Power point review NR 511
1/99
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
100 Terms
actinic keratosis
a precancerous skin growth that occurs on sun-damaged skin; flesh colored, hard, sand-paper like; precancerous lesion that can progress into a squamous cell carcinoma

Based on presentation
actinic keratosis diagnosis
Cryotherapy
actinic keratosis treatment
sun exposed skin
who is at risk for actinic keratosis
dermatologist
actinic keratosis referal
fungal skin infections
Skin infections that live on dead outer surface or epidermis; popular rash, satellite lesions; not likely to develop into anything; no referral needed
treatment of fungal infections
•antifungal cream, pill; keep area as dry as possible; favors moisture, warmth and poor air circulation (consider the location of the rash)
At risk for fungal infections
Can be opportunistic (immunocompromised patients); look at patient's age; older, younger (could be diaper rash); diabetics, antibiotic therapy
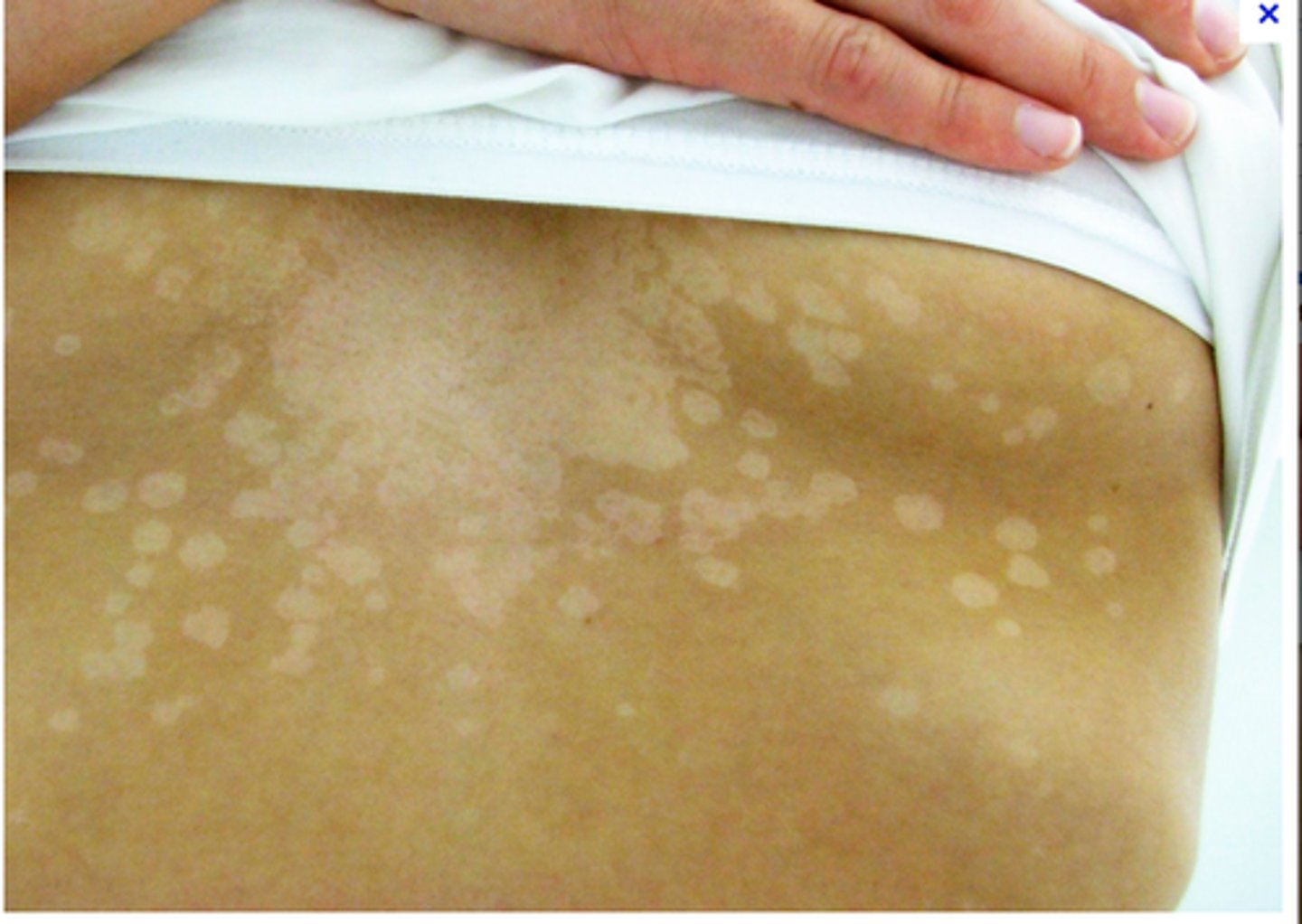
Tinea Vesicolor
fungal infection of skin caused by yeast, treated with topical selenium sulfide, topical antifungals; flat to slightly elevated brown papules and palques that scale when they are rubbed along with areas of hypopigmentation; puritis; most commonly found on trunk and shoulders
balanitis
inflammation of the skin covering the glans penis; candidiasis

Tinea Coporis
ringworm of the body; annal lesions with scaly boarders and central clearing on the trunk

Tinea pedis
athlete's foot; on the feet and between the toes

Tinea cruis
known as Jock itch. it is found in the groin area
brownish-red lesions in groin area, pruritus, skin excoriation

Cellulitis
diffuse, acute infection of the skin marked by local heat, redness, pain, and swelling; without sharp demarcated border; is a spreading infection of the epidermis and subcutaneous tissue that usually begins after a break in the skin

folliculitis
inflammation of the hair follicles; bacterial infection of the hair follicle; papules are characteristic of folliculitis

Erythema infectiosum
A viral disease characterized by a face that appears as "slapped cheeks," a fiery red rash on the cheeks. •Sore throat, slight fever, upset stomach, headache, fatigue, and itching are among other symptoms. Usually resolves on its own. Viral

Varicella rash
The rash starts on the trunk and spreads to the extremities and head. Each lesion progresses from an erythematous macule to papule to vesicle to pustule, and then crusts over. Lesions at various stages of development are seen in the same area of the body. There is usually a mild fever. The disease is self-limited, lasting about 1 week. is contagious 48 hours before the onset of the vesicular rash, during the rash formation and during the several days it takes the vesicles to dry up; characteristic rash appears 2-3 weeks after exposure. Viral

Warts
are growths on your skin caused by an infection with human papilloma virus, or HPV; caused by the human papillomavirus; most warts recur despite treatment. Contrary to popular opinion, warts do not have roots; the underside of a wart is smooth and round. Abrading the skin can spread the virus; vigorous rubbing, shaving, and nail biting, can do the same

Pityriasis rosea
is a common, self-limiting, usually asymptomatic eruption with a distinct initial lesion. This "herald patch," which appears suddenly and without symptoms, usually is on the chest or back. Secondary lesions appear 1 to 2 weeks later while the herald patch remains. The collarette scaling is another classic symptom. The lesions usually resolve spontaneously in 4 to 12 weeks without scarring. Outbreaks have been known to occur in close quarters like military barracks and dormitories.

hives
Red, itchy, possibly raised blotches on the skin that often result from allergic reactions; Look at the location of the rash; the first step is to determine the need for epinephrine; Look for respiratory symptoms, difficulty breathing, hoarseness; look at location of rash; is it on the neck, around the face, etc.; if it is, epinephrine must be administered

Cholinergic urticaria
Hives . Onset following emotional stain, intense exercise, perspiration, staying in hot environment, or intake of high calorie food. Lesions are wheal with itching, affecting any part of the body. Severe cases include headache, abdominal pain, diarrhea, or shock. Lesions disappear within 1-2 hours, but can relapse for months or years. are hives or wheals that are pruritic and occur on the trunk and arms following exercise, anxiety, elevated body temperature, hot baths and showers.
Hives and cholinergic
skin inflammation: urticaria
antihistamines
Hives and cholinergic treatment
history taking is important
Hives and cholinergic interview importance
Poison Ivy
Anacardiaceae Toxicodendron radicans; a form of contact dermatitis, is not contagious and it cannot be spread from one area of the body to another by touching it
latex sensitivity and poison ivy
Skin inflammation: contact dermatitis and
Keratosis pilaris
Redness and bumpiness common on the cheeks or upper arms; it is caused by blocked hair follicles. The patches of irritation are accompanied by a rough texture and small pinpoint white milia. mildly pruritic that looks like "gooseflesh."; the rash appears as small, pinpoint, follicular papules on a mildly erythematous base. Is a benign condition that resolves by adulthood

Atopic triad
asthma, eczema and allergic rhinitis
RAST
may be done to identify antigen-specific mast cell activation or to quantify levels of antigen-specific IgE; usually available to primary-care practitioners, whereas scratch testing is typically done only by board-certified allergists. However, interpretation of this results requires specialized knowledge of the specificity and sensitivity of the assay because false positives are not uncommon; should not be used as a general atopic screening tool; panels include antigen-specific IgE levels but also contain antigen-specific IgG and IgM levels, which are not helpful in the diagnosis of atopic disease and are therefore prone to misinterpretation
Atopic dermatitis
Consider an allergy; atopic triad; RAST test
hair loss
Alopecia areata; Trichotillomania; Minoxidil (Rogaine)
Alopecia areata
systemic cause of alopecia; nonscarring hair loss of rapid onset, the pattern of which is most commonly sharply defined round or oval patches
Trichotillomania
Non-scarring, non-systemic causes of alopecia include trichotillomania, trauma, bacterial or local fungal infections, and radiation to the head
Minoxidil (Rogaine)
a vasodilator and may stimulate vertex hair growth.
pediculosis
infestation with lice; Parasitic infection; Client education is essential when treating; be informed that itching may continue for up to a week after successful treatment because of the slow resolution of the inflammatory reaction caused by the lice infestation.

otitis externa
tenderness on traction of the pinna and/or pain on applying pressure over the tragus. There is typically an erythematous ear canal, and usually a history of recent swimming. Using ear drops made of a solution of equal parts alcohol and vinegar in each ear after swimming is effective in drying the ear canal and maintaining an acidic environment, therefore preventing a favorable medium for the growth of bacteria, the cause of swimmer's ear.
otitis media
•Diagnosis of acute otitis media is made by otoscopic examination. The tympanic membrane will appear red and bulging with or without visible effusion. Light reflex is usually diminished or absent. Mobility is decreased (not increased). The external auditory canal is red and erythematous in AOE the treatment of choice for AOM for otherwise healthy children who attend daycare or received antibiotics within the last month is Amoxicillin 80-90mg/kg/day

otitis media with effusion
change in the hearing threshold greater than 25 dB and has notable speech and language delays, more aggressive treatment is indicated. When the child's hearing examination reveals a change in the hearing threshold, it is extremely important that the provider evaluate the child's achievement of developmental milestones in speech and language. Any abnormal findings warrant referral.
Sensorineural loss
comes from exposure to loud noises, inner ear infections, tumors, congenital and familial disorders, and aging. Sensorineural loss comes from exposure to loud noises, inner ear infections, tumors (acoustic neuromas), congenital and familial disorders, Meniere's disease, medications, trauma, certain diseases and aging
Conductive hearing loss: Presbycusis
In conductive hearing loss, bone conduction is greater than air conduction, so the patient will report the bone conduction sound longer than the air conduction sound. Serous otitis media can result in conductive hearing loss
weber test
vibrating tuning forkl is placed on the top of the head equidistant from the patient's ears. In the normal patient, the Weber tuning fork sound is heard equally loud in both ears. In a patient with conductive hearing loss the Weber tuning fork sound is hear louder in "bad" ear. In sensorineural hearing loss, the tuning fork is heard louder in the "good" ear.
•Meniere's disease
triad of symptoms associated with Meniere's disease include progressive hearing loss, tinnitus and vertigo
Skin vesicles (if present) and a corneal infection with a "dendrite"
hallmark characteristics of HSV-1 or HSV-2 conjunctivitis
adenovirus
The causative organism of viral conjunctivitis; •It can present with or without cold symptoms. Patients complaint of itchy, red eyes and may have clear to no discharge. Preauricular lymph node swelling and tenderness is hallmark for viral conjunctivitis.
Blepharitis
an inflammation around the eyelid margins that is caused by staphylococcal infection at the lash base and dysfunctional Meiobian glands
Meniere's disease risk factors
Age of onset 30-60; most cases develop in 50's. Rare in young children and adults >70 years. White Americans of European descent at increased risk. Equally affects men/women. Stress, allergies; high sodium, caffeine, alcohol intake; hormonal changes; changes in barometric pressure; exposure to high noise levels for many years.
Inflammatory response of inner ear from insults (blunt trauma, viral infections, allergies, reduced or negative middle ear pressure). Familial history. History of migraines, autoimmune conditions (systemic lupus erythematosus), RA, certain thyroid disorders.
Meniere's disease subjective
Recurrent tinnitus, vertigo, and progressive low-frequency hearing loss or complete hearing loss in severe cases. Acute episode last anywhere from 20min-3hrs. Attacks rarely last > 4 hrs. Characterized as sudden attacks of nausea, emesis, pallor, diaphoresis, dizziness (spatial disorientation), vertigo, roaring tinnitus, increased pressure, fullness, and hearing loss in affected ear. Rapid movement aggravates symptoms, and possible report of falls or accidents during episodes. Frequency and severity may decrease over time with hearing improvement post attack, but some episodes may last 24 hours.
Meniere's disease objective
No apparent abnormalities on otoscopic exam unless otitis media present. Dilation of inner ear endolymphatic system present on autopsy. Spontaneous nystagmus is observed after preventing eye fixation by having pt wear 40 diopter glasses (Frenzel Lenses). Is a diagnosis of exclusion; numerous disorders mimic this disease.
Ménière's disease diagnosis
Careful history, neurologic assessment, and response to empiric therapy. Weber and RInne show sensorineural hearing loss; diagnostic criteria involves 2 episodes of vertigo lasting 20 minutes along with sensorineural hearing loss and either tinnitus or a perception of aural fullness. Audiometry shows low-frequency hearing loss and impaired speech discrimintation. Cold and warm caloric responses are typically reduced in the affected ear, as demonstrated by electronystagmography or direct patient observation (while wearing 40-diopter Frenzel lenses); the direction of the fast phase of nystagmus is variable. These findings are not diagnostic.
Meniere's disease treatment
1st, r/o other cause of symptoms. No proven cure; palliative tx given for reducing symptoms. Acute attacks treated with rest by closing eyes and protection from falling. Vestibular rehab reduces symptoms of unilateral peripheral vestibular dysfunction. Meds: Vestibular sedatives like prochlorperazine for severe n/v; a antihistamine like betahistine to reduce frequency and severity of vertigo attacks. Intratympanic dexamethasone used in pts refractory to lifestyle changes. Last resort: Aminoglycosides like streptomycin or gentamicin ablation therapy to reduce unbearable vestibular symptoms.
Meniere's disease education
Education on reducing sodium 1g/day, caffeine, and alcohol intake; stop smoking. Manage stress levels. Avoid all ototoxic drugs and polypharmacy. Return if further symptoms worsen or acute episodes increase in frequency. Acute attacks best managed by quiet bedrest and prevention of falls - not medicine. Reduce food intake during episodes to avoid n/v.
Actinic keratosis risk factors
Most common precancerous skin lesion in light skinned patients, more common in patients 50 years or older (most common in Celtic, Irish, and Scottish descent); Found in sun exposed areas; Caused by skin cells that accumulate from repeated sun exposure Continued sun damage from UV radiation damages the DNA in epithelial cells Primary lesions: macules or plaques, poorly circumscribed
Secondary lesion: erythematous and scaly
May feel like sandpaper when touched ; Not an aggressive form of cancer if/when it changes to squamous cell unless on the lip
actinic keratosis subjective
Patient complains of irritated, rough or scaly rash, pruritus, tenderness or stinging sensation
actinic keratosis objective
Reddened, scaly, rough, or uneven surfaces. Hard or spiny lesion. Sandpaper like texture. Flesh-colored; irregular.
actinic keratosis diagnosis
Fluorescence using photosensitizing drug (methyl ester of 5-aminolevulinic acid) over area of concern will have a pink fluorescence with the wood's lamp
actinic keratosis treatment
No evidence to support removal of lesion as most will not turn cancerous however it is standard to REMOVE the lesion(s) Topical Therapy:
5-fluorouracil (5-FU) cream (Efudex, Carac) applied in a thin layer over the lesion BID for 3 weeks, avoid eyelids, lips, and folds of the nose. This treatment causes red, raw, and painful skin in the areas applied which may lead to noncompliance. Exposure to sunlight makes this worse Imiquimod 5% cream used for face and scalp lesions. Applied 3x weekly for 8 weeks. Diclofenac 3% in 2.5% hyaluranon gell (Solaraza) applied BIF for 60 to 90 days Adapalene 0.1%to 0.3% (topical retinoid)applied daily for 4 weeks and then increased to BID; Side effects of these treatments include redness, itching, rash, and dry skin; Topical chemotherapy combined with phototherapy with blue or red wavelength have better cosmetic results than cryosurgery. 2 day course; Cryosurgery tissue is destroyed by freezing using liquid nitrogen. Hypopigmentation may occur at site of previous lesion; Surgical curettage or shave excision are not considered first line treatments for actinic keratosis; Surgical biopsy is the only way to obtain an intact sample to be analyzed as a way to confirm diagnosis; If treatment does not work, no matter the choice always refer to dermatologist
actinic keratosis education
Centered around prevention, avoidance of excessive sun exposure, use of protective clothing, and use of sunscreen. Should teach patients ABCDE mnemonic; A= asymmetry B= border irregularity C= color change D= Diameter larger than a pencil eraser E= elevation from a flat lesion to a raised or evolving lesion
Tinea vesicolor risk factors
Common in summer time. Tinea versicolor obvious during summer, when tanning exposes hypopigmented macules that do not tan. Common in teens and young adults but can occur at any age.
Tinea vesicolor subjective
Become noticeable in summer, since the macules do not tan. Asymptomatic with gradual onset. Mild pruritus - rare. People of African descent complain of hypopigmented or hyperpigmented spots. Will complain of these macules to back, upper chest, arms, and sometimes neck and face.
tinea vesicolor objective
Macules that may be round or oval, pink or hypo or hyperpigmented. Asymptomatic. Not associated with pruritus. Will be seen mainly on back, chest, arms, and sometimes neck. In children, rash common on face or forehead. Sometimes very fine scales are visible, especially if patient has not showered or bathed for several days. Daily bathing usually eradicates the scales.
tinea vesicolor diagnosis
Fungal culture not required unless clinical is unsure of diagnosis or if infection not responsive to treatment. Caused by yeast P. orbiculare (which causes round lesions) or Pityrosporum ovale (which produces oval lesions);
tinea vesicolor treatment
Treated with selenium sulfide lotion (selsun) daily for 7 days from neck to waist with small amounts of water lathered and left for 10 minutes); repeated once a week for 1 month. Clotrimazole 1% cream and solution (Lotrimin) twice daily for 2-8 weeks; Terbinafine 1% solution (Lamisil solution) twice daily for 1 week. Education: Do not use on face or mucous membranes; avoid broken or irritated skin. Ciclopirox 0.77% cream, lotion (Loprox) twice daily for 2-4 weeks. Do not use in children younger than 10 years. Avoid occlusion. Ketoconazole 2% shampoo (Nizoral) 1 application applied to damp scalp, leave for 5 minutes and rinse ; Econazole 1% cream, foam (Spectazole) (Ecoza) once daily for 2 weeks
Sulconazole 1% cream, solution (Exelderm) 1-2 daily for 3 weeks; Oxiconazole cream, lotion (Oxistat) 1-2 times daily for 2 weeks; Fluconazole (diflucan) 150-300mg single weekly dose for 2-4 weeks of 300mg weekly for 2 weeks; Itraconazole 200mg daily for 7 days; Some success with photodynamic therapy
tinea vesicolor education
Treatment will eradicate infection but will not remove the hypopigmented spots from skin which take longer to resolve. Educate on high rate of recurrence because P. orbiculare (M. furfur) is a normal habitant of the skin. sunlight can speed up resolution of hypopigmented spots. High risk of hepatotoxicity with systemic (oral) antifungals and treatment does not prevent recurrence
Trichotillomania
a disorder characterized by the repeated pulling out of one's own hair
Trichotillomania risk factors
Seen more commonly in children and teens. Family hx, age, stress, depression, anxiety, obsessive-compulsive disorders (OCD).
Trichotillomania subjective
Reports balding, sense of pleasure with pulling hair, or pull hair without realizing it. Pull hair due to stress, anxiety, tension.
Trichotillomania objective
Reports balding, sense of pleasure with pulling hair, or pull hair without realizing it. Pull hair due to stress, anxiety, tension.
Trichotillomania diagnosis
observation
Trichotillomania treatment
Trichotillomania education
Refer to dermatologist or psychologist. An SSRI for 1st line treatment of OCD in children and adults. Cognitive behavior therapy is another option as a first line management for OCD.
varicella risk factors
Immune compromised such as AIDS and HIV
Risk -No prior history of varicella-No vaccination -Immunocompromised *Patients are contagious for 2 days prior the appearance of the rash and until all lesions have crusted.*infection in adults is more likely to produce serious illnesses
Varicella subjective
subjective -Malaise -Anorexia -Abdominal pain -Headache -fever/chills -arthralgia -Childhood: onset of exanthem; Then 1-2 days later, the urticarial (or itching) erythematous macules and papules appear, which quickly turn unto vesicles and pustules. Rash starts on the face and chest then spreads over the entire body. The blisters may even appear in the ear canal or mouth. Lesions dry up within 1 week.
varicella objective
Rash with widely distributed papules and vesicular lesions; appear on head and neck area
objective rash phase -small erythematous macules appear on the scalp, face, trunk and limbs with rapid progression within 12-24 hrs to papules, clear vesicles and pustules with central umbilication and form crusts. -vesicles appear on palms, soles, mucous membranes, oropharyngeal area and urogenital areas
varicella diagnosis
Diagnostic: none indicated unless in pregnant women -tzanck smear -vesicular fluid culture -serology -chest xray if pneumonia suspected -PCR
varicella treatment
Treatment is symptomatic care with oral antihistamines for itching, NSAIDS, cool compresses, and oatmeal baths. Valacyclovir (Valtrex ) 1 gm po q8h for 7 days or
Acyclovir (Zovirax) 800mg po 5 times a day for 7-10 days or; Famciclovir (Famvir) 500mg po TID for 7 days plus topical silver sulfadiazine for skin lesions. No evidence of fetal harm if used during pregnancy. treatment Non pharmacologic -Supportive therapy -good hygiene to prevent bacterial secondary infections -cut fingernails short to prevent scratching in younger children; -Tepid bath, oatmeal bath for itching Pharmacologic
Skin protectant such as calamine; antipyretics: avoid aspirin due to increased risk of Reye's syndrome with varicella patients -Antiviral agents: consider in adolescents, adults and high-risk patients to decrease viral shedding and duration of fever; Acyclovir (2-16 years old) 20mg /kg/dose (max 800 mg /dose, 4 times daily for 5 days
varicella education
education -Do not immunize pregnant women -In pregnant woman who has never had chicken pox or immunization, avoid contact with recently vaccinated individuals for 6 weeks; Prevention includes vaccination. A patient is contagious 2-3 days before rash erupts and may return to school, sports, or work after lesions have scabbed over. A client who has a varicella rash can return to work once all the vesicles are crusted over. Varicella is contagious 48 hours before the onset of the vesicular rash, during the rash formation (usually 4-5 days), and during the several days it takes the vesicles to dry up. The characteristic rash appears 2 to 3 weeks after exposure.
warts
are primarily caused by HPV serotypes 1 to 5, 7, 27, or 29, whereas HPV serotypes 3, 10, 28, and 29 cause flat warts. HPV serotypes 1 to 4, 27, 29, and 57 typically causes plantar warts, whereas HPV serotypes 6 and 11 cause anogenital warts.
warts risk factors
Skin trauma, contact with wart exudate after treatment, immunocompromosed state
warts subjective
Patients typically complain of a wart or small "bump" (or group of bumps) that has been present for several weeks to many months and sometimes for years. Some patients report the same wart being treated before and then recurring in the same area. Many adult patients with common warts attempt self-treatment with over-the-counter (OTC) wart remedies with limited to no success. Warts are usually asymptomatic but may be cosmetically undesirable. Plantar warts may cause discomfort with weight-bearing.
warts objective
Common wart: rough-surfaced, elevated, flesh-colored papules
warts diagnosis
None needed but if unable to distinguish lesions, small specimen can be sent for identification.
warts treatment
Salicylic acid solution/plasters; Cryotherapy with liquid nitrogen; Surgical excision; Studies suggest that one-half of warts resolve without treatment within 1 year, and two-thirds resolve within 2 years. Therefore, first-line therapy for new warts is watchful waiting with no treatment. Initial management for established warts should be geared toward relieving pain and pressure and minimizing skin trauma and scarring caused by available therapies. It is important to note that several treatments for warts are contraindicated in pregnant women; however, salicylic acid applied to a small area of the skin for a short duration and liquid nitrogen cryotherapy are considered safe during pregnancy.
Warts education
Avoid contact with wart exudate from self and others by covering wart; avoid skin trauma; Can cause scarring, autoinoculation, and nail deformity; The clinician should educate the patient on the prevention of self-inoculation and the routes of transmission for common warts. These measures include limiting shaving of the affected area until warts are eradicated, strategies to control nail biting, and avoidance of scratching and rubbing warts. Wearing protective foot coverings in wet public areas such as showers, locker rooms, and pools and keeping warts dry are additional approaches to prevent infection
Folliculitis
a superficial to deep skin infection of the hair follicles. Mainly caused by gram-positive bacteria, occasional by fungus or by gram-negative bacilli. Bacteria infect the hair follicle at a superficial level which leads to the clinical presentation of little pustules or erythema surrounding the base of the hair follicle.
Pseudomonas folliculitis
presents as follicular erythematous papules, pustules, or vesicles over the back, buttocks, and upper arms. Associated features include pruritus, malaise, low-grade fever, sore throat and eyes, and axillary lymphadenopathy. This type of folliculitis usually resolves spontaneously within 10 days.
shaving folliculitis
result of sebaceous follicles which are colonized by gram negative bacteria become infected due to trauma from shaving. "Hot tub" folliculitis is a form of folliculitis that is caused by pseudomonas aeruginosa, which can withstand temperatures of up to 107 degrees F and chlorine levels up to 3mg/L.
folliculitis risk factors
Common in middle-age (40-60) and children, especially if immunocompromised. Predisposing factors include diabetes, obesity, a chronic carrier of Staphylococci (present in the nares, axillae, or perineum), poor hygiene, hyperimmunoglobulin E (Job's syndrome, a primary immunodeficiency disorder), exposure to chemicals and solvents (cutting oils), and chronic skin friction. Wet environment, inadequate chlorinated pools. Those on long term, oral ABX like tetracycline for acne or rosacea or older men with seborrhea. Prolonged steroid users. At risk for Candida folliculitis due to antibiotic use which kills normal flora; May occur anywhere on skin as a result of trauma or damage to hair follicle from chronic irritation or friction
folliculitis subjective
Pt shaves, burrowed someone razor, or was recently in a hot tub. Complains of bumpy rash that can appear anywhere on the body. Rash located on hair follicles of face, forehead, back of earlobes, neck, shoulders, buttocks, torso, or extremities. Usually NOT accompanied by itching. No hx of previous skin eruptions or of pertinent hx of diabetes.
folliculitis objective
Lesions can range from minute white-topped pustules in newborns to large, yellow-white tender pustules in adults. NO involvement of surrounding skin. Eyelids, face, scalp, and extremities most common sites. A hair in the center of the pustule sometimes perforates the lesion. This presentation is a hallmark for diagnosis. Pustules resolve into red macules, which fade to leave post inflammatory hyperpigmented scars in susceptible persons. usually asymptomatic, but it can be very pruritic and is sometimes accompanied by burning; Check adjacent lymph nodes for spreading lymphadenitis.
folliculitis diagnosis
H&P; sampling pustule to identify pathogen for gram strain and culture to help differentiate folliculitis from other bacterial infections. Obtain KOH prep to see under microscope in office if a fungal infection is suspected
folliculitis treatment
Topic ABXs: mupirocin (Bactroban), Retapamulin (altabax), Clindamycin, Erythromycin. Antifungal for fungal - ketoconazole (Nizoral) may be in cream, shampoo, or tablet form With deeper forms of folliculitis, especially in the presence of positive blood cultures or systemic symptoms, an ER referral for hospitalization and IV antibiotics are recommended. Clearance of nasal colonization of Staph. Aureus by treatment with mupirocin intranasally BID x 5 days has been shown to significantly reduce the incidence of recurrent folliculitis. Eosinophilic folliculitis treated with anti-inflammatory agents. 1st-line is systemic indomethacin AND topical corticosteroids. Large pustular lesions with necrotic areas should first be cleansed with a weak soap solution, followed by soaking of (or the use of compresses on) the affected skin with saline or aluminum subacetate twice daily. When the skin is softened, the clinician can gently open the large pustules and trim away necrotic tissue.
folliculitis education
Gentle cleansing by washing the skin twice daily with an antibacterial soap. Hand-hygiene and good hygiene. Avoid shaving during treatment to allow healing. Electric shaver preferred once shaving is resumed. Avoid burrowing or using older razors when shaving infected areas. Avoid tight fitting cloths.
Pityriasis rosea risk factors
Affects people of both sexes; more common in females, and in 15-30 years age group although also seen commonly in elderly and children
Pityriasis rosea subjective
The eruption is usually preceded by a prodrome of sore throat, gastrointestinal disturbance, fever, upper respiratory tract infection, viral infection, and arthralgia. Rash can be itchy and patient may have a low-grade fever, headache, and fatigue.
Pityriasis rosea objective
1st a herald patch appears, typically on the trunk. The large lesion is commonly 2 to 10 cm in diameter, ovoid, erythematous, and slightly raised, with a typical collarette of scale at the margin. Collarette scaling is seen typically. 2-3 weeks later, a general rash appears. Resembles shape of Christmas tree on the trunk. Face, Palmar, and sole surfaces usually spared.
Pityriasis rosea diagnosis
H&P
Pityriasis rosea treatment
Management includes antihistamines, and unlike Fifth's disease the sun could help the rash instead of exacerbate the rash. Acyclovir for 1 week may decrease severity.
Pityriasis rosea education
Patients may be contagious 7-14 days prior to rash eruption ; Rash can possible last 1-2 months or even longer. Returning to activities will depend on the patient's symptoms, by the time the rash has appeared though, the patient is not contagious anymore.
contact dermatitis
A common condition categorized as either irritant dermatitis or allergic dermatitis. Allergic dermatitis is from immunologically mediated response and irritant dermatitis is the result of repeated insults to atopic skin by caustic or irritant substances
acute contact dermatitis
Erythema and edema
Clear, fluid filled vesicles or bullae ; Exudate, clear fluid
Distinct margins