PSYC 2400: Resilience Lecture
1/24
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
25 Terms
What is stress?
Stress is not just a reaction to external threats, but a biological and psychological state that emerges when safety is absent.
old view - stress triggered by external threat
new view - brains threat system is active by default, stress occurs when safety signals are weak; stress = absence of safety and not just presence of danger
Biological:
The amygdala (threat detection)
The prefrontal cortex (regulation and control)
The parasympathetic nervous system (PNS), especially via the vagus nerve (calms)
physiological — RSA - high RSA - calm, low RSA - stress
depends on perception of safety of social relationships, environment cues
What is adversity?
Adversity is a broad umbrella term referring to events or conditions that threaten health and well-being; normal and common, not rare. it varies across severity, chronic, timing, type, subjective meaning
It includes experiences like:
Injury, illness
Bullying or peer victimization
Moving
Family dysfunction
Key distinction:
Adversity = the event or condition
Stress = the experience/response to it
What are the kinds of life events categorized as childhood adversities?
Threat-related experiences where child safety is at risk - Exposure to violence, Abuse, Dangerous environments
Deprivation-related experiences - Lack of cognitive stimulation, Lack of resources, Neglect, Household dysfunction, Social disadvantage
Ex. Death of loved ones, Divorce, Verbal conflict, Bullying, Witnessing distressing events, Moving
These are extremely common—most children experience multiple.
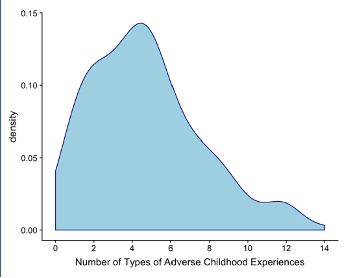
Early Life Stress Interview
Method:
Sample: Children ages 9–13, included both highly advantage youth and less advantaged but more on advantage side
Assessed 30+ types of stressful/adverse experiences
Follow-up questions captured subjective experience
Independent raters coded severity
Included both high SES and lower SES groups
Key Findings:
97% reported at least 1 adverse experience
Most common number = 5–6 experiences per child
Even privileged children showed high exposure
Conclusion:
Adversity is nearly universal
Not limited to “at-risk” populations
Why is it important to study adversity?
Highly prevalent (majority of children experience at least one; many experience several) - more than half in US experience 1 adverse event
A powerful predictor of mental health - includes internal + external
~50% of childhood psychiatric disorders
1/3 of adult-onset disorders
Linked to physical health outcomes - immunity dysfunction
Diabetes
Heart disease
Cancer
Inflammatory conditions
It also:
Has long-term effects across the lifespan (affect immediately and years later as it shapes emotional and cognitive functioning)
Can affect future generations (intergenerational transmission - parenting behaviors, prenatal environment, child develop)
alters brain development and biological systems (changes in hippocampus, amygdala, prefrontal cortex)
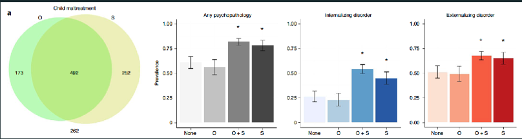
objective v subjective adversity and psychopathology
Four groups:
Objective + Subjective:
Documented adversity + self-reported
Interpretation: objective history matches memory/report
Objective Only:
Documented adversity but NOT reported
Interpretation: forgetting, repression, denial/unwillingness to disclose, or different interpretation
Subjective Only:
No documentation but self-reported
Interpretation: unrecorded experiences OR perception/interpretation as adverse
Highlights limitations of official records
Neither Objective nor Subjective:
No documentation + no self-report
Likely lowest exposure group (NOT guaranteed none)
Measures (outcomes assessed):
Internalizing disorders: Anxiety, depression
Externalizing disorders: Behavioral problems, aggression
Finding: Same pattern across ALL mental health outcomes
Key findings:
Strongest predictor = subjective recall/report (NOT objective exposure)
Individuals who report adversity (subjective groups) → higher psychopathology
Individuals with objective records but NO subjective recall → lower psychopathology
Similar to those with no documented or reported adversity
Individuals in objective-only or neither groups may still have unrecognized/unreported adversity
Impact / Conclusion:
Not just what happened matters — but whether/how it is remembered
Subjective experience + memory are critical for mental health outcomes
Objective records alone are NOT sufficient to predict risk
Many individuals across groups may still have some level of adversity exposure
Key definitions (explicit):
Objective adversity: Court-documented childhood maltreatment
Subjective adversity: Adult self-reported childhood maltreatment history
What are different types of adversity and stress studied?
Toxic stress Chronic, high stress + lack of support - MOST DAMAGING
Traumatic stress - single severe event (e.g., disaster, assault)
Chronic vs. acute stress Chronic = repeated over time more harmful biological, Acute = sudden, short-term
Threat vs. deprivation adversity Threat = danger (violence), Deprivation = lack of resources/stimulation
Objective vs. subjective adversity, Objective = documented (e.g., court records), Subjective = personal perception/report
Cumulative adversity - Total number and severity of experiences
Timing and exposure - When it occurs (prenatal, childhood), Direct vs. indirect exposure
Intergenerational study
Children of mothers with adversity showed:
Lower vagal tone
Indicates reduced parasympathetic regulation
Behavioral problems
Reduced intracranial volume (brain size)
Altered brain connectivity
Specifically in emotional regulation networks
Mechanisms:
Prenatal stress
Parenting behaviors
Maternal mental health
Conclusion:
Adversity can be transmitted across generations, affecting children even before birth
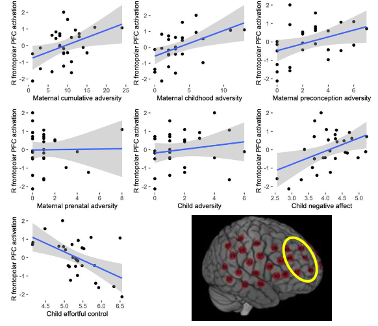
fNIRS study
Sample: 150 families
Maternal adversity (risk factors):
Measured through maternal self-reports
Includes family/environmental stressors (e.g., hardship, stress, contextual risks affecting child)
Cognitive task (inhibitory control):
Children repeatedly touch a screen but must occasionally inhibit/stop their response
Measures ability to override automatic behavior and control impulses - Focus on prefrontal cortex (key for cognitive control)
Child temperament (negative control): Children who are more sensitive, reactive, easily distressed
Key findings:
Prefrontal oxygenation (brain activity) is linked to Maternal risk factors, Child temperament (negative reactivity/control)
fNIRS findings across studies:
Prefrontal oxygenation increases as task difficulty increases
More difficult tasks → greater neural resource recruitment
Main results:
Children with higher maternal adversity + more negative temperament → Show greater prefrontal oxygenation during tasks
Indicates increased brain activation during inhibitory control
Interpretation:
Increased activation = more neural effort/resources required — Cognitive control tasks are more effortful at the neural level for these children - Even if behavior looks similar, their brains are working harder
Conclusion / Impact:
Maternal adversity is associated with increased right prefrontal activity in children
Children exposed to higher risk are not incapable, but:
Must recruit more neural resources
Tasks are harder at the neural level to achieve the same performance
Demonstrates how early environmental risk influences brain function, not just behavior
What are ways to measure stress and adversity?
Reports
Child self-report
Parent report
2. Objective records
Court documents (abuse, neglect)
3. Interviews
Early Life Stress Interview
Captures severity + subjective experience
Key measurement insight:
Must consider:
Severity
Chronic vs. acute
Timing
Direct vs. indirect exposure
What are the two definitions of resilience?
Definition 1 (Panter-Brick & Leckman):
Resilience is the process of harnessing biological, psychological, social, and cultural resources to sustain well-being
Definition 2 (Masten et al.):
Resilience is the capacity of a dynamic system to adapt successfully to challenges that threaten function, survival, or development
Key idea:
Resilience is not a trait, but a process + outcome
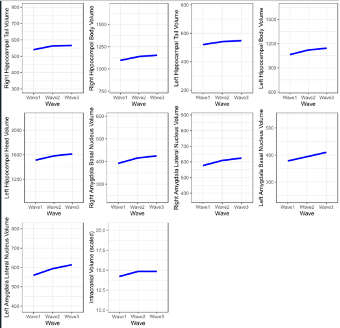
Study design (longitudinal waves):
Wave 1: 4½ years
Wave 2: 6 years
Wave 3: 7½ years
Measured growth trajectories over time
Brain regions examined: Hippocampus Amygdala Intracranial Volume (ICV) → overall brain volume
Key findings on growth patterns:
Brain growth is NOT constant over time
Growth is nonlinear (changes in rate across development)
Age-related growth differences:
4½ → 6 years: Steeper slope → rapid growth period
6 → 7½ years: Less steep slope → slower growth rate
Individual differences: Significant variability among children
Differences in: Starting point (initial brain size) Growth rate over Tim → Not all children develop at the same speed
Interpretation of variability:
Faster/slower growth may reflect: Environmental influences Indicators of risk or adaptation
Overall conclusion:
Growth in hippocampus, amygdala, and ICV is nonlinear and highly variable
There is substantial individual variation in both initial size and pace of development across childhood
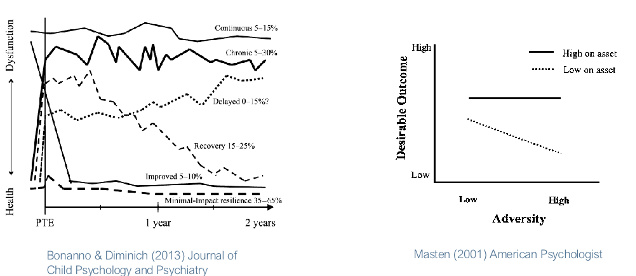
Trajectory Study of Resilience
Longitudinal tracking of individuals
Measured well-being: Before adversity Immediately after Over time
LEFT GRAPH: Trajectories of well-being over time (before → after adversity) (applies to many events: loss, divorce, military, accidents, etc.)
Minimal-impact resilience (35–65%, most common):
Stable functioning before, Small, temporary distress afte Quick return to baseline → no long-term disruption
Recovery pattern: Functioning well before
Significant distress after event Gradual return to baseline over time
Chronic dysfunction:
High distress after event Symptoms remain elevated long-term
Continuous maladjustment:
High distress before AND after Reflects ongoing vulnerability, not just the event
Post-traumatic growth (less common):
Lower functioning before Improved well-being after event Positive psychological change (e.g., new perspective, gratitude, life meaning)
RIGHT GRAPH: Resilience & protective factors
Focus: what protects people, not just what harms them
Types of protective factors: Internal: personality traits, coping skills External: supportive family, peers, social connections
Moderation model:
Protective factors moderate (change) the relationship between adversity and outcomes
With protective factors:
Reduce or even eliminate negative effects of adversity
Without protective factors:
Stronger negative impact of adversity
Bottom line:
Adversity ≠ destiny
Outcomes depend on access to protective resources
Explains why many people exposed to adversity still do well
Internal and external sources of resilience
Internal factors: Personality traits, Coping skills, Emotion regulation, Self-control
External factors: Supportive family, Friends/peers, Social relationships, Community resources
Resilience comes from everyday resources, not rare traits; Resilience factors moderate (change) the relationship between adversity and outcomes: When protective factors are present — The negative impact of adversity is reduced or even eliminated; When protective factors are absent —- The negative impact becomes much stronger
What is Polyvagal Theory?
RSA is a measure of vagus nerve/parasympathetic activity.
High RSA indicates strong vagus nerve activity, supporting the slowing of heart rate and decreased arousal.
High vagus nerve activity is involved in evaluating the environment as safe and supporting social engagement. High vagus nerve activity as indexed by high baseline RSA is often linked to better outcomes.
In contrast, if vagus activity is consistently low (low RSA), this is a sign that your nervous system does not evaluate the environment as safe, and that you're typically in a defensive state that doesn't allow you to effectively interact with others (e.g., misread people, act aggressively, etc.)
Low vagus nerve activity as indexed by low baseline RSA is often linked to worse or less socially desirable outcomes.
Higher RSA →
Better emotional regulation
Better social competence
Adaptive response:
RSA decreases during challenges
Conclusion:
RSA reflects ability to detect safety vs. threat
nonadaptive models of stress/adversity
Early environment leads to damage vs. optimal development
Adversity = negative outcomes, supportive environments = positive outcomes
Key assumptions:
Development is linear and cumulative
Good early environment → always good outcomes
Bad early environment → poor outcomes (unless partially repaired)
Phenotype concept: Early environment creates a fixed developmental/brain phenotype
Supportive environment → “good/optimal” phenotype
Adverse environment → “bad/suboptimal” phenotype
Outcomes:
Good early environment → positive functioning regardless of future
Bad early environment → maladaptation and poor outcomes
If environment improves → possible partial recovery (“catch-up”)
Connection to toxic stress model:
Early stress damages the brain Effects are long-lasting, Continued stress → worse outcomes, Improved environment → some reduction in harm
Bottom line:
Early adversity = damage model
Outcomes are largely fixed by early experience
Adaptive models of stress/adversity
Early environment programs the brain/nervous system for a predicted future environment Development is about adaptation, not just damage
Key mechanism:
Early experiences shape behavioral and neural phenotype
This acts as a “prediction” (biological bet) about future conditions
Match vs. mismatch:
Match (early = later environment): Phenotype is adaptive → better functioning + survival advantage
Mismatch: Phenotype becomes maladaptive → poor adjustment
Key principle: Traits are NOT inherently good or bad Their value is context-dependent
Examples:
Supportive early environment:
Produces calm, open phenotype
Works best in safe, stable future
Struggles in harsh/unpredictable environments
Adverse/unpredictable early environment:
Produces threat-sensitive, hypervigilant phenotype
Works best in dangerous/unpredictable future
Becomes maladaptive in safe environments (e.g., anxiety)
Bottom line:
Early adversity does not just harm—it prepares
Outcomes depend on fit between early and later environments
Adaptation ≠ always beneficial (depends on context)
Stress acceleration hypothesis
Harsh/adverse environments → faster development (accelerated maturation)
Leads to earlier independence and “growing up faster”
Adaptive logic (why this happens):
In high-adversity environments:
Caregivers may be unreliable/unavailable
Children must become self-sufficient earlier
Faster development may:
Help cope with instability/threat Increase survival + reproductive success
Key requirements for it to be adaptive:
Adversity → accelerated development (environment shapes faster growth)
Accelerated development → better outcomes (must reduce risk in that context)
BOTH must be true
Findings:
In high-adversity environments:
Accelerated development → better adjustment, fewer negative outcomes Acts as a protective/buffering factor
Without acceleration → Greater vulnerability, worse outcomes
Important nuance:
Context-dependent (NOT universally beneficial)
In low-adversity/safe environments:
No need to “grow up fast”
Acceleration does not occur or provide benefit
Bottom line:
Accelerated development is an adaptive response to adversity
Helps individuals function better in high-risk environments, but only in that context
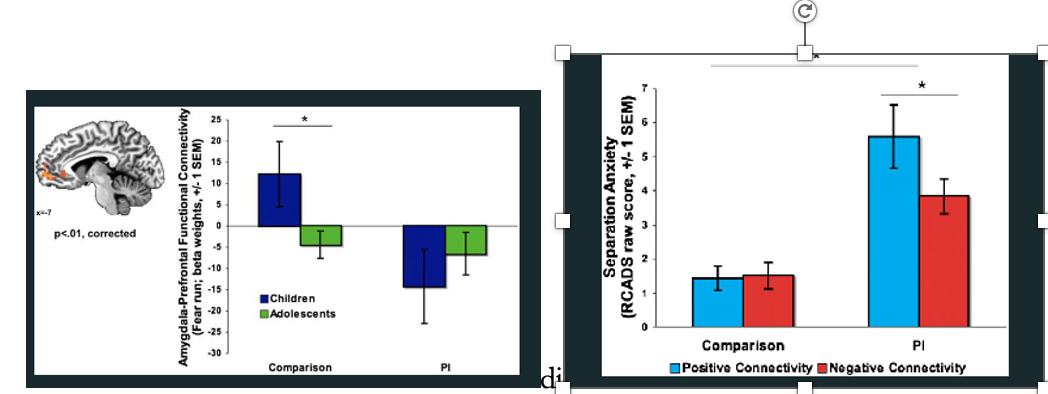
Romanian Orphanages - Institutionalized Children - SAH
Previously institutionalized children (Romanian orphanages = severe deprivation, low social/cognitive input, neglect/abuse)
Control group (raised by biological families)
Key brain system THIS IS NORMAL:
Frontoamygdala connectivity (emotion regulation)
Normative development:
Childhood → positive connectivity (less mature; co-activation)
Adolescence → negative connectivity (mature; prefrontal cortex regulates amygdala)
Key finding (Step 1: adversity → accelerated development):
Institutionalized children show negative connectivity already in childhood → Earlier-than-normal emergence of mature brain pattern → Evidence of accelerated neural development
Key finding (Step 2: does it improve outcomes?):
Institutionalized children overall have higher anxiety risk
BUT: Those with negative (mature) connectivity → lower anxiety
Those without it → higher anxiety → Acceleration reduces risk (doesn’t eliminate it)
Control group (low adversity):
Connectivity pattern NOT related to anxiety → No added benefit in safe environments
Putting it together (Adaptive Model):
Step 1: Adversity → accelerated development ✔
Step 2: Acceleration → better outcomes (in adversity) ✔
Step 3: Benefit is context-specific ✔
Conclusion:
Early adversity → earlier maturation of emotion regulation systems
This neural pattern is an adaptive response
Helps children cope better in high-risk environments
Not all children show this, but those who do → better outcomes than peers
Stress inoculation hypothesis
early moderate stress acts like a vaccine, reducing sensitivity to future stress.
Moderate stress exposure strengthens the stress response system.
Like a vaccine exposes the body to a mild virus to build immunity, moderate stress “trains” the brain and stress hormones to respond more effectively later.
Early moderate stress → system learns how to respond
Later stress → more controlled, regulated response
Outcomes of moderate early stress:
Increased resilience
Better emotional regulation
Lower emotional reactivity
More adaptive coping
More flexible stress response system
Important distinctions:
❌ Too little stress → lack of preparedness
❌ Too much stress → dysregulation & negative outcomes
✅ Moderate stress → resilience and adaptive functioning

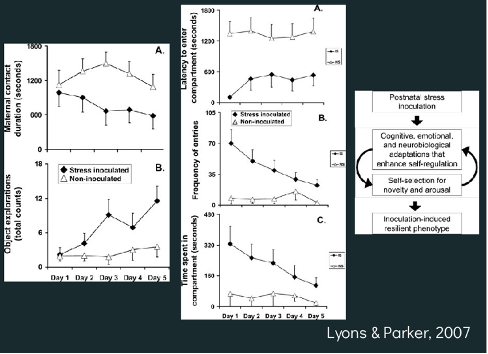
Monkey Study - SIH
Stress-inoculated group: Monkeys experienced weekly brief social separations (moderate stress).
Control group: No separations; stable social environment.
Later, both groups were exposed to stress-inducing situations.
Key Findings:
Response to Novel Objects/Environments
Inoculated monkeys → more exploration, less fear, less clinging
Control monkeys → more hesitation, more anxiety, more clinging
(Exploration of novelty = lower anxiety / greater confidence)
Stress Hormone Response (Cortisol Test)
Inoculated monkeys → lower cortisol response to stress (e.g., restraint)
Control monkeys → higher cortisol response
Conclusion:
Moderate early stress “trains” the stress response system, leading to:
Lower physiological stress reactivity
Greater exploration
Reduced anxiety-like behavior
Better adaptation to future stressors
Moderate early stress → adaptive, controlled resilience.
Biological aging measures
Telomeres
Shorter telomeres = faster cellular aging
Linked to adversity
2. Puberty timing
Adversity → earlier puberty
3. Brain development (pace of growth)
Changes in:
Hippocampus
Amygdala
Overall brain volume
Adversity →
Faster or altered development
Sometimes accelerated brain “age”
Key idea:
Adversity can speed up biological aging
pandemic brain study + hippocampal growth study
andemic brain study:
Adolescents showed older brain age than expected
Longitudinal hippocampus study
Longitudinal (followed children to ~age 15)
Focus: early adversity (prenatal + early postnatal) → later outcomes
Perinatal adversity score (cumulative risk):
Risk factors: smoking during pregnancy, maternal depression (pre/postnatal), low SES, low maternal education, birth complications (e.g., low birth weight)
Protective factors: good maternal mental health, high SES
Higher score = more early adversity (even before birth)
Key mental health finding:
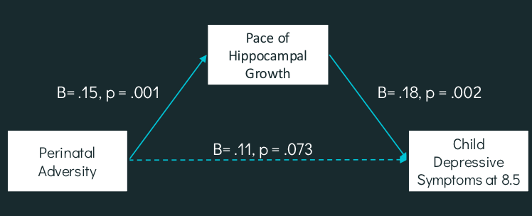
Higher adversity → more depressive symptoms at age 8.5
Effect is significant but small
Hippocampus (memory + emotion, stress-sensitive):
Higher adversity → Faster hippocampal growth, Smaller overall volume early in life
Mediation (mechanism):
Adversity → hippocampal changes → depression
When hippocampus is included → direct adversity–depression link weakens
Interpretation:
Adversity alters brain development, which then affects mental health
Faster growth = accelerated/altered development due to stress
Important nuance:
High-adversity kids show faster growth BUT still lag behind peers
By ~age 7 → developmental gap remains
Bottom line:
Early adversity (even before birth) → long-term brain + mental health effects
Acceleration ≠ advantage (they don’t “catch up”)
What is skin-deep resilience?
Outward success + internal physiological cost
Individuals may show:
High achievement
Good mental health
BUT also:
High inflammation
Insulin resistance
Cardiovascular risk
Why?
Constant effort and self-regulation under adversity →
Chronic stress activation
“Wear and tear” on the body
Key idea:
Resilience is not always free—it can come with hidden biological costs
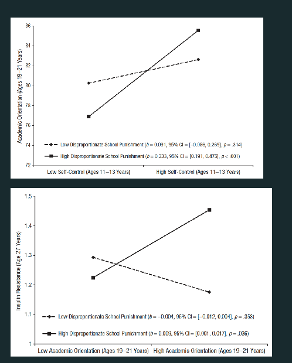
Skin deep resilience study
Researchers studied Black adolescents in schools that varied in disciplinary bias.
School Context:
Some schools disproportionately punished Black students (high discrimination).
Others showed less bias.
Psychological & Academic Findings:
In high-discrimination schools, high self-control predicted:
Greater academic orientation
Higher educational attainment
Higher income in adulthood
Better mental health
→ Self-control functioned as a protective factor in harsh environments.
Physiological Findings (Same Individuals):
Despite outward success, these youth showed:
Higher insulin resistance
Higher inflammation
Increased blood pressure
Interpretation:
Success required sustained self-regulation in stressful contexts.
Chronic activation of the stress response led to long-term physiological costs.
Even with upward mobility, structural inequalities (healthcare access, resource gaps) persisted.
Moving into higher-status environments may also bring isolation, pressure to fit in, or distance from cultural community.
Conclusion:
In discriminatory environments, self-control promotes achievement — but may increase long-term cardiometabolic risk.