CM3 M3L2: Upper GI and Biliary Surgery
1/96
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
97 Terms
EGD reveals patient's PUD is due to the most common etiology. Tx?
Clarithromycin (Macrolide), amoxicillin & PPI x14 days (Tx for H. Pylori)
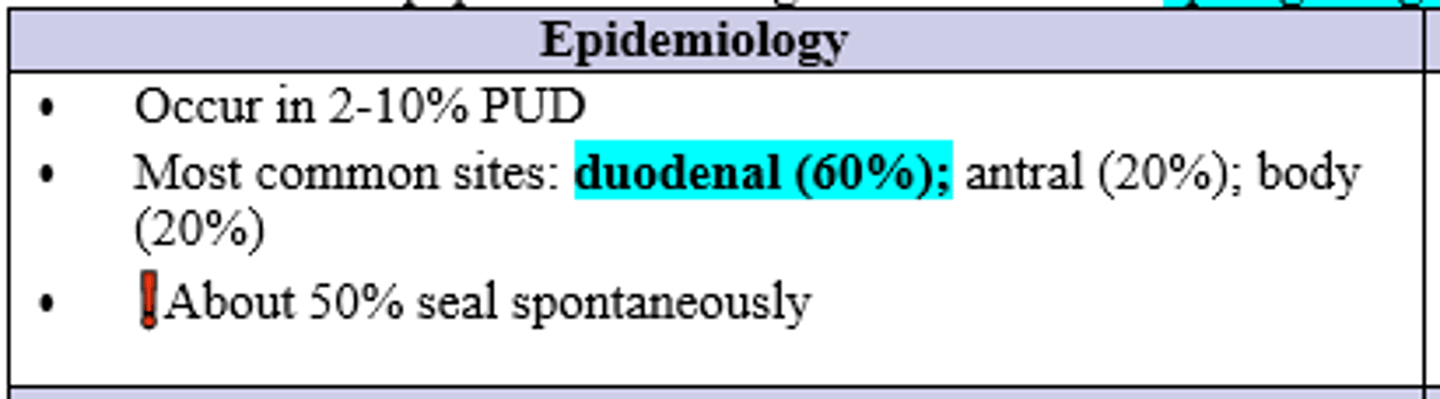
Where is the MC site for a peptic ulcer to erode through the serosa and perforate causing spillage of gastric contents into the peritoneum?
Duodenal (60%)
20% antrum of gastric/stomach
20% body of gastric/stomach
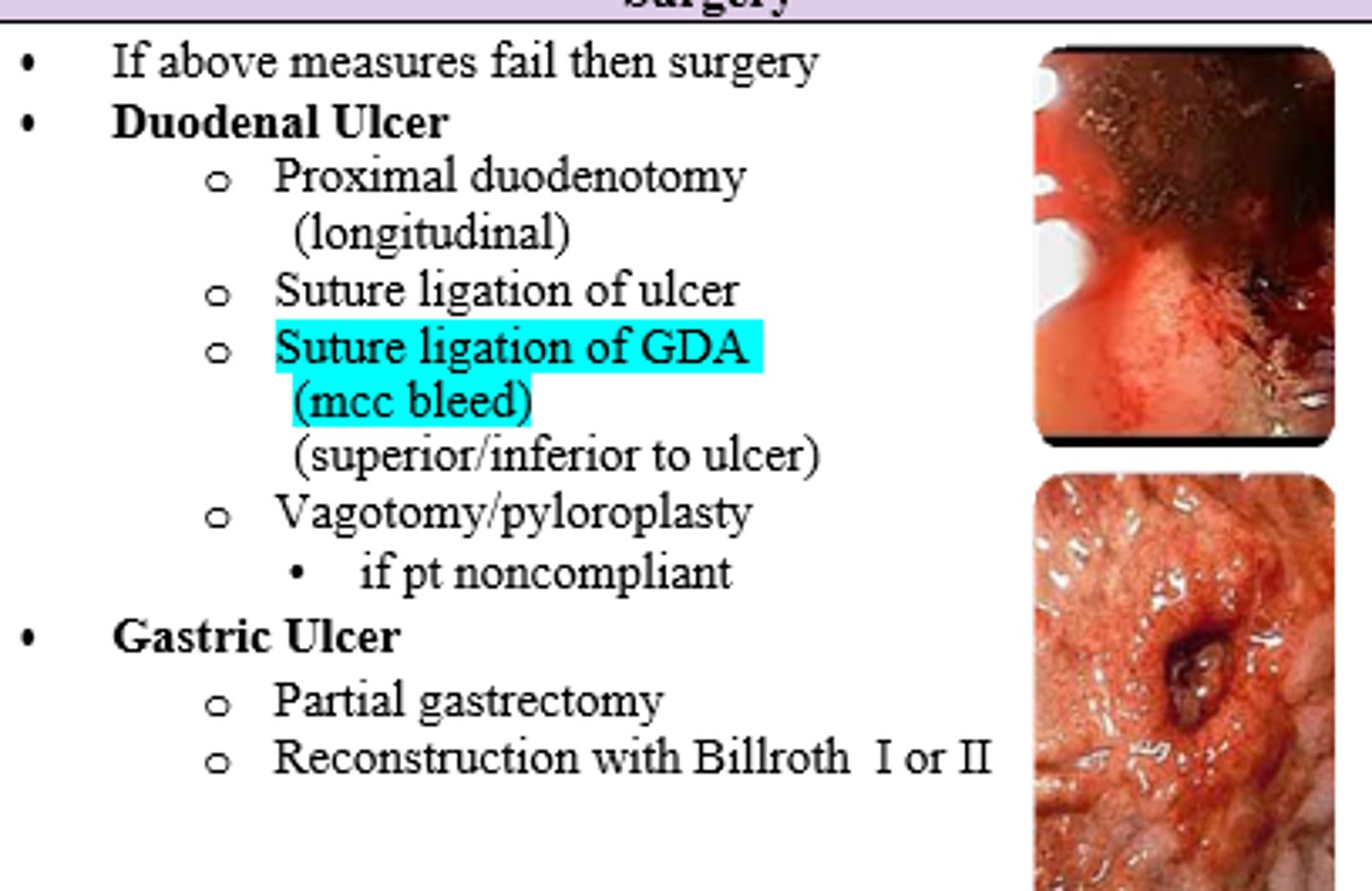
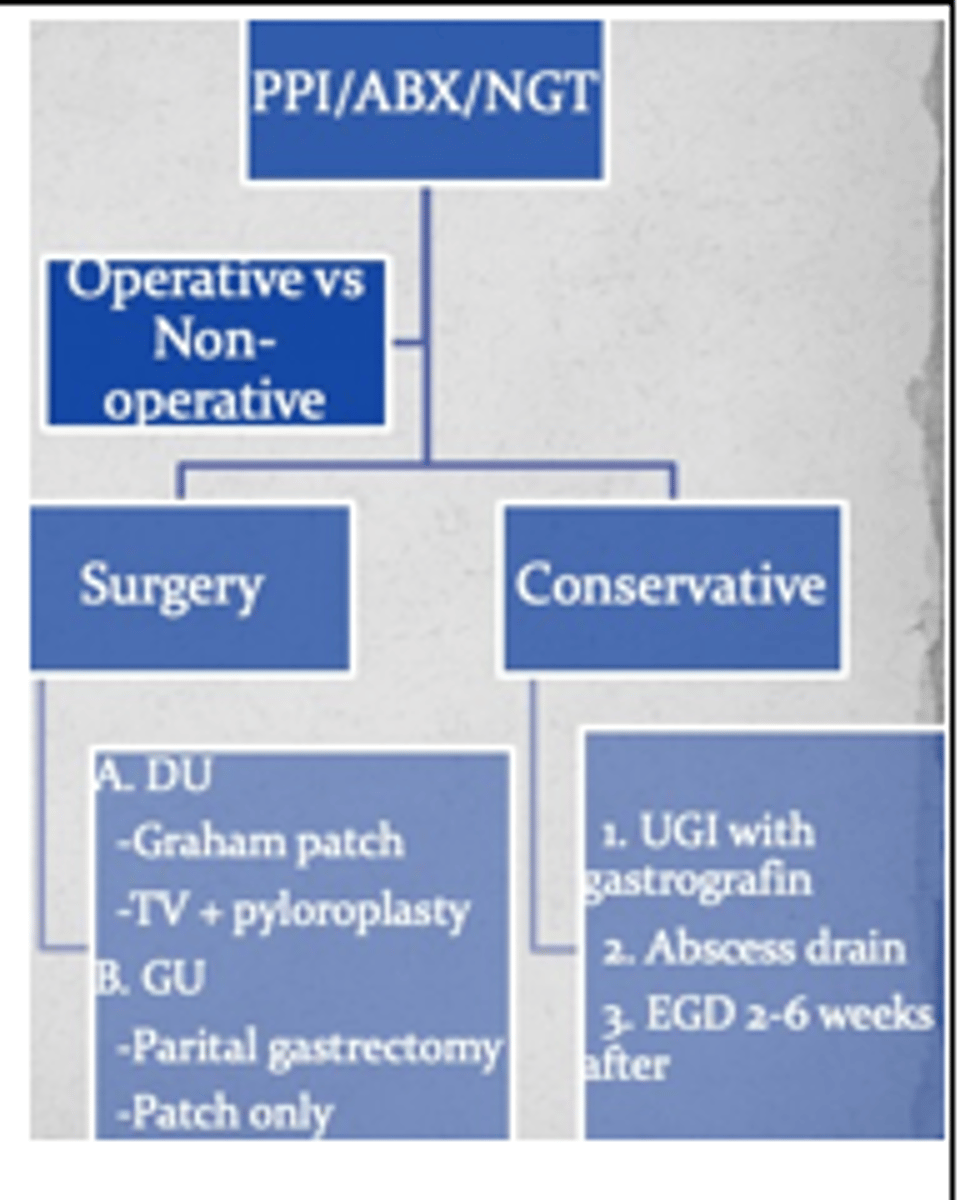
After free air above diaphragm (= perforation) is confirmed on ABD xrays, CT, or Upper GI series, of a nonstable pt with worsening symptoms what are your treatment options?
- Surgical intervention:
1. if Duodenal ulcer-->
Graham patch
+/- Pyloric Exclusion and Gastrojujunostomy or TV/pylorplasty
2. if Gastric ulcer -->
Graham patch
+/- Partial Gastrectomy/Antrectomy w/ Billroth reconstruction (I or II)
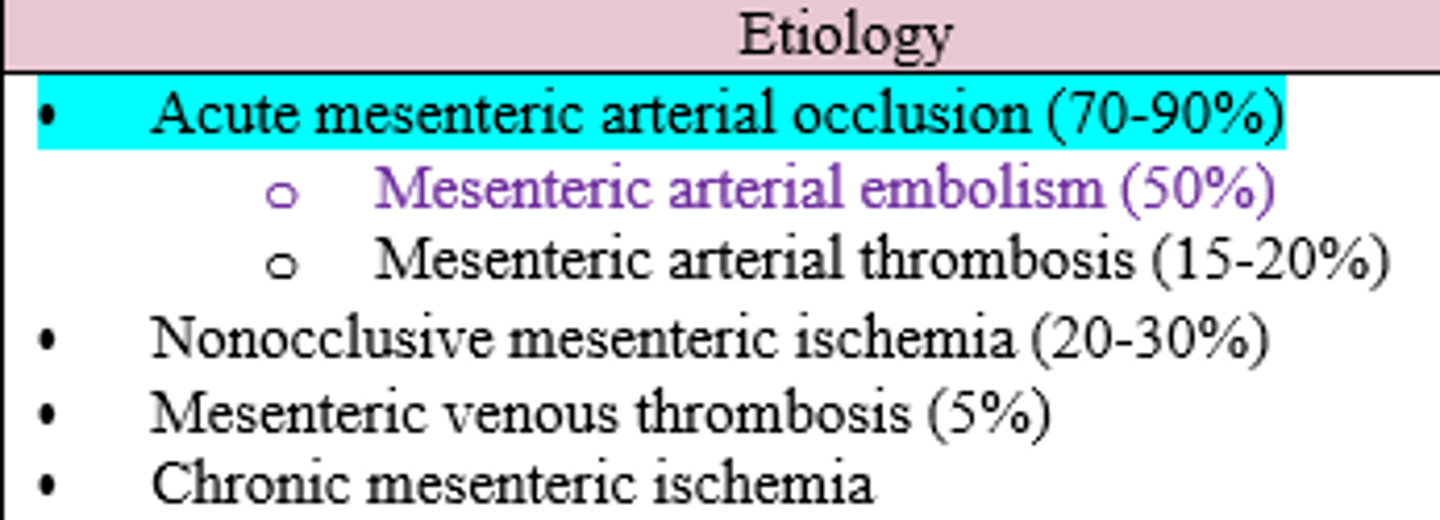
What is the MCC of reduced blood flow to the intestines (Mesenteric Ischemia) ?
Acute Mesenteric Arterial Occlusion (70-90%)
- embolism (50%) vs. thrombosis (15-20%)
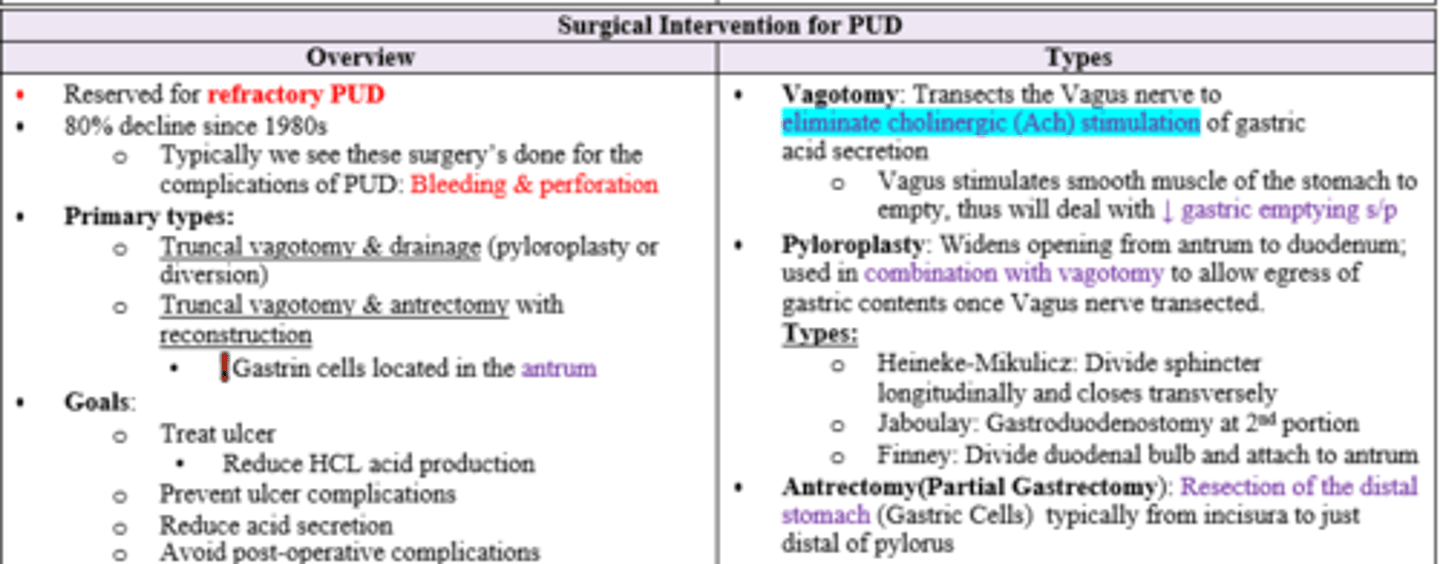
Which portion of the stomach contains gastrin cells which secrete HCl?
Antrum
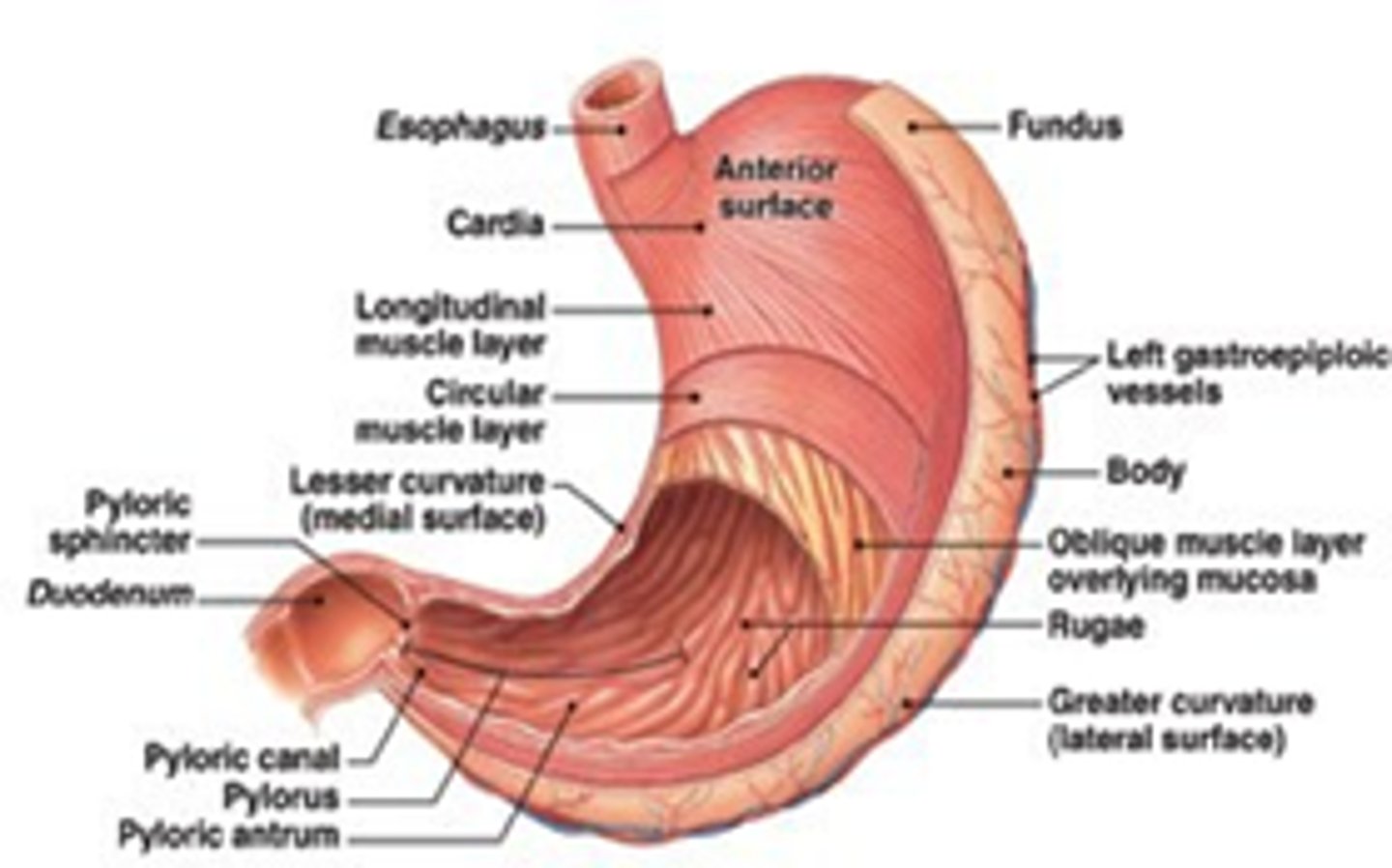
Which cells produce gastric acid (HCl)?
Parietal cells (basement membrane)
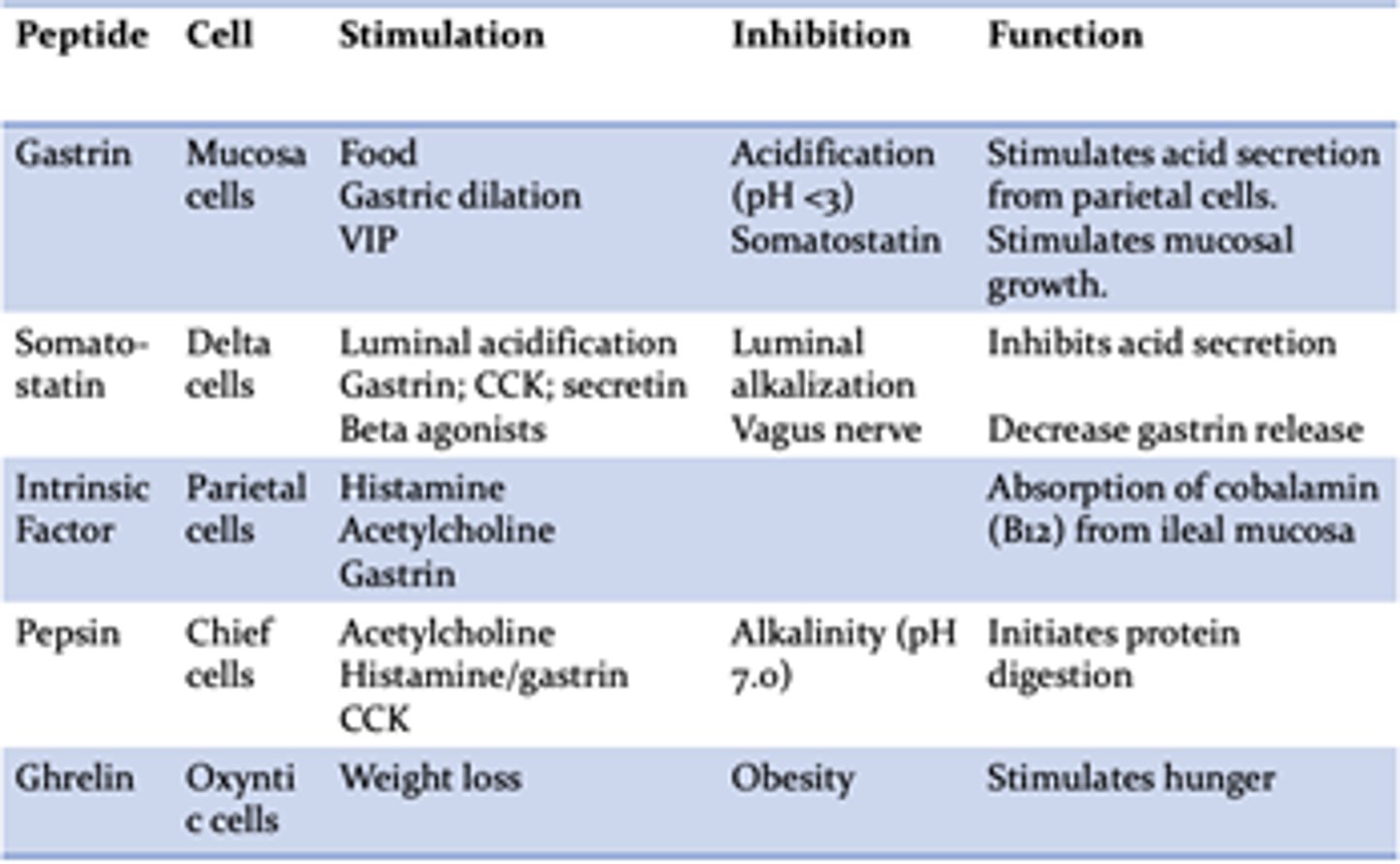
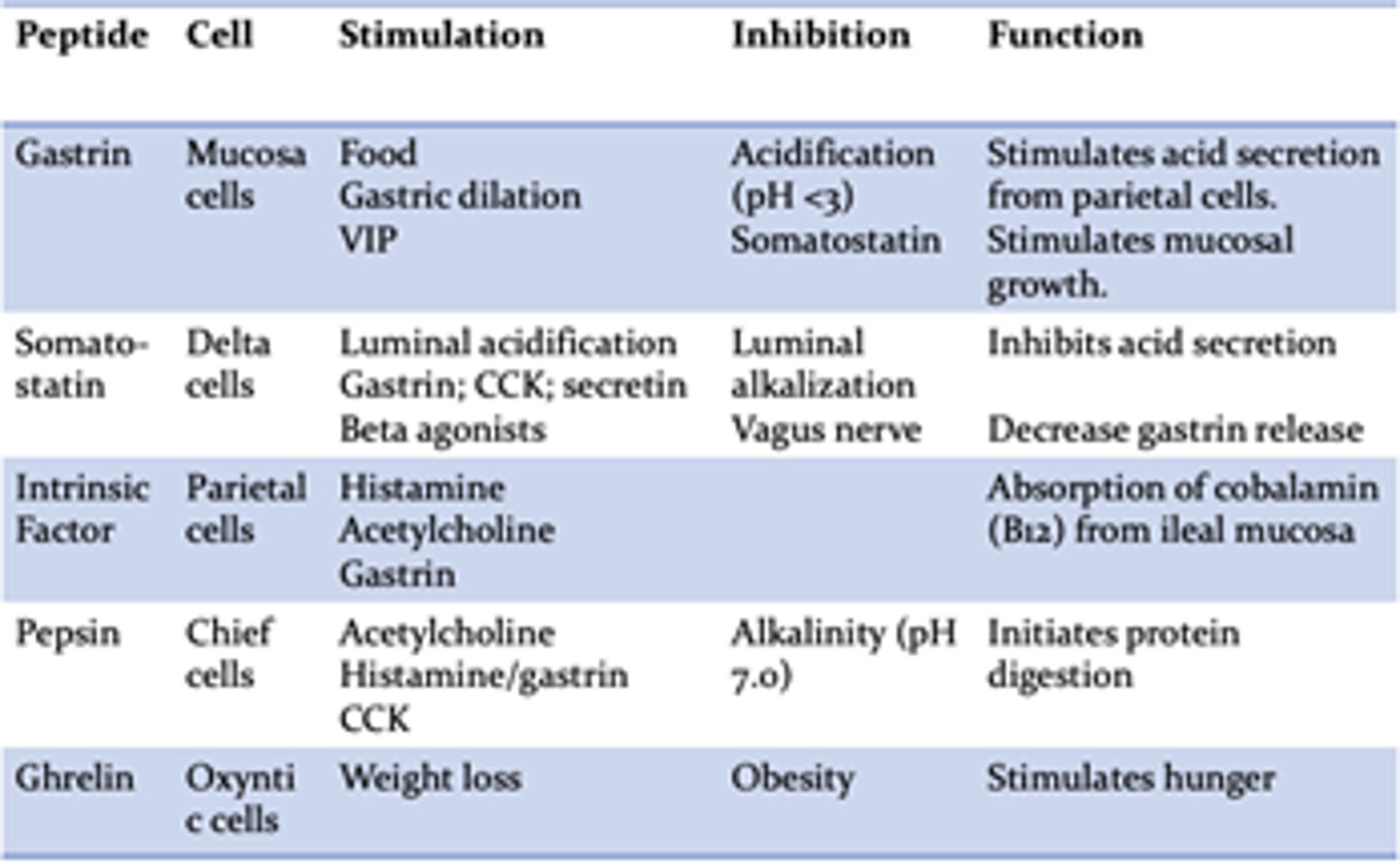
Which of the following are gastric acid (HCl) stimulants and which are inhibitors?
Histamine
Gastrin
Acetylcholine
Somatostatin
PGE-2
Stimulants: Histamine, Gastrin, Acetylcholine
Inhibitors: Somatostatin, PGE-2
Which nerve is responsible for afferent and efferent signals to the stomach?
What about sympathetic/pain stimulation?
Vagus nerve (afferent > efferent); T5-T10 (pain)
Which portion of the duodenum does 90% of ulcerations occur at and which artery is nearby?
1st portion; Gastroduodenal artery

Which portion of the duodenum houses the ampulla of vater and is retroperitoneal?
2nd portion

What condition results from a defect in gastric/duodenal mucosa, extending from mucosa through the muscularis?
Peptic Ulcer Disease
Patient has an imbalance of acid secretion and mucosal defense resulting in defect in duodenum extending from mucosa through the muscularis. What is the biggest risk factor for suspected diagnosis?
H. Pylori (85% , gram negative bacteria causing chronic gastritis; dx = PUD)
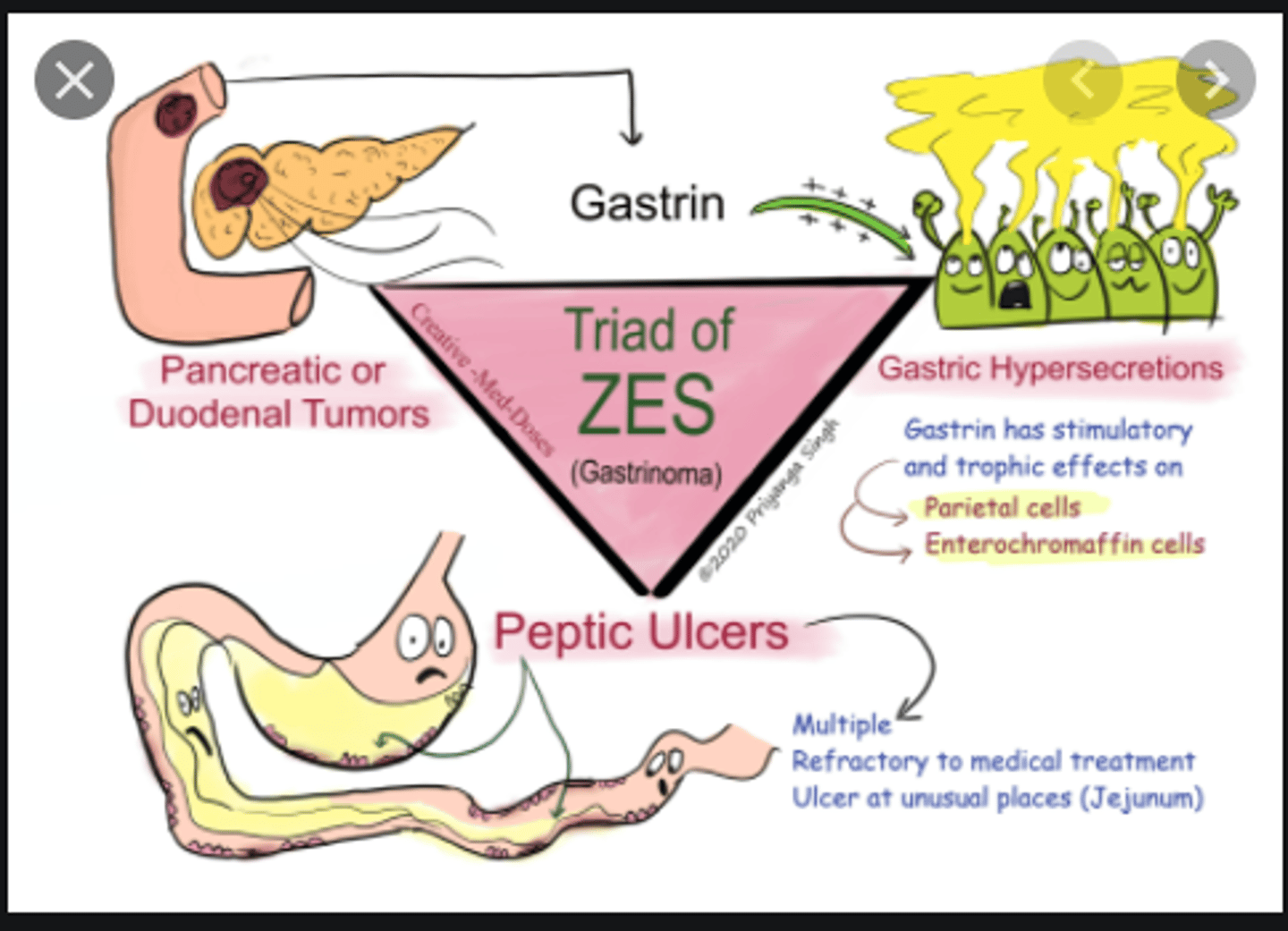
Patient has a rare gastrin secreting tumor with MEN 1 association. Dx?
Zollinger-Ellison Syndrome
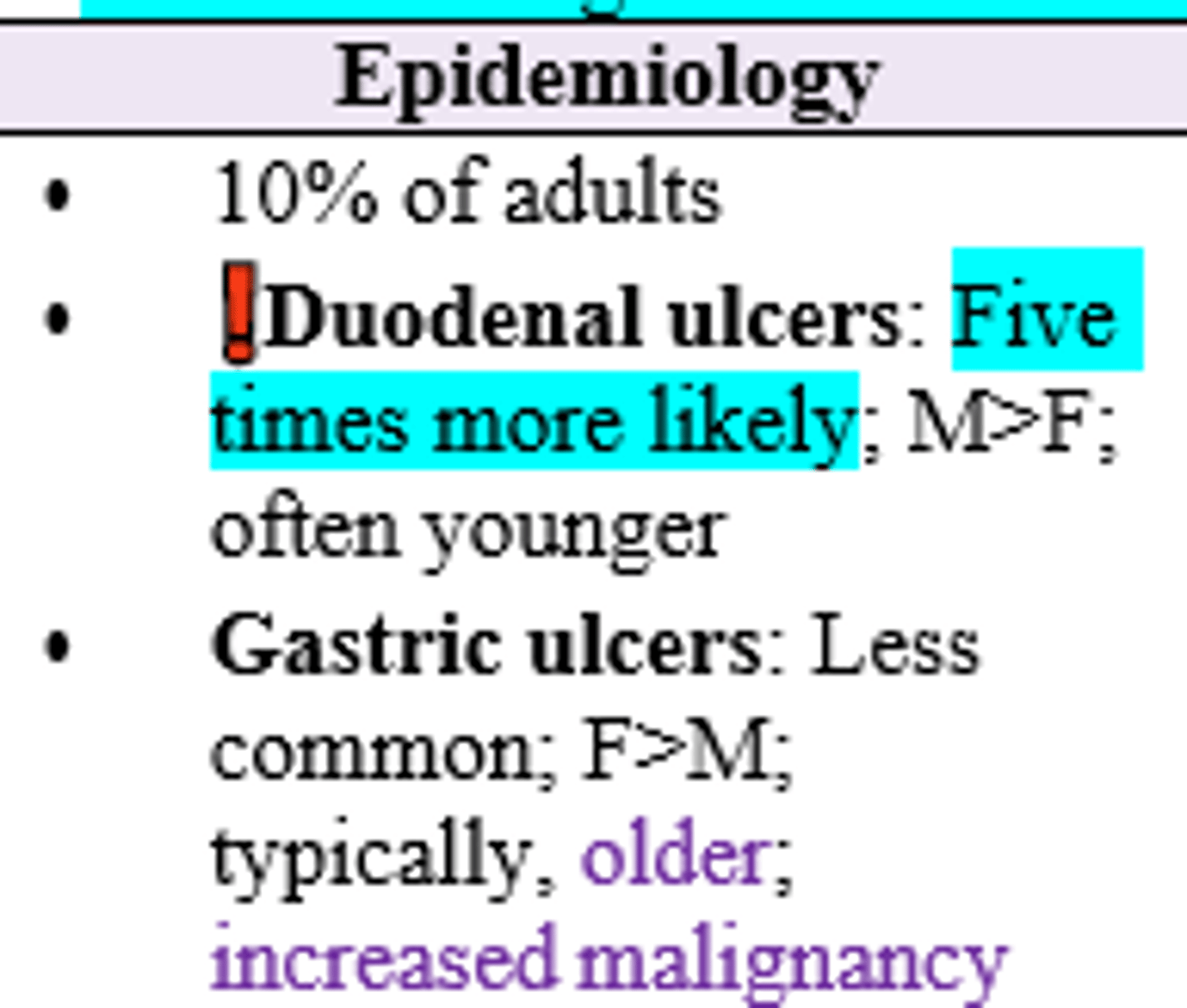
(Gastric/Duodenal) ulcers are more common and (Gastric/Duodenal) ulcers are more often associated with malignancy
Duodenal; Gastric
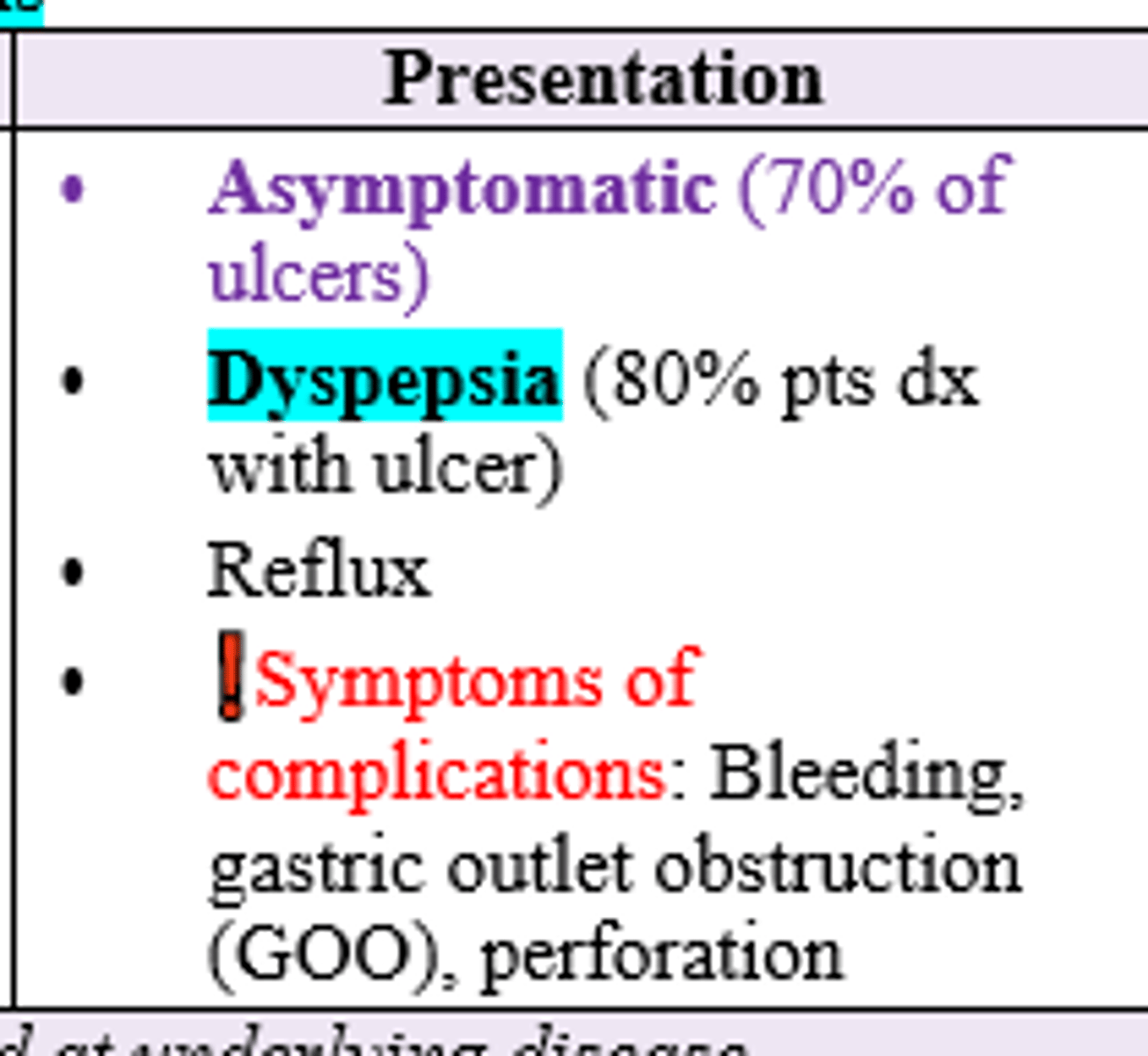
What is the most common presentation of patients without diagnosis of PUD?
What about with dx of PUD?
Asymptomatic; Dyspepsia
Older female patient with social hx + for smoking, ETOH, and NSAID use c/o dyspepsia and reflux. Diagnostics and Tx for suspected diagnosis?
H. Pylori Testing (+/- bx or stool antigen)
EGD (90% sensitive, allows for bx, diagnostic test of choice)
Treat underlying cause of PUD (H. Pylori = Clarithromycin, amoxicillin, and PPI x 14d)
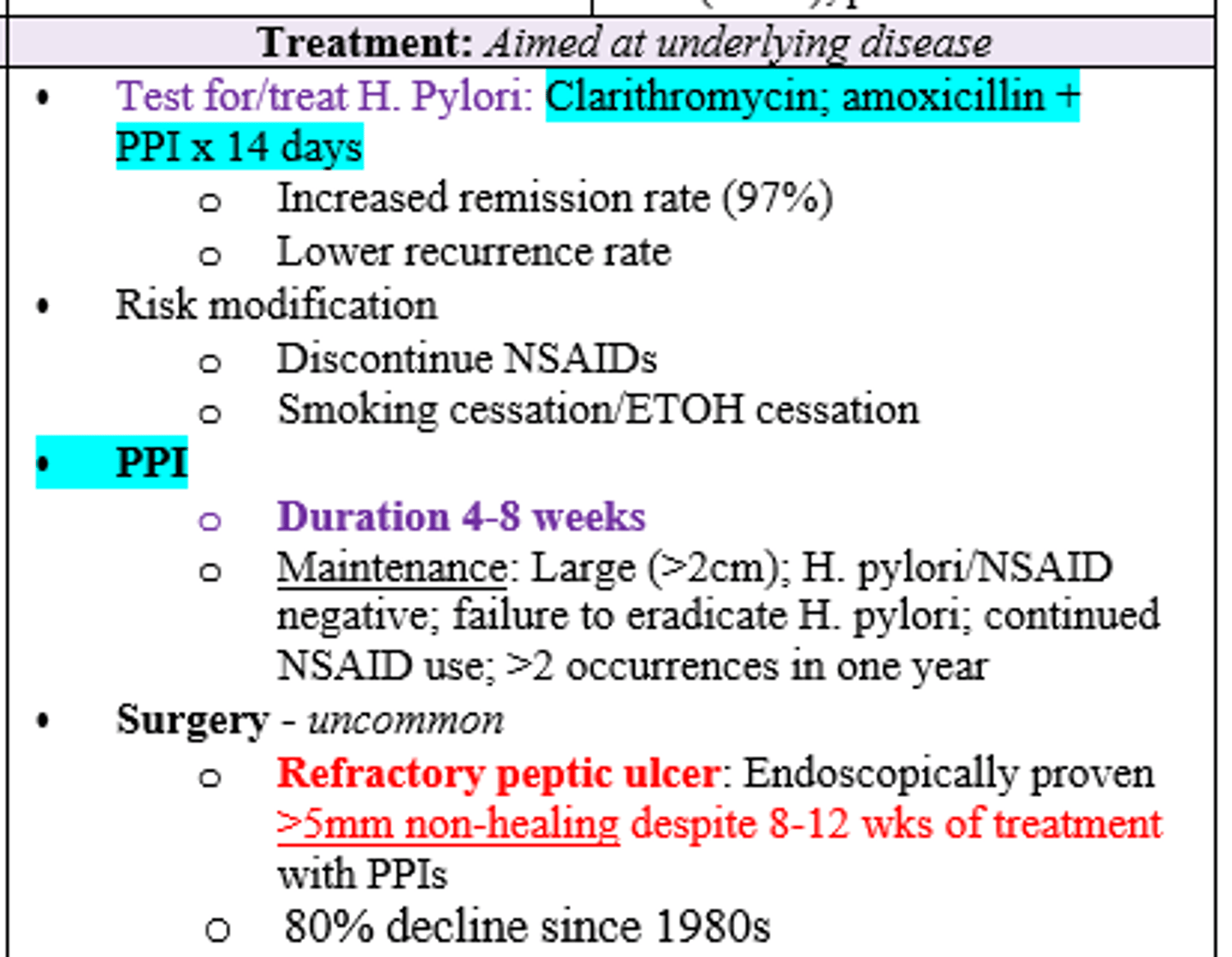
After 8-12 weeks of treatment with PPI, patient still has endoscopically proven >5mm non-healing peptic ulcer. Tx?
Surgery (Truncal Vagotomy & Drainage vs. Truncal Vagotomy & Antrectomy with Reconstruction)
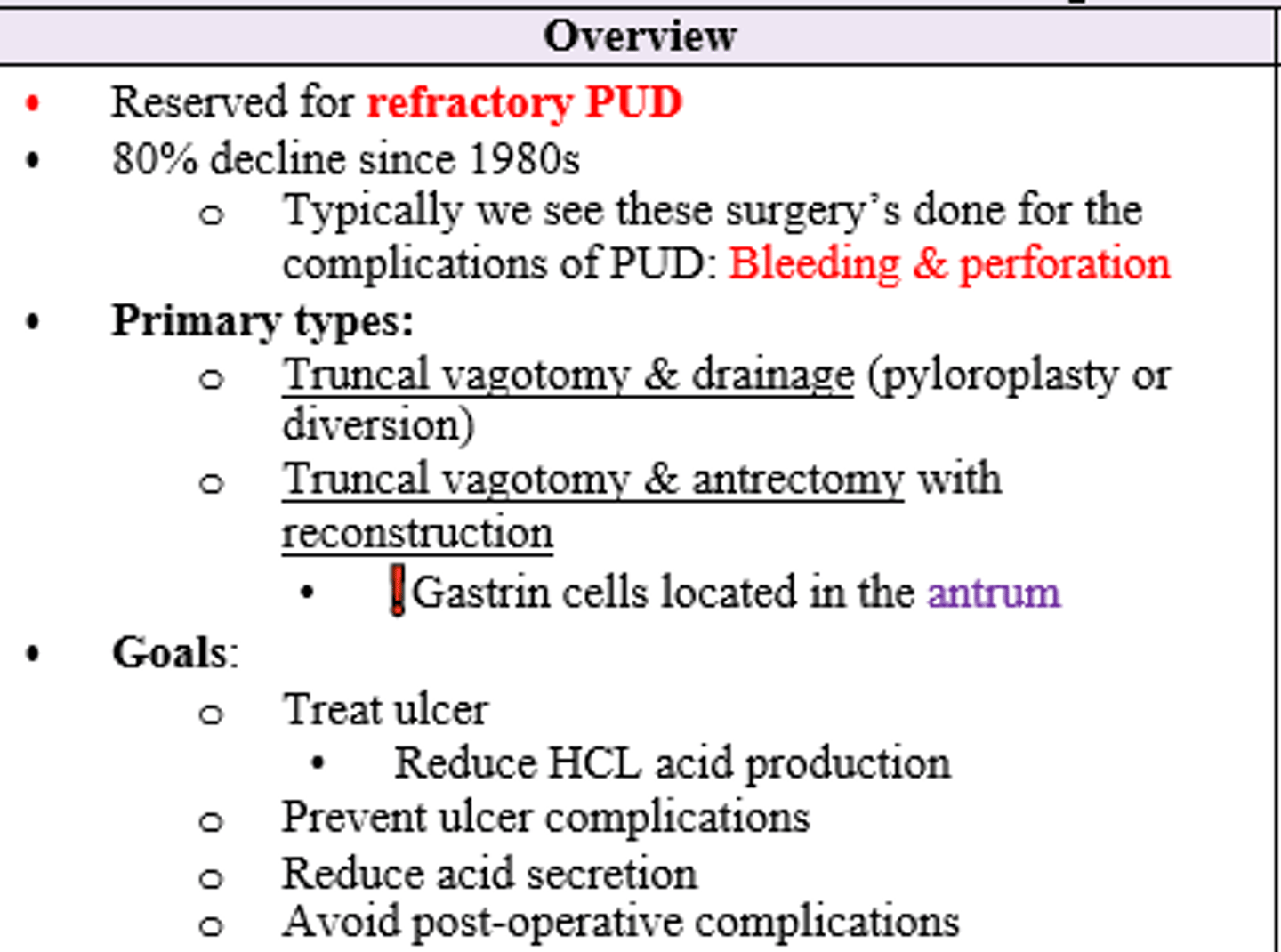
What is the mechanism by which performing a vagotomy leads to treatment of PUD?
Transecting vagus nerve eliminates gastric acid secretion by eliminating Ach stimulation.
Also will lead to decreased gastric emptying dt decreased stimulation of smooth muscle in stomach (why it is performed w drainage procedure like pyloroplasty)
Which gastric reconstructions correspond to the following:
1. End-to-End Anastomosis
2. End-to-Side Anastomosis
3. Side-to-Side from rement and end-to-side from other limb
1. Billroth I
2. Billroth II
3. Roux-en-Y Gastrojejunostomy
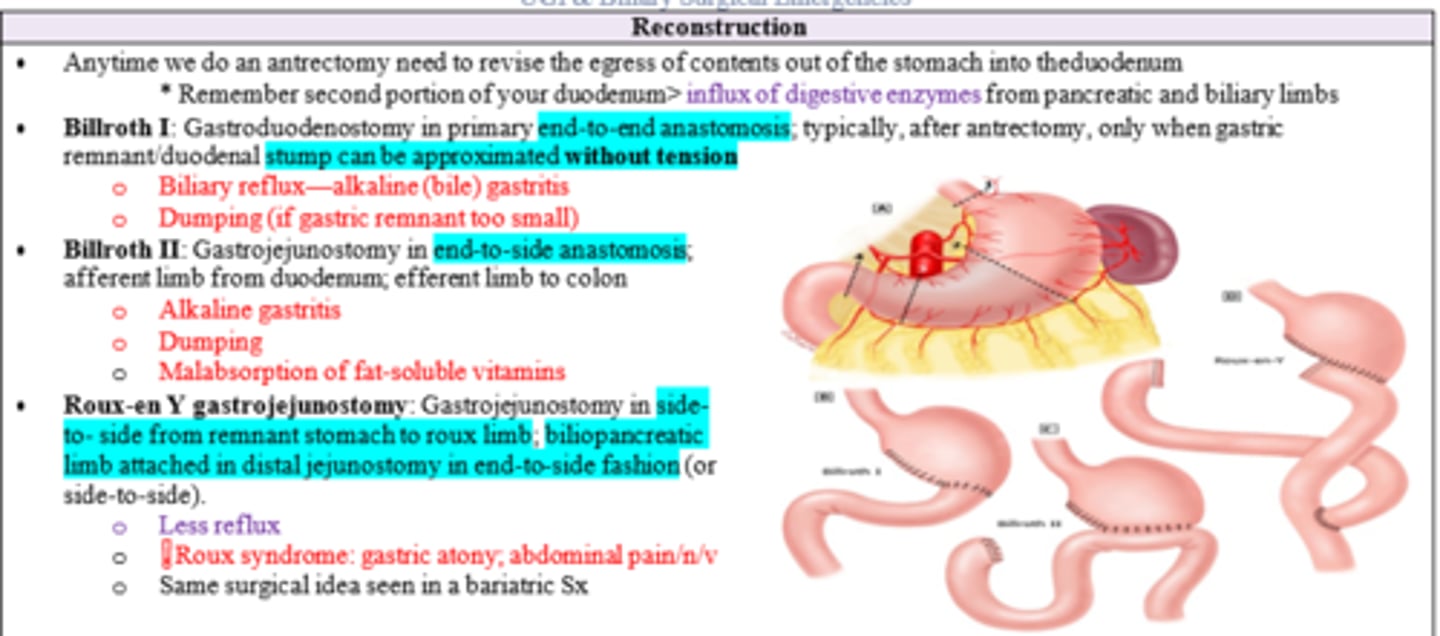
After gastric reconstruction, patient develops gastric atony (lost muscle strength), abdominal pain, nausea, and vomiting. Dx?
Roux Syndrome (complication of Roux-en-Y gastrojejunostomy)
What is the leading cause of death associated with PUD?
Upper GI Bleeding (bleeding from GIT proximal to ligament of Treitz)
What is the mcc of Upper GI Bleeding?
PUD (65%; others = esophagitis, varices, aorto-esophageal fistula, mallory-weiss tear, marginal ulcers, malignancy)
Patient presents w significant abdominal pain. Hx reveals hematemesis (BRB or coffee grounds in vomit) and melena (dark tarry stools). Top DDx?
Upper GI bleed 2/2 PUD
Patient has upper GI bleeding associated with odynophagia (painful swallowing) and dysphagia (trouble swallowing). Top DDx?
Esophageal ulcer
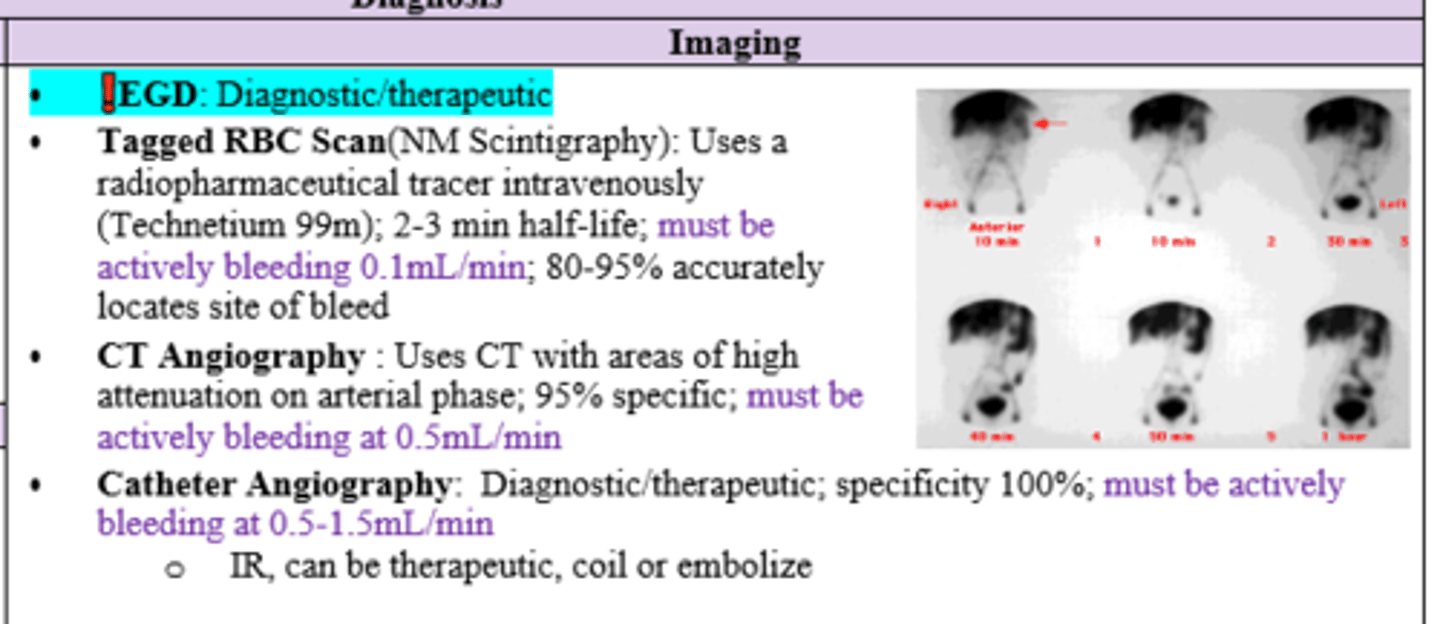
Which imaging technique for an upper GI bleed is both diagnostic AND therapeutic?
EGD
Which imaging technique for upper GI bleed requires the following:
1. Active bleeding 0.1mL/min
2. Active bleeding 0.5mL/min
3. Active bleeding 0.5-1.5mL/min
1. Tagged RBC Scan
2. CTA (CT angio)
3. Catheter Angiography
Which medications can cause upper GI bleeds?
NSAIDs, ASA, Anticoagulants
If a patient comes in with an upper GI bleed, what labs should be performed?
CBC/H&H, CMP
LFT (acute hepatitis)
BUN:Cr Ratio
Coagulation Studies
Type/Screen
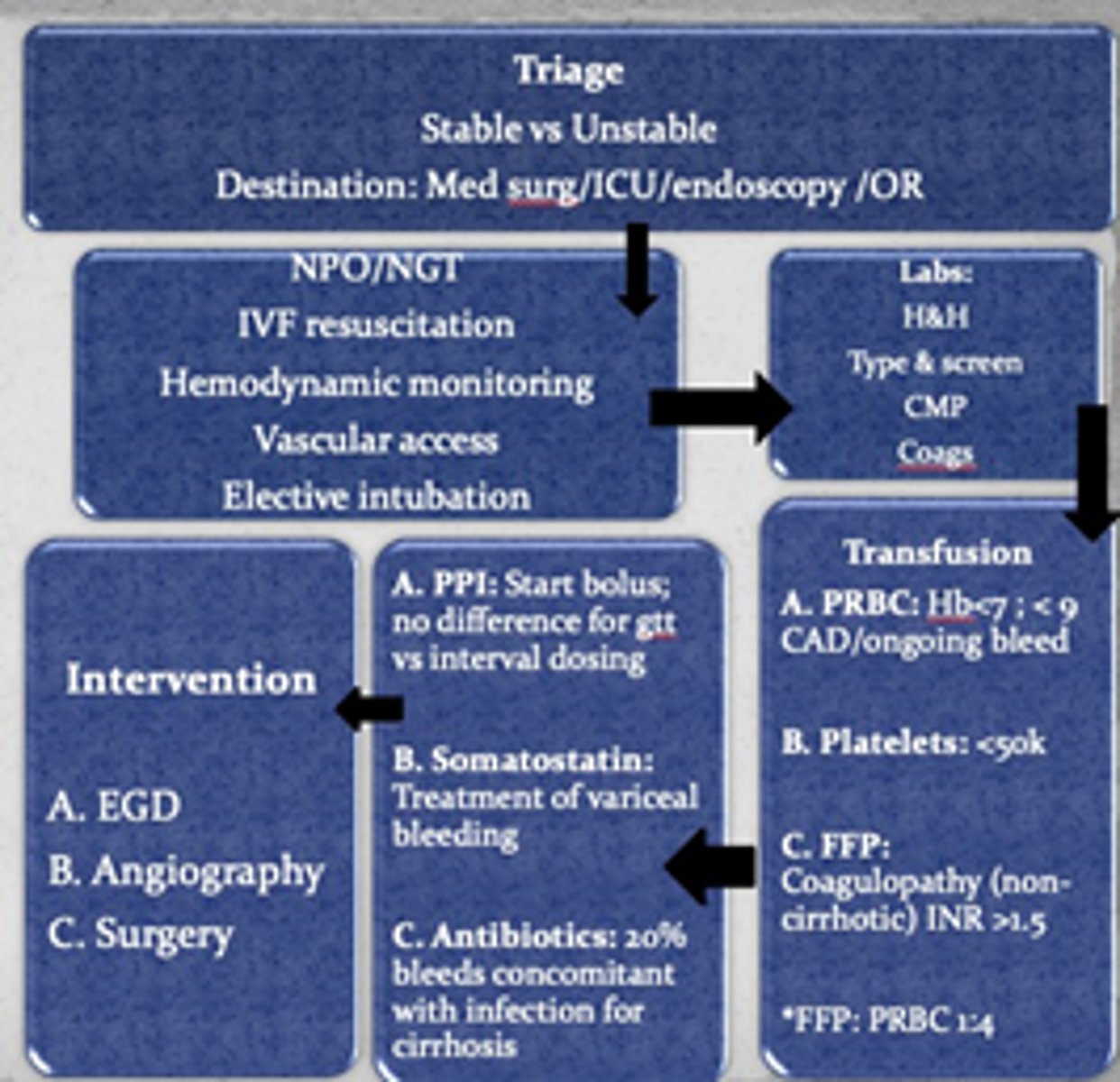
After EGD for treatment of upper GI bleed, patient's hgb drops after 2 stable values. What should be suspected?
Re-bleeding (repeat endoscopy unless risk for perforation)
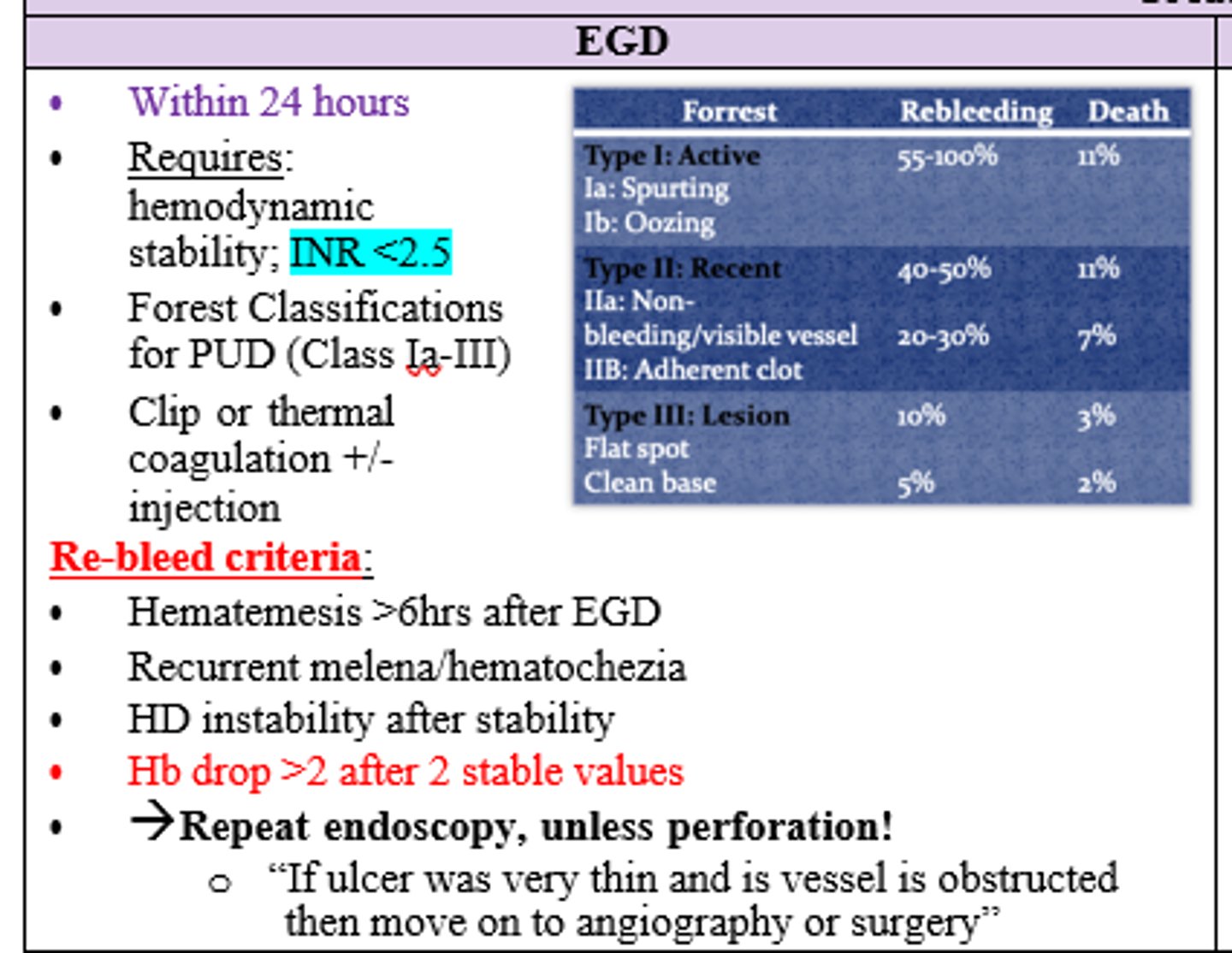
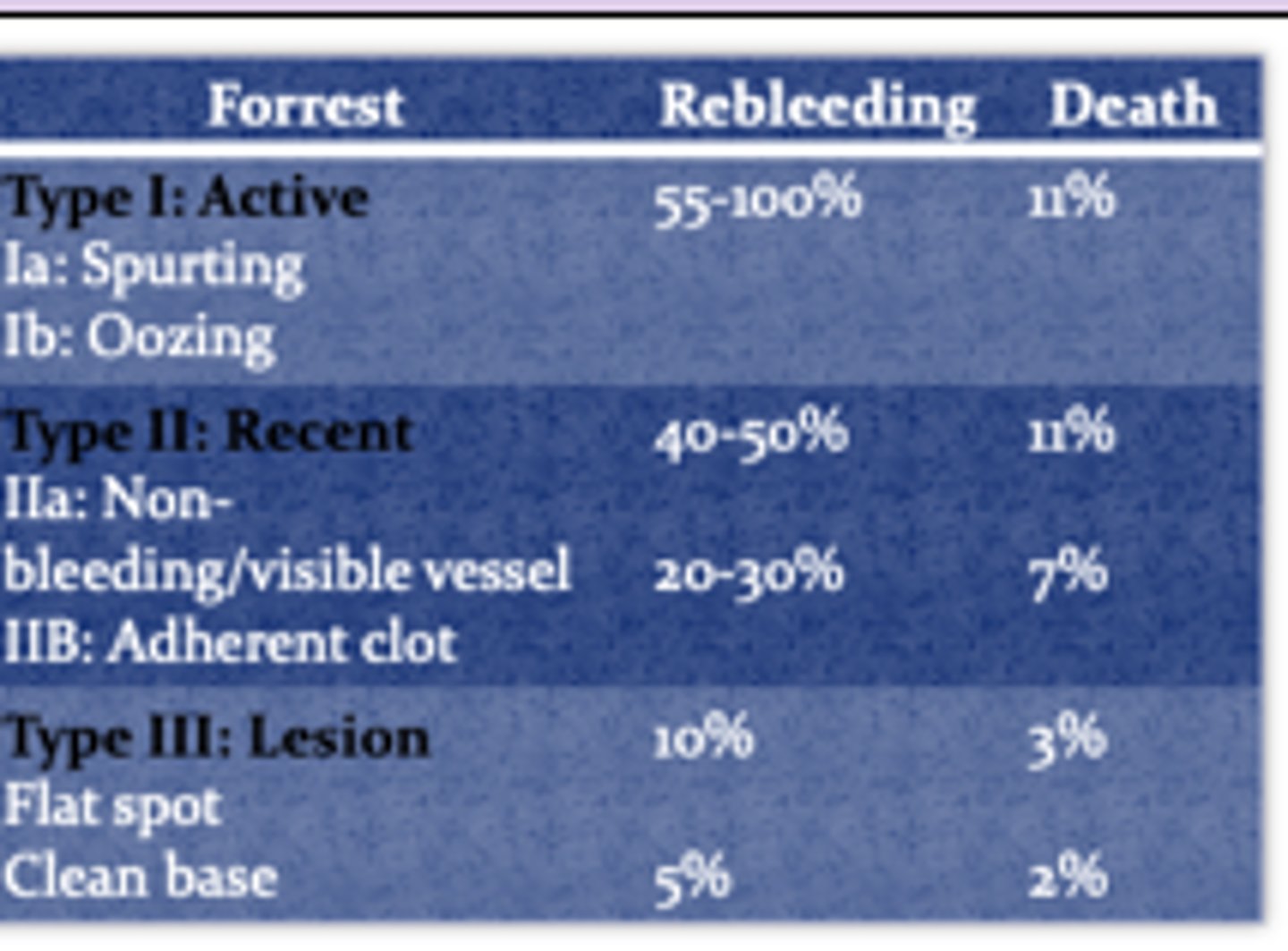
Which Forrest Classification for PUD corresponds with the following:
- Flat spot/ Clean Base (Lesion)
- Non-bleeding/ Adherent Clot (Recent)
- Spurting/ Oozing (Active)
Lesion: Type III
Recent: Type II
Active: Type I
In order to have EGD as not only a diagnostic tool but also treatment for Upper GI Bleed, how soon must this be performed?
Within 24h
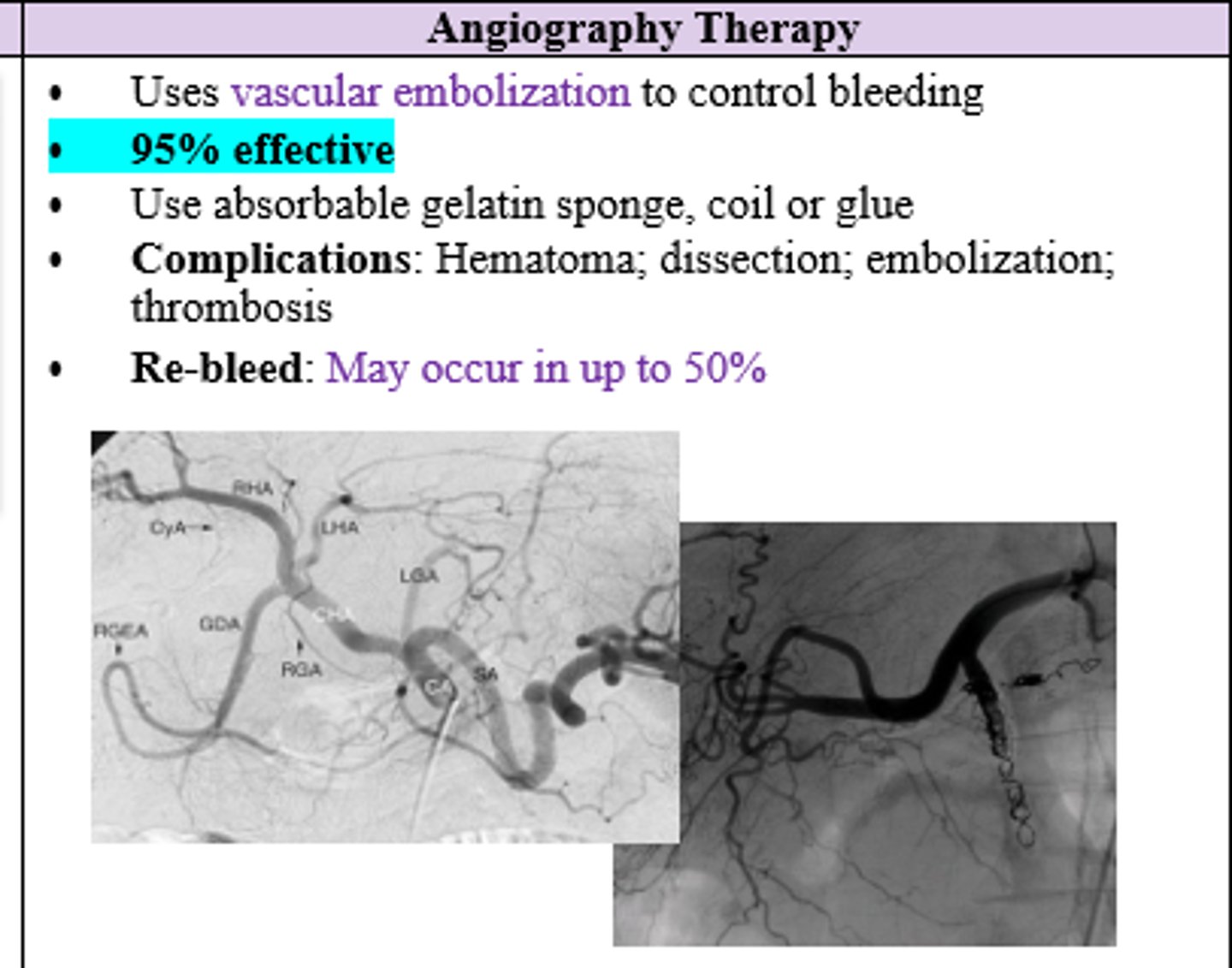
Which therapy for Upper GI Bleed is 95% effective and uses absorbable gelatin sponge, coil, or glue to stop bleed?
Angiography Therapy (uses vascular embolization)
EGD and Angiography Therapy failed to stop a patient's upper GI bleed. Next step?
Surgery
What is the most common site for a perforated peptic ulcer?
Duodenum
Elderly patient has distention and hypotension and you fear they're going into septic shock due to an event that likely occurred 12+ hours before resulting in abdominal RLQ pain/tenderness and fever. Dx?
Perforated PUD (latent presentation >12 hours)
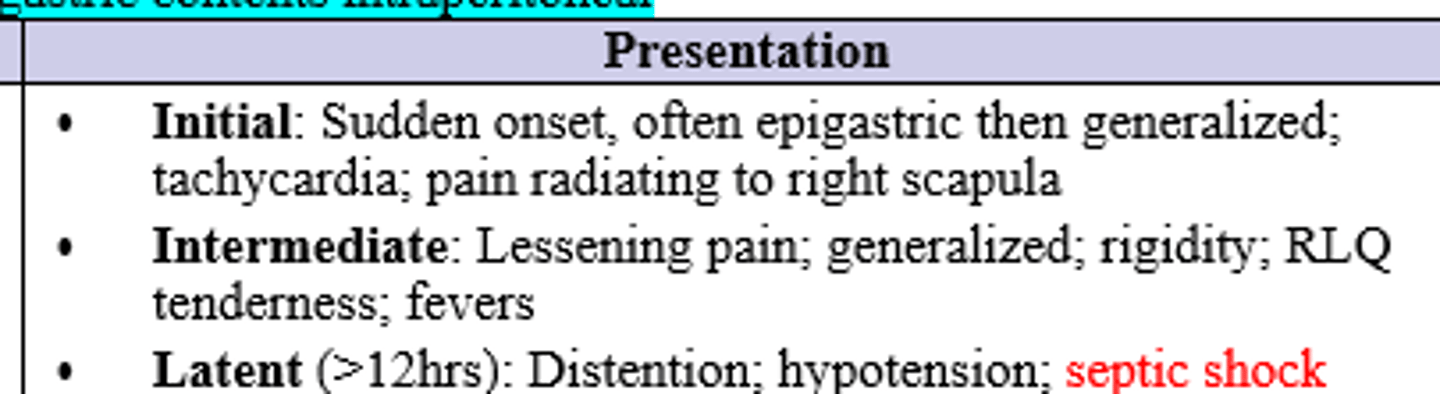
Patient has sudden onset of epigastric pain that radiates to the right scapula and later generalizes. He is tachycardic, but otherwise stable. Diagnostics and Tx for suspected dx?
Labs (CBC, CMP, LA, T&S)
Imaging (CXR/CT > UGI)
Treat conservatively with ABX, Bowel Rest, & drainage if small or no leak on CT (50% perforated ulcers heal spontaneously)
or
Surgery if worsening sx, presentation >24h from onset, large volume pneumoperitoneum, or age >70
T/F Majority of perforated duodenal ulcers have no free air seen on CXR
False (20% reveal no free air)
Which ulcer perforation has a higher risk of mortality, gastric or duodenal?
Gastric (10-40%)
Which surgery provides definitive repair of perforated duodenal ulcer that can be used in high recurrence risk patients (ex. continued NSAIDs)
Graham Patch + TV/Pyloroplasty
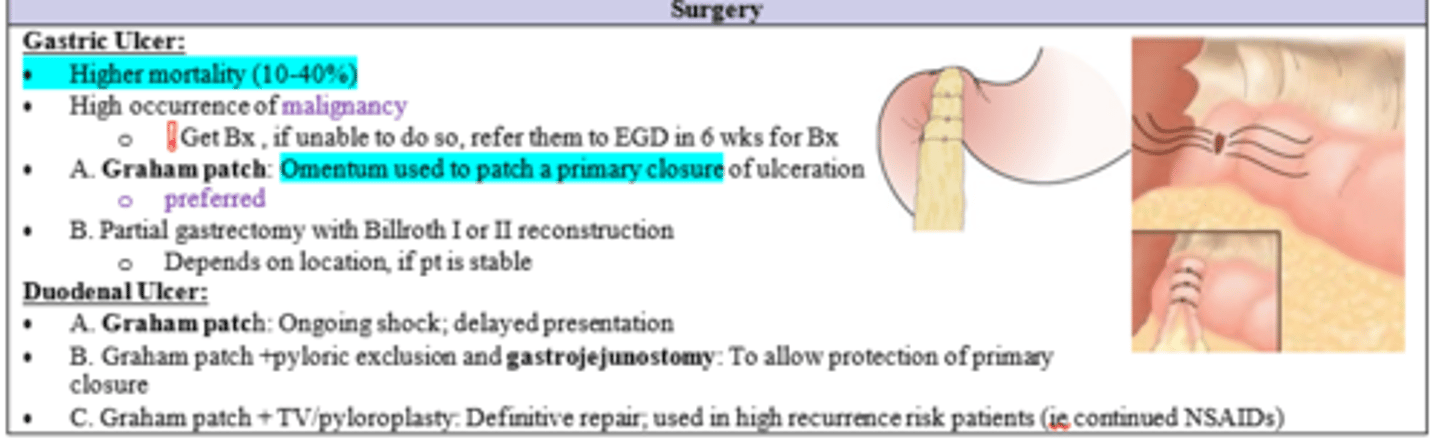
What should be done at the time of surgical intervention for gastric ulcer?
biopsy (if unable, refer to get EGD in 6 weeks)
What is the mc etiology of Mesenteric Ischemia?
Acute Mesenteric Arterial Occlusion (embolism > thrombus)
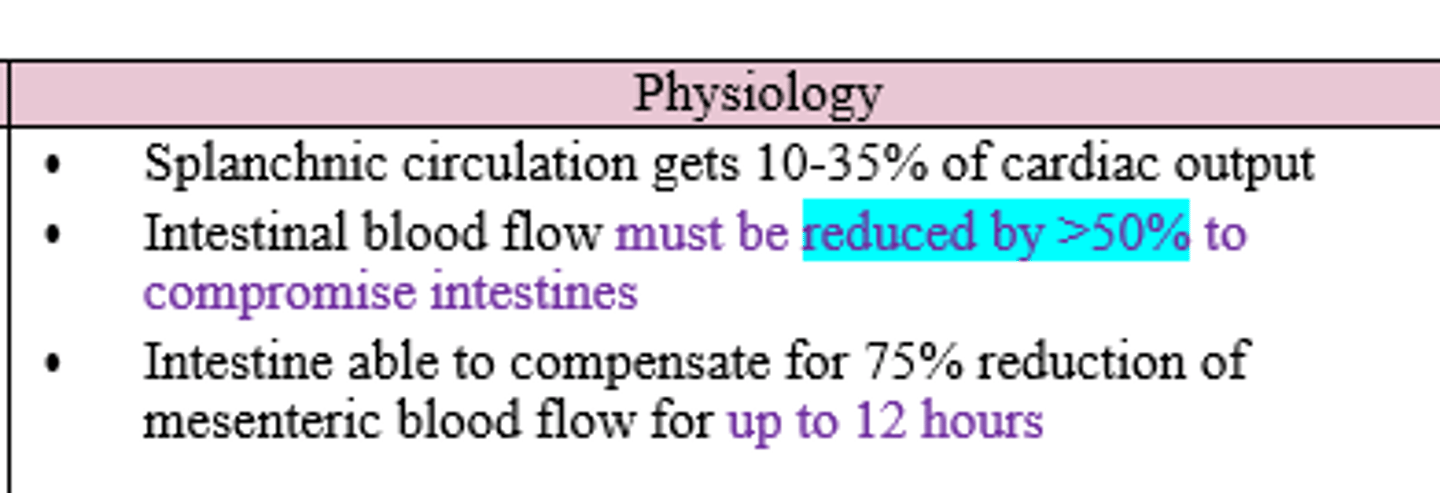
In order for intestines to be compromised, what percentage must blood flow be reduced and how long can intestine compensate?
>50%; can compensate for redux of 75% for up to 12 hours
In Acute Mesenteric Arterial Occlusion, where do the majority of emboli originate from?
Heart (CAD/PAD = risk factors)
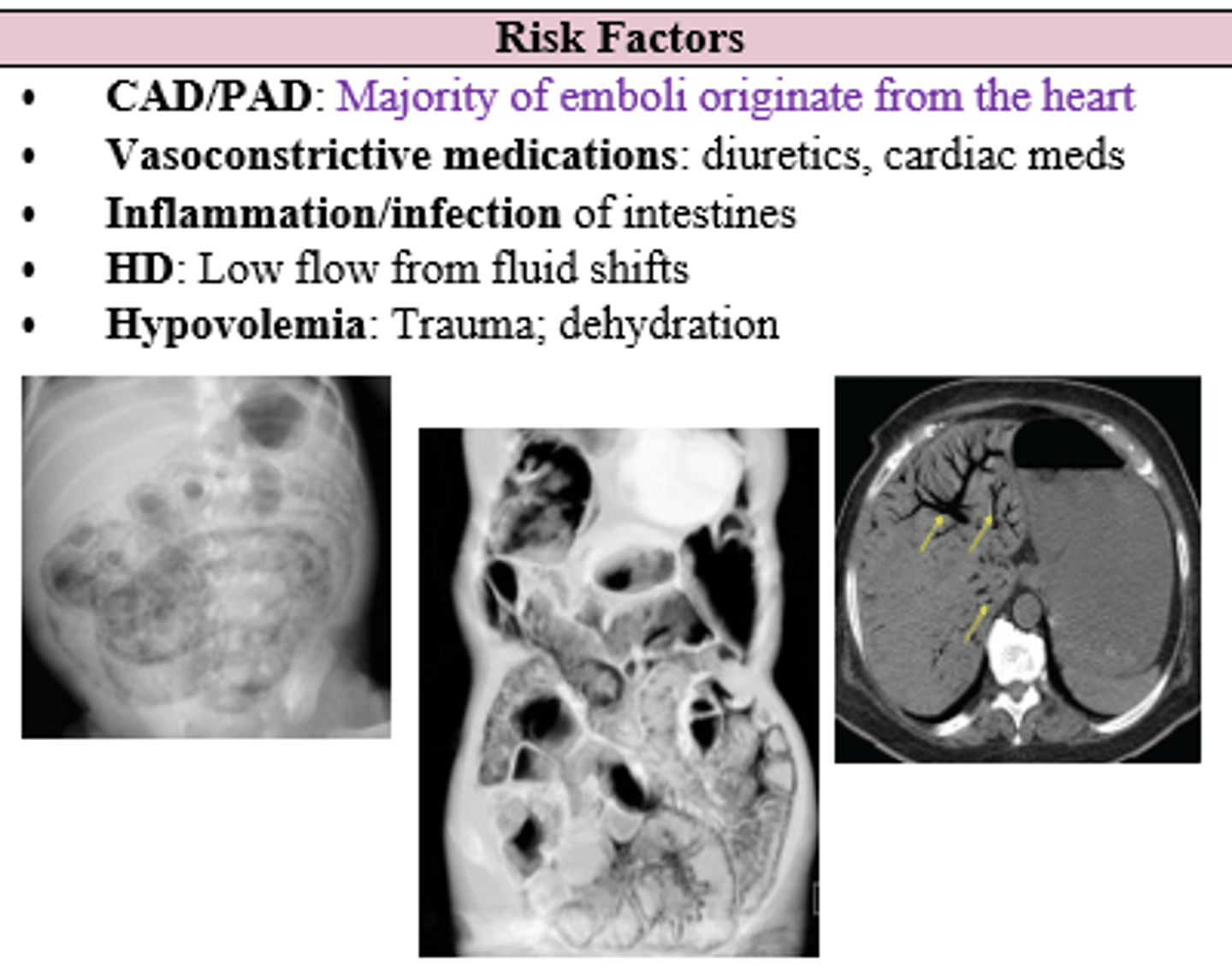
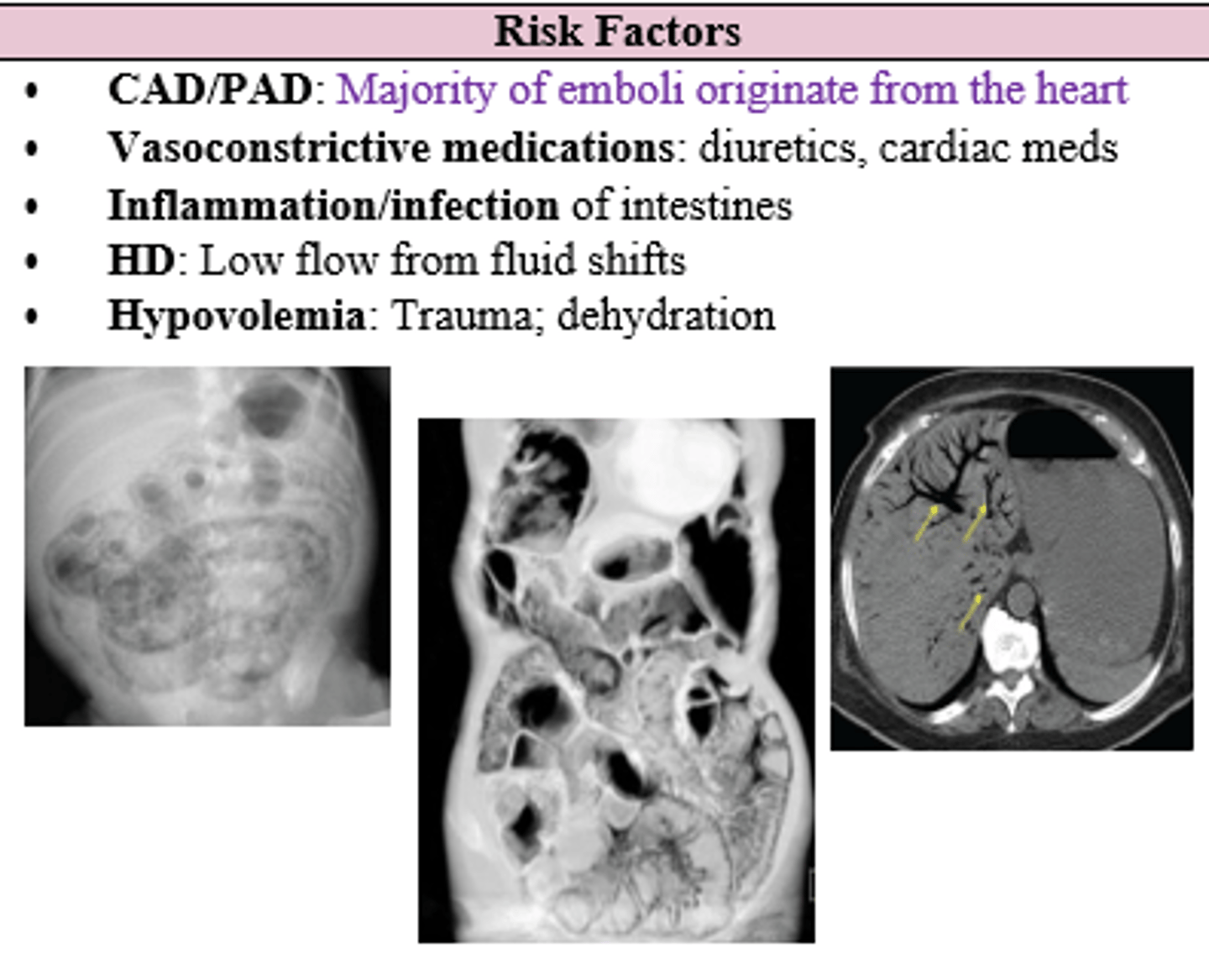
What are the risk factors for mesenteric ischemia?
CAD/PAD
Vasoconstrictive Meds
Inflammation/Infection
HD (hemodialysis?)
Hypovolemia
Patient with hx of prior embolic event c/o post prandial pain, food aversion, and abdominal pain out of proportion to the exam. Labs and reason for obtaining?
CBC (+/- marked leukocytosis)
ABG (metabolic acidosis)
Lactic Acid (86% specific for acute mesenteric ischemia)
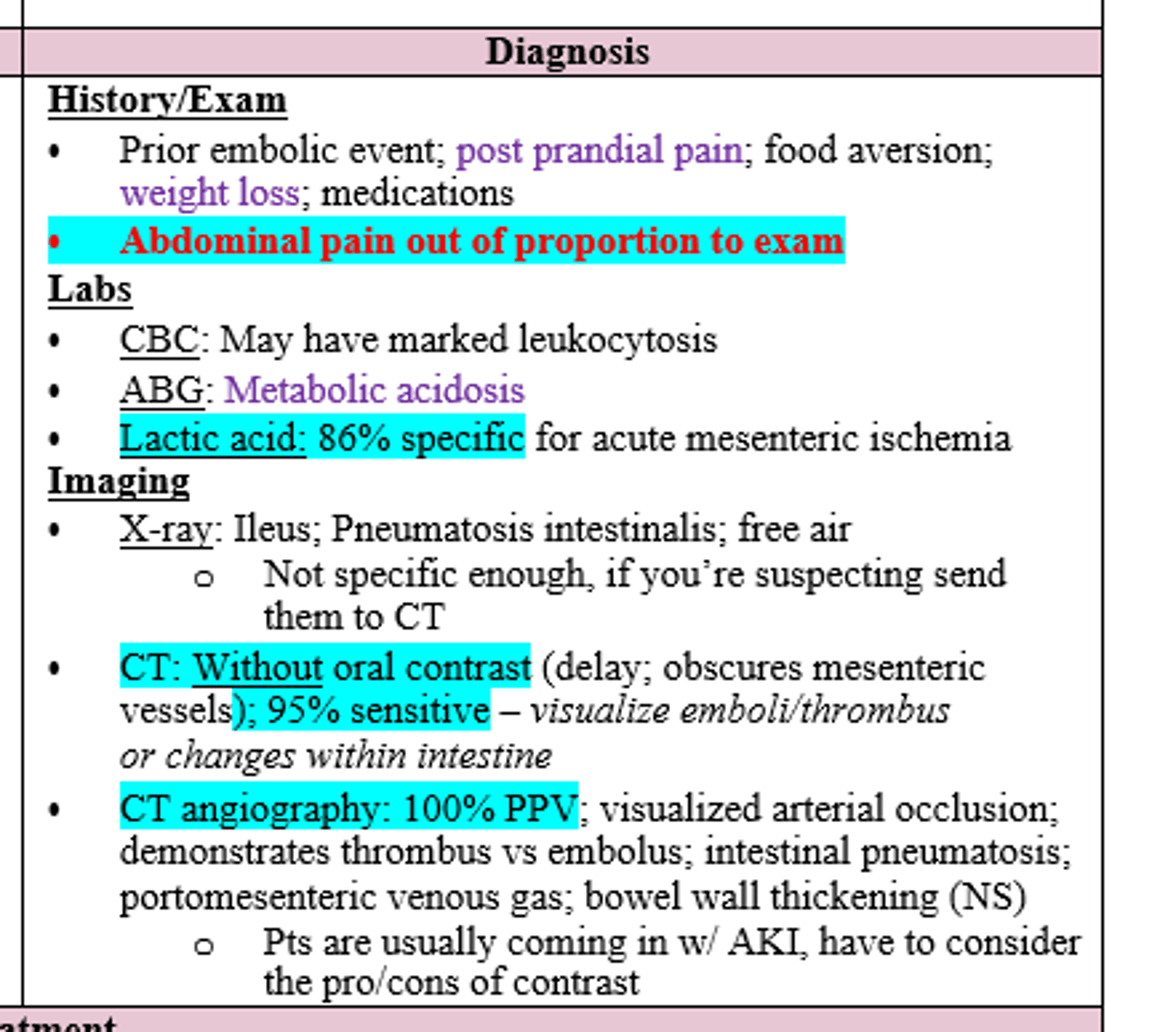
Patient with hx of prior embolic event c/o post prandial pain, food aversion, and abdominal pain out of proportion to the exam.
CBC showed leukocytosis, ABG reveals metabolic acidosis, and lactic acid is elevated.
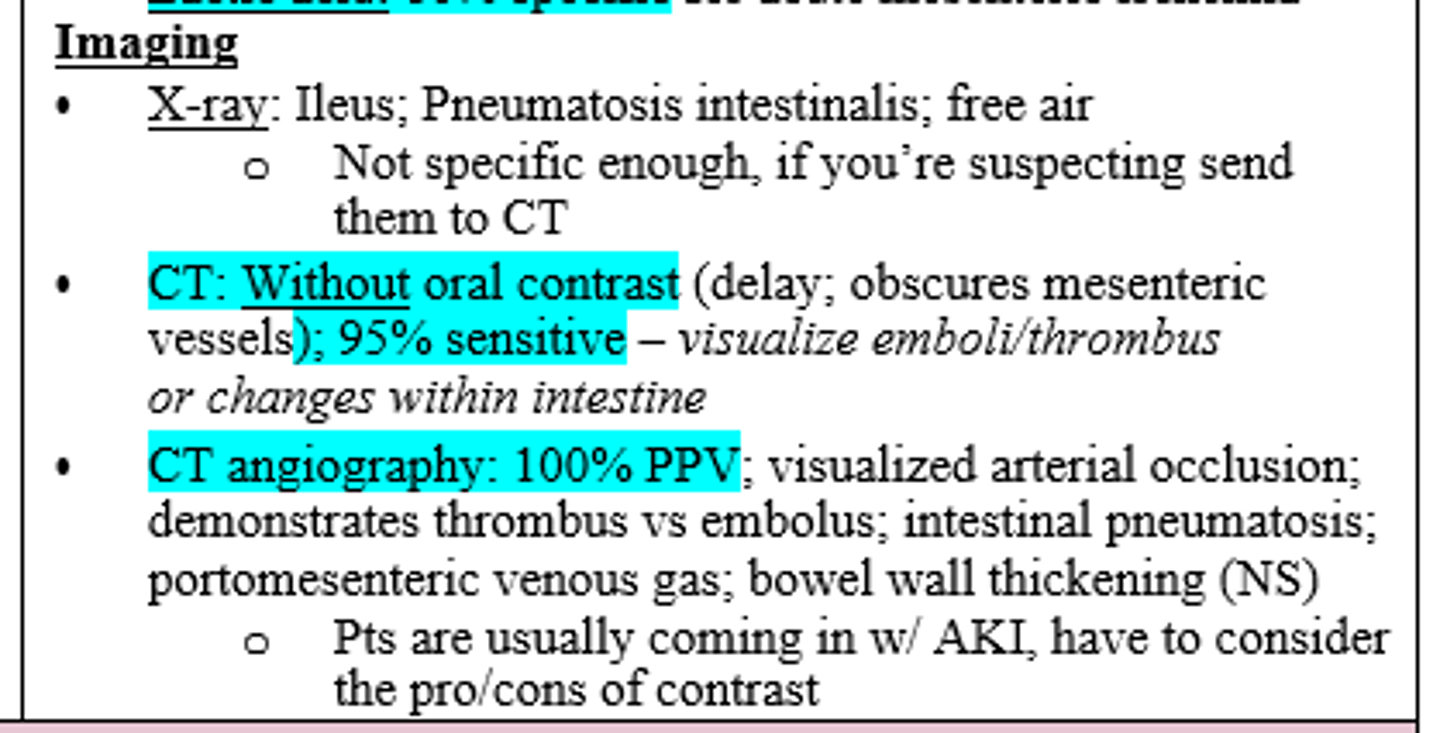
Imaging of choice for suspected dx?
CT without oral contrast (95% sensitive; dx = Acute Mesenteric Ischemia) or CTA if CT is inconclusive (100% PPV, but not great for pts with AKI)
In the ER, you dx your patient with Acute Mesenteric Ischemia after confirming with CT w/o contrast. What is your next order?
NPO/NGT (surgery prep)
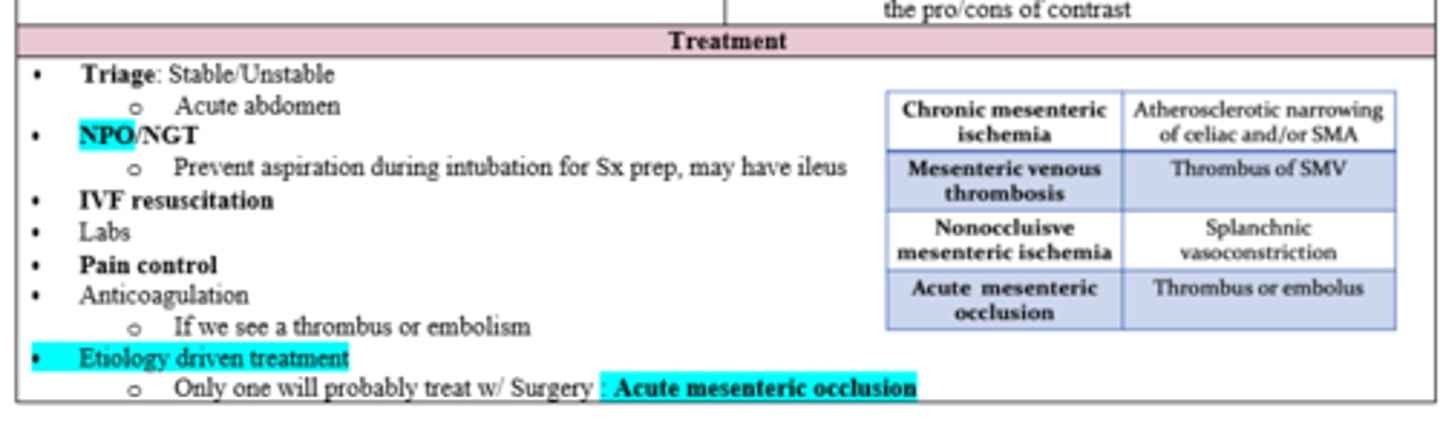
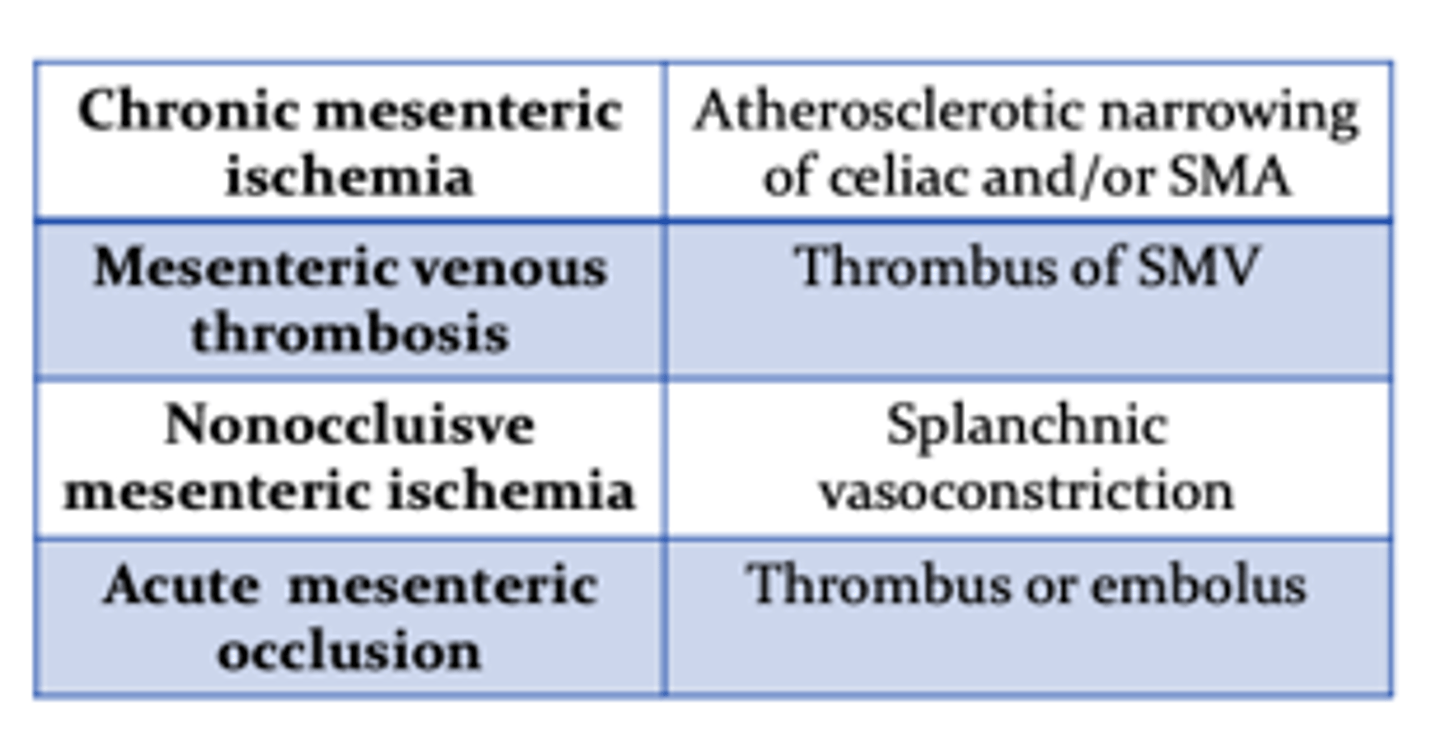
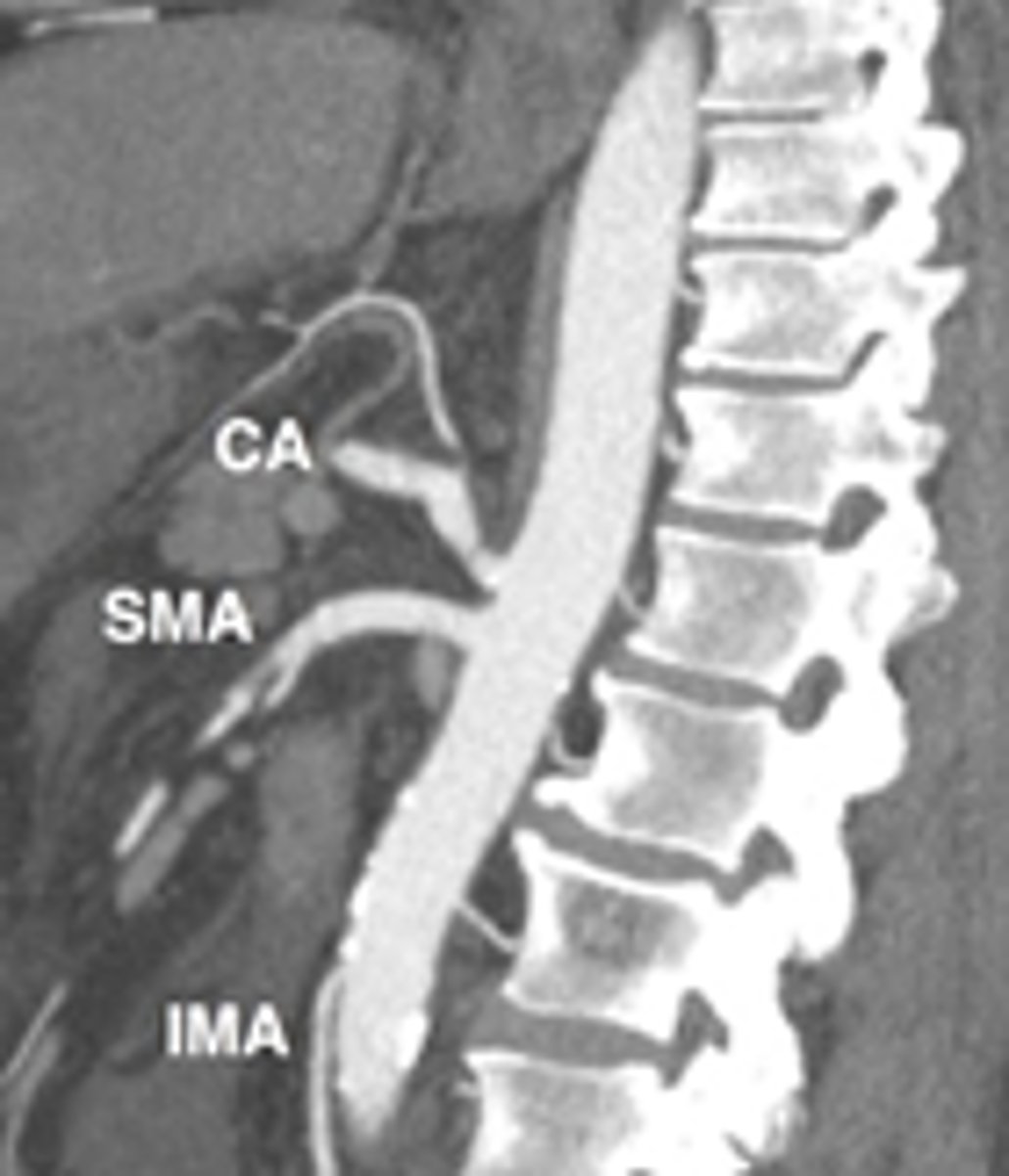
What is the most likely etiology of Chronic Mesenteric Ischemia?
Atherosclerotic narrowing of celiac and/or SMA
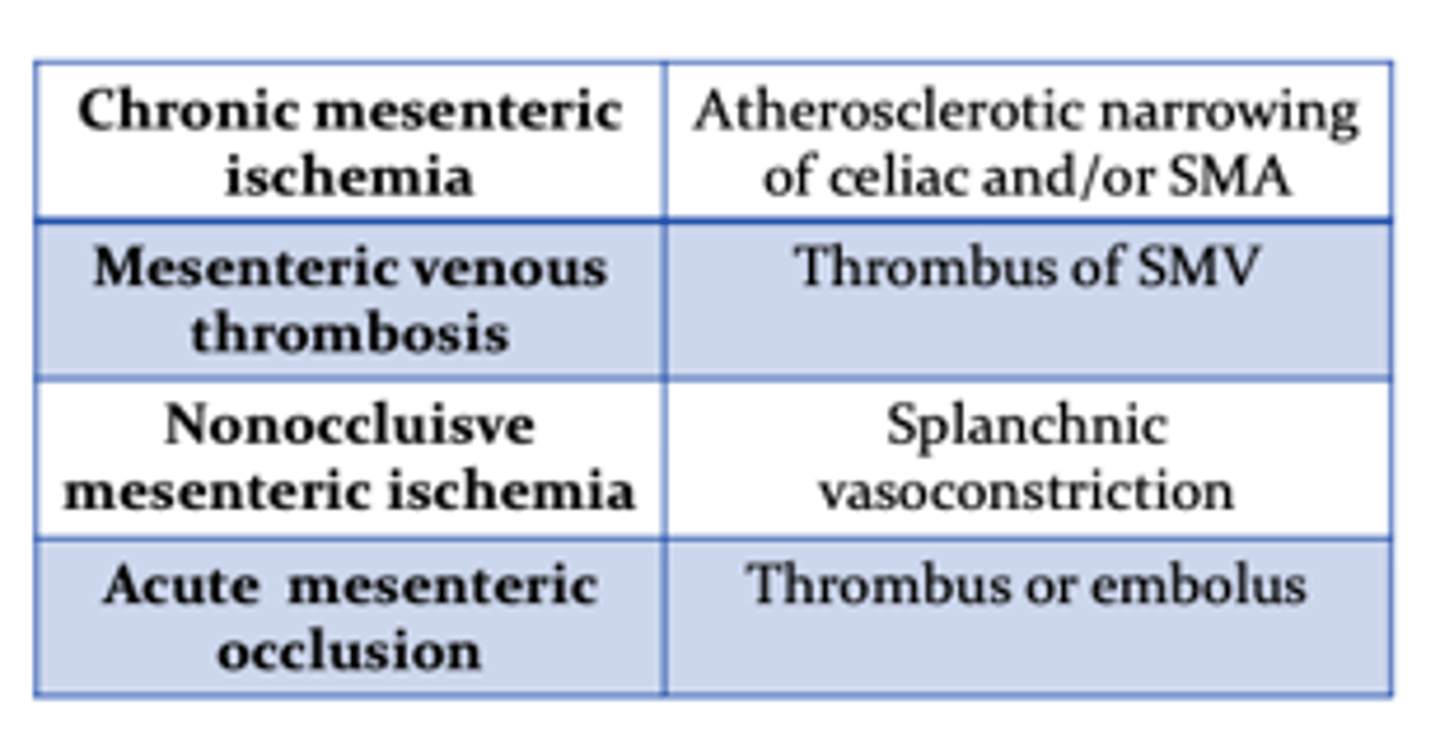
Where is the most likely location of a Mesenteric Venous Thrombosis?
Thrombus of SMV
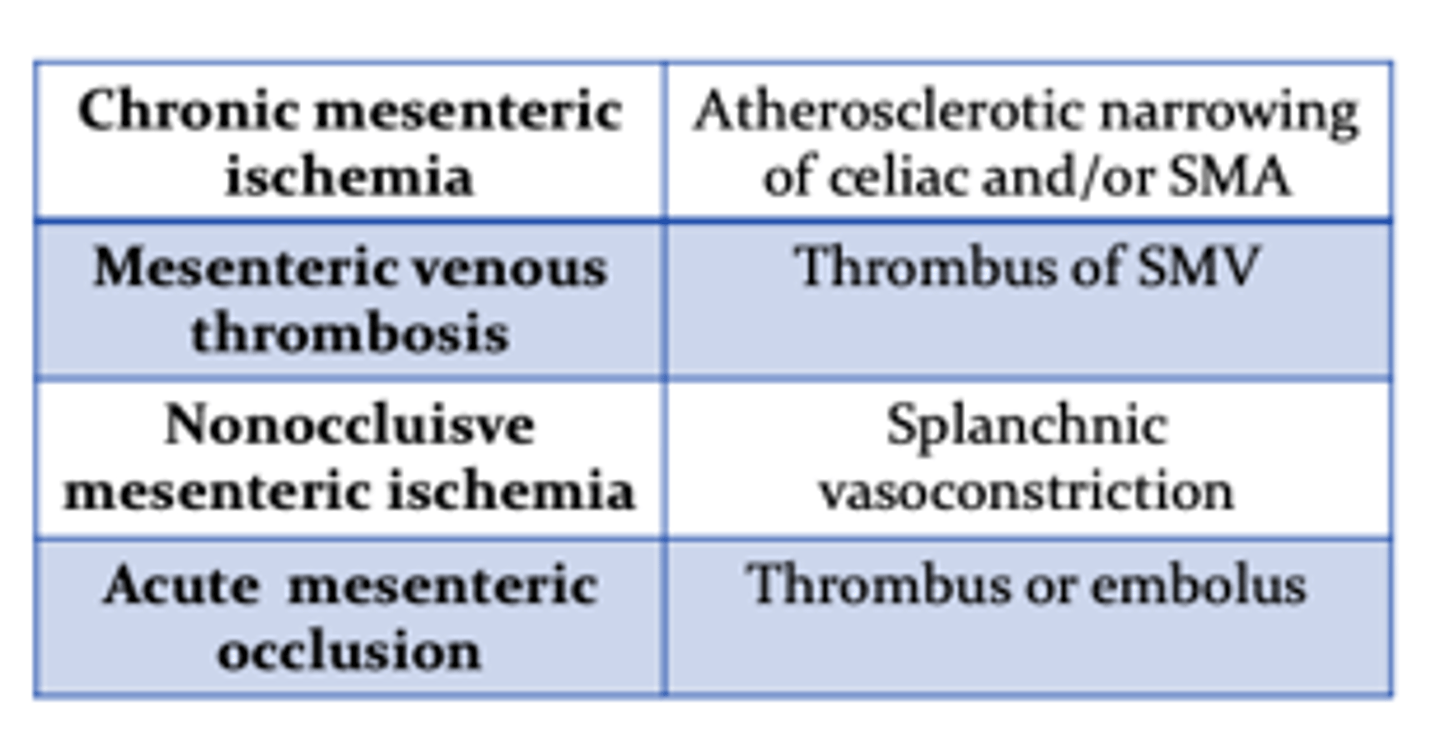
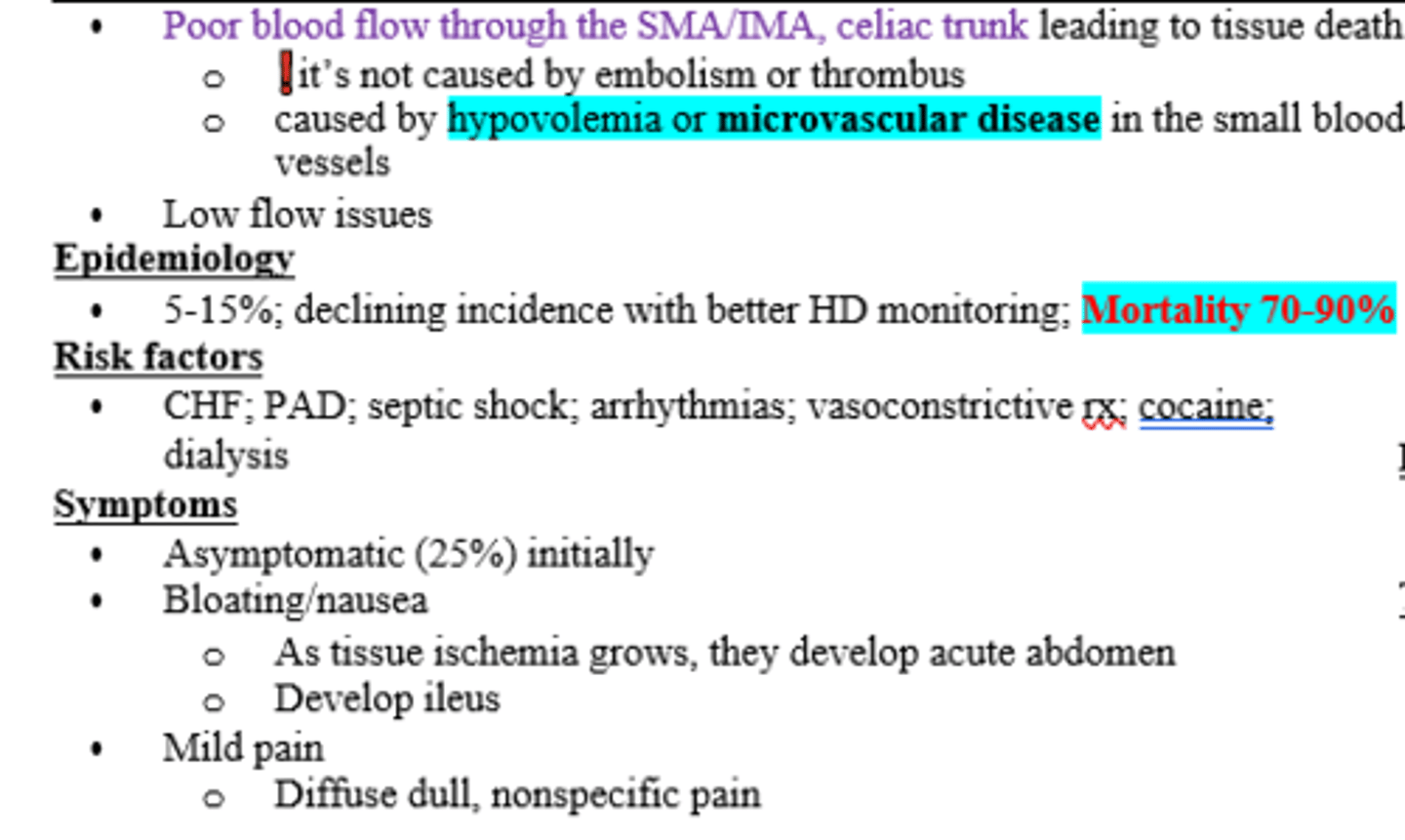
What is the most likely etiology for Nonocclusive Mesenteric Ischemia?
Splanchnic vasoconstriction
Which etiology of Chronic Mesenteric Ischemia is dt compression of celiac trunk?
Median Arcuate Ligament Syndrome
Pt c/o rapid weight loss and postprandial pain (not epigastric). Though rare, you suspect their dx could be due to Median Arcuate Ligament Syndrome. Top DDX?
Chronic Mesenteric Ischemia (MALS is rare etiology of CMI)
60+ yo Female with + smoking history and PMH of hyperlipidemia presents to her PCP c/o weight loss dt fear of eating from postprandial pain. How do you make your dx and what is the tx?
Duplex US (+/- CTA or CTA wIVC)
Tx: Behavior mod, antiplatelet therapy, +/- revascularization if enough of an occlusion (refer to vascular surgeon)
FYI dx = Chronic Mesenteric Ischemia
Patient presents to PCP dt dull, nonspecific abdominal pain x 2-3 days with associated bloating and constipation. PMHx is notable for pancreatitis and splenectomy a few years ago. Work up and Tx for suspected dx?
MR Venography vs CTA
Tx: NGT/IVF, anticoagulation or refer to vascular surgeon for transvenous thrombolysis/ thrombectomy
(Dx = Mesenteric Venous Thrombosis with 2ndary ileus)
Which form of mesenteric ischemia has the highest percentage of mortality?
Nonocclusive Mesenteric Ischemia (70-90%)
Dialysis patient with hx of CHF, PAD and cocaine use c/o bloating, constipation, and nausea. They c/o diffuse, dull abdominal pain that is nonspecific to palpation. Mesenteric CT arteriography confirms suspected dx. Dx and Tx?
Dx: Nonocclusive Mesenteric Ischemia
Tx: NGT decompression, IVF (correct for acidosis), Abx
correct underlying issue of hypovolemia/ hypotension
Avoid vasoconstriction
Surgery to resect dead intestin (emergent if acute abdomen)
In acute mesenteric arterial occlusion, what is the most common etiology, thrombus or embolus?
Embolus (typically lodges 3-10 cm distal to take off, sparing first jejunal branches)
Which risk factors put a patient at risk for BOTH thrombus and embolus induced acute mesenteric arterial occlusion?
Smoking, HTN, HLD, DM
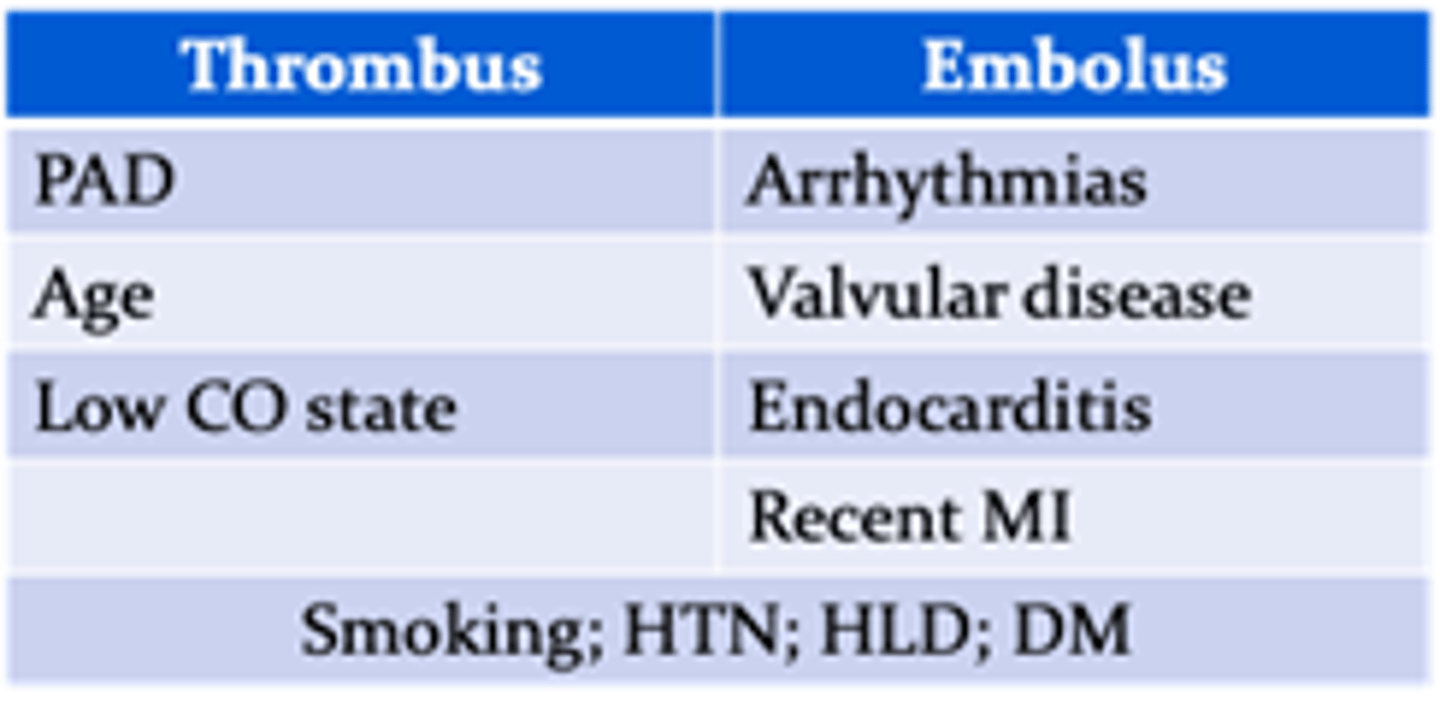
When a thrombus causes acute mesenteric arterial occlusions, which arteries are typically involved?
Both SMA & Celiac (dt collateral formation; thrombus typically forms at the take off of celiac axis or SMA)
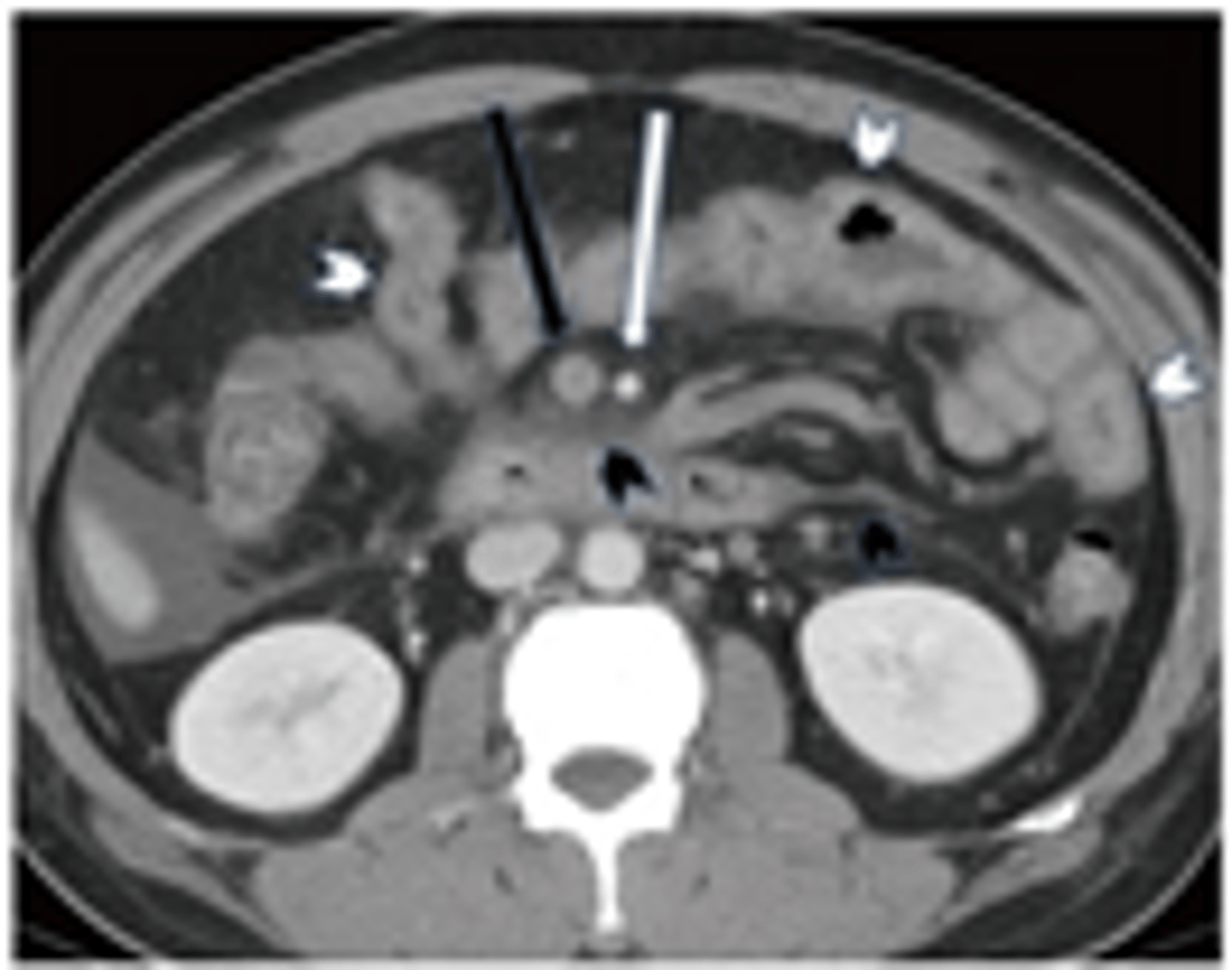
When a patient presents for Acute Mesenteric Arterial Occlusion, confirmed by CTA, what is the treatment?
Surgery (following NPO/NGT, IVF [avoid vasopressors], Heparin, Empiric Abx, PPIs)
![<p>Surgery (following NPO/NGT, IVF [avoid vasopressors], Heparin, Empiric Abx, PPIs)</p>](https://knowt-user-attachments.s3.amazonaws.com/5f65fc51-f53e-4aa9-9d62-bfe80be0b077.png)
What is typically done [>70% of cases]24-48 hours after surgery for Acute Mesenteric Arterial Occlusion?
Second-Look Laparotomy (28% require further resection)
Looking for color, distension, peristalsis, or bleeding
(FYI keep abdomen open if anticipating this during 1st surgery)

What is the prognosis for Acute Mesenteric Arterial Occlusion?
30-60% need open or endovascular surgery
40% 1 year survival
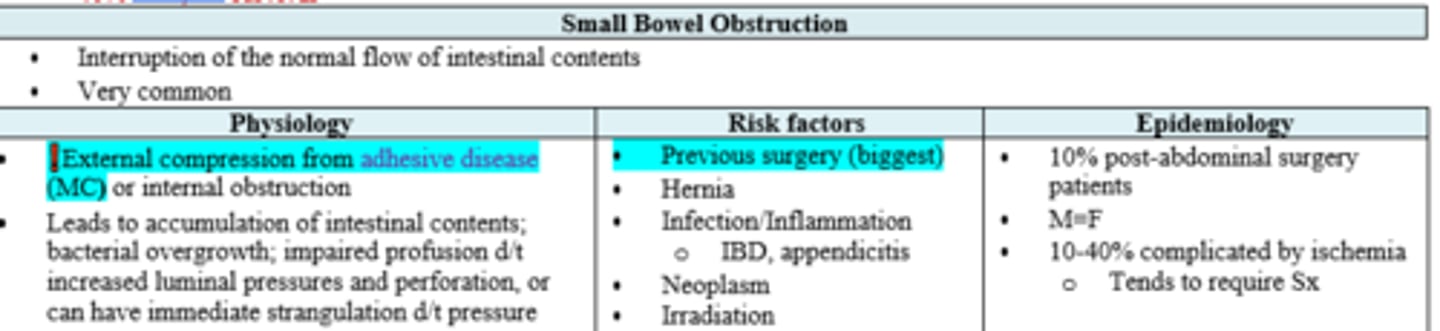
What is the most common etiology for SBO?
What about the biggest risk factor?
External compression from adhesive disease (aka adhesions- 70%);
Previous surgery
Patient c/o cramping abdominal pain and n/v/d followed by constipation then obstipation. PE reveals distended abdomen thats diffusely tender with tympany present. PSH + appendectomy as a young adult. Work up?
X-Ray or CT

What on x-ray indicates probably SBO?
Dilated loops with air-fluid levels, lack of gas in colon
(FYI - non-diagnostic in 10-20%)

What treatment for SBO is effective 80-90% of the time?
NGT/NPO
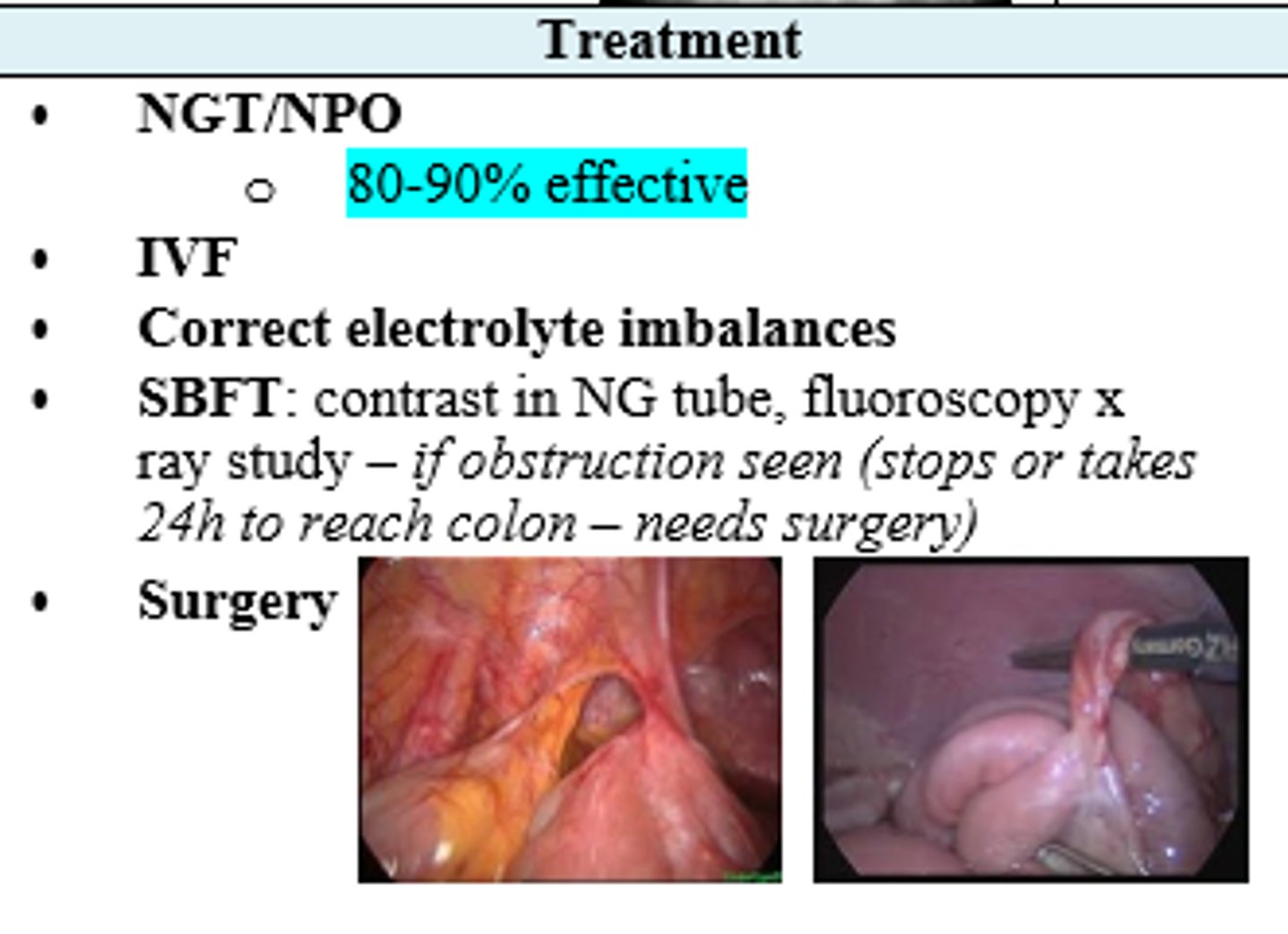
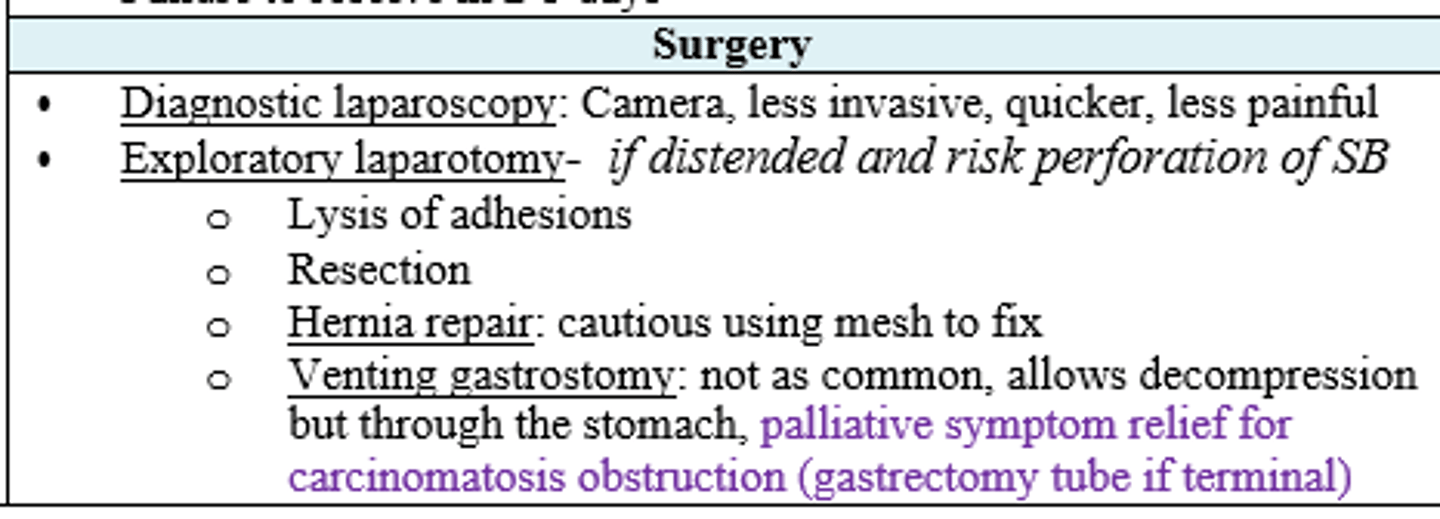
What are the surgical indications for a patient with SBO?
Free air
Peritonitis
Closed Loop Obstruction (NG will not help usually)
Failure to resolve 2-5 days
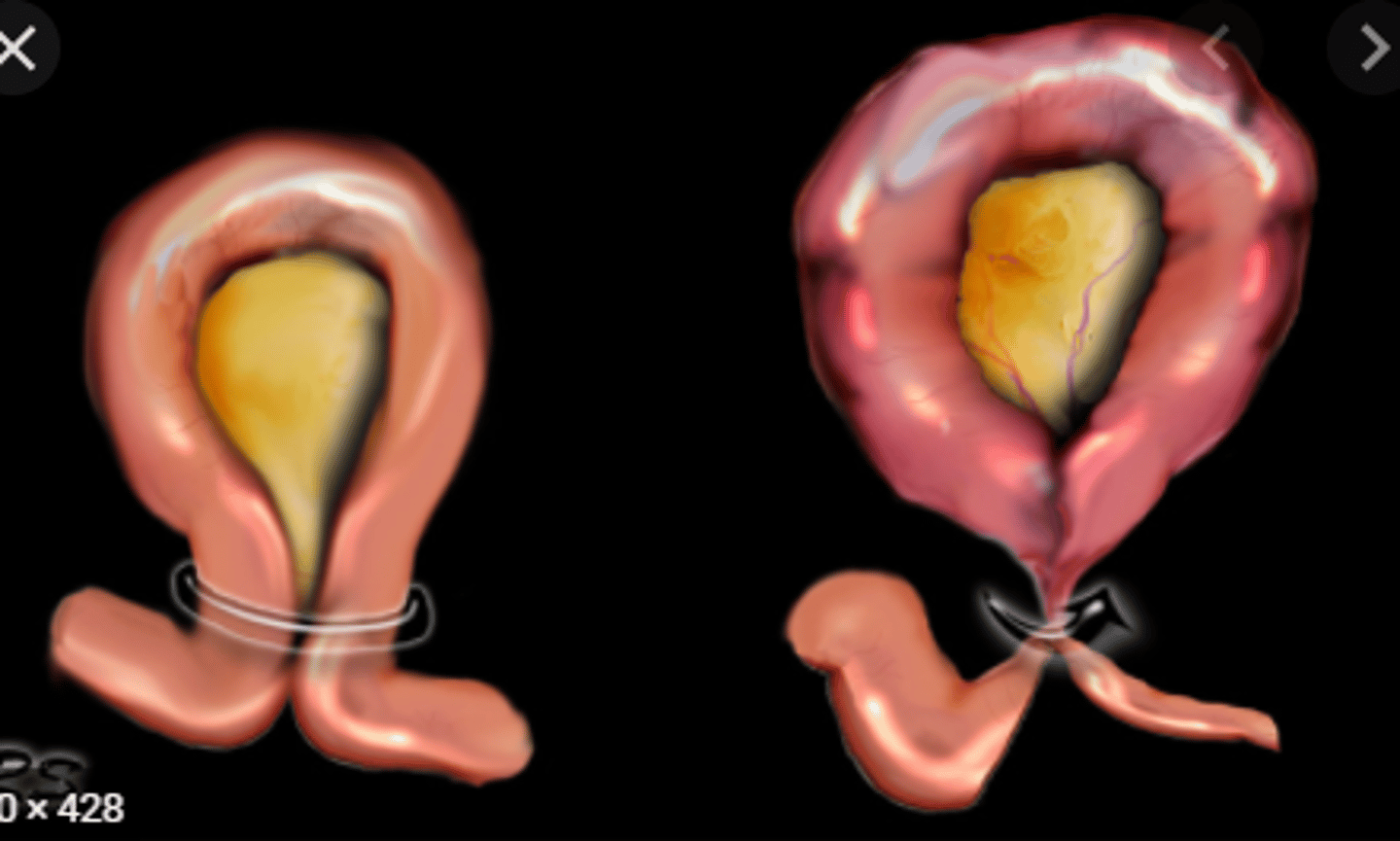
Patient with distended abdomen and SBO is at high risk of perforation. Which surgical method is preferred?
Exploratory laparotomy
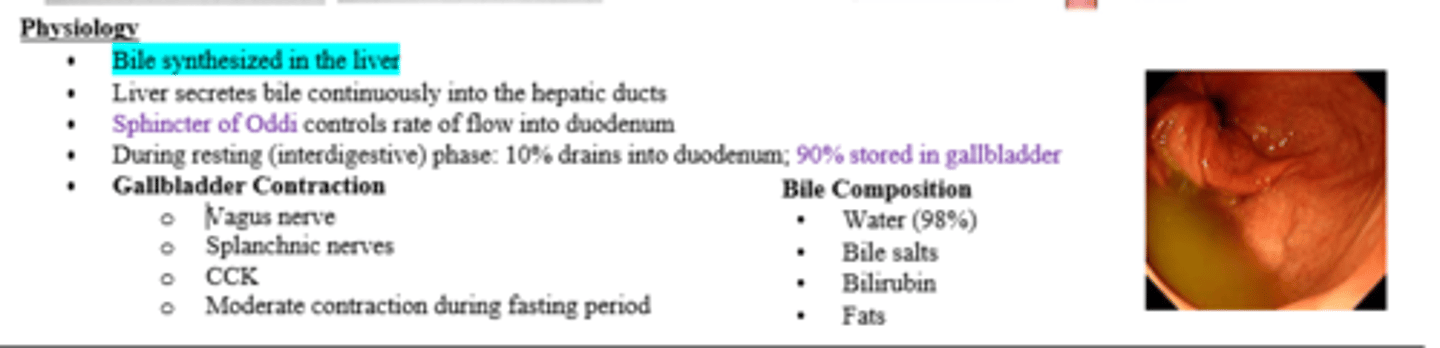
How many mL does gallbladder typically store?
30-50mL
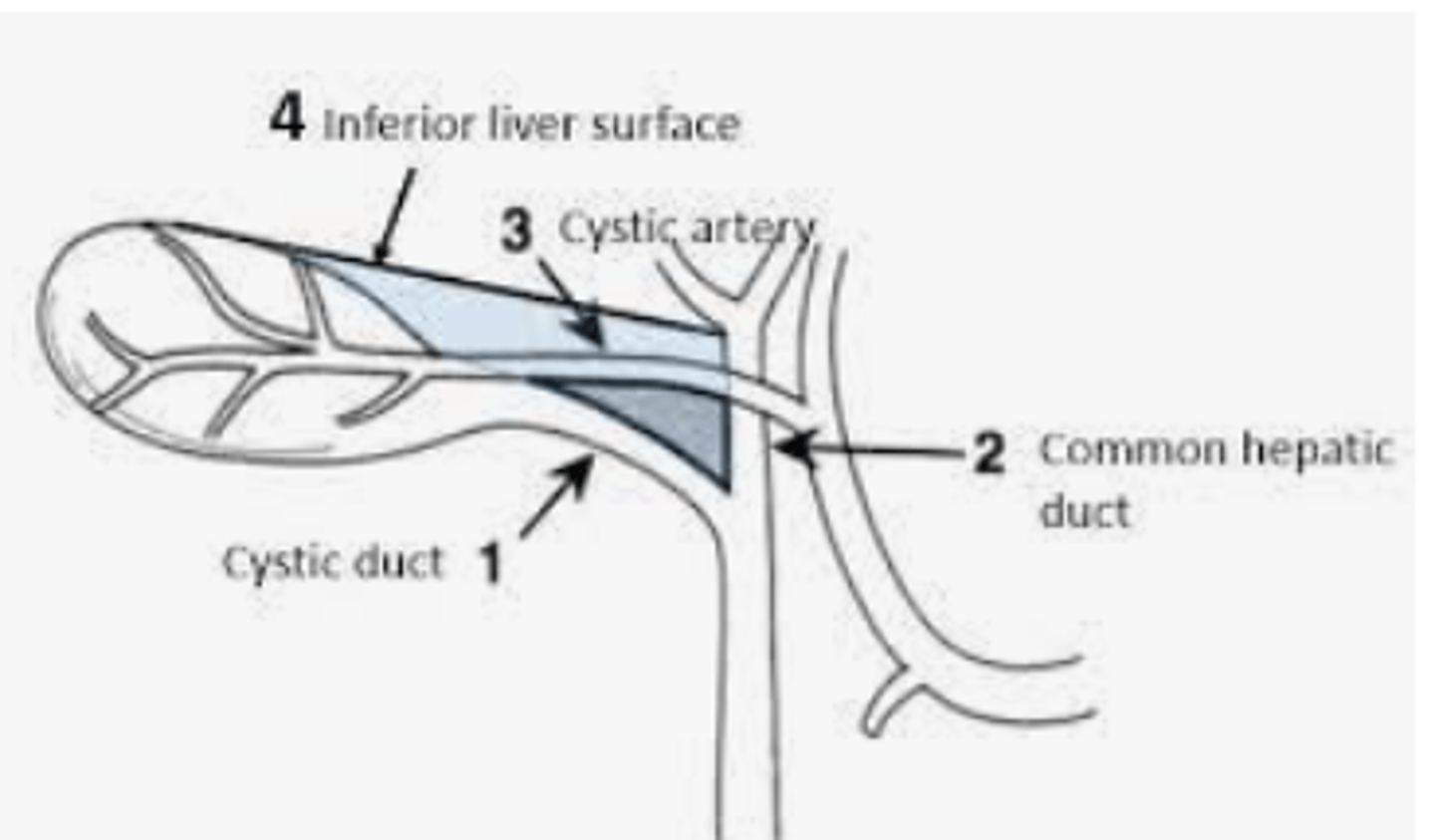
What makes the Triangle of Calot?
What structure typically transverses this triangle?
Common Hepatic Duct
Cystic Duct
Inferior Edge of Liver;
Cystic Artery
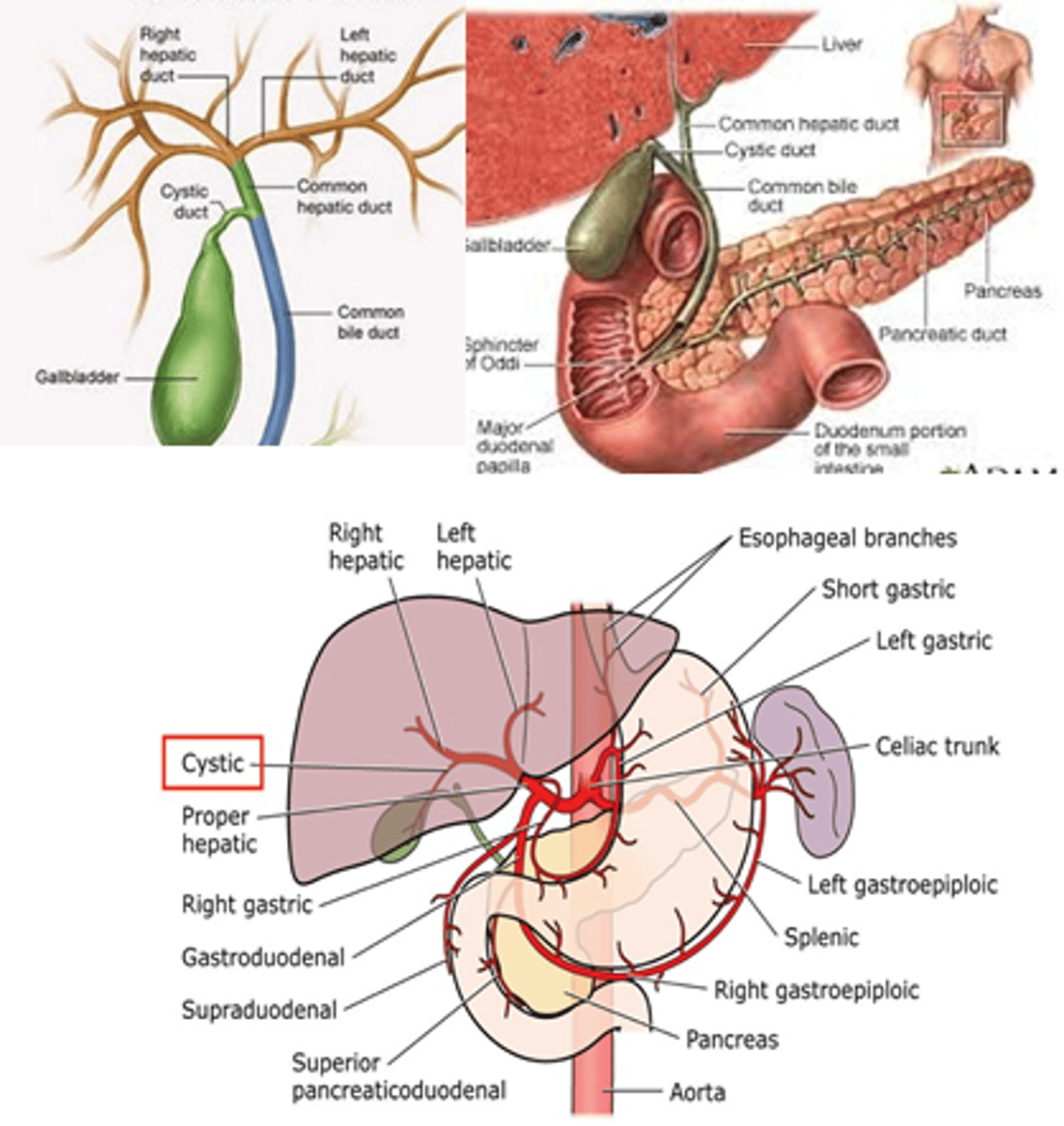
Describe the flow of bile starting at hepatic ducts
Hepatic ducts >
CHD >
CD >
CBD >
Major Duodenal Papilla/Ampulla of Vater [along w Pancreatic Duct] >
Duodenum
![<p>Hepatic ducts ></p><p>CHD ></p><p>CD ></p><p>CBD ></p><p>Major Duodenal Papilla/Ampulla of Vater [along w Pancreatic Duct] ></p><p>Duodenum</p>](https://knowt-user-attachments.s3.amazonaws.com/b29a0b82-2854-49f6-a287-970fcff34eb1.png)
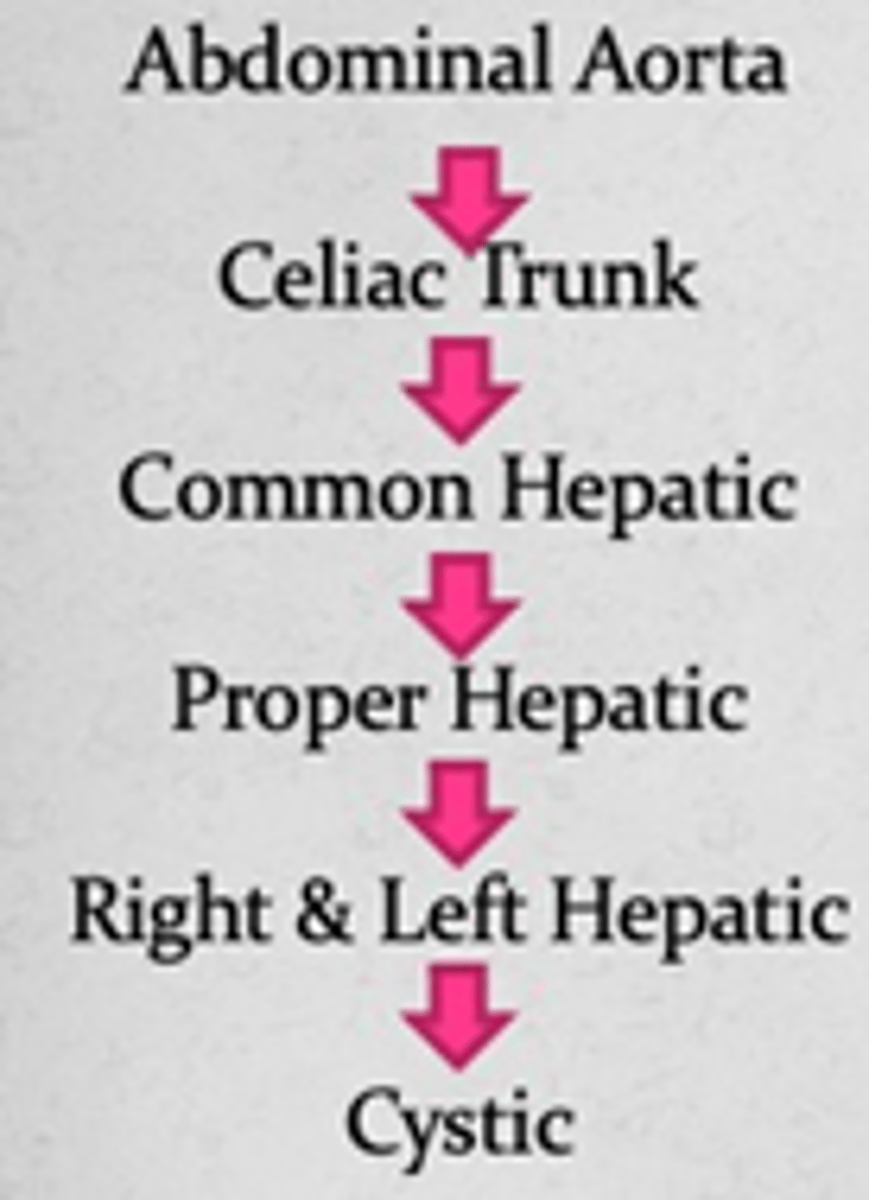
Describe the arterial blood flow to the cystic artery
Abdominal Aorta >
Celiac Trunk >
Common Hepatic >
Proper Hepatic >
R/L Hepatic >
Cystic
What is bile composed of?
Water (98%), Bile salts, bilirubin, fats
What percentage of patients with Cholelithiasis are asymptomatic?
80%
Female pt with hx DM and obesity experiences rapid weight loss after starting at a gym. She states she still eats fast food from time to time, but has noticed afterward she has RUQ/Epigastric pain lasting anywhere from 30m-6h. Labs are all normal. Next step?
US of gallbladder (dx= cholelithiasis; because of biliary colic + stones - send to surgeon)
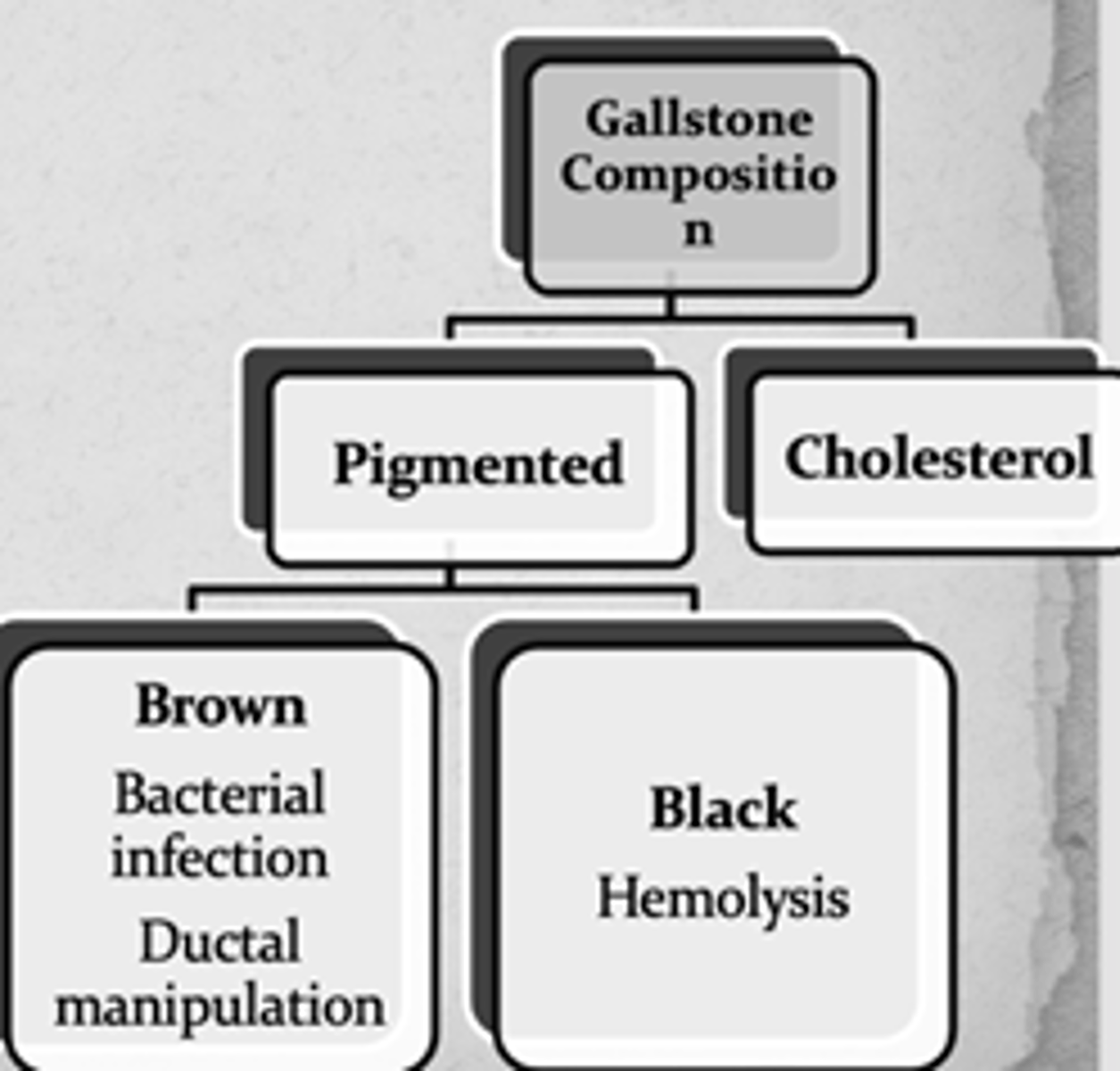
What color pigmented gallstones indicate hemolysis?
What about bacterial infection or ductal manipulation?
Black; Brown
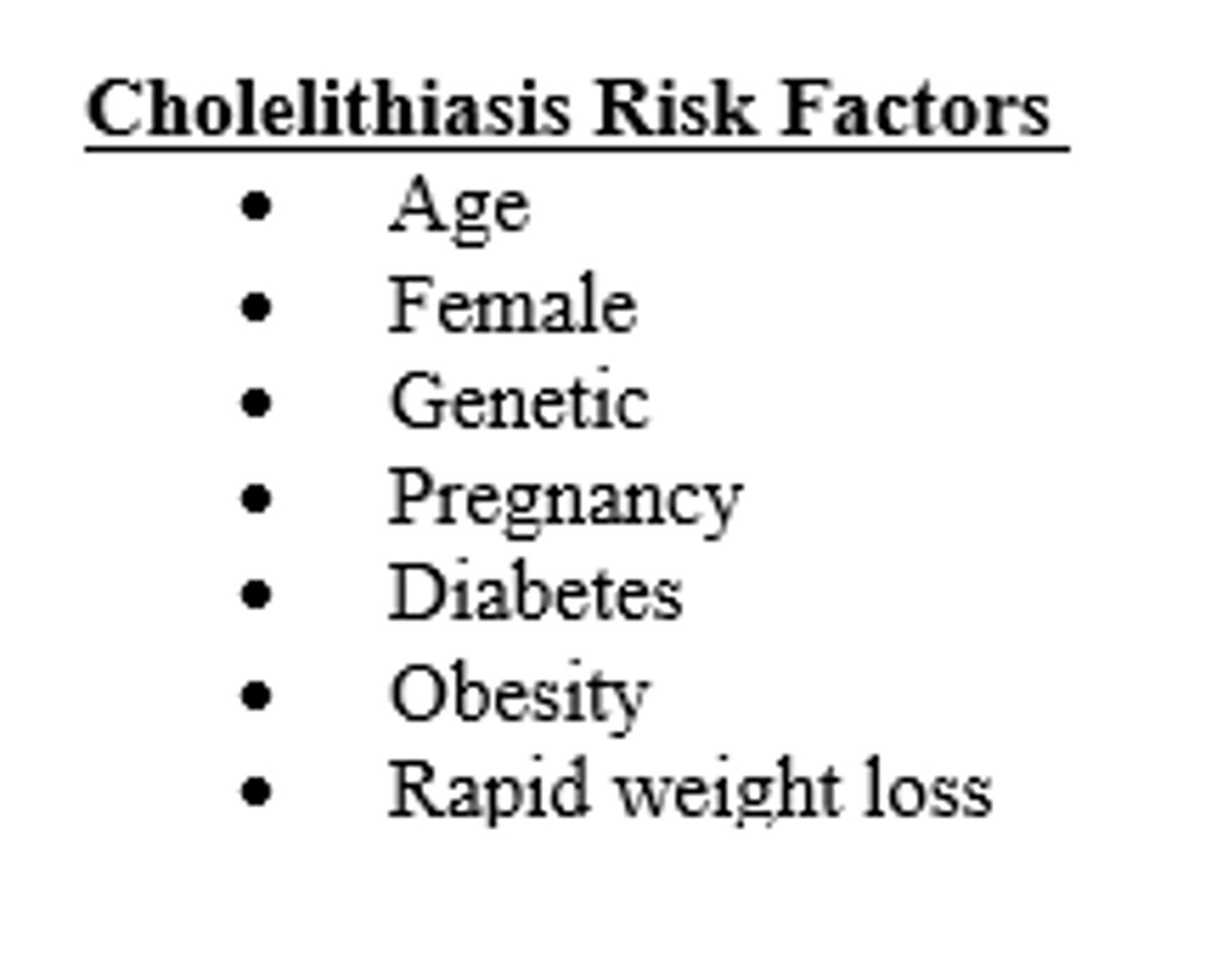
Which of the following is NOT listed as a risk factor for cholelithiasis:
A. Rapid weight loss
B. Pregnancy
C. Genetic
D. Male
D. Male (all of the other are listed as risk factors)
What is the most common complication of cholelithiasis?
Acute Cholecystitis (inflammation/infection of GB; 95% calculous)
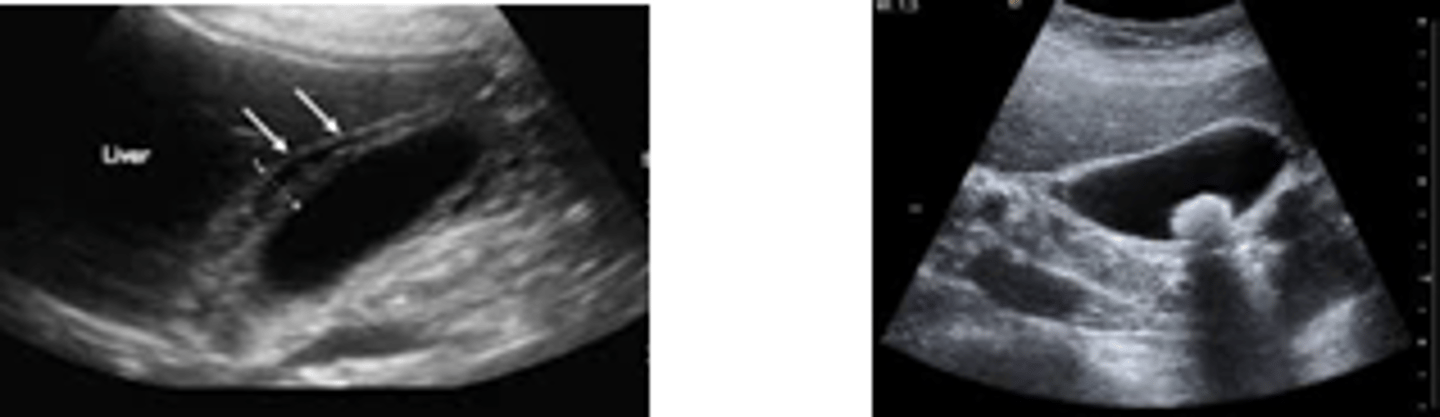
Female complains of constant RUQ pain with accompanying nausea and vomiting. Vitals reveal temp of 100.4+ and HR >100. Murphy's sign is positive. Work up?
Labs: CBC, BMP, LFTs, Lactic Acid
Imaging: US (study of choice)
(Dx = Acute Cholecystitis)
What on US indicates Acute Cholecystitis?
Wall thickening, edema, gallstones, pericholecystic fluid (highly sensitive and specific)
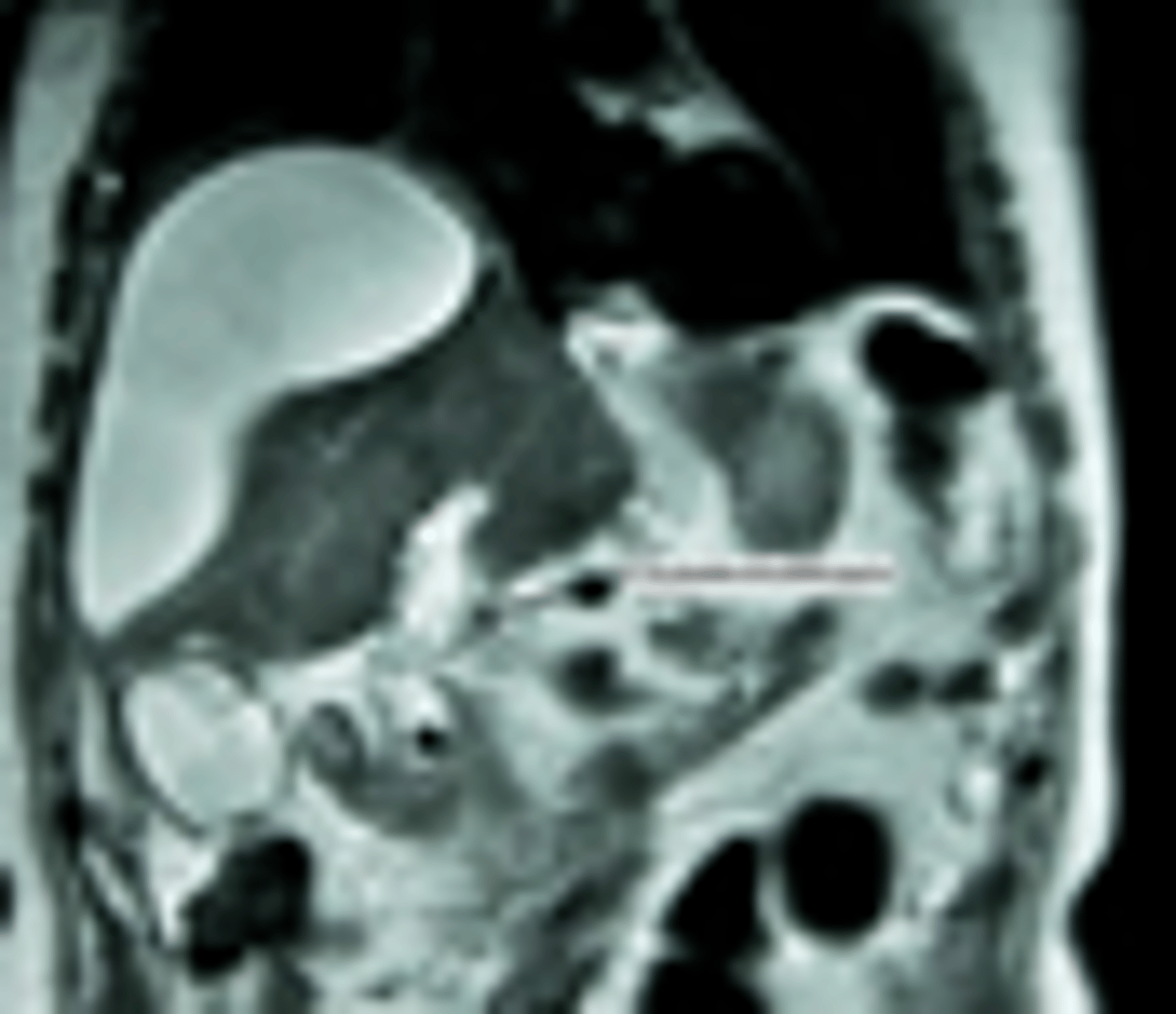
What imaging study for Acute Cholecystitis is used when there is a concern for a ductal obstruction (biliary colic AND elevated transaminase/BR)
MRCP
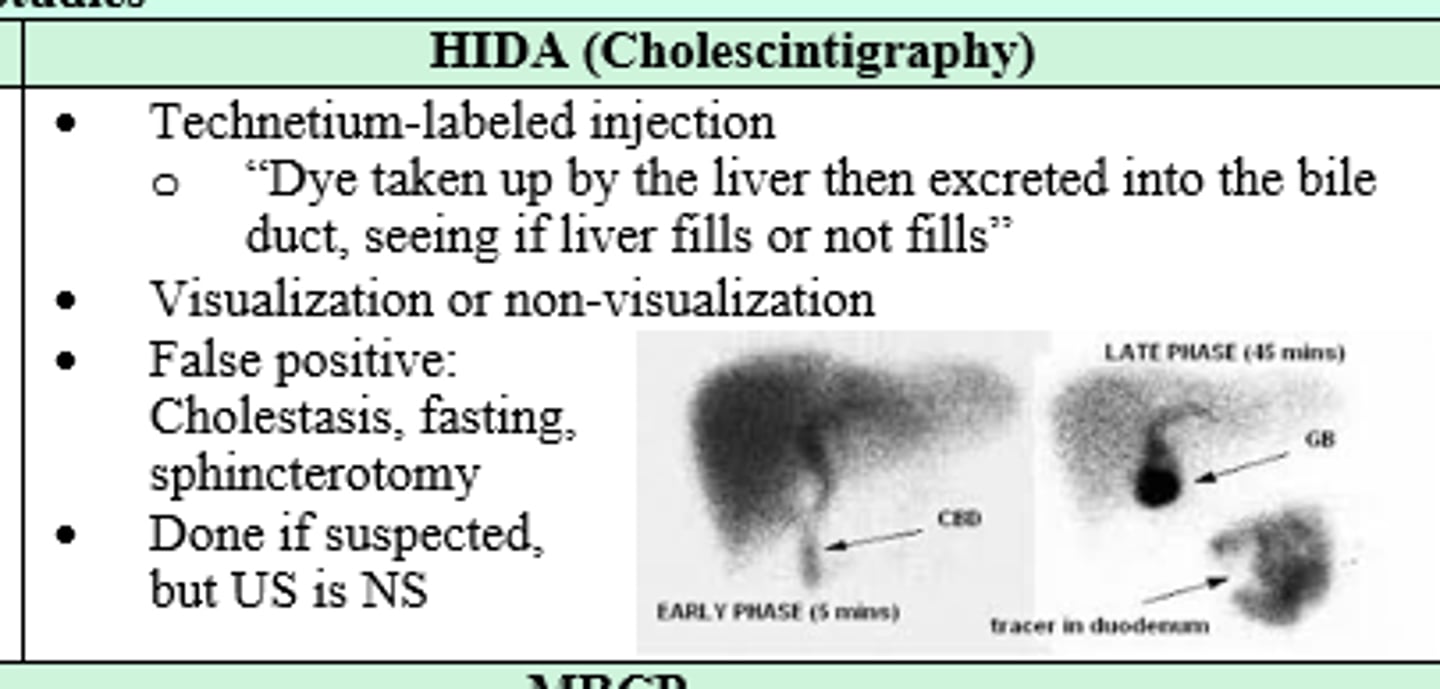
You suspect your patient has Acute Cholecystitis, but US is nonspecific. Next imaging modality?
HIDA (Cholescintigraphy)
Treatment of choice for acute cholecystitis?
Laparoscopic Cholecystectomy (within 72h onset)
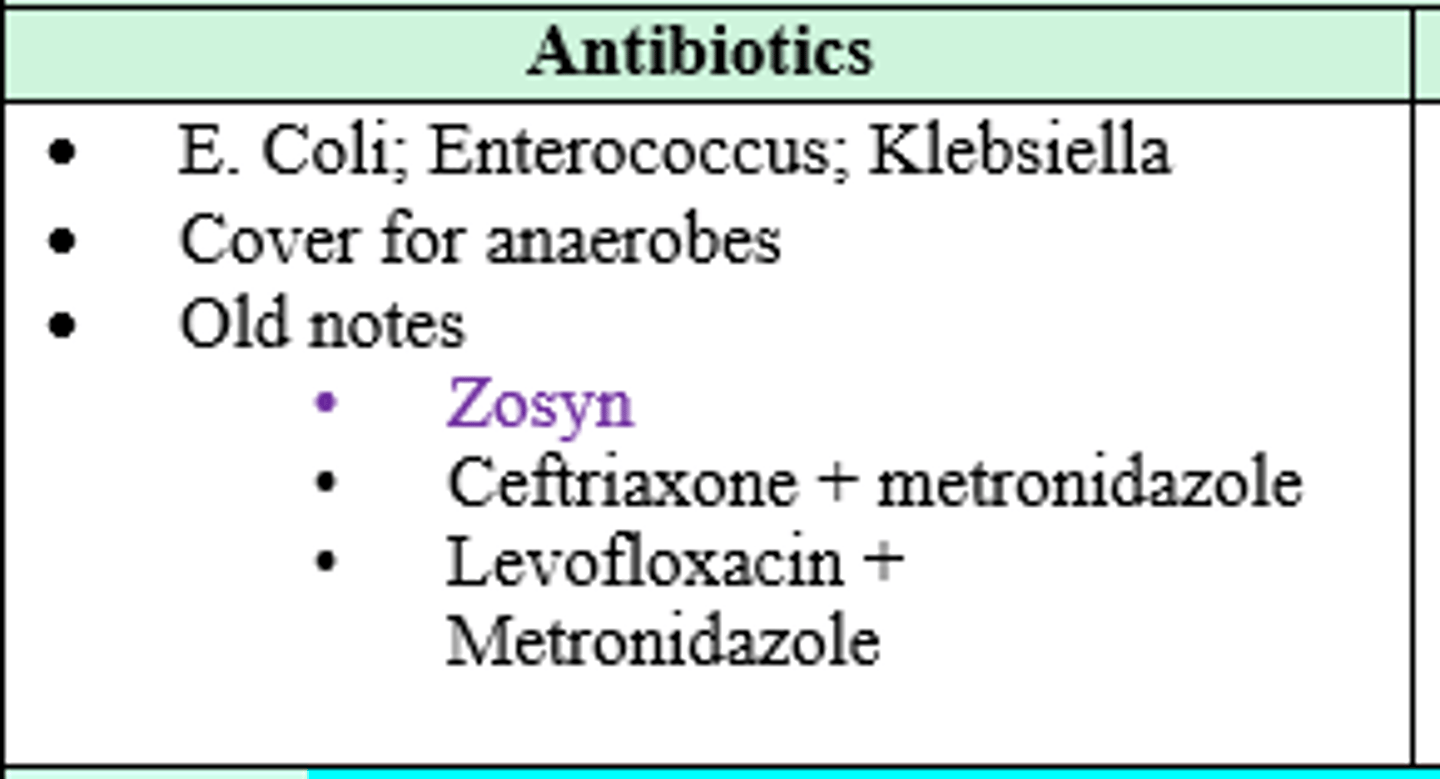
What organisms should you cover for in a pt with acute cholecystitis?
E Coli, Enterococcus, Klebsiella, and anaerobes
(Zosyn, Ceft + Metro, Levo + Metro)
Patient was undergoing a laparoscopic cholecystectomy, but the GB had an obstructed view dt inflammation and gangrene. In order to avoid bile duct injury, what should be done?
Switch to open cholecystectomy
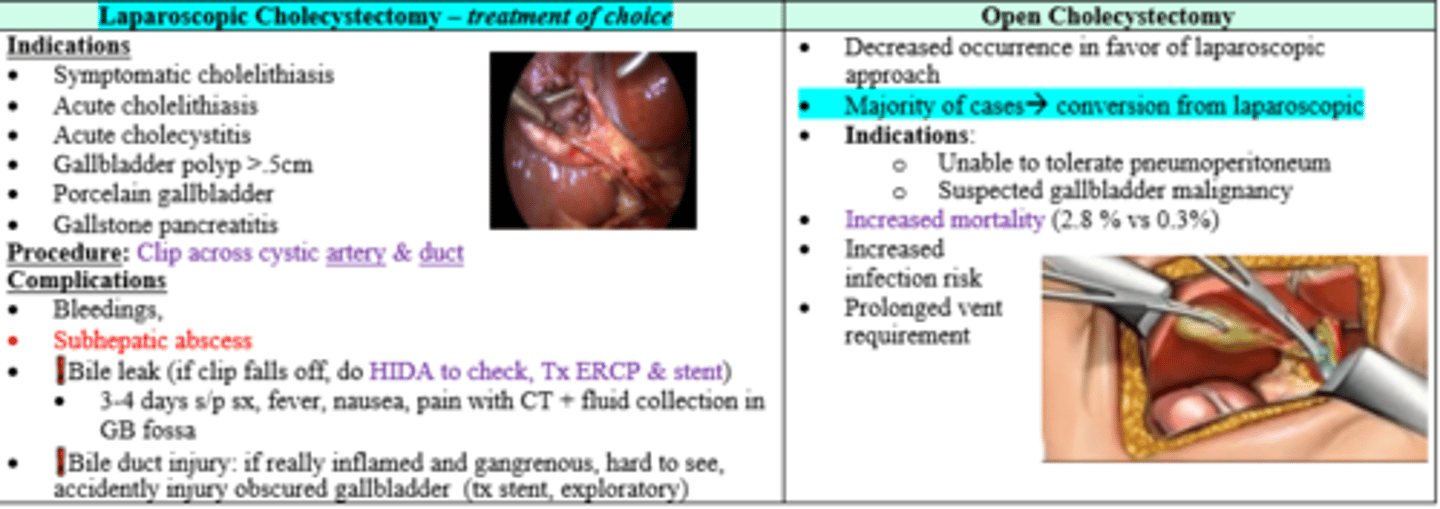
3-4 days after placing a clip across cystic artery and duct patient develops fever, nausea, and pain. CT is + for fluid collection in GB fossa. Dx and Tx?
Bile leak; HIDA to check, Tx with ERCP & Stent
What is the term for presence of gallstones in the common bile duct?
Choledocholithiasis
What might labs reveal in a patient with choledocholithiasis?
Transaminitis, Hyperbilirubinemia, elevated lipase, leukocytosis
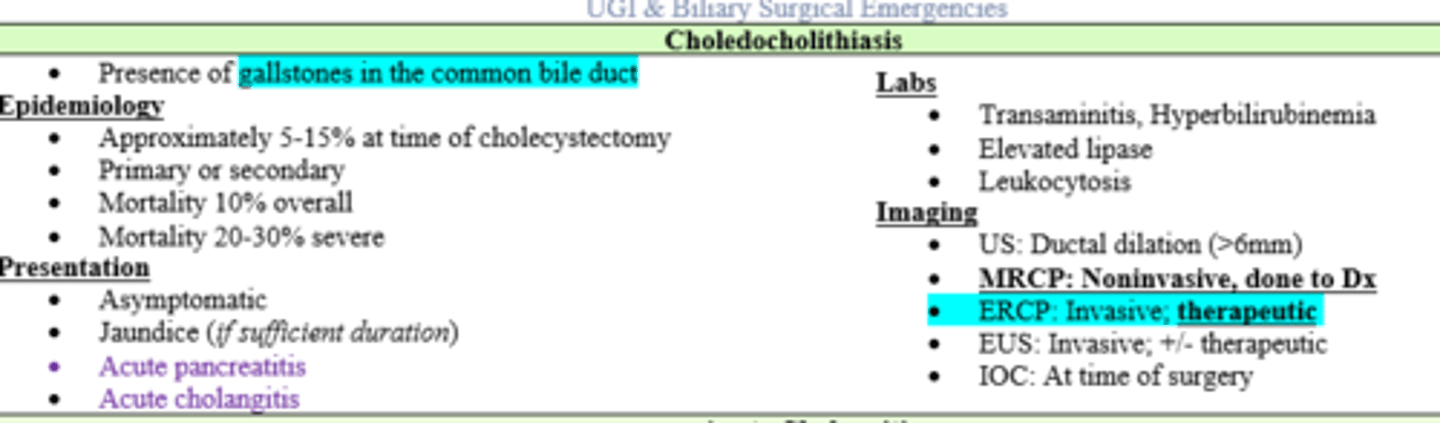
What imaging study for choledocholithiasis is invasive and therapeutic?
ERCP; EUS
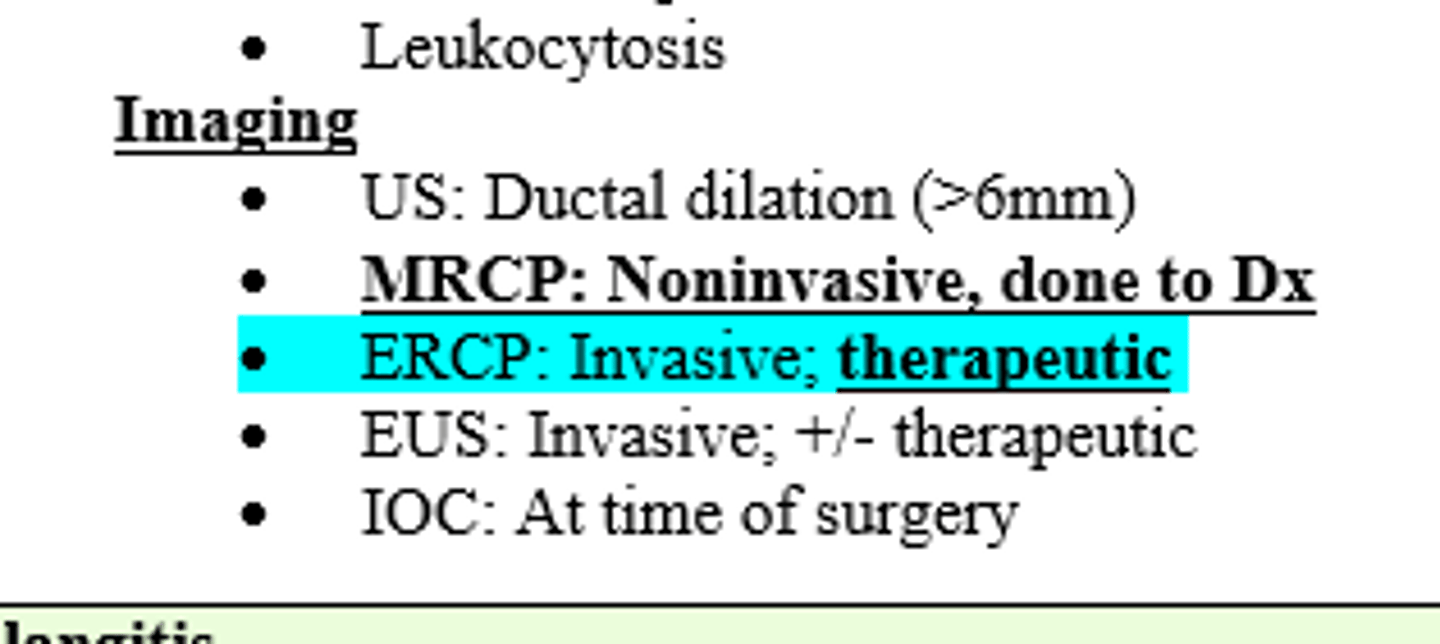
Ductal dilation of _____mm on Ultrasound in is indicative of choledocholithiasis
>6mm
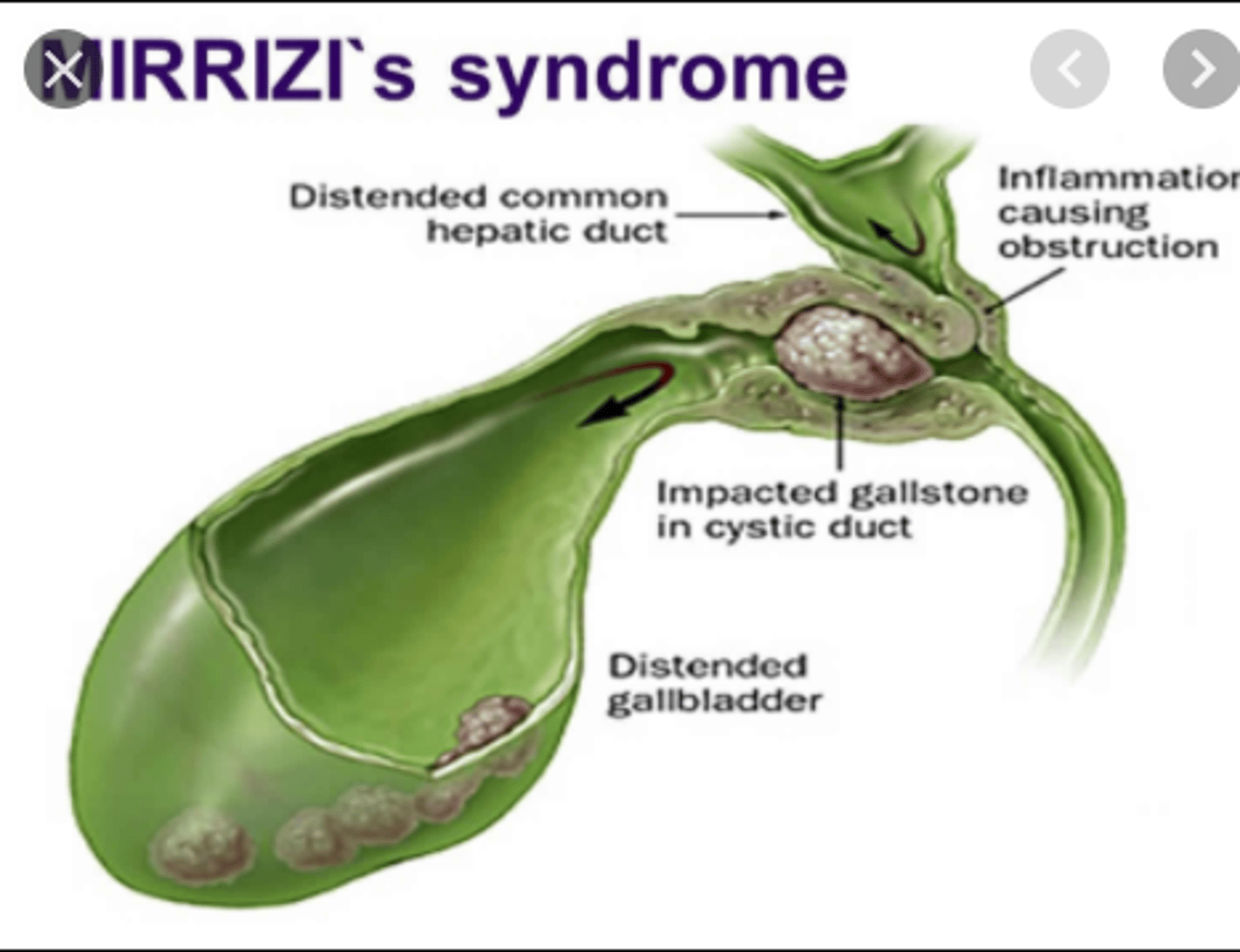
What is a less common etiology of Acute Cholangitis in which there is external compression of the common bile duct from a large stone that is threatening to erode through?
Mirizzi Syndrome
What is Charcot's Triad?
RUQ pain, fever, jaundice
(sx of Acute Cholangitis)
What is Reynold's Pentad?
Charcot's triad, hypotension, altered mental status
(sx of Acute Cholangitis)
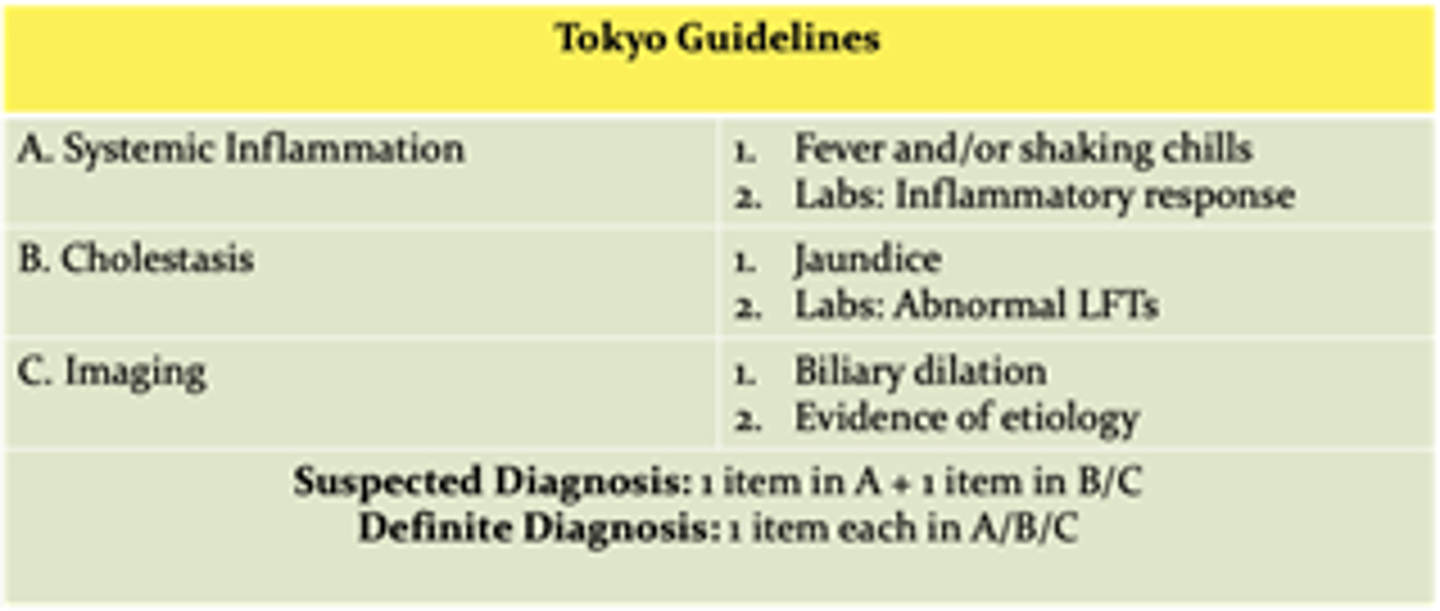
Which guidelines outline the degree of severity of Acute Cholangitis?
Tokyo Guidelines
(look at Systemic Inflammation, Cholestasis, and Imaging)
Patient c/o RUQ pain and confusion. PE reveals fever, scleral icterus, and BP 96/60. Labs are + for leukocytosis and hypoalbuminemia. US reveals biliary calculi. Treatment for suspected dx?
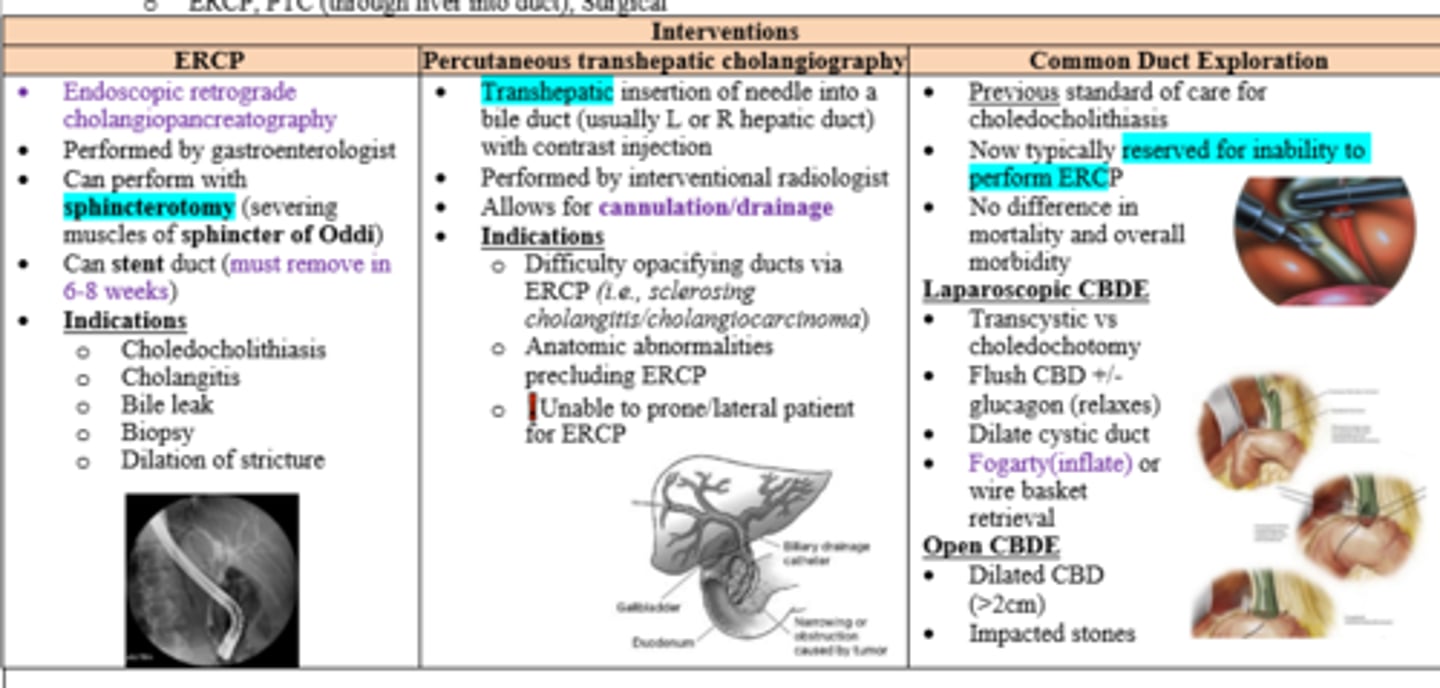
Hemodynamic support, Abx, and biliary drainage (ERCP, PTC, or surgery)
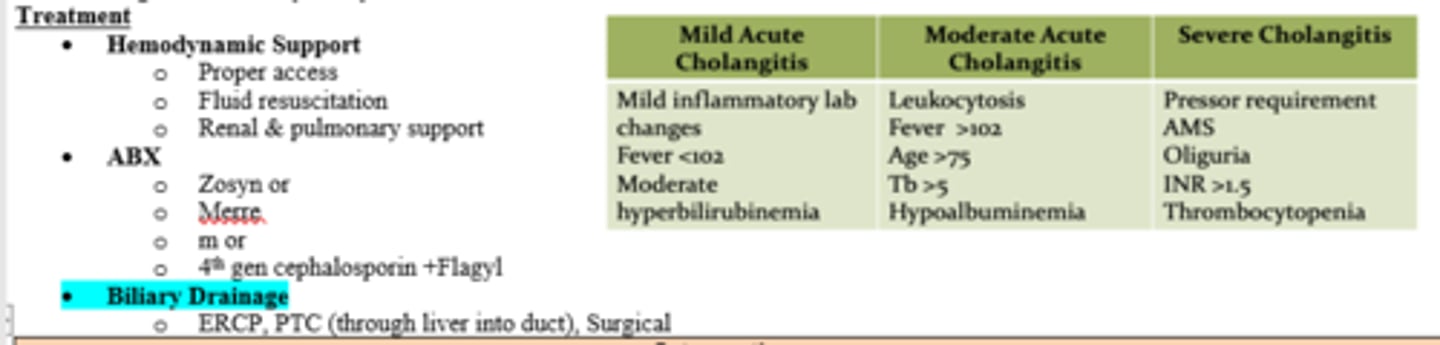
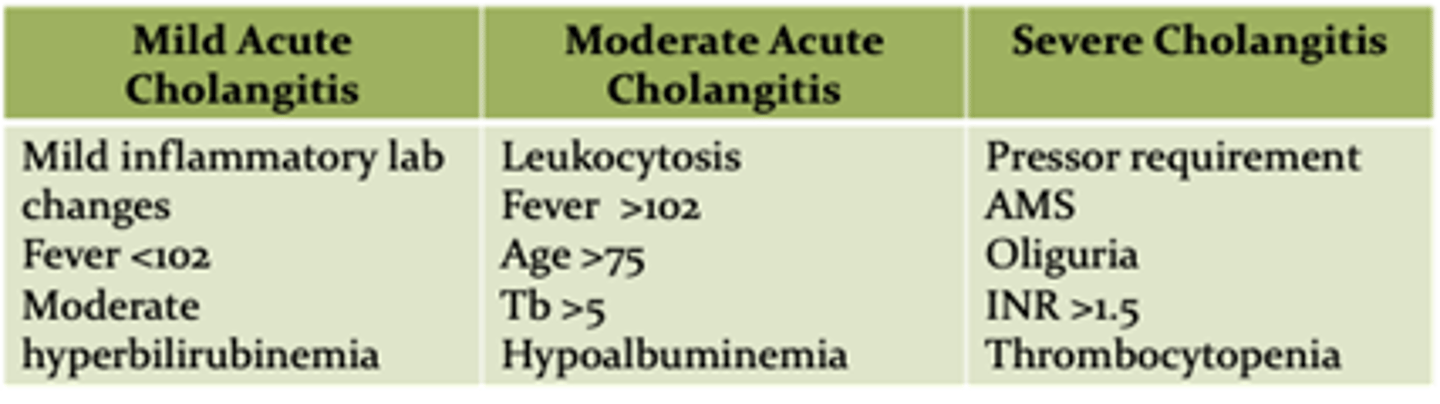
What factors are representative of severe cholangitis?
Pressor requirement
AMS
Oliguria
INR >1.5
Thrombocytopenia
Patient with acute cholangitis is unable to position either prone or lateral for ERCP. Intervention?
Percutaneous Transhepatic Cholangiography by IR