Weeks 7-8 PHAR3913
1/50
Earn XP
Description and Tags
Contraception, Perinatal medicine, Infertility, Pregnancy Termination, Drug Safety in Pregnancy and Lactation, Complimentary Medicine in Pregnancy
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
51 Terms
Emergency contraception options available


Levonorgestrel Emergency Contraception: Use within how many hours?

Urlipristal Emergency Contraception: Use within how many hours?

After emergency contraception, when can you start/resume hormonal contraception?

If patient has taken a progestogen in the last 7 days (such as their usual hormonal contraception), which oral emergency contraceptive is prefered?

Copper IUD Emergency Contraception: Insert within how many hours?

If patient is using hormonal contraception, what situations define contraceptive failure that warrants emergency contraception?
In most cases, which oral emergency contraceptive is preferred (most effective)? And when is it not preferred?

What is folic acid (folate) supplementation during pregnancy used for?
To reduce risk of neural tube defects such as spina bifida or anencephaly by 72%
When to take folic acid (folate) during pregnancy?
For minimum 1 month before conception and the first 12 weeks of pregnancy
What is iodine supplementation during pregnancy used for?
To avoid poor infant neurodevelopment
What is Vitamin D supplementation during pregnancy used for?
To improve maternal Vitamin D levels when the mother is deficient. May reduce the risk of pre-eclampsia, low birthweight and preterm birth
What is iron supplementation during pregnancy used for?
To reduce the risk of low birth weight, maternal anaemia and iron deficiency
What is the current evidence for Vitamin C during pregnancy?
Evidence does not support routine high dose (1,000 mg/day) vitamin C supplementation for fetal loss. May cause harm
What is the current evidence for Vitamin E during pregnancy?
Insufficient evidence to conclude efficacy and safety during pregnancy. May cause harm.
What is the current evidence for Vitamin A during pregnancy?
Evidence does not support vitamin A supplementation for the prevention of fetal loss, maternal mortality or preterm birth
What is calcium supplementation during pregnancy used for?
To reduce the risk of gestational hypertension and pre-eclampsia
Prevalence of morning sickness (nausea and vomiting in pregnancy) in NSW
Occurs in 69% of pregnant women in NSW
When does morning sickness (nausea and vomiting in pregnancy) begin and end?
Begins in weeks 4-9
Ceases at 16-20 weeks for 9 out of 10 women
What is the severe form of morning sickness (pregnancy nausea and vomiting) called and how many women in NSW are affected?
Hyperemesis gravidarum
~1% of pregnant women in NSW
What are the symptoms of hyperemesis gravidarum?
Severe nausea or vomiting
Inability to drink or eat normally
Limitations to daily activities
Dehydration or electrolyte abnormalities
In pregnancy, what does NVP stand for?
Nausea and Vomiting in Pregnancy (morning sickness)
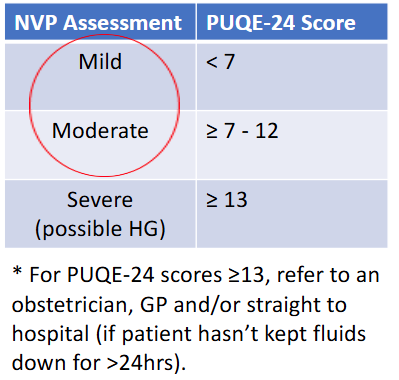
What 3-question tool can be used to quickly quantify the severity of nausea and vomiting in pregnancy?
PUQE-24: Pregnancy Unique Quantification of Emesis 24
What are the PUQE-24 score classifications for NVP? And which scores warrant referral?
How to optimise vitamin and mineral supplements in the management of nausea and vomiting (morning sickness) in pregnancy
stick to essential micronutrients: folic acid >400mcg/day & iodine 150mcg/day
stop any iron supplementation which can worsen morning sickness, nausea and vomiting
Non-pharmacological management of morning sickness
streamline vitamin and mineral supplements to just iodine and folate; stop taking iron supplements
optimise activities to minimise fatigue and increase rest
small, regularly meals as tolerated
stay hydrated
acupressure bands for nausea
ginger supplements
pyridoxine (Vitamin B6) - often in combination with doxylamine
How much ginger to take for morning sickness (nausea and vomiting in pregnancy)
200 mg to 600 mg every 8 hours
How much pyridoxine (Vitamin B6) to take for morning sickness (nausea and vomiting in pregnancy)
10 mg to 50 mg every 6 hours (short term, as long-term use increases neuropathy risk).
How much doxylamine to take for morning sickness (nausea and vomiting in pregnancy) and example dose regimens
Start with a low dose and titrate up if required. Most effective combined with Vitamin B6.
6.25 mg (one-quarter tablet) to 25 mg (1 tablet) at night, increase to every 8 hours if required. Maximum dose 50 mg (2 tablets) in 24 hours.
Examples:
1 tablet at night
Quarter tablet in the morning, quarter tablet at lunch, 1 tablet at night (avoiding daytime drowsiness)
Half a tablet in the morning, half a tablet at lunch, 1 tablet at night.
How much metoclopramide to take for pregnancy nausea and vomiting?
10 mg every 8 hours for up to 5 days (risks of extrapyramidal side effects to mother)
Pharmacological treatments for morning sickness (nausea and vomiting in pregnancy)
doxylamine first line (ideally in combination with Vitamin B6) or other sedating antihistamines (diphenhydramine, cyclizine)
metoclopramide (max 5 days)
odansentron (with concurrent laxatives to manage constipation)
Prevalence of heart burn (reflux) in pregnancy
30-50% of pregnancies
Why does heart burn / GI reflux occur in pregnancy
hormones lower oesophageal sphincter pressure
increased intrabdominal pressure against the stomach
Non-pharmacological treatments for heartburn/reflux in pregnancy
Raising head of bed
Avoid food 2-3 hours prior to bed or exercise
Small, more frequent meals
Drinking fluids between, not with meals
Sit up straight when eating
Avoid spicy & fatty foods, chocolate, caffeine, citrus, alcohol, tobacco
Pharmacological treatments for heartburn/reflux in pregnancy in order, from first line to last
Antacids
H2 antagonists
PPIs
Approach to treating reflux in pregnancy: steps from first line to last
Non-pharmacological (diet and lifestyle modifications) - usually all that is required.
Antacids
H2 antagonists
PPIs
After antacids, which drugs are preferred in pregnancy
H2 antagonists:
ranitidine
famotidine
If a PPI is required during pregnancy, which PPI is preferred?
Omeprazole (most data available in pregnancy)
Prevalence of constipation in pregnancy
Common, up to 40% of women in the first trimester. This figure halves by the third trimester as it improves.
What causes constipation in pregnancy?
Progestogen rises during pregnancy, causing reduced GI motility
Low fibre intake
Iron supplements
Approach to treating constipation in pregnancy: steps from first line to last
Increase water, fibre and exercise; reduce caffeine
Bulk forming (fibre) laxatives
Osmotic laxatives
Stimulant laxatives (avoid where possible; one-off exposure is acceptable)
When to start routine UTI testing in pregnancy?
From 12-16 weeks
What complication risks do UTIs present during pregnancy?
Risk of pyelonephritis, associated with low birth weight & pre-term birth
What three micronutrient deficiencies can cause anemia in pregnancy?
Iron, folate, and vitamin B12
Australian iron intake recommendations in pregnancy
27 mg a day
What measures can be taken to manage/prevent varicose veins in pregnancy?
Compression stockings
Most resolve after pregnancy, but if not, can consider surgery after
What agents can be used to prevent venous thromboembolism in high risk pregnancies and during what points of the perinatal period should they be used?
Low molecular weight heparin (LMWH) or subcutaneous heparin during the pregnancy, stopped at onset of labour
Low molecular weight heparin (LMWH) or warfarin prophylaxis after delivery for 6 weeks
Treatment options to manage pelvic girdle pain in pregnancy
Physiotherapy
Exercise
Acupuncture
Prevalence of hypertensive disorders of pregnancy amongst pregnant women?
9-10% of pregnant women
How does blood pressure usually change throughout pregnancy?
It falls in the first trimester, then increases towards non-pregnant levels by delivery
Hypertension in pregnancy is defined as…
> 140 / > 90 mmHg