Immunohematology
1/162
Earn XP
Description and Tags
Comprehensive Review
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
163 Terms
Epitope (antigenic determinant)
Which term refers specifically to the smallest portion of an antigen that is recognized by an antibody?
Immunogens can elicit an immune response; antigens may not
What best distinguishes an immunogen from an antigen?
IgM
Which antibody is most efficient at activating complement?
IgG - reacts best at 37°C and requires AHG for detection.
A weak antibody is detected only at AHG phase. Which is most likely?
IgM can span larger distances between RBCs; Pentameric structure → better lattice formation → visible agglutination.
Why does IgM produce stronger agglutination than IgG in saline?
IgM
Which immunoglobulin predominates in a primary immune response?
Secondary
A patient previously exposed to an antigen shows a rapid, high-affinity response. This is what kind of response?
Higher affinity antibodies
Which is TRUE of secondary immune responses?
IgG or IgM bound to antigen
What initiates the classical complement pathway?
C5b–C9
Which complement component forms the Membrane Attack Complex (MAC)?
Cell lysis, Opsonization, Inflammation
What are 3 functions of complement?
Too much antibody = false negative
What happens in antibody excess (prozone)?
Reducing ionic cloud around RBCs
Low ionic strength solution (LISS) enhances agglutination by:
False positives
Overcentrifugation may result in:
4+
A reaction showing one solid clump with clear background is graded:
1+
Microscopic agglutination with many free cells is:
Antigens encoded by a single gene or gene cluster
In transfusion medicine, a blood group system is defined by:
What is “dosage”?
Stronger reaction with homozygous cells
Codominant
Which inheritance pattern applies to ABO blood groups?
A, B, AB, O
A mother is type A (AO), father is type B (BO). Possible child types?
O
If both parents are type O, what are the possible offspring?
91%
A patient has anti-K (K antigen frequency ≈ 9%). What % of units are compatible?
31%
K-negative = 0.91
Fya-negative = 0.34
0.91 × 0.34 = ~0.31 (31%)
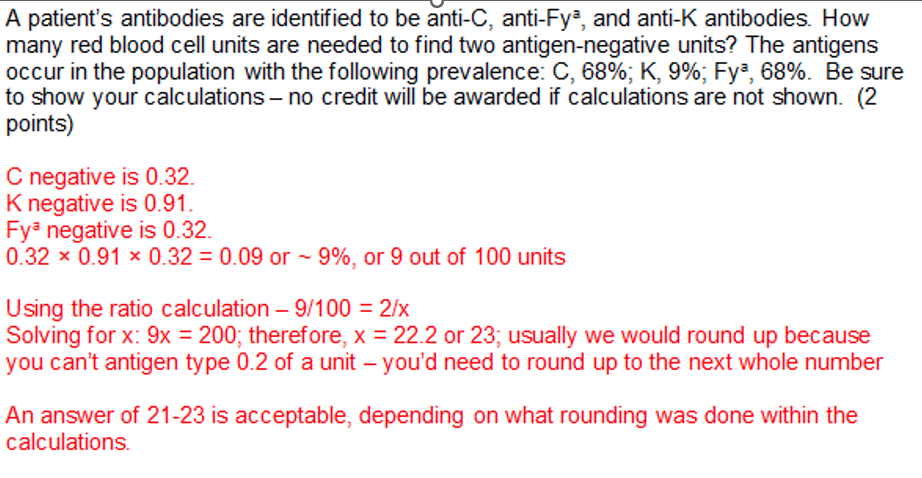
Patient has anti-K (9%) and anti-Fya (66%). Probability of compatible units?
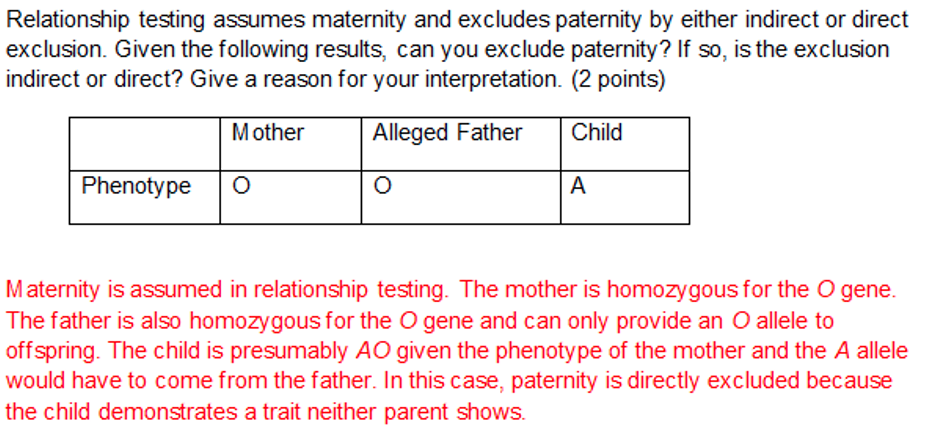
Direct exclusion
A child is type AB. Alleged father is type O. Conclusion?
Missing expected antigen
What indicates indirect exclusion?
Patient recently transfused
Molecular testing is most useful when:
Determines genotype independent of transfusion
What is a major advantage of molecular typing?
Antigen
Antigens bind antibodies, but may not trigger an immune response.
Binding ≠ stimulating
Which term refers to any substance capable of binding to an antibody?
Some antigens cannot stimulate an immune response
Immunogenicity requires immune activation, not just binding.
Hint: If it doesn’t “activate,” it’s not an immunogen
All immunogens are antigens, but not all antigens are immunogens because:
Epitope
Epitope = antigenic determinant.
Hint: Epi = “on top” → the part exposed to antibody
The specific site on an antigen that binds an antibody is called:
Antigenic determinant
What is another term for epitope?
Size and complexity
Larger, complex molecules (proteins) are more immunogenic.
Hint: Big + complex = immune system notices.
Which factor most strongly influences whether a substance is an immunogen?
Hapten
Classic example: drugs (e.g., penicillin).
Hint: Hapten = “helper needed.”
A small molecule that is not immunogenic alone but becomes immunogenic when attached to a carrier is:
Proteins or carbohydrates
In transfusion medicine, RBC antigens are typically:
Immunogen
It stimulated an immune response → immunogen.
Hint: If antibodies formed → it WAS immunogenic.
A patient develops an antibody only after transfusion. The antigen is best described as:
Antibody binds a specific site on antigen
Which scenario best represents an epitope-specific reaction?
It can bind multiple different antibodies
Multiple epitopes → multiple antibody binding sites.
Hint: More epitopes = more immune “targets.”
One antigen may have multiple epitopes. This means:
Hapten
Drug becomes immunogenic only when attached to RBC.
Hint: Classic “drug-induced hemolysis” setup.
A patient receives a drug that binds to RBC membranes and later develops antibodies. The drug alone is most likely a:
Epitope
A lab identifies an antibody reacting with only one part of an antigen. That part is the:
Polyclonal response
Multiple epitopes → multiple antibodies → polyclonal.
Hint: Mono = one epitope, poly = many.
A patient has antibodies to multiple epitopes on the same antigen. This is best described as:
Large protein with complex structure
Hint: Think: vaccines = proteins.
Which is MOST likely to be a strong immunogen?
They are less accessible or less foreign
Accessibility + foreignness matter.
Hint: If immune system “ignores” it → weak immunogen
Why are some RBC antigens weakly immunogenic?
Widely distributed and recognized as foreign
Which best explains why ABO antigens are highly immunogenic?
It cannot bind antibody effectively
No epitope = nothing to recognize
If an antigen loses its epitope structure, what happens?
Immunogenic antigen
Which mismatch is most likely to produce antibodies?
Immunogenic
A transfused patient develops antibodies 10 days later. The transfused RBC antigen must have been:
Epitope structure
A lab modifies an antigen so antibodies can no longer bind. What was most likely altered?
5 basic Ig molecules held together with a joinging (J) chain; pentamer
first responder; EFFICIENTLY activate complement
direct agglutination; immediate spin (IS) phase detection
IgM
bivalent; classic Y configuration
Key in HUMORAL immune response; infefficiently activates complement; CROSSES PLACENTA
inefficient in direct agglutination; ANTIGLOBULIN test detection
IgG
Primary
B cells are immune cells involved
smaller level of response
Ab produced in 5-10 days
IgM Immune response
MEMORY B cells are immune cells involved
LARGER level of response
Ab produced in 1-3 days
IgG Immune response
Strength of bond betw. Ab and Ag
Increases after each exposure
Higher in secondary (anamnestic) response
Due to affinity maturation
What is Ab affinity? In what stage of the immune response is Ab affinity higher? Why?
Classical is activated by Ag/Ab complexes
Ca and Mg
Anaphylatoxins, chemotactic, opsonization
How is the initiation of the classical complement pathway different from the alternative pathway? What ion must be present to activate the classical pathway? What are the biological effects of the activation of the complement cascade?
PRO = too much Ab
POST = too much Ag
bothat cause FALSE NEG
Prozone vs. Postzone
Temperature helps inc. the rate of the rxn.
IgG = warm temp = 37C = CINICALLY SIGNIFICANT
IgM = cold temp (room temp or below) = clinically insignificant
Why does temp matter in Ab/Ag rxns?
The lattice network of red cells may not form leading to a FASLE NEGATIVE interpretation
What would happen if the centrifuge speed is too low?
The shielding effect around the red cells are reduced allowing an inc. in Ab uptake
How does lowing the ionic strength of the test system affect agglutination rxns?
Finding units of blood when given prevalence
Relationship test - Direct vs. indirect exclusion
Immunogen
Foreign molecule that elicits an immune response
Blood group system
group of Ags in the RBC membrane that are related serologically and inherited though the same genetic inheritance pattern
dosage
variation in Ag expression because of the number of alleles present for a given trait
recessive
trait expressed in an individual only when inherited from both parents
Antigen (Ag)
foreign molecule that binds to an Ab or T-cell receptor
Law of independent Assortment
Genes on separate chromosomes behave randomly during meiosis
Phenotype
Determined by the presence or absence of hemagglutination of RBC Ags using specific antisera
Homozygous expression
Inheritance of 2 identical alleles for a given trait
Hardy-Weinburg equation
statistical formula to estimate the frequency of genetic diseases or observations of traits
Genotype
Genes inherited from each parent; determined through family studies or molecular testing
Heterozygous expression
inheritance of 2 different alleles for a given trait
Law of independent segregation
traits that are transmitted in a predictable fashion from one generation to the next
Epitope
antigenic determinant
dominant
trait expressed over another trait; requires inheritance of only one allele for expression
codominant
2 different inherited alleles are equally expressed in an individual
protiens are the best immunogens, then complex carbs
degree of foreignness - greater from self the more like it will cause an immune response
size > 10K Daltons
dosage and Ag density - # of RBCs and the amount of Ag they carry
route of admin - IM or IV injections are good at eliciting an immune response
What factors contribute to immunogenicity?
involves several WBCs
humoral - B cells receptors recognize foreign RBC Ags - B cell presents Ag to T cell - T cell cytokines tell B cell to turn into plasma cells that produce Abs (glycoproteins) with the same specificity as the B cell receptor - each plasma cell is a clone - Memory B cells also made at this time that can quickly respond if there is another exposure - Memory B cells dont need the T cell to be activated - think vaccination -
Describe the immune response in a transfusion setting
G - secondary immune response (anamnestic)
A - resides in mucus lining
M - primary immune response
D - Ag receptor on the naive B cell
E - activate mast cells = immediate hypersensitivity rxn
What are the 5 classes of Abs and their function?
pepsin and papain
What enzymes are used to divide Igs into the Fab and fc regions
heavy chain - variable and constant region that determines the class of Ag
light chain - variable and constant region made of only kappa and lambda
Fab region - Ag binding site
Fc region - determines the Ab function (contains complement binding region and cell activation region)
variable region - where the Ags bind on the heavy chain
hinge region - betw. Fc and Fab providing flexibility and 2 Ag binding sites
Ag binding site - Specificity determined by variable region that fits epitopes
macrophage binding site - opsonization and attaches to the Fc portion that signals activation = phagocytosis
Describe the regions of the antibody
extravascular hemolysis
Abs attached to RBCs signal clearance by liver and spleen
heavy chain - Mu / Gamma
light chain - kappa or lambda / kappa or lambda
J chain - yes / no
Molecular Wt - 900K / 150K
Valency - 10 / 2 (bivalent)
Total serum conc. - 5-10% / 70-80%
serum ½ life days - 5 / 23
crosses placenta - no / yes
activation of classical pathway of complement - very efficient (only needs 1) / not so efficient (needs 2)
Red cell clearance - intravascular / extravascular
detection in lab tests - IS = direct agglut. / AHG
structure - pentamer / monomer
exposure - acute or early / chronic or previous
IgM vs. IgG
intravascular hemolysis
complete activation of the classical pathway of complement and destruction of RBC
ABO is usually IgM
affinity maturation
the reason why Abs produce a stronger rxn after repeat exposure
IgG - Secondary Immune response
Anamnestic
w/in 1-3 days of exposure
higher conc. for longer because of memory B cells (larger # of plasma cells)
chronic or previous exposure
Lag after immunization - 5-10 days / 1-3 days
Peak response - smaller / larger
Ab isotype - usually IgM>IgG / Inc. IgG
Ab affinity - low avg. more variable / high avg. affinity maturation
Primary vs. secondary immune response
Immune complex
Antigen-Antibody Complex (combined Ab-Ag)
avidity
overall strength of rxn based on antigenic factor like size, shape and charge (goodness of fit)
overall stability and strength of the immune complex
influenced by Ab affinity and valency, size, shape, charge, noncovalent attractive forces
affinity
strength of binding betw. single Ab and epitope of an Ag affected by valency & fit of Ag
high affinity = binds quickly
Electrostatic forces (ionic bonds) - attraction based on opposite charges
hydrogen bonds - attraction of 2 neg charged groups for an H+ atom
hydrophobic bonds - weak bond from exclusion of water from the Ag-Ab complex
van der Waals forces - attraction betw. electron cloud (-) of one atom and the proton (+) w/in the nucleus of another atom
What are weak non-covalent bonds betw. Ab/Ag that hold the immune complex together?
transfusion rxn, anemia or HDFN (anemia and high levels of bilirubin in the fetus/newborn)
The destruction of RBCs result in what 3 thing?
alloantibodies
Abs produced in response to transfusion and pregnancies
Complement System
group of protein who’s responsible for antigen clearance, cell lysis and vasodilation
C1 - C9 circulate inactive as proenzymes - activation = active enzymes that enhance the immunological process
goal = opsonization, lysis of the target cells and stimulation of inflammatory mediators
C3→C3a (inflammation) & C3b (deposited on target cell for opsonization and phagocytosis)
C5→C5a (inflammation) & C5b →C9 = cell lysis
Complement proteins form membrane attack complex
Classical Pathway Described
Complement proteins react in specific seq. resulting in cell lysis
AB-Ag complex → C1 binds to Ab → activates C4, 2 then 3 → C1 splits C4 and C2 into a & b fragments → b binds to the cell and a enhances inflammatory response → C4bC2a complex forms called C3 convertase that converts C3 into active form which splits C3 into fragments → C3 convertase join with C3b to form C5 convertase which splits C5 → C5 to C9 = MAC causing lysis → MAC attaches to cell surface producing holes in the cell membrane and osmotic lysis
Alternative Pathway Described
Initiated by cell surface constituents
Results of Complement Activation
Anaphylatoxins - C3a, C4a and C5a complement proteins recruit phagocytes and promote inflammation, attach to mast cells and promote release of vasoactive amines (makes blood vessels permeable for fluid and cells to enter the area)
Chemotaxis - C5a attracts Neut. and Plt. to site of injury
Opsonization - C3b and C4b are Opsonin - molecule binds to Ag to promote phagocytosis & making the process most efficient → phagocyte + opsonin = really efficient phagocytic process → they also have a “c” & “d” fragment → d fragments can attach to red cells also
Mononuclear Phagocyte System
Present in secondary lymphoid organs - liver, spleen (largest), liver, lungs that clears old cells and ab-ag complexes
Stages of Agglutination
SENSITIZATION
Ab binds to Ag on the red cell membrane
recognition → antigenic determinants on RBC combine w/ Ag binding site on Ab → no visible agglut.
more Abs = better chance of collision events → relies on serum to cell ratio → add patient serum if rxn is weak
temp - IgG, 37C; IgM < or = 22C
Incubation - IS or after a specific time at 1-8C, RT or 37C
pH - 7.0
Ionic strength - can be adjusted with reagents
LATTICE FORMATION
Cell-Cell interactions - random collisions betw Ab coated cells develop cross-linkages = visible agglut.
Antigenic determinants bind with Ab binding sites on adj. cells (IgM because it is larger = direct agglutimation)
zeta potential - dist. bewt. cells caused by charged ions
zone of equivalence - Ag and Ab conc. → prozone = too much Ab = false neg → postzone = too much Ag = false neg
Centrifugation - time & speed to bring cells closer together → over = false pos & under = false neg
2-5% red cell suspension in salineis optimal
anti-I and anti-M
What antibodies are readily detectable when the pH is reduced?
Grading Agglutination
shake and tilt tube until button fully resuspended
0 - all red cells completely resuspended, red cells flow off button during grading
1+ - medium and small agglutinates - turbid background/many free cells
2+ - many medium agglutinates - clear background
3+ - several large agglutinates - clear background
4+ - RBC button is solid - clear background
HEMOLYSIS IS A POSITIVE RXN!
If activated by an immune complex → complement system → MAC → membrane damage → intracellular fluid released
Serum = active complement proteins
Plasma = anticoagulant binds Ca (needed to activate complement) → no complement activation
Abs to the LEWIS system Ags and Anti-Vel
What red cell Abs naturally display hemolysis?