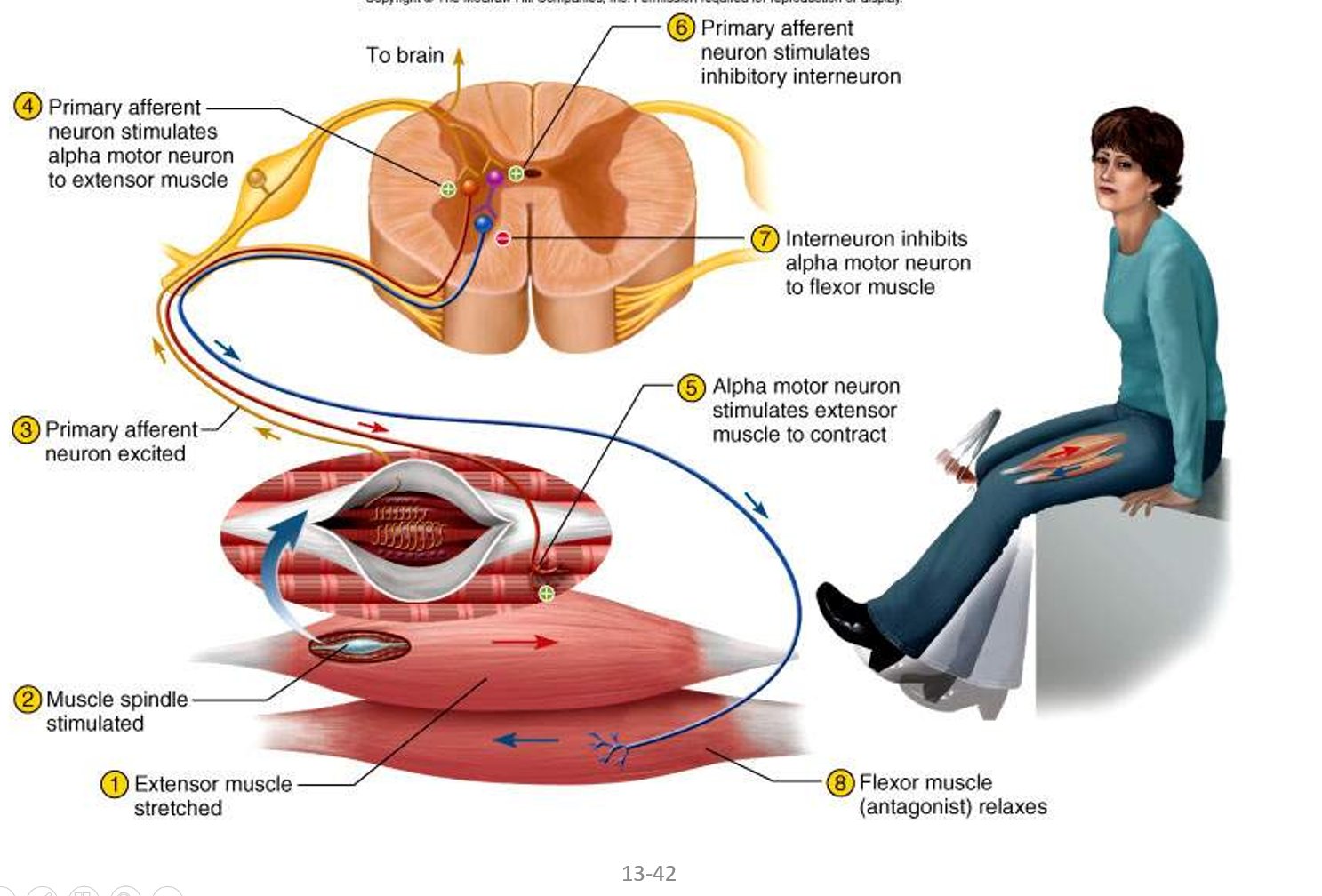
The knee-jerk (patellar) reflex is a monosynaptic reflex
Testing somatic reflexes helps diagnose many diseases
Reciprocal inhibition prevents muscles from working against each other
Simple Stretch Reflex
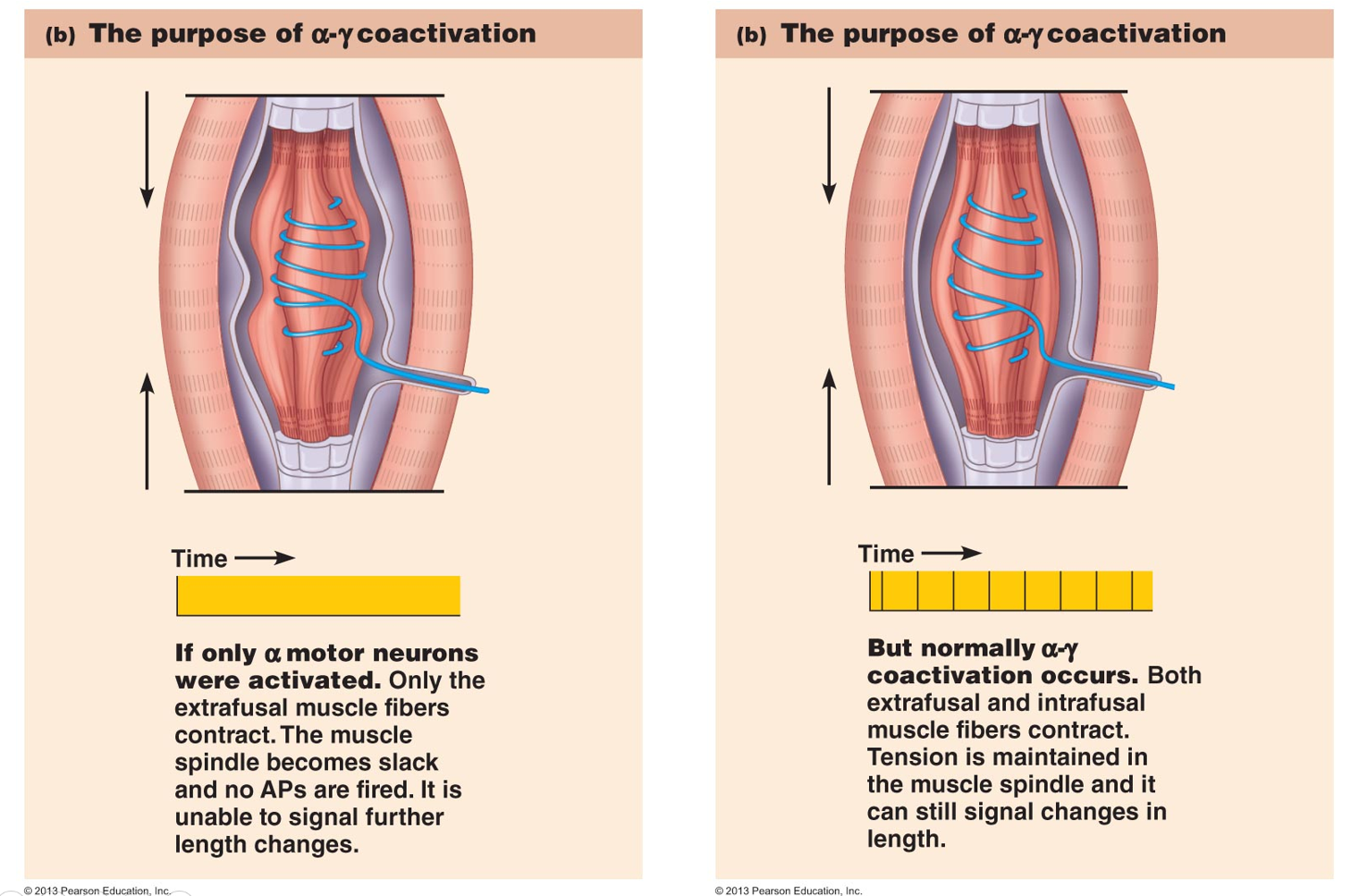
Functions of the Alpha - Gamma Coactivation Mechanism
Detect changes in muscle length, even when muscle is partially contracted
Monitor if the muscle (extrafusal fibers) shortened as commanded
A feedback mechanism to determine if recruitment is needed
The Patellar Tendon Reflex Arc
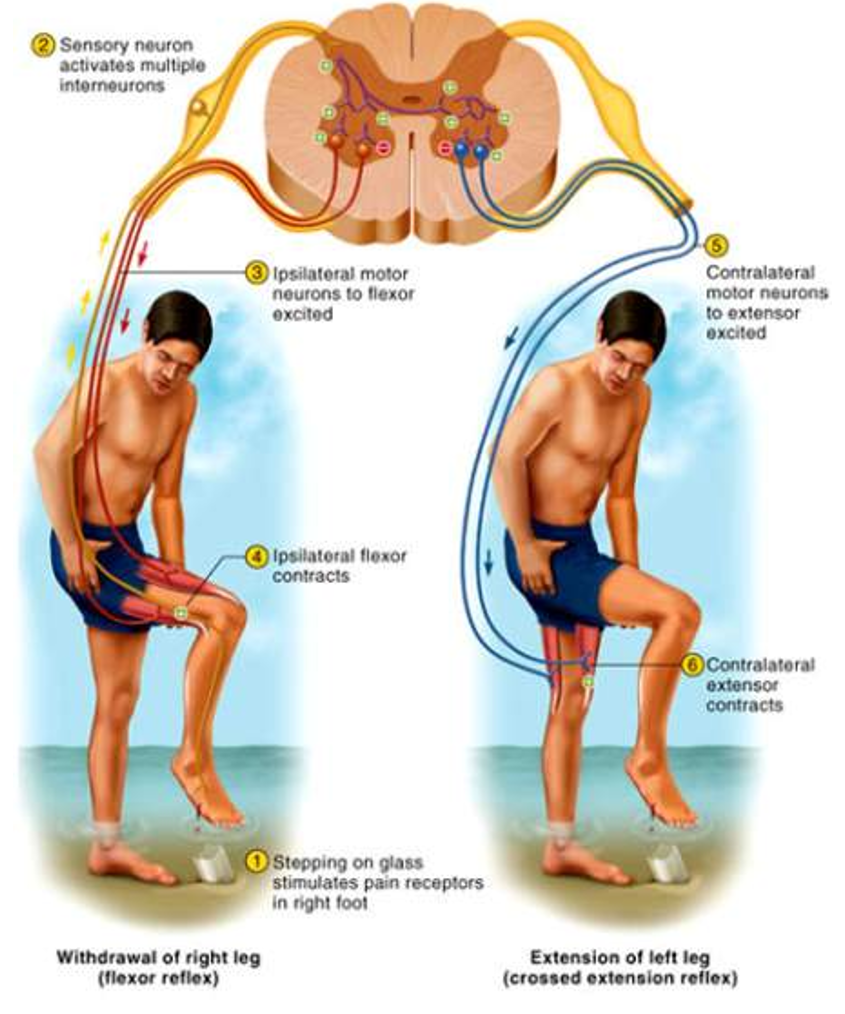
Flexor Withdrawal Reflexes
Occurs during withdrawal of foot from pain
Polysynaptic reflex arc
Neural circuitry in spinal cord controls sequence and duration of muscle contractions
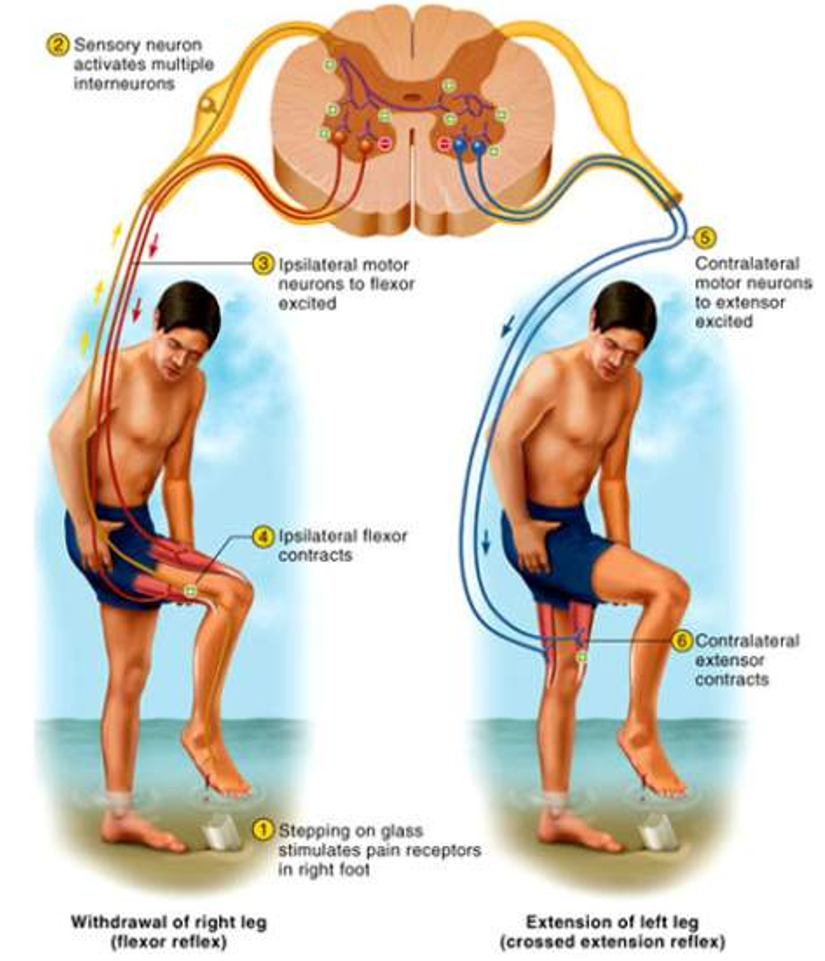
Crossed Extensor Reflexes
Maintains balance by extending other leg
Intersegmental reflex extends up and down the spinal cord
Contralateral reflex arcs explained by pain at one foot causes muscle contraction in other leg
Golgi Tendon Reflex
Proprioceptors in a tendon near its junction with a muscle -- 1mm long, encapsulated nerve bundle
Excessive tension on tendon inhibits motor neuron
Muscle contraction decreased
Also functions when muscle contracts unevenly
Spinal Cord Trauma / Injury
10-12,000 people/ year are paralyzed
55% occur in traffic accidents
This damage poses risk of respiratory failure
Early symptoms are called spinal shock
Tissue damage at time of injury is followed by post-traumatic infarction
Spinal Cord Injuries
Trauma
Tumours
Ischemia
Developmental Disorders
Neurodegenerative Diseases
Demyelinated Diseases
Transverse Myelitis
Vascular Malformations
Spinal Cord Trauma
Automobile Crashes
Falls
Gunshots
Diving Accidents
War Injuries
Etc…
Spinal Cord Tumours
Right Tumour
Ependymomas
Astrocytomas
Metastatic Cancer
Spinal Cord Ischemias
Occlusion of Spinal Blood Vessels
Including Dissecting Aortic Aneurysms
Emboli
Arteriosclerosis
Spinal Cord Developmental Disorders
Spina Bifida
Meningomyolcoele
Etc…
Spinal Cord Neurodegenerative Diseases
Friedreich's Ataxia
Spinocerebellar Ataxia
Etc…
Spinal Cord Demyelinative Diseases
Multiple Sclerosis
Etc…
Spinal Cord Transverse Myelitis
From Spinal Cord Stroke
Inflammation
Etc…
Spinal Cord Vascular Malformations
Arteriovenous Malformation (AVM)
Dural Arteriovenous Fistula (AVF)
Spinal Hemangioma
Cavernous Angioma
Aneurysm
Spinal Cord Injury (SCI) Immediate Response
Initial mechanical trauma secondary to traction and compression forces
Direct compression of neural elements by bone fragments, disc material, and ligaments damages CNS and PNS
Blood vessel damage leads to ischemia
Rupture of axons and neural cell membranes also occurs
Microhemorrhages occur within minutes in the central gray matter and progress over the next few hours
Massive cord swelling within minutes, leading to secondary ischemia
Loss of autoregulation and spinal shock cause systemic hypotension, exacerbate ischemia
Ischemia, toxic metabolic compounds, and electrolyte changes cause a secondary injury cascade
Spinal Cord Injury (SCI) Delayed Response
Hypoperfusion of gray matter extends to the white matter, altering propagation of action potentials along the axons, contributing to spinal shock
Massive release of glutamate leads to excitotoxicity - overstimulation of neighbor neurons, production of free radicals, death of healthy neurons
Excitotoxic mechanisms, via glutamate receptors, kill neurons & oligodendrocytes, leading to demyelination
Wave of apoptosis affects oligodendrocytes up to 4 segments from the trauma site days and weeks after the initial trauma
Spinal Cord Plegia
Plegia: paralysis, stroke, or a significant loss of muscle function
Extent of plegia dependent on position of injury
Cervical Injury:
Quadriplegia, loss of autonomic control
Thoracic Injury:
Paraplegia, respiration intact
Lumbar & Sacral Injury
Decreased control of legs, hips, urinary system and anus
Pain
Discomfort caused by tissue injury or noxious stimulation, and typically leading to evasive action
Important since helps protect us
Lost in diabetes mellitus – diabetic neuropathy
Nociceptors
Two types provide different pain sensations
Fast pain travels in myelinated fibers at 12 - 30 m / sec
Sharp, localized, stabbing pain is perceived with injury
Slow pain travels through unmyelinated fibers at 0.5 - 2 m / sec
Longer-lasting, dull, diffuse feeling
Somatic Pain
From skin, muscles and joints
Visceral Pain
From the viscera
Stretch, chemical irritants or ischemia of viscera (poorly localized)
Chemicals Released from Injured Tissue
Stimulates pain fibers
Bradykinin - most potent pain stimulus known
Makes us aware of injury and activates cascade or reactions that promote healing
Histamine, prostaglandin & serotonin also stimulate nociceptors
Projection Pathway for Pain
Two main pain pathways to the brain, and multiple subroutes
Head
Neck
Pain Signals from the Head
First-order neuron cell bodies in dorsal root ganglion of spinal nerves or cranial nerves V, VII, IX, and X
Second-order neurons decussate and send fibers up spinothalamic tract or through medulla to thalamus
Gracile fasciculus carries visceral pain signals
Third-order neurons from thalamus reach postcentral gyrus of cerebrum
Pain Signals from the Neck Down
Travel by way of three ascending tracts:
Spinothalamic Tract – most significant pain pathway
Carries most somatic pain signals
Spinoreticular Tract – carries pain signals to reticular formation
Activate visceral, emotional and behavioral reactions to pain
Gracile Fasciculus – carries signals to the thalamus for visceral pain
Referred Pain
Pain in viscera often mistakenly thought to come from the skin or other superficial site
Results from convergence of neural pathways in CNS
Brain “assumes” visceral pain is coming from skin
Brain cannot distinguish source
Heart pain felt in shoulder or arm because both send pain input to spinal cord segments T1 to T5
Steps of Pain Perception