1 - intro to glaucoma anatomy and physiology
1/85
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
86 Terms
What is the AOA's definition of glaucoma?
group of ocular disease with various causes that are associated with progressive optic neuropathy leading to loss of visual function
What is important to note about the definition of glaucoma?
it does NOT INCLUDE IOP
What are the 3 main important components of the definition of glaucoma?
1. it gets worse with time (progressive)
2. causes loss of structure (optic neuropathy)
3. causes loss of visual function (visual field loss)
What eye structures are important to glaucoma?
1. aqueous humor
2. ciliary body
3. iris
4. trabecular meshwork
5. optic nerve
What are the anatomical sites of treatment for glaucoma?
1. ciliary body
2. iris
3. trabecular meshwork
What are the functions of the aqueous humor?
1. provides nutrients to avascular tissues of the eye + washes away their metabolic waste
2. maintains the shape of the globe
What is the flow of AH?
1. non-pigmented ciliary body epithelium produces AH
2. some AH flows into the vitreous cavity
3. majority of AH flows through pupil and into anterior chamber
4. AH drains from ant chamber via TM + uveoscleral outflow
How is AH produced at the ciliary body? (steps)
1. plasma moves from blood to stroma of ciliary processes via passive process called ultrafiltration
2. ions and proteins are actively transported from ciliary process core to posterior chamber across the non-pigmented epithelium to create osmotic gradient
3. water follows gradient into the posterior chamber
How can we modulate AH production at the ciliary body?
aqueous suppressors:
1. CAI: stops CA from moving bicarbonate across the CB → ↓ the osmotic gradient
2. β-blocker: ↓ the production of AH
what is dorzolamide?
topical CAI
what is brinzolamide?
topical CAI
what is acetazolamide?
oral CAI
what is timolol?
topical β-blocker
what is propanolol?
oral β-blocker
what beta-adrenergic agonists increase production of AH?
1. epinephrine
2. norepinephrine
3. terbutaline
4. isoproterenol
Where does the iris root insert?
into anterior aspect of CB
Where is the thinnest part of the iris?
iris root
What is the thickest part of the iris?
collarette
What divides the iris into the pupillary and ciliary zones?
collarette
Why can AH not flow through the iris?
both the anterior and posterior epithelium of the iris has tight junctions and desmosomes
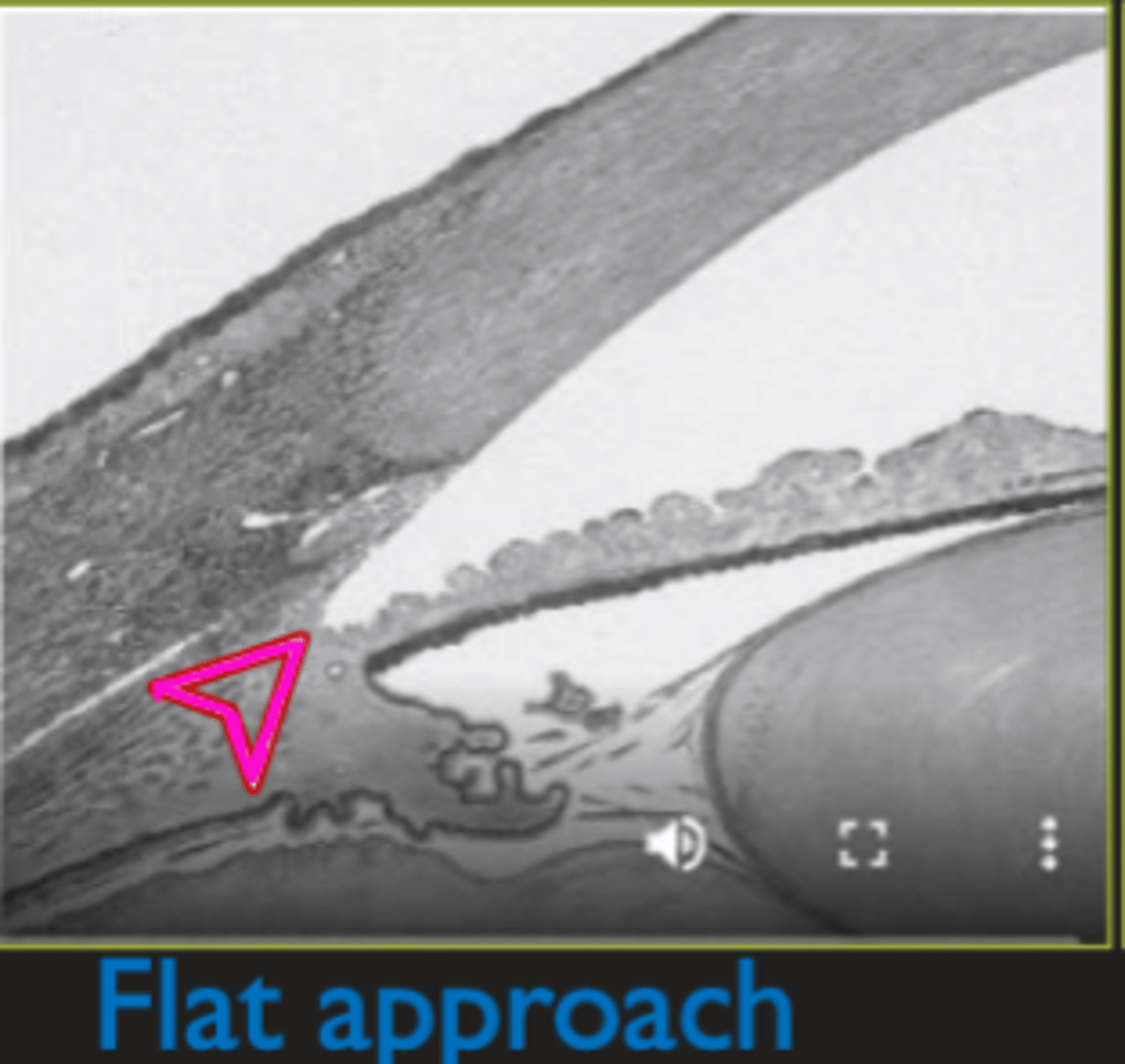
What is a flat approach?
flat iris
What does it mean if the iris has posterior concavity?
iris bends/concaves backward → can scrape across zones releasing pigment
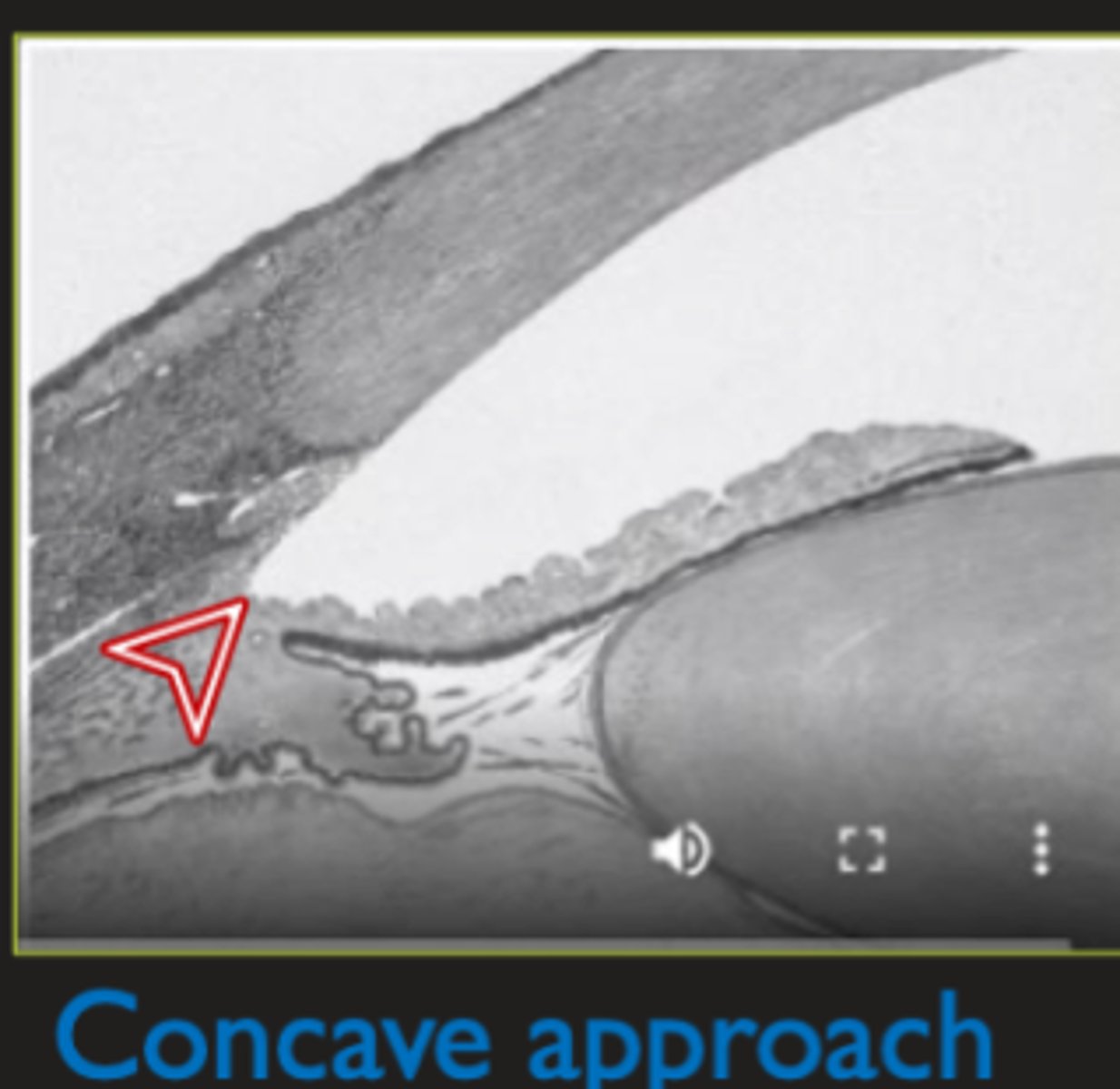
What does a posterior concavity iris look like?
1. pigment accumulation angle on gonio
2. area of iris concave back
3. area where iris is not concave appears elevated
What is an anteriorly bowed iris?
iris is pushed forward → pupil margin may have too much contact with lens
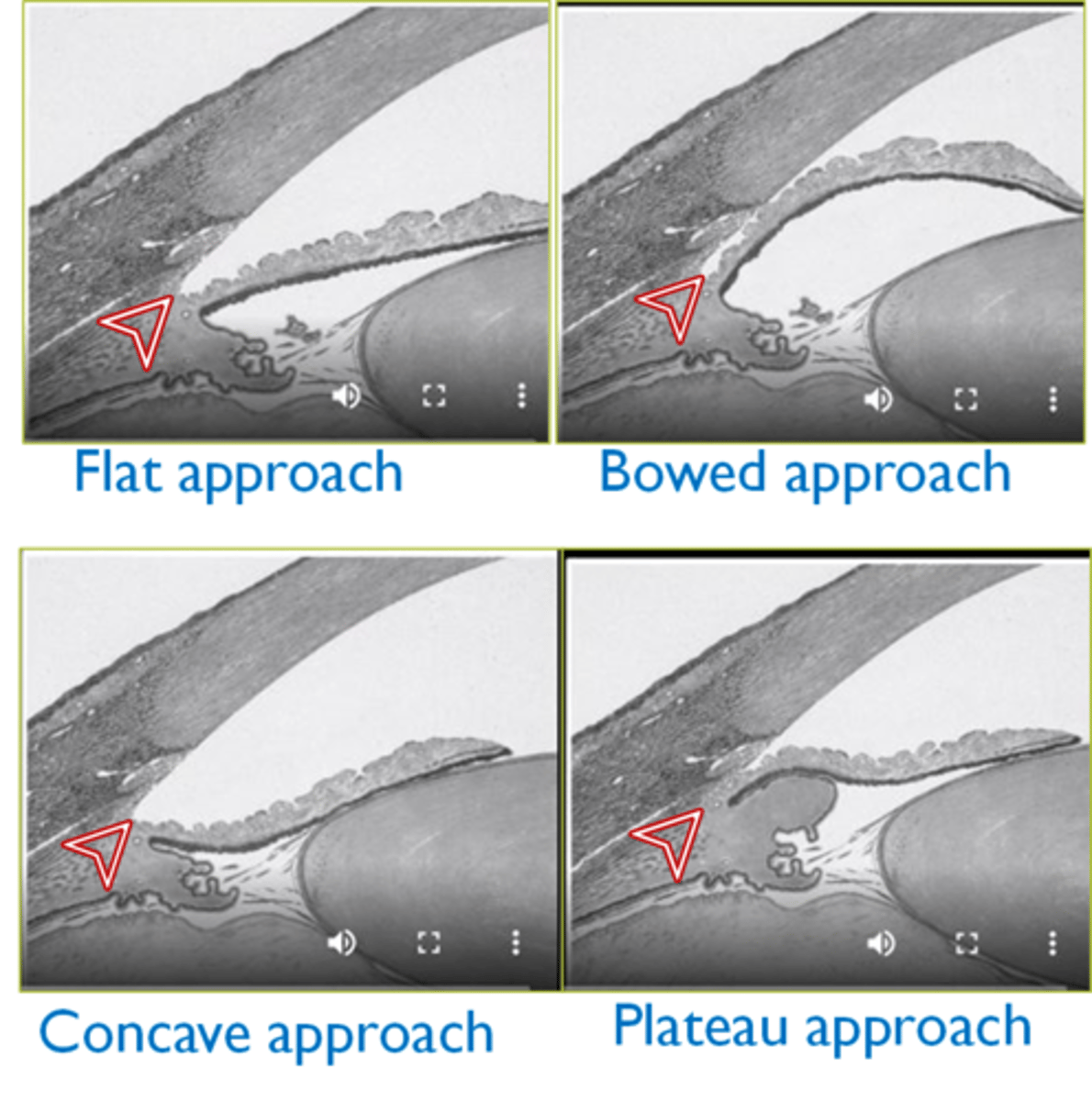
what is a plateau iris configuration?
a flat iris plane but shallow angle recess (seen with deep anterior chamber)
anterior positioned CB that mechanically supports the peripheral iris → angulated, sharp drop-off of the peripheral portion of the iris next to the angle wall
what does a plateau iris configuration look like?
1. deep anterior chamber
2. anteriorly positioned CB that mechanically supports the peripheral iris
3. angulated, sharp drop-off of the peripheral portion of the iris next to the angle wall
What does the TM encircle?
circumference of the anterior chamber
Where is the apex of the TM?
Schwalbe's line
Where is the base of the TM?
scleral spur
Where does the outer face of the TM lay?
against the scleral spur, Schlemm's canal, and corneal stroma
Where does the inner face of the TM border?
anterior chamber
What is the TM made up of?
1. spongy connective tissue beams/lamellae with core of collagen and elastic fibers
2. flat TM cells that lay on/cover beams
How are the connective tissue beams arranged in the TM?
attached to one another in several layers forming a porous filter-like structure
What are the 3 layers of the TM from inner to outer?
1. uveal meshwork
2. corneoscleral meshwork
3. juxtacanalicular tissue (JCT)
Which part of the TM is cord-like?
uveal meshwork
Which part of the TM is sheet like?
corneoscleral meshwork
Which part of the TM is a thinly distributed matrix?
JCT
Where is the JCT anchored to?
anchored to the basement epithelium of Schlemm's canal
What is the #1 source of resistance to AH outflow?
JCT
How can we modulate the TM?
1. rhokinase inhibitor
2. prostaglandin
what is rhopressa (netarsudil)?
inhibits rhokinase which relaxes the TM
what is vyzulta (latanoprostene bunod)?
prostaglandin prodrug that releases NO when activated → NO relaxes the TM → ↑ AH outflow
works on both uveoscleral (prostaglandin) outflow and TM (NO) outflow pathways
What is Schlemm's Canal?
venous channel beyond TM
Where is Schlemm's canal located?
directly outer to TM
What increases the surface area of Schlemm's canal?
internal collector channels of Sondermann
What is the process of drainage from the TM to SC?
1. endothelial cells are connected with tight junction and line the walls of SC
2. endothelial cells create vacuoles and AH from TM enters SC thru them
3. vacuoles open and close intermittently allowing transient, transcellular unidirectional flow
What type of process is AH drainage from TM to SC?
passive process but pressure dependent
efficient → not a source of outflow resistance
what has the highest oncotic conductivities of the body?
endothelial cells in TM
What are the two ways AH can drain from SC?
1. SC → external collector channels → deep scleral plexus or intrascleral plexus → episcleral + conjunctival veins
2. SC → aqueous veins of Ascher → episcleral veins
What is normal episcleral venous pressure (EVP)?
8-10 mmHg
How does EVP change in different positions?
going from sitting to laying (supine) increases EVP by 1-9 mmHg
How does EVP affect the IOP increase at night?
EVP increases when laying down → causing IOP to increase at night (EVP is the floor of IOP)
What is the relationship between EVP and IOP?
direct relationship between EVP and IOP
0.8mmHg change in EVP = 1.0mmHg change in IOP
How does AH flow through the uveoscleral pathway?
1. no recognizable channels/vessels → instead AH seeps through the anterior face off ciliary muscles and uveal tissues
2. exits the eye through sclera or is absorbed into suprachorodial space and choroidal vessels
Which outflow system is IOP independent?
uveoscleral outflow
What % of all outflow is done by the uveoscleral pathway in young pts?
25-57%
How do prostaglandins affect uveoscleral outflow?
PG binds FP receptors in CB + sclera → ↑ MMP activity → expanding the ECM + decreasing collagen
what is latanoprost?
prostaglandin
What is IOP equal to?
IOP = AHP - TM(Out) - UvSc(Out) + EVP
AHP: aqueous humor production
TM(Out): trabecular meshwork outflow
UvSc(Out): uveoscleral outflow
EVP: episcleral venous pressure
what is the optic nerve?
collection of RGC axons (~1.2 mil axons in young pts)
What is the ganglion cell layer made up of?
RGC cell bodies
What is the NFL made up of?
RGC axons
What is the optic nerve head?
opening in sclera where a collection of RGC axons exit the globe
What is the average H + V diameter of an optic nerve?
1.9 mm V
1.7 mm H
What retinal layers are in the ONH?
RNFL and ILM
Why is the ONH a physiological blind spot?
no photoreceptors
Why is the ONH paler than the rest of the retina?
lack of RPE and capillary network
Why is the cup of the ONH lighter than the disc?
less axons at the cup, more axons at the rim (darker than cup)
Where do axons far from the ONH enter the nerve?
go to posterior portion of RNFL → rim (outer portion of nerve)
Where do axons close to the ONH enter the nerve?
go to anterior portion of RNFL → into the cup (inner portion of nerve)
What is the lamina cribrosa?
10 layers of collagenous plates that lie at the level of the scleral opening with 100 micron wide perforations (room for axons to pass)
What is the function of the lamina cribrosa?
provides structural protection to the RGC axons
How do the RGC gets support before reaching the lamina cribrosa?
glial cell processes
How do the pores change in lamina cribrosa based on location?
S+I have larger pores → less support
central, N, and T have smaller pores → more support
what is the mechanical stress in normal/healthy eyes?
shearing stress imposed on RGC axons as they bend 90° at the ONH
What is the mechanical theory of glaucoma?
increased IOP increases the physical stress (shearing and pinching) of RGC axons at the ONH → decreases axoplasmic flow → leading to deprivation of neurotrophic factors that keep RGCs healthy → death of RGC
How does the mechanical theory of glaucoma correlate to increased loss of superior and inferior RGC axons?
S+I axons are affected the most because they have less support from the lamina cribrosa → larger pores
What supplies blood to the ONH?
major blood supply: circle of Zinn-Haller
partial profusion to superficial ONH + RFL: arterioles from CRA (central retinal artery)
What is the circle of Zinn-Haller?
anastomoses of medial + temporal short posterior ciliary arteries
Is the circle of Zinn Haller fenestrated or non-fenestrated?
non-fenestrated → creates blood-nerve barrier
What is the ocular perfusion pressure equal to?
OPP = diastolic BP - IOP
What is the vascular theory of glaucoma damage?
increased IOP compresses capillaries → impairing perfusion of ONH → causing interference with axoplasmic flow → death of RGC
Why does the OPP decrease at night?
BP decreases
IOP increases
What factors influences the ocular perfusion pressure?
1. treatment of hypertension (CCB and β-blockers) → worsen nocturnal hypotension
2. sleep apnea → repetitive closure of the upper airway during sleep
3. migraines → vasospasm
what is the biochemical theory of glaucomatous damage?
ganglion cell death in glaucoma takes place via apoptosis → release glutamate → excitotoxic injury to RGCs → cont progression of damage to neighboring cells
What is the hallmark of glaucoma?
progressive optic neuropathy that leads to the death of RGC axons