Sepsis and septic shock
1/42
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
43 Terms
what is sepsis
systematic illness caused by microbial invasion of normally sterile parts of the body
life-threatening organ dysfunction caused by dysregulated host response to infection
•Organ dysfunction can be identified as an acute change in total SOFA score >2 points consequent to the infection
•SOFA score >2 reflects an overall mortality risk of approximately 10% in a general hospital population with suspected infection
septic shock
sepsis with persisting hypotension requiring vasopressors to maintain MAP >65mmHg and having a serum lactate of >2mmol/l despite adequate volume resuscitation
SIRS
temp >38C or <36C
HR >90
RR>20 or PaCO2 <32
WBCs > 12,00 or <4,000 or >10% bands
what do they use in intensive care for sepsis
SOFA
sequential organ failure assessment score
qSOFA
hypotension - systolic BP < 100mmHg
altered mental status
tachypnea, RR>22/min
-score of >2 suggests greater risk of a poor outcome
what do you use for patients with suspected infection who are likely to have a prolonged ICU stay or die in the hospital
qSOFA
body’s physical barrier against sepsis
skin
mucosa
epithelial lining
body’s innate immune system against sepsis
Iga in GI tract, dendritic cells/macrophages
adaptive immune system against sepsis
lymphocytes
immunoglobulins
how does sepsis originate
breach of integrity of host barrier, physical or immunological
organisms enter the bloodstream creating a septic state
pathophysiology of sepsis and 3 phases in the pathogenesis of sepsis
uncontrolled inflammatory response
release of bacterial toxins
release of mediators
effects of specific excessive mediators
patients with sepsis have features consistent with what?
immunosuppression
•Loss of delayed hypersensitivity
•Inability to clear infection
•Predisposition to nosocomial infection
how does sepsis syndrome change over time
initially increase in inflammatory mediators
Later, there is a shift toward an anti-inflammatory immunosuppressive phase
what are the two types of toxins released
endotoxins
exotoxins
release of bacterial toxins
•Bacterial invasion into body tissues is a source of dangerous toxins
•May or may not be neutralised and cleared by existing immune system
commonly released toxins
Gram negative
•Lipopolysaccharide (LPS)
Gram positive
-Microbial-associated molecular pattern (MAMP)
•Lipoteichoic acid
•Muramyl dipeptides
-Superantigens
•Staphylococcal toxic shock syndrome toxin (TSST)
•Streptococcal exotoxins
release of mediators in response to infection
•Effects of infections due to endotoxin release
•Effects of infections due to exotoxin release
•Mediator role on sepsis
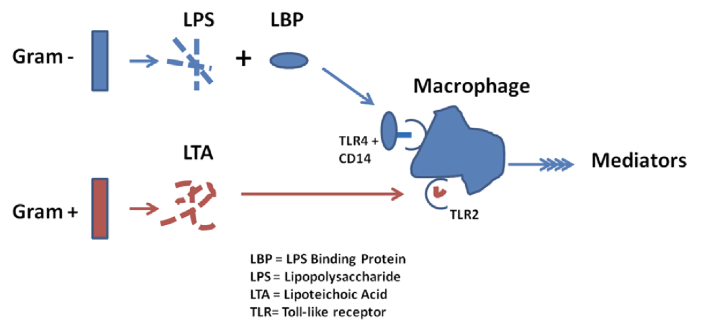
endotoxin release
LPS needs an LPS-binding protein to bind to macrophages
LTA binds to macrophages and taken up by toll-like receptors
-both release mediators from macrophage
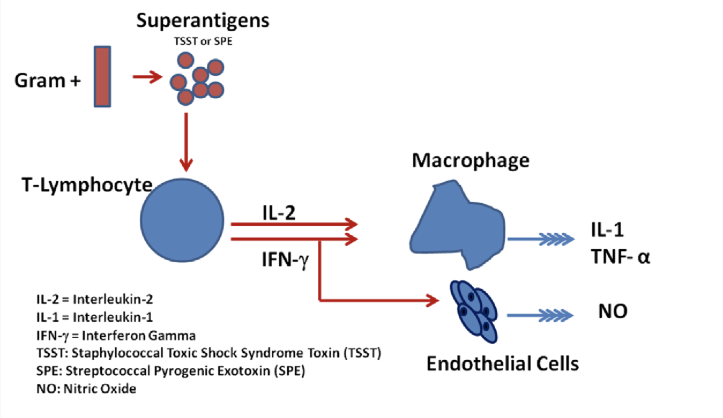
exotoxin release
Pro-inflammatory response
Small amounts of superantigens will cause a large amount of mediators to be secreted: cascade effect
pro inflammatory mediators
causes inflammatory response that characterises sepsis
Th1
compensatory anti inflammatory reaction
can cause immunoparalysis
Th2
effects of specific excessive mediators - pro-inflammatory mediators
•Promote endothelial cell – leukocyte adhesion
•Release of arachidonic acid metabolites
•Complement activation
•Vasodilatation of blood vessels by NO
•Increase coagulation by release of tissue factors and membrane coagulants
•Cause hyperthermia
effects of specific excessive mediators - anti-inflammatory mediators
•Inhibit TNF alpha
•Augment acute phase reaction
•Inhibit activation of coagulation system
•Provide negative feedback mechanisms to pro-inflammatory mediators
if compensatory anti-inflammatory > pro-inflammatory
septic shock with multiorgan failure and death
-need balance
if pro-inflammatory > compensatory anti-inflammatory
immunoparalysis with uncontrolled infection and multiorgan failure
-need balance
general features of sepsis
•Fever >38oC – presenting as chills, rigors, flushes, cold sweats, night sweats, etc
•Hypothermia <36oC – especially in the elderly and very young children (remember the immunosuppressed)
•Tachycardia >90 beats/min
•Tachypnoea >20 /min
•Altered mental status – especially in the elderly
•Hyperglycaemia >8mmol/l in the absence of diabetes
inflammatory variables in sepsis
•Leucocytosis (WCC > 12,000/ml)
•Leucopenia (WCC < 4,000/ml)
•Normal WCC with greater than 10% immature forms
•High CRP
•High procalcitonin
haemodynamic variables in sepsis
•Arterial hypotension (systolic <90mmHg or MAP <70mmHg)
•SvO2 >70%
organ dysfunction variables in sepsis
•Arterial hypoxaemia (PaO2/FiO2 < 50mmHg)
•Oliguria (<0.5ml/kg/h)
•Creatinine increase compared to baseline
•Coagulation abnormalities (PT >1.5 or APTT >60s)
•Ileus
•Thrombocytopenia (<150,000/ml)
•Hyperbilirubinaemia
tissue perfusion variables in sepsis
•High lactate
•Skin mottling and reduced capillary perfusion
effect of host on sepsis presentation
Age
Co-morbidities (COPD, DM, CCF, CRF, disseminated malignancy)
Immunosuppression
•Acquired – HIV/AIDS
•Drug-induced – steroids, chemotherapeutic agents, biologics
•Congenital – agammaglobulinaemia, phagocytic defects, defects in terminal complement component
Previous surgery - splenectomy
effect of organism on presentation of sepsis
•Gram positive versus Gram negative
•Virulence factors (example: MRSA, toxin secretion, ESBL, KPC, NDM-1)
•Bioburden
effect of environment on presentation of sepsis
occupation
travel
hospitilisation
sepsis 6
take 3
blood cultures
blood lactate
measure urine output
give 3
oxygen aim sats 94-98%
IV antibiotics
IV fluid challenge
OR
2As, 2Bs, 2Cs
Air enriched with O2
Antibiotics after blood culture
Blood culture
Blood gas with lactate
Crystalloid bolus
Catheter (urinary) if severe sepsis or septic shock
what is the use of blood cultures
makes microbiological diagnosis
what is the purpose of lactate
marker of generalised hypoperfusion/severe sepsis/poorer prognosis
what is the purpose of low urine output
marker of renal dysfunction
what to consider when giving antibiotics
allergy
previous MRSA, ESBL, CPE
antibiotic toxicity/interactions
lactate type A
hypoperfusion
lactate type B
mitochondrial toxins
alcohol
malignancy
metabolism erros
IV fluids
30ml/kg fluid challenge
2.1L 70kg patients
when to consider high dependency unit referral
•Low BP responsive to fluids
•Lactate >2 despite fluid resuscitation
•Elevated creatinine
•Oliguria
•Liver dysfunction, Bil, PT, Plt
•Bilateral infiltrates, hypoxaemia
when to consider intensive therapy unit
•Septic shock
•Multi-organ failure
•Requires sedation, intubation and ventilation