BIPN 152 Midterm 3
1/50
Earn XP
Description and Tags
covers part of LE 9 - not all of LE 13, (no DI slides were posted), MB review session info(?), MB practice questions (posted in Canvas Inbox)
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
51 Terms
ALS stands for… (& another name for it) which is a __ __ disease
def. ALS
describe (1 w/ 2) (1)
age of onset is __ to __ years, but can occur in people younger and older than this range
it causes (2)
symptoms (4)
when symptoms begin in arms, is called __ onset; when first notice the mouth-related problems, is called __ onset
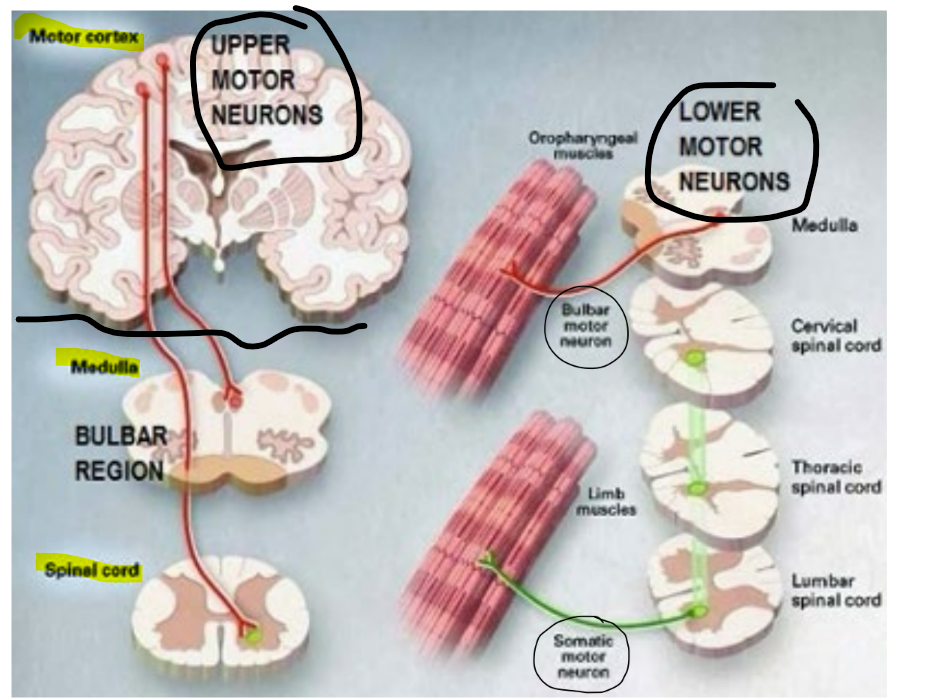
amyotrophic lateral sclerosis / Lou Gehrig’s disease, is a motor neuron disease
is a chronic neurodegenerative disease that attacks upper & lower motor neurons (aka motor neurons in the motor cortex of brain and spinal cord or brainstem)
where attack of lower motor neurons:
attack of somatic motor neurons in SC will impair muscle control (of limbs)
attack of bulbar motor neurons in brainstem will impair speech & swallowing (by impairing oropharyngeal muscles)
where attack of upper motor neurons will affect the motor cortex
__
onset is 40-60 years
causes loss of muscle control & eventual paralysis
muscles twitches & cramps
tight and stiff muscles (aka spasticity)
slurred and nasal speech
difficulty chewing or swallowing
when symptoms begin in arms, is called limb onset; when first notice the mouth-related problems, is called bulbar onset
for ALS
t/f: bulbar onset ALS typically shows a poorer prognosis/result of survival (aka faster progression towards death) compared to limb onset ALS
__
most cases of ALS are __, but some are __
…
for familial ALS, most identified mutations occur in which 4 genes/proteins?
which mutation of the 1 specific gene is focused on in class (b/c found in most ALS cases)?
approx. % found in sporadic vs. familial cases
describe (1)
how does it act/behave when it is a healthy vs. disease gene (1 / 1)?
what is interesting about this protein w/in disease genes?
___
although loss of normal protein function might contribute to ALS, the major factor that causes ALS and other neurodegenerative diseases is the (1), which is a __ __ of function
true
__
most cases of ALS are sporadic, but some are familial
…
for familial ALS, most identified mutations occur in the genes/proteins:
C9orf72
SOD1
FUS
TDP-43
TDP-43 mutation is found in most ALS cases
4% in familial, 1% in sporadic (where TDP-43 is likely made de novo)
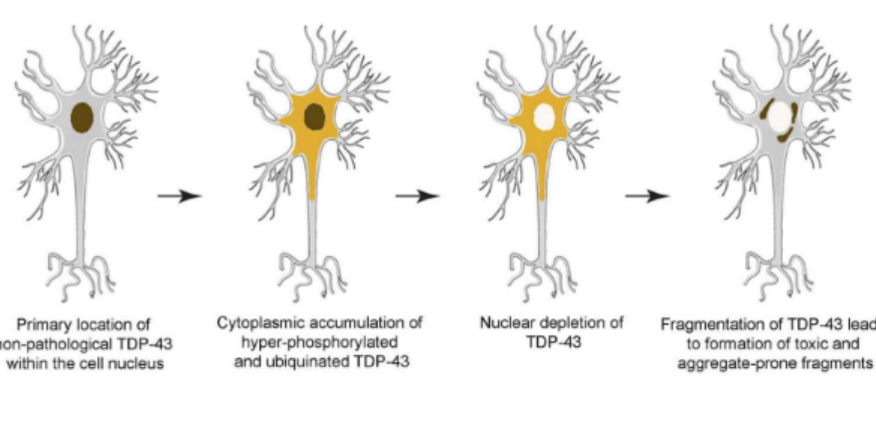
in ALS, TDP-43 gets mislocalized to the cytoplasm, instead of the nucleus which is where it normally is
in health gene: TDP-43 acts as a RNA binding protein used in RNA processing
(^ is the normal function, and TDP-43 aggregates would be in the nucleus NOT cytoplasm)
in disease gene: TDP-43 forms intracellular protein aggregates
(^ while is in cytoplasm b/c is a disease gene aka gene w/ TDP-43 mutation)
almost all patients have clumps/aggregates of TDP-43 in their motor neurons, including people who don’t have the TDP-43 mutation
___
although loss of normal protein function might contribute to ALS, the major factor that causes ALS and other neurodegenerative diseases is the aggregation of misfolded proteins, which is a toxic gain of function
remember that “aggregates” are accumulation/clumps of toxic misfolded proteins
def. LATE
__
t/f: LATE involves a different anatomical pattern/path for the spread of aggregate pathology compared to AD
explain how (1)
how will it affect normal vs. toxic function?
_
explain the hypothesis relating to spread and “seed” aggregates (1)
t/f: LATE dementia & ALS are different diseases, and are only related b/c they both involve TDP-43 pathology
is a type of dementia that involves the TDP-43 protein, NOT tau or amyloid
__
true
TDP-43 is mislocalized from the nucleus → to the cytoplasm (as hyperphosphorylated TDP-43)
…
loses normal function (aka loses function as a RNA binding protein)
gains a toxic function (aka TDP-43 will aggregate)
__
TDP-43 pathology first occurs in a small subset of neurons BUT will spread progressively to other neurons via releasing seed aggregates & uptake
true
LATE dementia & ALS are different diseases, and are only related b/c they both involve TDP-43 pathology
name 2 acute injuries to the brain
def. acute vs. neurodegenerative
stroke & TBI (traumatic brain injury)
^ are acute injuries to the brain, where:
acute injuries have sudden/fast onset
vs. neurodegenerative disease that are chronic, long-lasting/slow, and progressive
def. stroke
is one of the leading causes of (2)
symptoms of stroke (5)
which 1 symptom is more common in hemorrhagic strokes?
def. infarct
__
loss of blood flow to the brain will deprive the brain of (2), which will form the __ source called (1)
__
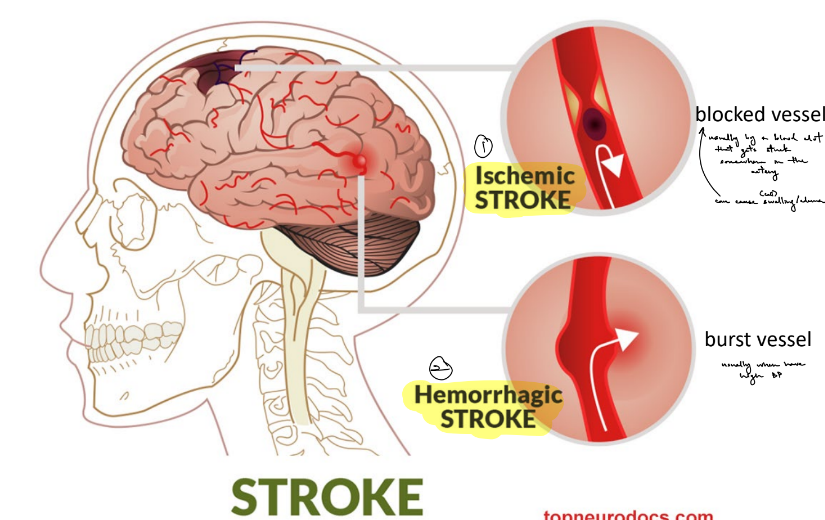
name the 2 types of stroke
def. each
state how each stroke usually occurs (1 each)
which type of stroke can cause swelling/edema? explain how ← but will also be explained in later flashcard
stroke — localized/focal loss of blood flow to the brain due to brain hemorrhage or vessel occlusion/blockage
is one of the leading causes of death & long-term disability
symptoms:
numbness or weakness of the face, arm, or leg ESPECIALLY unilaterally
trouble speaking or understanding words
vision problems
loss of balance & coordination
headache (more common in hemorrhagic strokes)
infarct — local area with dying or dead cell tissue, b/c lack of blood flow
__
loss of blood flow to the brain will deprive the brain of glucose & oxygen, which will form the energy source called ATP
____
ischemic stroke — localized loss of blood flow to the brain due to blocked blood vessel/vessel occlusion
usually due to blood clots that get stuck in the vessel
can cause swelling/edema
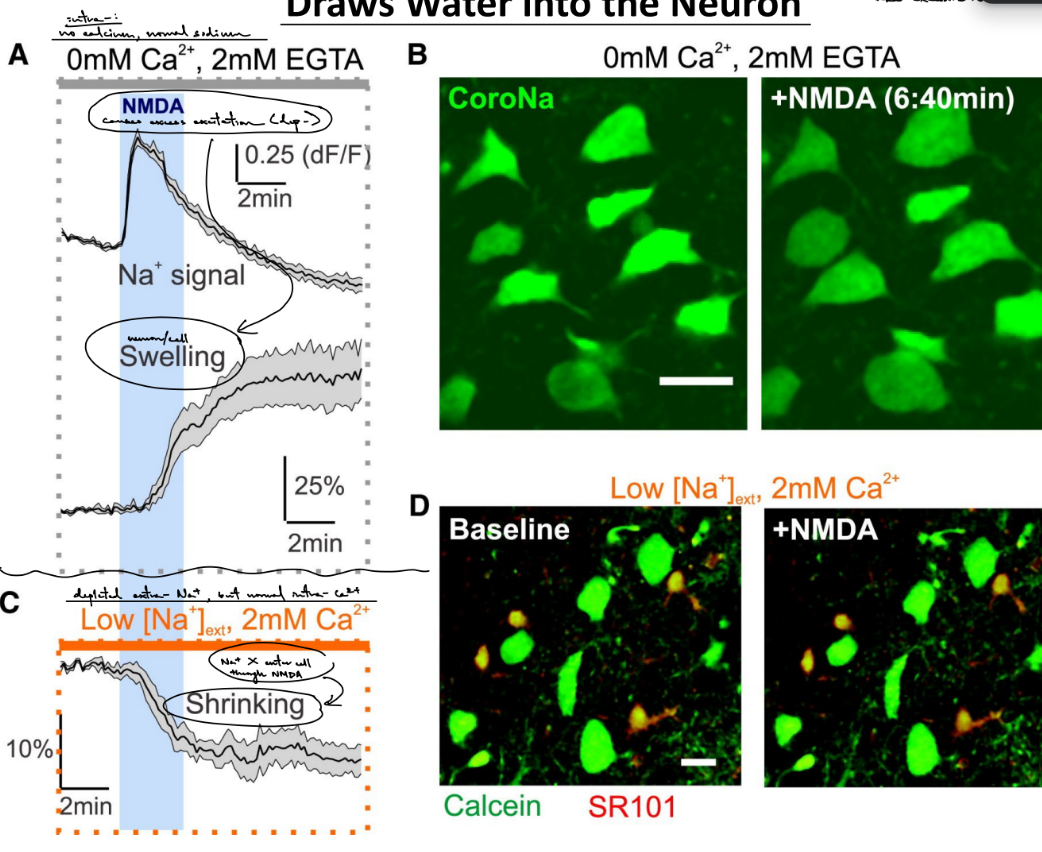
(b/c decrease of blood flow to the brain means less oxygen and glucose to the brain means less ATP is made, causing the cells in the vessel to have buildup of sodium → dep- → excess glutamate release into synaptic cleft → hyperactivation of NMDARs → excess Na and Ca influx into post- → excess Na brings in water & the cell swells)
^ for buildup of intra- sodium b/c ATP power the Na/K pump to move sodium out of the cell
hemorrhagic stroke — localized loss of blood flow to the brain due to burst blood vessel
usually due to high BP
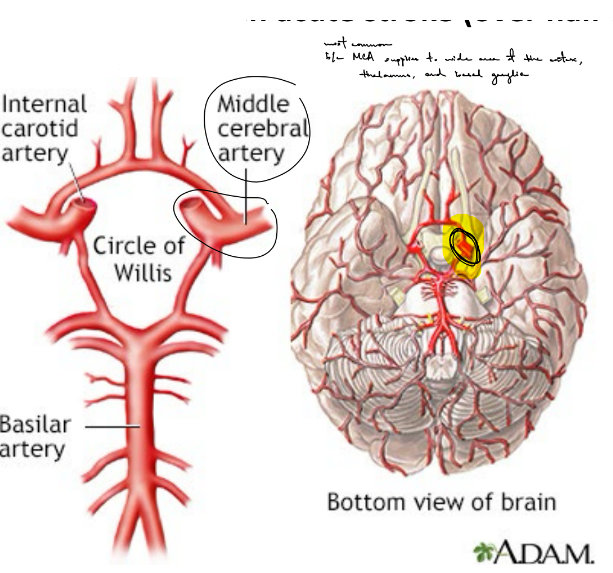
what is the most common artery involved in strokes?
this artery is involved in most (over half) of __ strokes
why is this artery the most common?
explain the type of effects (1)
__
middle cerebral artery (MCA) is most common artery involved in strokes
involved in most ischemic strokes
is the most common b/c the MCA supplies blood to a large area of the cortex, thalamus, and basal ganglia
SO it has a wide range of symptoms depending on which branches/structures are affected
name the 2 categories of stroke risk factors (& def. each)
state the risk factors in each category (4 ← describe / 5)
__
def. mini-strokes
another name for it
describe (1)
__
what does the “BE FAST” acronym for stroke stand for?
non-modifiable risk factors: ← can’t change its risk of causing strokes
age (risk increases w/ age)
sex (more young men than young women are affected, BUT young women w/ stroke have higher mortality)
race (higher risk in POC)
genetics (i.e. cardiovascular factors)
__
modifiable risk factors: ← can change the risk of causing stroke (either increase or decrease the risk)
smoking
alcohol consumption
diet & obesity
physical inactivity
hypertension aka high BP
__________
mini-strokes / transient ischemic attack (TIA)
the temporary loss of blood flow to the brain due to a blood clot that reverses itself w/in a day
are warning signs for stroke risk, where 1/3 of people who experience TIA will experience a stroke w/in a year
__
Balance (loss of balance, headache, dizziness)
Eyes (blurred vision)
Face (unilateral face drooping)
Arms (arm or leg weakness or numbness)
Speech (trouble speaking or understanding speech)
Time (to call ambulance)
for ischemic stroke
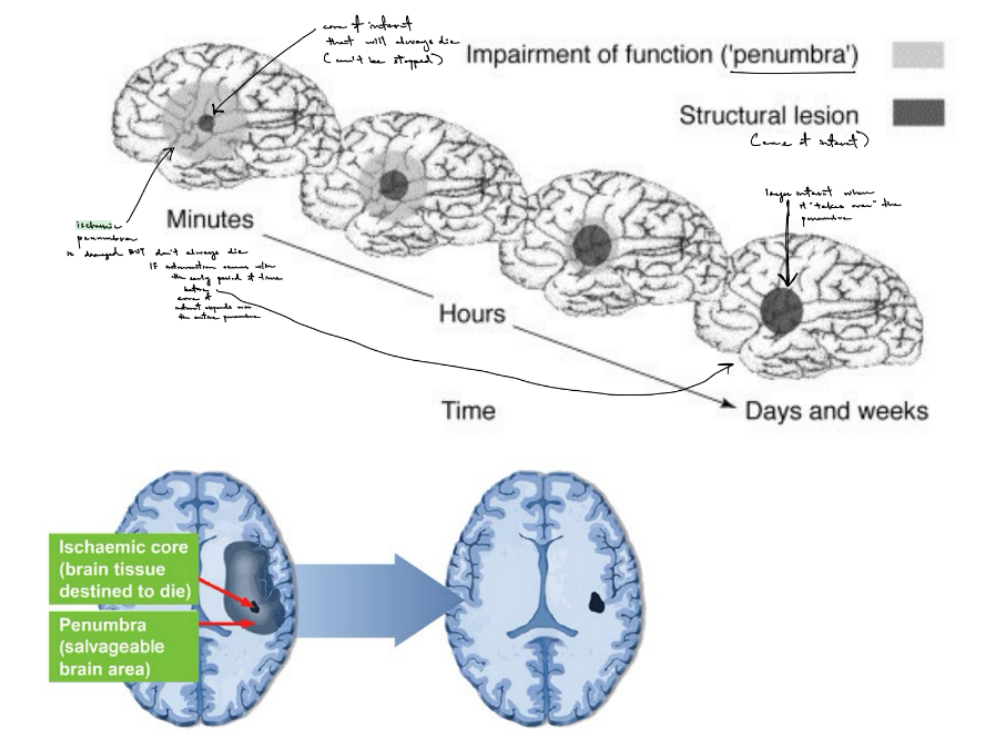
explain how the area impacted by the stroke grows AKA spatiotemporal expansion of the infarct
minutes after the start of a stroke, will have a small infarct core surrounded by ischemic penumbra, where:
cells in the core will always die (← dead tissue, irreversible, death is via cell edema)
cells in the penumbra is only partially damaged AND can be rescued/saved IF intervention/treatment occurs w/in an early period of time before the core expands to include the penumbra
over hours, the core will expand to encompass/include the penumbra
days to weeks after the start of a stroke, the core takes over the penumbra completely, SO all the cells in the infarct will die
for ischemic stroke
term for blood vessel?
what is the term defined as emergency ischemic stroke treatment that aims to restore blood flow in the vessel?
name the 2 approaches to this & briefly def. them
describe each approach of this ischemic stroke treatment (3, each w/ 2-3 more / 1)
thrombus = blood clot
recanalization — emergency ischemic stroke treatment that aims to restore blood flow in the vessel
thrombolysis — breaking apart blood clots
thrombectomy — removing blood clots
__
thrombolysis
ischemic stroke patients will receive tPA (tissue plasminogen activator) if:
diagnosed w/ ischemic stroke
is w/in 4.5 hours from the start of the (ischemic) stroke
cannot receive tPA if:
diagnosed w/ hemorrhagic stroke
have high BP
had recent head trauma or head surgery
2 tPA treatments are:
Alteplase
Tenecteplase
__
thrombectomy ← done when the clot/thrombus is too large for tPA OR if after the 4.5 window
insert stent into femoral artery (of thigh) that will move through blood vessels to get to the brain, where the stent will grab the thrombus/blood clot & pull it out
for ischemic stroke
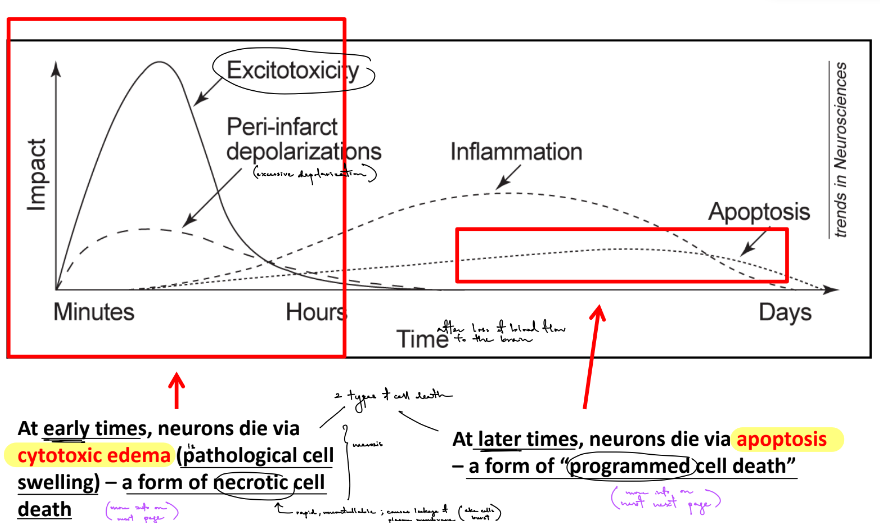
b/c spatiotemporal expansion of the infarct occurs over time, what happens at early vs. later times? (← use a specific term for each & def. it)
state the 3 ~stages that occur over time
describe 1 of them (1)
in early time, neurons die via cytotoxic edema ← pathological cell swelling that is a type of necrotic cell death
(^ cytotoxic edema/swelling is what happens before the onset of necrosis)
in later time, neurons die via apoptosis ← a type of programmed cell death
__
excessive infarct depolarization, where this excessive excitation will destroy neurons — called excitotoxicity (where cytotoxic edema & necrosis can occur)
→ inflammation
→ apoptosis
for ischemic stroke
explain cytotoxic edema, which occurs in the early stage after stroke (2)
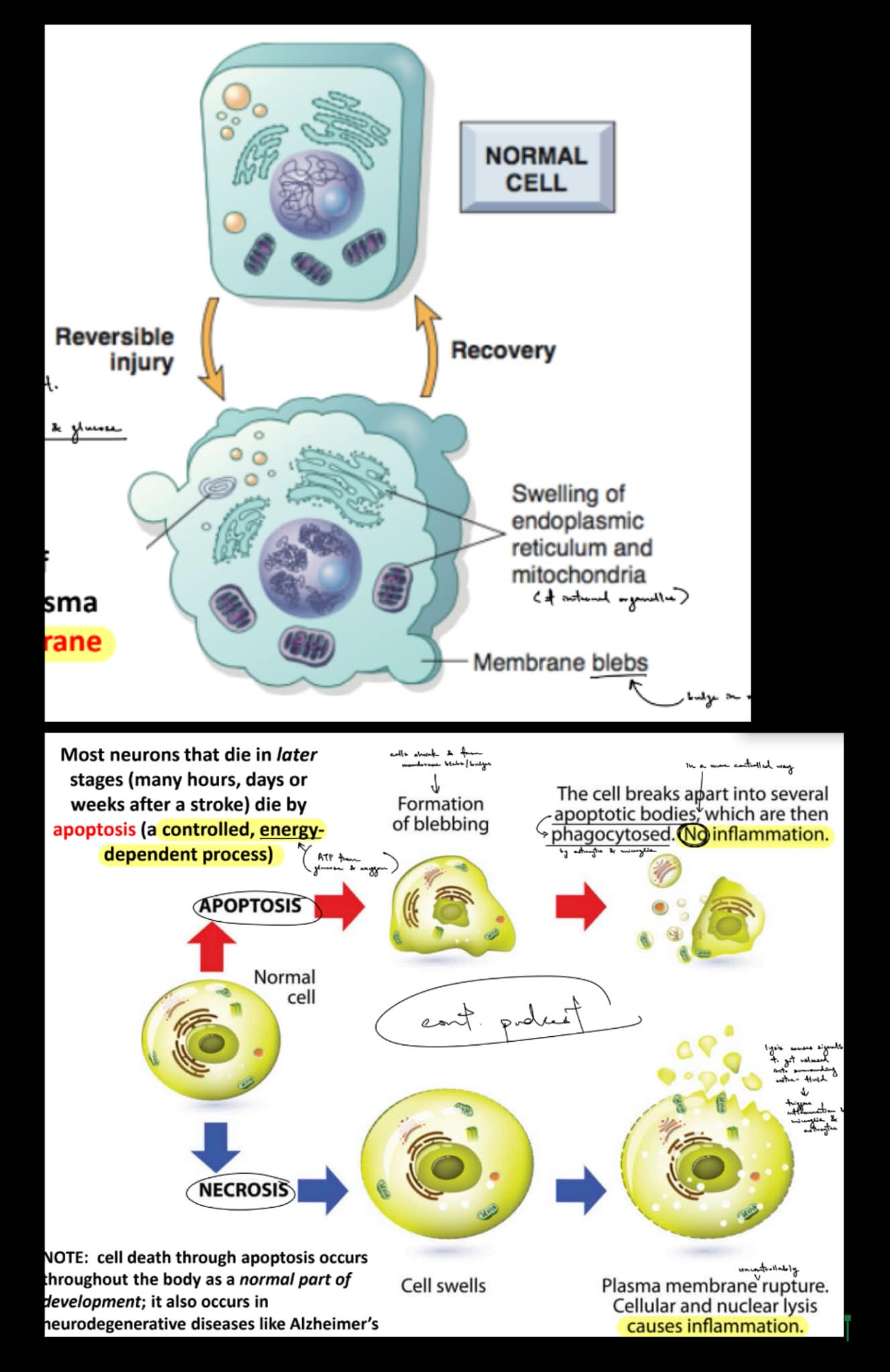
explain how a normal cell/neuron can undergo either apoptosis or necrosis
apoptosis is a __, __-__ process
__
t/f: cell death through apoptosis occurs throughout the body as a normal part of development; it also occurs in neurodegenerative diseases like AD
cytotoxic edema is seen as the swelling of organelles & forms membrane blebs, which are bulges in the membrane
cytotoxic edema makes the membrane leaky b/c the neuron loses control of membrane permeability (as seen w/ the membrane bleb)
__
if normal cells does apoptosis, then membrane blebs will form → then, the cell breaks apart into apoptotic bodies that are phagocytosed by microglia & astrocytes
apoptosis does NOT cause inflammation
if normal cells does necrosis, then the cell swells → then, the plasma membrane bursts (lysis)
necrosis causes inflammation
…
apoptosis is a controlled, energy-dependent process
(^ energy-dependent meaning that apoptosis relies on ATP for energy)
__
true
for ischemic stroke
differences b/w necrosis & apoptosis, in terms of:
affected cells are
induced by
inflammation or no inflammation
effect on cytoplasm & nucleus or mitochondria
effect on plasma membrane
energy & passive or active
which one has a key feature of calcium overload?
necrosis (N), apoptosis (A)
N affects groups of cells vs. A affects individual cells
(b/c N is uncontrolled, passive process, while A is controlled, energy-dependent (active) process)
N is caused by pathogens/toxins vs. A is caused by physiological stimuli (i.e. development)
(b/c physiological events occur over time, like how N is a delayed process that occurs over/after longer period of time)
N causes inflammation vs. A doesn’t
N does swelling of cytoplasm + mitochondria/organelles vs. A does shrinking of cytoplasm (b/c breaks into apoptotic bodies) & condensation of nucleus
N has ruptured membrane vs. A has membrane blebbing, where membrane is intact
N doesn’t require energy / is passive vs. A is energy(ATP)-dependent / is active
N involves calcium overload
for ischemic stroke
t/f: a stroke triggers neuronal cell death
what are the immediate cellular changes after a stroke? (7)
the delayed cellular changes? (2)
true
__
immediate cellular changes:
ATP depletion (b/c stroke is loss of blood)
excess depolarization
excess glutamate (b/c of excess dep-/excess excitation)
increased intra- Ca2+
get cytotoxic edema that causes necrosis is in the core
get cytotoxic edema that does NOT cause immediate necrosis is in the penumbra
make ROS (reactive oxygen species)
_
delayed cellular changes:
inflammation
apoptosis of the penumbra
for ischemic stroke
ischemia includes a __ of subcellular & transcellular events
state the general events above (~2/3 parts)
ischemia includes a cascade of subcellular & transcellular events (← ischemic cascade)
__
excess Na+ and Ca2+ influx through NMDARs
excess Ca2+ → causes mitochondrial damage → causes apoptosis, WHILE excess Na+ → causes excess depolarization & cell swelling/edema

for ischemic stroke
explain the immediate cellular effect after stroke: ATP depletion (2)
swelling is caused by (2), which (function ← 1)
loss of blood flow to the brain will bring less glucose & oxygen to the brain, SO less of these 2 will makes less ATP (energy)
the Na+/K+ pump uses a lot of ATP b/c the pump maintains the RMP by using ATP to move ions against their concentration gradient
…
swelling is caused by depolarization & excess Na+ influx, which brings water into the neuron
for ischemic stroke
explain the immediate cellular effect after stroke: excess depolarization (4)
dendritic beading is a sign of __ __
t/f: Excitatory networks are especially vulnerable during ischemia
__
explain the immediate cellular effect after stroke: excess glutamate (2)
also contributes to excess intracellular __ (← step where get increased/excess intra- Ca2+)
the core of the infarct experiences a loss of blood flow (and glucose + oxygen)
core doesn’t make ATP so has no energy
core will excessively dep- (aka excess excitation), which releases glutamate out of the core into the penumbra
the penumbra triggers neighboring cells to dep- via dendritic beading, which might expand the infarct
^ called “spreading depolarization”
__
dendritic beading is a sign of cytotoxic edema/swelling
__
true
glutamate buildups in the synaptic cleft faster than it can be removed
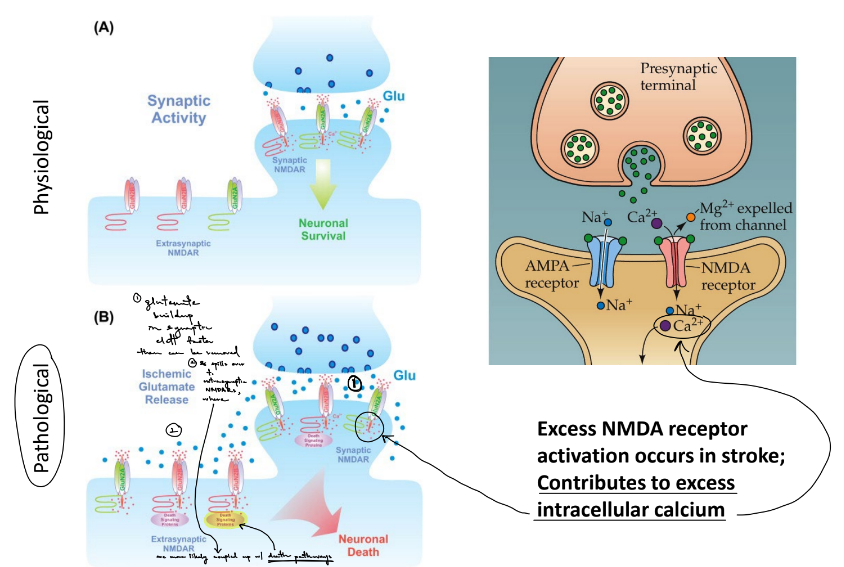
so, glutamate spills over to the extrasynaptic NMDARs which are coupled up w/ death pathways
also contributes to excess intracellular calcium (← step where get increased/excess intra- Ca2+)
for ischemic stroke
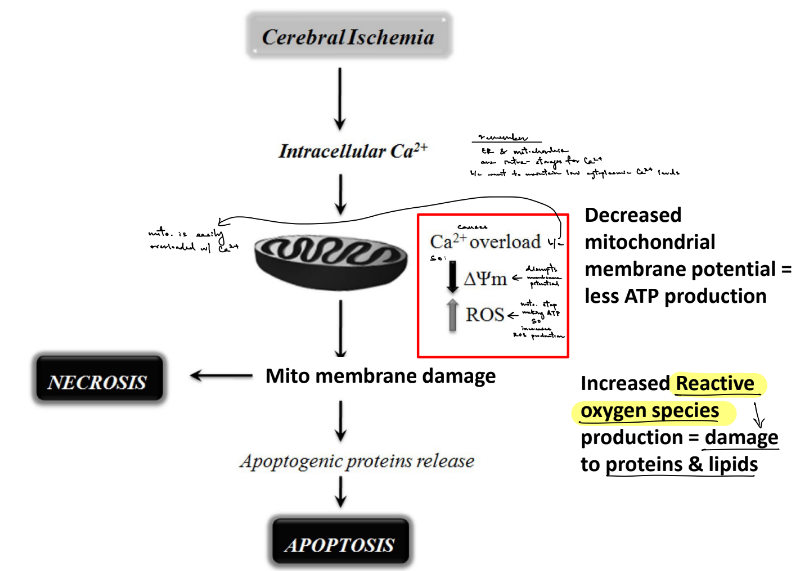
how does excess intra- Ca2+ damage mitochondria?
__
t/f: healthy mitochondria always make ROS in small amounts, but impaired mitochondria makes too much
t/f: excess unregulated production of ROS are bad for the cell b/c it leads to cellular damage & many types of disease
__
what do ROS do? (2)
Ca2+ is stored in ER and mitochondria in order to maintain a certain level of cytoplasmic Ca2+, BUT mitochondria is easily overloaded by calcium
→ SO, get decreased membrane potential & formation of ROS (b/c mitochondria stop making ATP, which increases ROS production) ← where ROS damages proteins & lipids
__
true
true
__
ROS have unpaired electrons that react w/ proteins, lipids, and nucleic acids, which impairs their function
you can slightly improve their functions w/ diet via antioxidants, like vitamin C and E
for ischemic stroke
for the delayed cellular effects after stroke: inflammation & apoptosis of the penumbra
damaged mitochondria initiate __ cell death by releasing (1 ← def.)
aka apoptosis is a __ form of cell death that is caused from (1)
_
(2 ← aka the 2 acute brain injuries mentioned) induce inflammation, which is triggered by BOTH (2)
for 1 of the triggers, explain how it activates inflammation (~4 steps/parts)
for the other trigger, explain how it controls inflammation:
BBB is part of the __ __ made of (3), whose signals will (1) in order to (1)
damaged mitochondria cause delayed cell death by releasing apoptotic factors/bodies (are proteins that trigger apoptosis)
aka apoptosis is a delayed form of cell death that is caused from damaged mitochondria
^^ this specifically refers to apoptosis w/ ischemic stroke, while the ATP failure, excess Na and Ca, etc. refers to necrosis w/ ischemic stroke
_
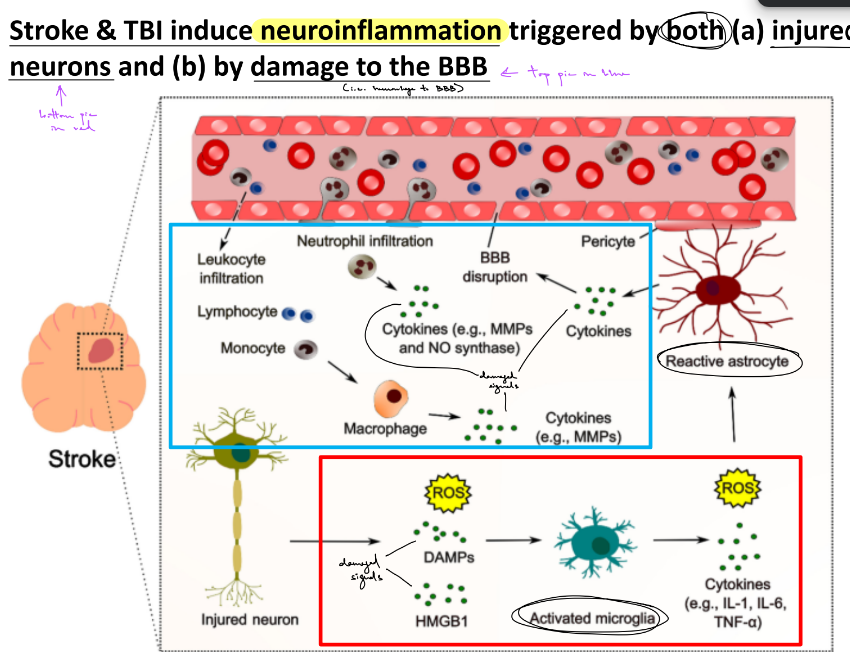
stroke & TBI induce inflammation, which is triggered by BOTH injured neurons & damage to the BBB
(^ cytotoxic edema/cell swelling is injured neurons, rupturing of membrane is damage to BBB)
injured neurons will release DAMPs (damage associated molecular patterns), which will bind to Rs of immune cells → activate signaling pathways (in immune cells) → immune cells release cytokines & chemokines → inflammation
specifically, sterile inflammation (is inflammation caused w/o pathogens)
BBB is part of the neurovascular unit made of neurons, astrocytes, and pericytes, whose signals will control the diameter of blood vessels in the brain → in order to control rate of local blood flow
(pic shows that astrocytes make contact w/ astrocytes & neurons, so is like the “in-between” structure of the two)
def. TBI (& stands for what?)
t/f: can appear w/o physical evidence
symptoms are classified as (3)
t/f: TBI and stroke have sim. cascades
concussion is a __ TBI
describe (1)
__
def. CTE
symptoms (3)
affects __ __ of the neocortex, which progressively spreads
CTE is a __ (def. term)
CTE tau tangles begin in __ __
CTE tauopathy is prominent around __ __
t/f: pattern of CTE tauopathy is distinct from other tauopathies
traumatic brain injury — is damage to the brain tissue caused by an external force
true (i.e. whiplash)
symptoms can be mild, moderate, or severe
true
concussion is mild TBI
usually have change in consciousness (i.e. disoriented, feeling dazed, foggy thinking), NOT loss of consciousness
__
CTE (chronic traumatic encephalopathy) — is a permanent, progressive neurodegenerative disease caused by repeated blows to the head / TBI (i.e. repeated concussions)
symptoms:
aggression
memory loss
depression & suicide
affects deep sulci of the neocortex, which progresively spreads
CTE is a tauopathy (NFTs containing abnormal tau aka tau that is hyperphosphorylated & mislocalized)
CTE tau tangles begin in deep sulci
CTE tauopathy is prominent around blood vessels
true
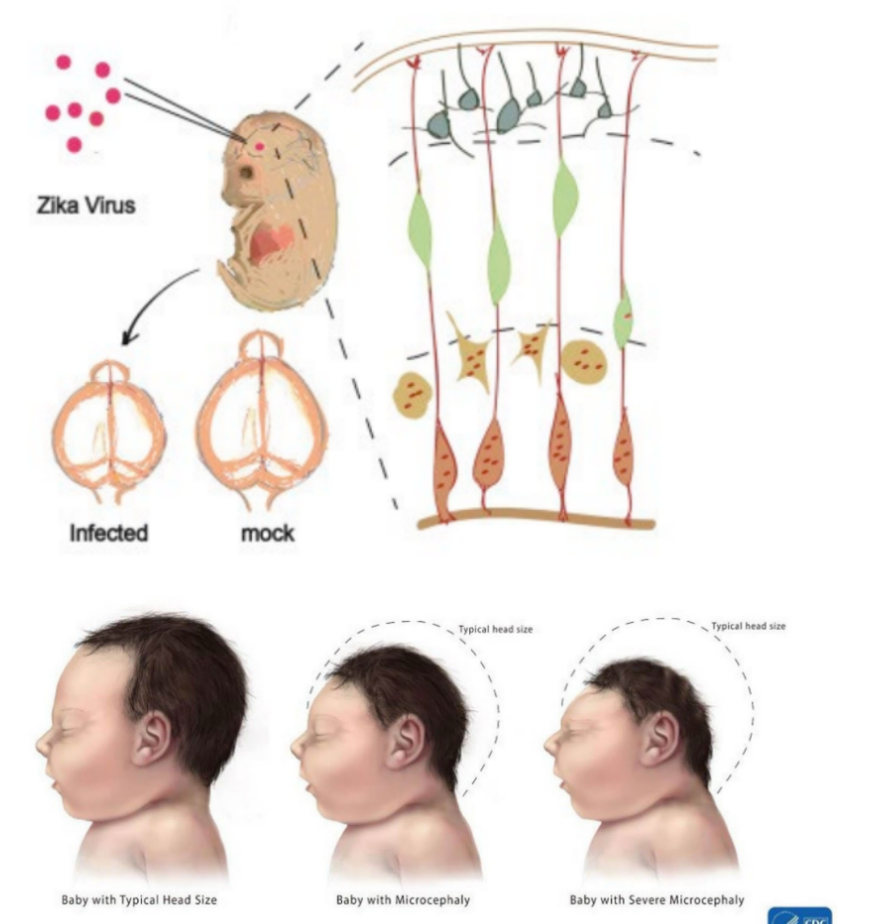
def. Zika
t/f: pregnant women advised not to travel to regions where Zika virus were present
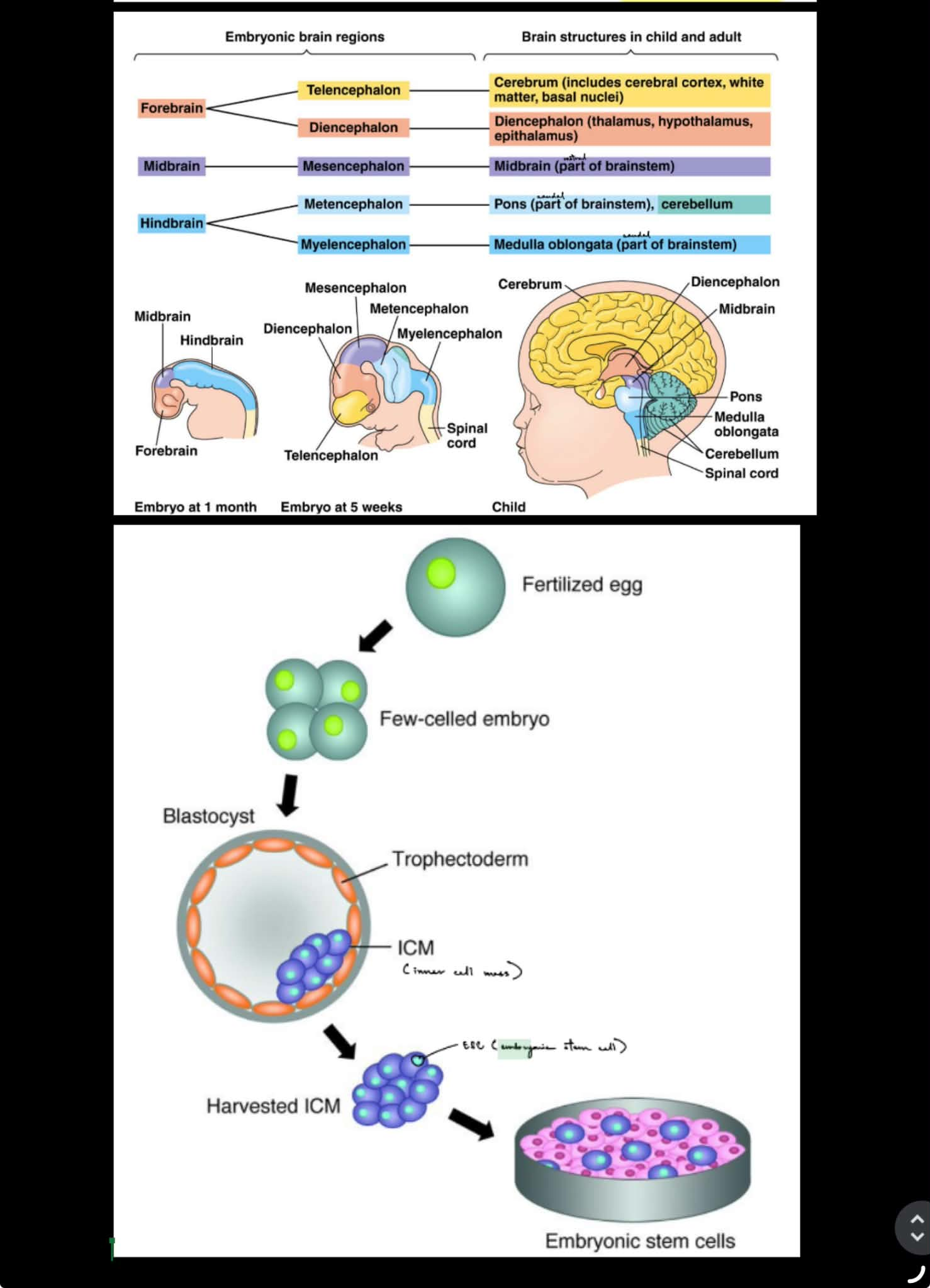
the NS forms during embryonic development, where (embyronic brain regions → brain structures in adult and children)
forebrain → (2) → (1) (2)
midbrain → (1) → (1)
hindbrain → (2) → (2) (1)
__
how are ESCs formed?
Zika — a mosquito-borne virus that can cause microencephaly (small brain size) in infants
true
forebrain
→ tele|encephalon → cerebrum
→ di|encephalon → thalamus, hypothalamus
midbrain
→ mes|encephalon → brainstem
hindbrain
→ met|encephalon → pons, cerebellum
→ myel|encephalon → medulla
___
fertilized egg → embryo → blastocyst w/ ICM (inner cell mass) → harvested ICM → ESCs
def. stem cell (2)
def. neural stem cell (2)
another name
can undergo either __ or __ cell division (← def. each)
t/f: cells cannot self-renew if they are differentiated
stem cells are self-renewing (aka replicate itself) & can differentiate into multiple cell types
neural stem cells also self-renew BUT can ONLY differentiate into neurons, astrocytes, or oligodendrocytes (← only structures present in the CNS)
(aka neural progenitors)
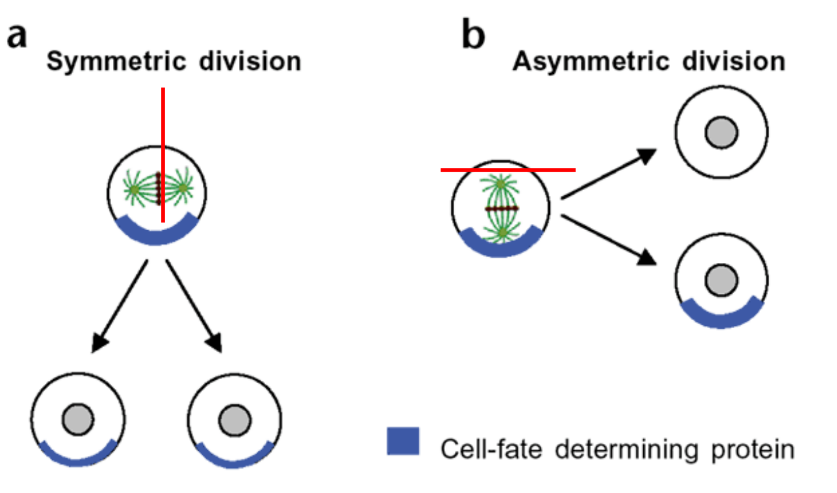
can do either symmetric or asymmetric cell division
symmetric — makes 2 SAME daughter cells
asym. — makes 2 DIFFERENT daughter cells: 1 stem cell & 1 other differentiated kind
true ← cells cannot self-renew if they are differentiated
how do you know whether sym. or asym. division is done?
cell-fate determining proteins will be separated either symmetrically or asymmetrically
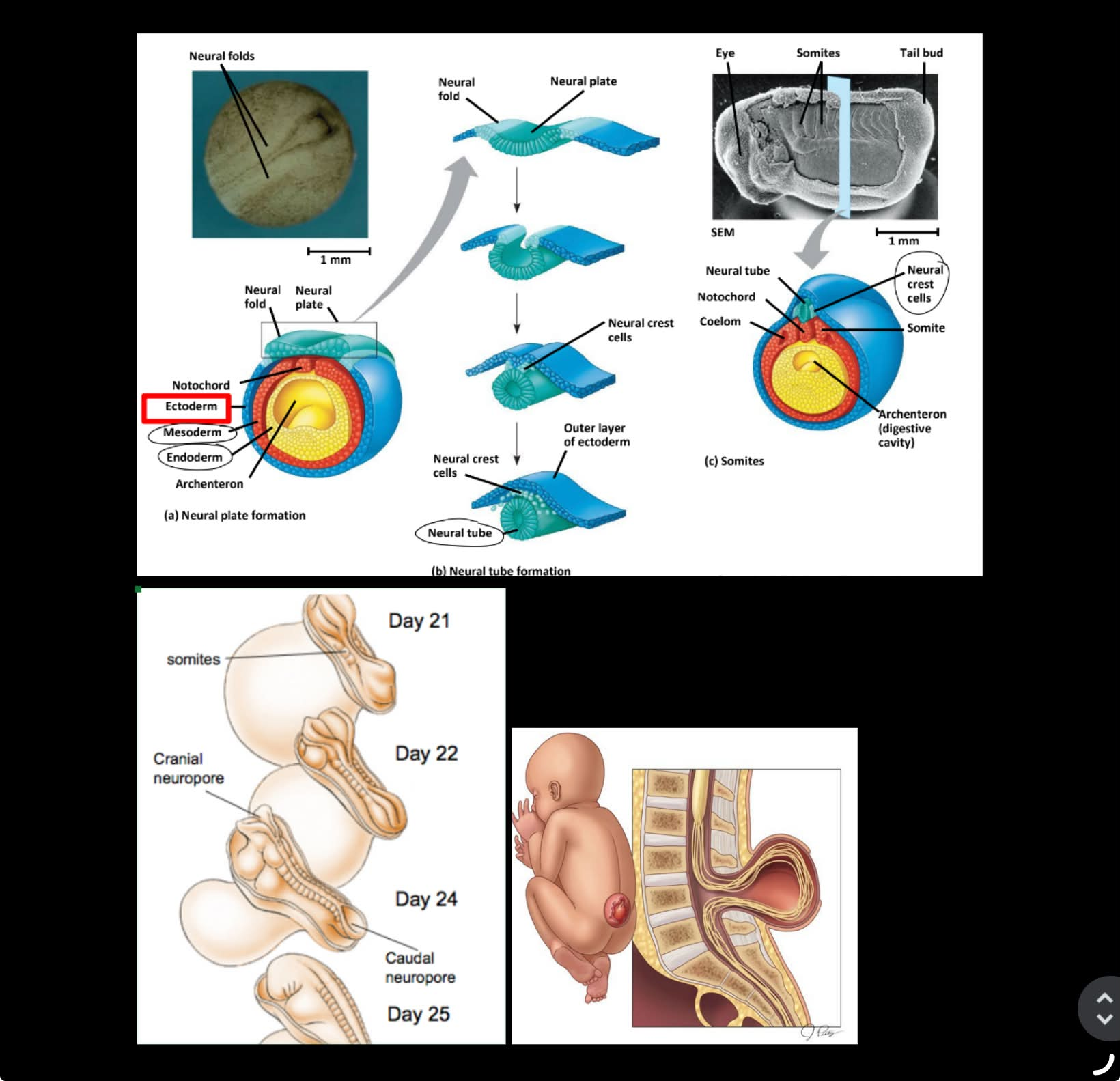
summary of neural tube formation in vertebrates (3)
__
what migrates away to/& gives rise to PNS neurons, melanocytes, and neuroendocrine cells?
neural tube closure starts in the center & proceeds in the __ & __ directions
__ __ results from failing to complete neural tube formation/closure
describe (1)
__
after development of neural tube, what occurs?
form the neural plate & 3 germ layers: ectoderm, mesoderm, endoderm
neural plate folds to → form neural tube (w/ ectoderm surrounding/encasing it)
form neural crest cells & somites (somites from mesoderm)
^^
neural crest cells migrate away & differentiate into PNS neurons
neural tube closure starts in the center & proceeds in the caudal & rostral directions
spina bifida results from failing to complete neural tube formation/closure
cause defects in SC and spinal bones
__
after development of neural tube, fore/mid/hindbrain will differentiate into the brain structures that are present in children & adults (← picture in prev. flashcard)
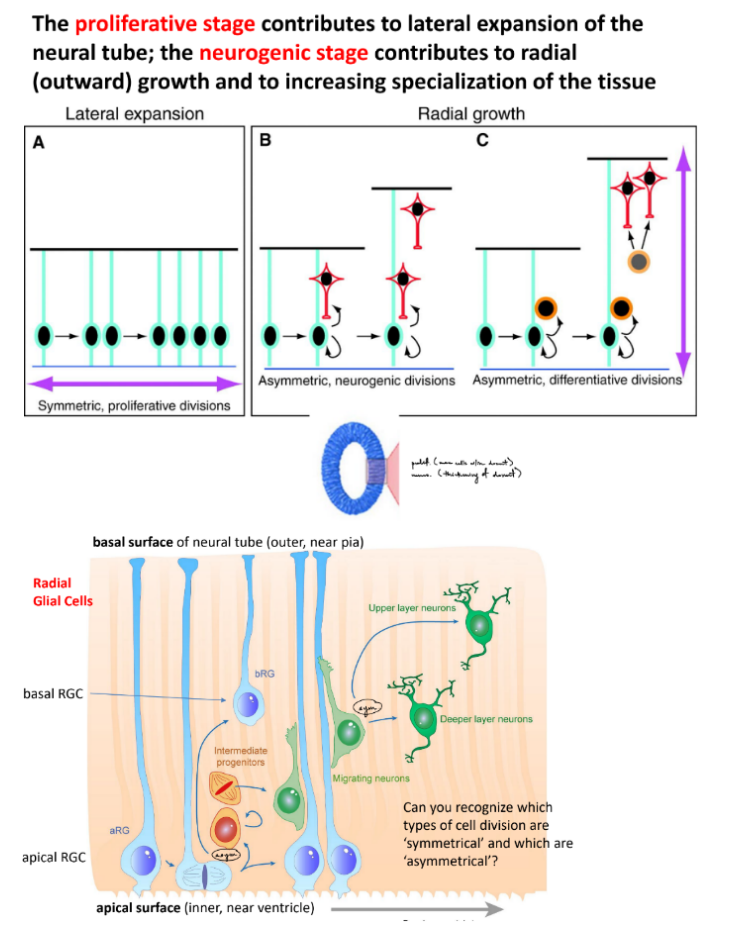
neural progenitors (aka precursor for neurons & glia) form in the __ __
name a key neural progenitor (1)
explain how cell differentiation occurs w/ these neural stem cells (← aka name the 2 stages)
what kind of division involved in each stage
what occurs in each stage
each stage’s relation to expansion/growth of neural tube
neural progenitors (aka precursor for neurons & glia) form in the neural tube
radial glial cells (RGCs)
proliferative stage ← mainly sym. division
1 RGC will produce another RGC → SO have 2 RGCs (same daughter strands)
neurogenic stage ← mainly asym. division
2 RGCs will differentiate into different things from e/o: neurons, oligodendrocytes, astrocytes
proliferative stage does lateral expansion of neural tube (more w/in the neural tube / concentrated)
neurogenic stage does radial growth (thickening) to increase specialization of tissue
note that for neurogenic stage, the ventricular end (apical surface) is deepest end & pial end (basal surface) is shallowest end where newly differentiated cells go
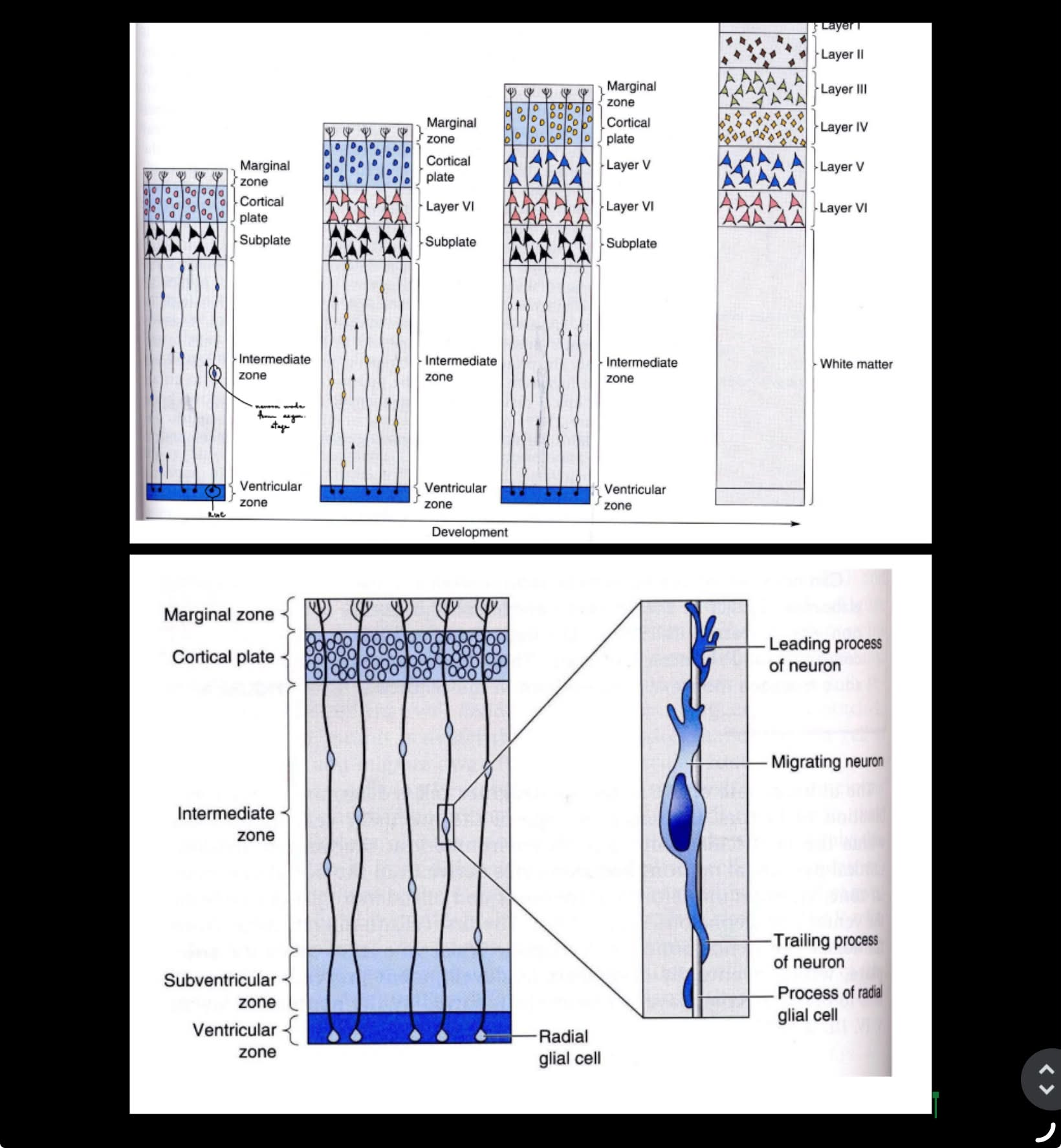
for neuronal differentiation
layers of neurons develop in an __-__ manner, where (1) b/c …
rel. migrating neuron & RGC
t/f: neurons in diff. layers of cortex have distinct circuit connectivity & function
inside-out manner, where oldest neurons are the deepest / closest to ventricular end (apical surface)
b/c the more recent neurons migrate past the earlier born neurons to reach the cortical plate
migrating neurons OFTEN will move up the RGC towards the cortical plate at pial end
__
true
t/f: specific mutations disrupt cortical cell migrations
state example of gene that’s mutated to disrupt migrations (← more mentioned about this gene in later flashcard)
during migration, neurons also begin to develop __
__
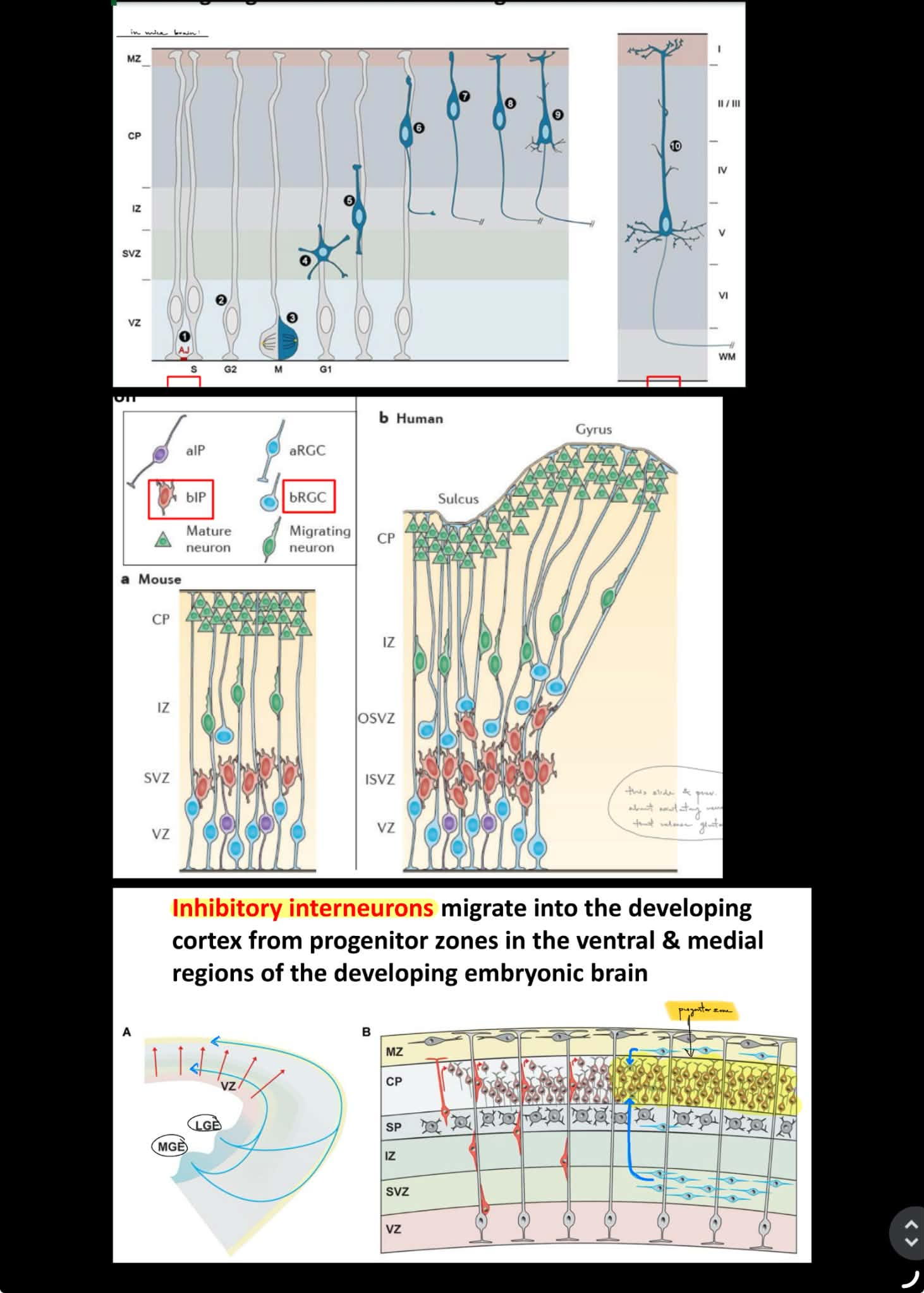
primate brains have subtypes of neural progenitors called (2), which will (1)
what type of neurons will also migrate from the __ __ (which is…) in the __ & __ regions of developing embryonic brain INTO the developing cortex
true
Reelin gene mutations will cause disorganization of migrating neurons
during migration, neurons also begin to develop axons
__
primate brains have subtypes of neural progenitors called intermediate progenitors (IPs) & basal radial glial cells (bRGCs), which will form a new zone of proliferation (aka new area/layer of proliferation)
inhibitory interneurons will also migrate from the progenitor zones in the ventral & medial regions of developing embryonic brain INTO the developing cortex
^^
progenitor zones are where neural progenitors aka neural stem cells are located
developing cortex (is area w/ lots of neurons)
how does Zika virus relate to microencephaly & neural progenitor development? (general statement & describe ← 4)
Zika virus disrupts neural progenitor development → leads to microencephaly in mice, where:
Zika virus replicates in embryonic mouse brain
infects neural progenitors cells (NPCs)
leads to defects in differentiation
induces immune response (inflammation) in the brain AND apoptosis of post-mitotic neurons
→ altogether: infected NPCs, differentiation defects, immune response, and apoptosis will cause microencephaly that ranges in severity
summary of early cortical development (from RGCs to differentiated neurons and glia) ← ~2/4
_
the mammalian cerebral cortex is said to have _#_ layers
describe the layers (3)
____
t/f: neuronal migration brings neurons from their birthplace near the ventricular zone (VZ) up to the marginal zone (MZ) (near the pia) to ultimately form the cortex
neural progenitors/neural stem cells do sym. division → 2 RGCs
intermediate progenitors (IPs) & basal radial glial cells (bRGCs) form a new zone of proliferation
migrating neurons move up RGCs
do asym. division → 2 different daughter cells that are a upper layer neuron & a lower layer neuron
__
the mammalian cerebral cortex is said to have 6 layers
layer 1 — has NO cell bodies
layers 2 & 3 — mostly upper layer neurons (closer to pial end / basal surface) that do communication b/w the 2 hemispheres
layers 4 & 5 — mostly deep layer neurons (closer to ventricular end / apical surface) that will project to subcortical regions
(layer 6 isn’t mentioned)
____
true
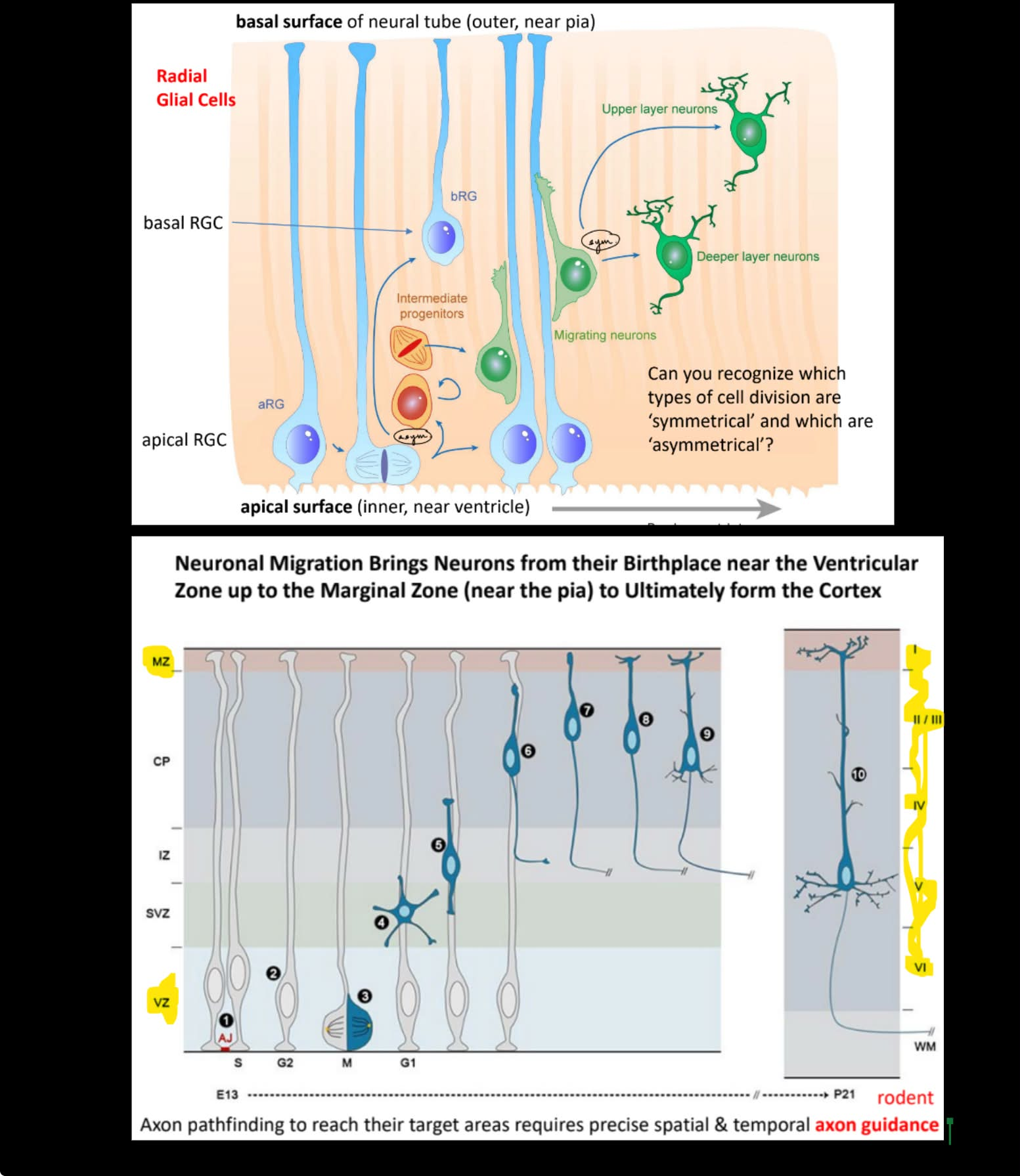
axon pathfinding, where axon reach target areas, will require spatiotemporal __ __ __ that determine when to __, __, and __
name the 2 types of cues (& 2 things from each)
t/f: these guidance molecules/cues are located OUTSIDE of the cell
VS.
how do growth cones steer the direction of the axon w/ INSIDE the cell mechanisms? (← mention 2 specific structures)
__
__ is the first guidance molecule/cue discovered that’s used in the spinal cord
how does it function?
t/f: this specific guidance cue is both NECCESSARY & SUFFICIENT for guiding axons
neuron migration is also guided by extracellular (OUTSIDE) cues, such as __
(optional: summarize what this cue is overall)
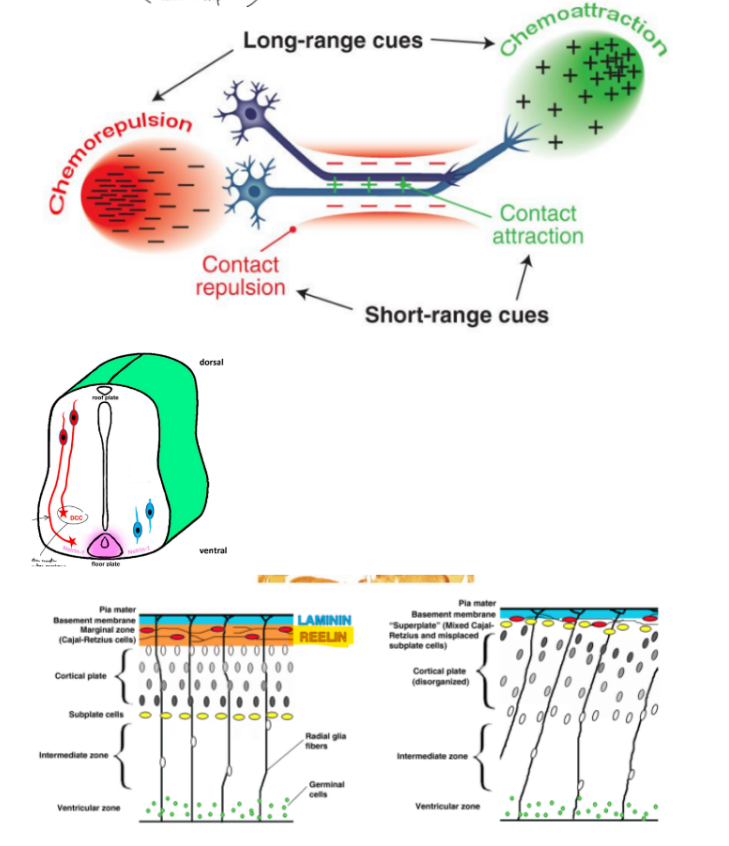
axon pathfinding, where axon reach target areas will require spatiotemporal axon guidance molecules that deter. where to extend, turn, and stop
short range cues: direct repulsion or direct attraction ← direct contact
long range cues: are chemoattractants or chemorepellants ← for the axon
VS.
growth cones steer the direction of the axon by polymerizing microtubules/MTs towards attractive cues & away from repulsive cues, where F-actin look for axon guidance cues in the environment & MTs polymerize to extends towards or away from certain cues
__
Netrin is the first axon guidance cue discovered
cells w/ DCC (Netrin R) extends down to the floorplate that secretes Netrin (on one side of the SC) → the axon crosses over the midline → cells moves away from the floorplate w/ Netrin (on other side of SC)
(^ Netrin is a chemoattractant, then cells get less attracted/repulsed by Netrin after crossing over)
true ← Netrin is NECCESSARY & SUFFICIENT for guiding axons
(as seen w/ experiments w/ knockout cells & adding Netrin to normal cells that initially don’t have Netrin)
neuron migration is also guided by extracellular (OUTSIDE) cues, such as Reelin
(Reelin is both an extra- axon guidance cue & a gene that will disrupt the organization of neuronal migration when mutated)
RGCs (radial glial cells) act as a structural __ to guide initial neuron migration
specifically, what aspect of MTs is key in neuronal migration? (1 & def. “term”)
SO mutations in several __ genes are associated w/ brain malformations, like microencephaly
…
3 roles of MTs in brain development
mutations in tubulin genes or MT-association proteins like (2) will disrupt these 3 functions above
…
a growth cone & leading tip of migrating neuron are similar in that (~1/2)
t/f: classifications of brain malformations are basically the abnormal functions of MTs
state the 3 classifications of brain malformations
RGCs (radial glial cells) act as a structural scaffold to guide initial neuron migration
specifically, microtubule cell motility (is a key mech. in neuronal migration)
is the transportation of neurons along MTs via motor proteins, like kinesin & dynein
SO mutations in several tubulin genes are associated w/ brain malformations, like microencephaly
…
MTs do:
cell division (proliferative stage: sym. & asym. division)
cell migration (neurogenic stage)
neurite outgrowth aka extension/growth of axons and dendrites (for axon pathfinding)
is related to post-migration cortical organization
mutations in tubulin genes or MT-associated proteins like LIS1 & DCX will disrupt these 3 functions above
…
a growth cone & leading tip of migrating neuron are similar in that they require MTs that coordinate w/ F-actin
true
abnormal cell proliferation or apoptosis
abnormal neuronal migration
abnormal post-migration cortical reorganization
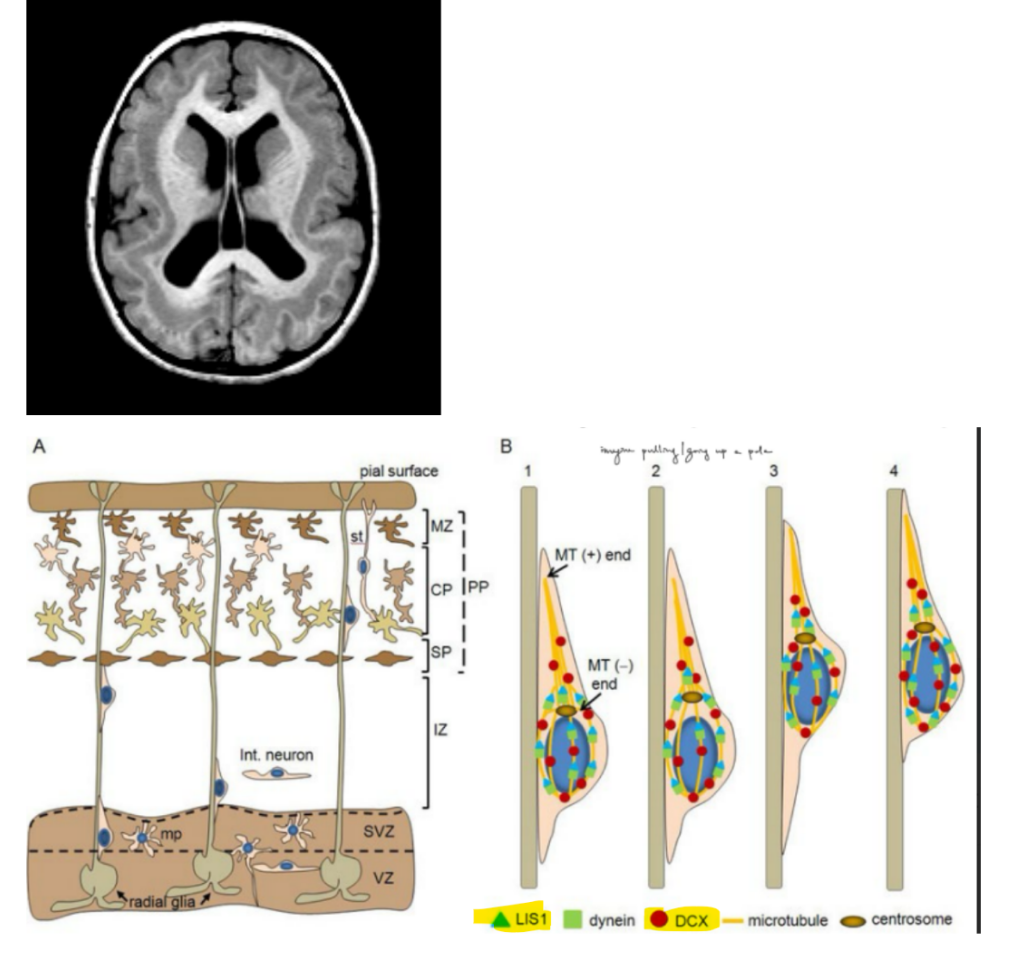
Lissencephaly is a type of brain developmental abnormality characterized by (2)
it results from abnormal / defective __ __ during cortical development, specifically what happens is __ __ aka …?
Type 1 lissencephaly has many unknown genetic defects, but the known genetic mutations are (5)
Lissencephaly seen to have:
large ventricles
missing sulci & gyri
it results from abnormal / defective cell migration during cortical development, specifically improper layering AKA abnormal/misorganization of the 6 layers of the mammalian cerebral cortex
_
Type 1 lissencephaly has many unknown genetic defects, but the known genetic mutations are:
PAFAH1B1 (aka LIS1 protein) gene mutation
DCX (X-linked doublecortin) gene mutation
Miller-Dieker syndrome (← involves LIS1/PAFAH1B1 genes)
XLAG
RELN (aka Reelin)
(^ where DCX and LIS1 are tubulin-associated proteins; LIS1 for Type 1 lissencephaly)
for Type 1 lissencephaly cause: Miller-Dieker syndrome & LIS1/PAFAH1B1 gene mutation
def. Miller-Dieker syndrome
…
MTs have __ of a __ end & __ end (where both ends differ structurally and functionally)
which end is the (rapidly) growing end?
name 2 MT motor proteins & what each does
LIS1 is a MT-associated protein, specifically a __-associated protein that does __ transport b/c …
…
how is LIS1 and RELN (reelin) similar? (1)
microdeletion in Chr 17 of PAFAH1B1 genes that code for LIS1 protein
…
MTs have polarity of a “-” end & “+” end (where both ends differ structurally and functionally)
“+” end is the end where MT polymerization occurs
kinesin does anterograde transport towards the "+” end
dynein does retrograde transport towards the “-” end
^ think “kid” aka k | d
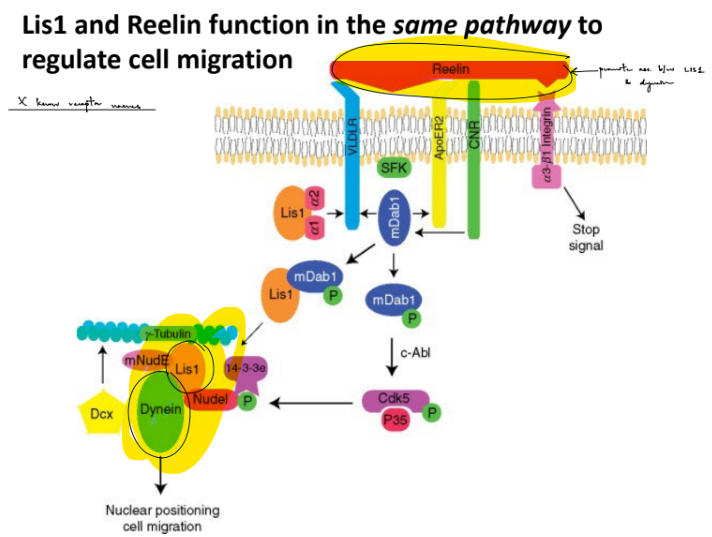
LIS1 is a MT-associated protein, specifically a dynein-associated protein that does retrograde transport b/c LIS1 protein forms a protein complex w/ dynein
…
LIS1 and Reelin function in the same pathway for cell migration, where Reelin promotes formation of the LIS1-dynein protein complex
(note that the MT “-” end is closer to soma, MT “+” end is closer to axon terminal)
for Type 1 lissencephaly cause: DCX (X-linked doublecortin) gene mutation
DCX (X-linked doublecortin) gene mutation results in (1) that resembles a __ __← def. a specific term w/in this
more common in __ b/c …
DCX is a __-associated protein
…
both LIS1 and DCX are involved in regulating MTs during cell migration, which includes __ (← def. term)
SO mutations of either of the 2 MT-associated proteins lead to (1) and as a result __ __
____________
growth cones and tips of migrating neuron both require MTs coordination with F-actin, but what key thing distinguishes their "action"? (1 general w/ 2 specific)
DCX mutation results in subcortical band heterotopia, that resembles a “double cortex”
^ heterotopia — “out of place”
more common in females b/c male fetuses die before birth due to having only 1 X chromosome (males have a more severe form of lissencephaly)
DCX is a microtubule-associated protein
…
both LIS1 and DCX are involved in regulating MTs during cell migration, which includes nucleokinesis (the translocation of the nucleus as the migrating neuron crawls up the MT)
SO mutations of either of the 2 MT-associated proteins lead to migration defects and as a result improper layering
(^ improper layering AKA misorganization of the 6 layers of the mammalian cerebral cortex)
____________
growth cones and tips of migrating neuron both require MTs coordination with F-actin, but they differ in what is being moved, where:
growth cones move the axon
migrating neurons move the nucleus
nearly all cortical malformations result in __ __ aka __
def. the 2 terms
describe (1)
nearly all cortical malformations result in seizure disorders aka epilepsy
(^ cortical malformations refers to abnormal cell division, cell migration, and post-migration cortical organization (of layers))
is a seizure disorder if they experience at least 2 seizures that are are separated by at least 24 hours
epilepsy — a chronic brain condition that causes seizures
seizures — a sudden disruption of the electrical communication b/w neurons (imbalance of excitatory & inhibitory inputs)
name 2 major types of seizures (& def. each)
name the types of seizures that are classified w/in each major seizure type (2 ← w/ another name for each / 3) (← def. each)
can detect seizures w/ __
seizures are an imbalance of __ (1) and __ (2) inputs
…
there are rare instances where epilepsy can be caused by __ (← def. term) that lead to __/__ imbalance
one treatment option of epilepsy caused by channelopathies is taking medications, where the medications target (1) or (1)
other treatment options are (4)
generalized seizures — affect both sides of the brain
absence seizures (aka petit mal seizures) — cause rapid blinking or a few seconds of staring into space
^ think “petit” mal as having petit/not obvious symptoms
tonic-clonic seizures (aka grand mal seizures) — cause a person to cry out, loss consciousness, fall to the ground, have muscle jerks or spasms
^ think “grand” mal as having grand/very obvious symptoms
focal seizures (aka partial seizures) — affect ONLY 1 side of the brain
simple focal seizures — affect small part of brain & causes twitching or change in sensation (i.e. strange taste or smell)
complex focal seizures — cause confusion and dazed state, where the person can’t respond for up to a few minutes
secondary generalized seizures — start in one part of the brain BUT spreads to both sides of the brain (aka person has a focal seizure that turns into a generalized seizure)
…
can detect seizures w/ EEG
seizures are an imbalance of excitatory (glutamate) and inhibitory (GABA, glycine) inputs
…
there are rare instances where epilepsy can be caused by channelopathies (mutations in ion channels) that lead to excitatory/inhibitory imbalance
one treatment option of epilepsy caused by channelopathies is taking medications, where the medications target ion channels or GABAA receptors
other treatment options are:
surgery
devices
diet
new therapies
for ONE treatment option of epilepsy caused by channelopathies is taking medications, where the medications target ion channels or GABAA receptors
how is GABA made? how is GABA transported? (2, 2)
which GABA Rs are iono- vs. metabotropic?
for GABAARs:
GABAARs induce __ SO:
anti-seizure medications work to prevent seizures by (1)
(1) work to cause seizures by (1)
GAD w/ vitamin B6 co-factor converts glutamate into GABA, where GABA exits the cell into the synaptic cleft through GAT (GABA transporters) OR exocytosis (w/ vesicles)
where GABA can either enter glial cells via GAT OR enter post- cell through GABA receptors (GABAA Rs or GABAB Rs)
GABA-A Rs — ionotropic; GABA-B Rs — metabotropic
GABAARs induce IPSPs (inhibitory PSPs) b/c these receptors release Cl- SO:
many anti-seizure medications prevent seizures by enhancing GABA transmission
b/c want to prevent E/I imbalance, so want to keep GABAARs normal function of releasing Cl- by activation of these receptors from GABA binding, SO want GABA production
many neurotoxins cause seizures by inhibiting GABA transmission
b/c want to cause seizures, so want E/I imbalance by preventing normal GABAAR function, SO don’t want GABA production
for ONE treatment option of epilepsy caused by channelopathies is surgery
how does surgery treat epilepsy
ex. is w/ patient __
for ONE treatment option of epilepsy caused by channelopathies is diet
__ diet may help prevent seizure disorders aka epilepsy b/c …
SPECIFICALLY, …
surgery cuts out the brain tissue where seizures originate/start in
ex. is w/ patient H.M.
ketogenic diet helps prevent seizure disorders aka epilepsy b/c the mitochondria metabolism will produce ketone bodies, which are used as an alternative source of fuel when glucose levels are low
SPECIFICALLY, the liver produces ketone bodies w/in the mitochondria & are used by the brain and heart as fuel
one POTENTIAL SOURCE of seizures disorders is __ __ __ (← def.)
specifically, it is the classification of brain malformation where there is abnormal …
one POTENTIAL source of seizures disorders is focal cortical dysplasia (clumps of abnormal neuronal cells in the cortex)
specifically, it is the classification of brain malformation where there is abnormal post-migration cortical reorganization
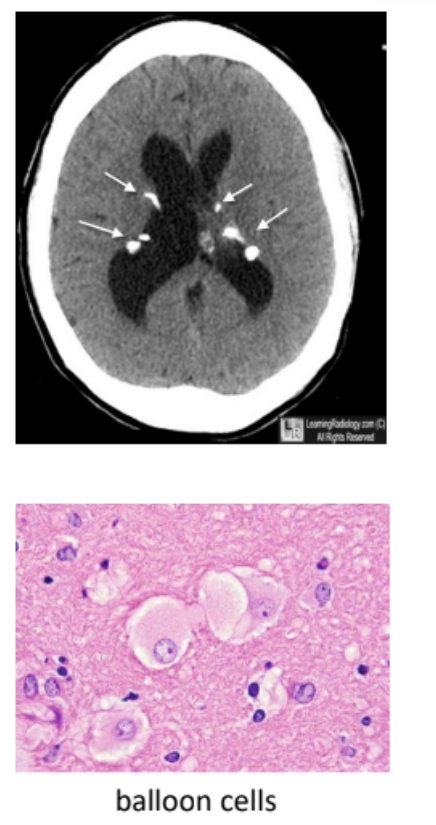
tuberous sclerosis is a type of cortical dysgenesis w/ abnormal cells, which are non-neoplastic
t/f: it refers to the abnormal formation of the cortex due to disruptions in:
cell growth/proliferation
differentiation
migration
cortical organization
def.
describe (1 ← def. term)
symptoms (3)
true
__
a rare autosomal dominant disorder that is secondary to mutations in the TSC1 and TSC2 tumor suppressor genes
associated with formation of hamartomas (non-cancerous tumors)
symptoms:
seizures
autism
intellectual disability
how are iPSCs (induced pluripotent stem cells) made?
where the starting specific type of cells are added together with (#) __ __( ← name them)
iPSCs can differentiate in 6 possible types of cells (← name them)
t/f: gene editing can control what type of neurons that iPSCs differentiate into
a method is used to reprogram / de-differentiate human somatic cells that are fully differentiated back into a stem cell-like state called induced pluripotent stem cells
where the fully-differentiated adult somatic cells are added together with 4 Yamanaka factors: Oct4, Sox2, Klf4, c-Myc
iPSCs can differentiate in 6 possible types of cells:
blood cells
pancreatic cells
motoneurons
dopamine-producing neurons
adipocytes
cardiomyocytes
true
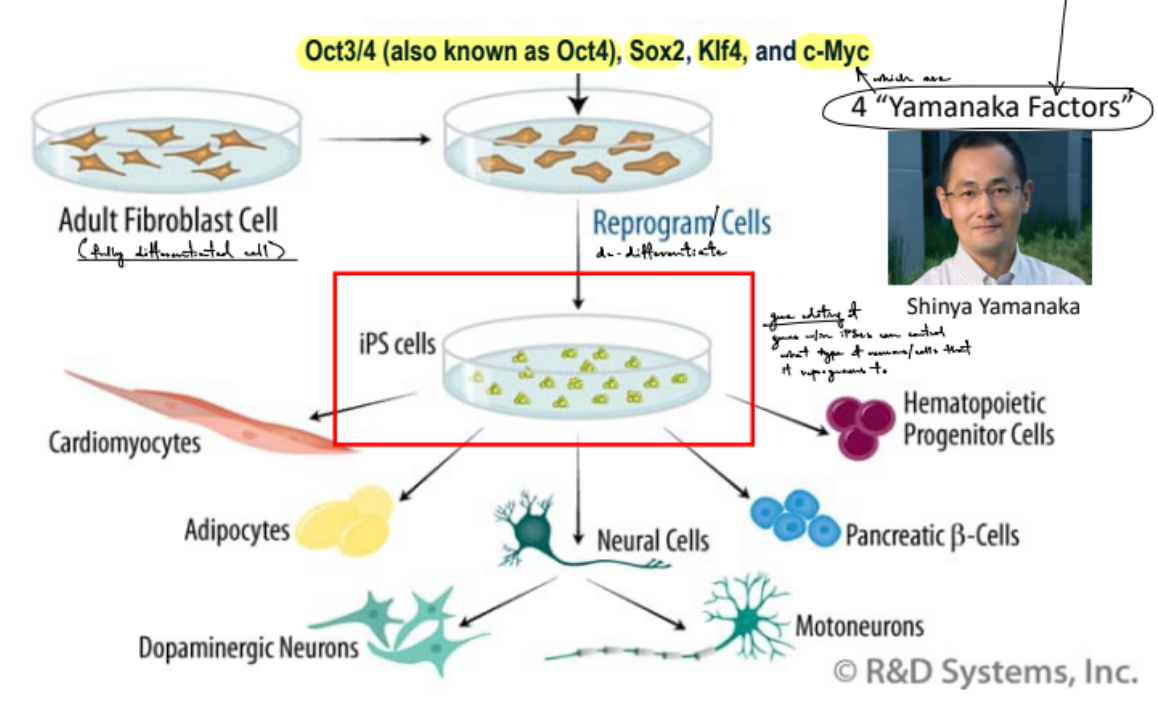
for gene editing can control what type of neurons that iPSCs differentiate into
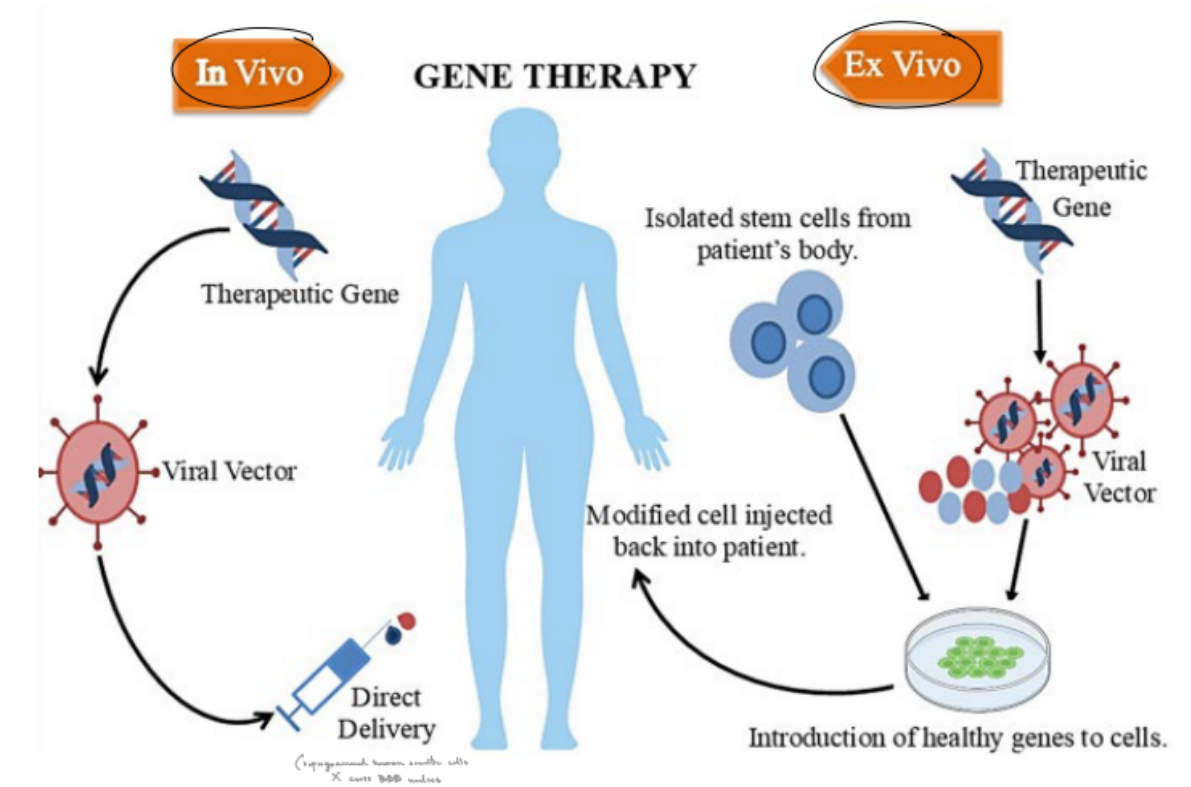
name the 2 types of gene therapies
describe each
t/f: gene editing, like CRISPR, can be used to treat diseases in humans
in vivo (done inside the body)
gene turns into a viral vector, which is then directly delivered
ex vivo (done outside the body, then injected)
gene turns into a viral vector, where the viral vector & isolated stem cells from the patient will come together to get a modified cell, which is then injected back into the patient
_
true
first successful case done last year in an infant w/ CPS1 deficiency
def. intellectual disability (ID)
def. the 2 things that are limited
another name for 1 of them
for the other one, describe the 3 aspects to it
IQ tests are done to measure intellectual functioning, where IQ of below __ indicates significant limitation in intellectual functioning
standardized tests are used to measure limitations in __ __
ID — condition where there is significant limitations in intellectual functioning & adaptive behavior before the age of 22
intellectual functioning aka intelligence — general mental capacity for learning, problem solving, etc.
adaptive behavior — the conceptual, social, and practical skills that are done by people in their daily lives
conceptual skills — language, money, time, etc. (← things we understand)
social skills — interpersonal skills, self-esteem, follow rules, etc. (← interacting with others & the social norms)
practical skills — personal care, healthcare, routines, etc. (← application of things we know)
IQ tests are done to measure intellectual functioning, where IQ of below 70 indicates significant limitation in intellectual functioning
standardized tests are used to measure limitations in adaptive function
for the genetics & underlying cellular properties of ASD and/or ID
t/f: All human traits emerge from an interaction of genes and environment
_
ID and ASD (autism spectrum disorder) are divided into 2 forms (← name & def. each)
for 1 of them, give 2 examples
__
for ID:
the causes usually unknown, but the known causes are divided into 2 categories (← name & describe each)
true
_
ID and ASD (autism spectrum disorder) are divided into:
syndromic forms — ID and/or ASD is associated w/ other detectable anomalies / medical/behavioral signs and symptoms
ex: Down syndrome, fragile X syndrome
non-syndromic forms — ID and/or ASD appear w/o other detectable anomalies
__
for ID:
the causes usually unknown, but the known causes are divided into 2 categories:
environmental exposures
most common is fetal alcohol syndrome (mother exposed to/consumed alcohol while pregnant)
genetic abnormalities
most common chromosomal abnormality is Down’s syndrome
most common gene mutation is Fragile X syndrome
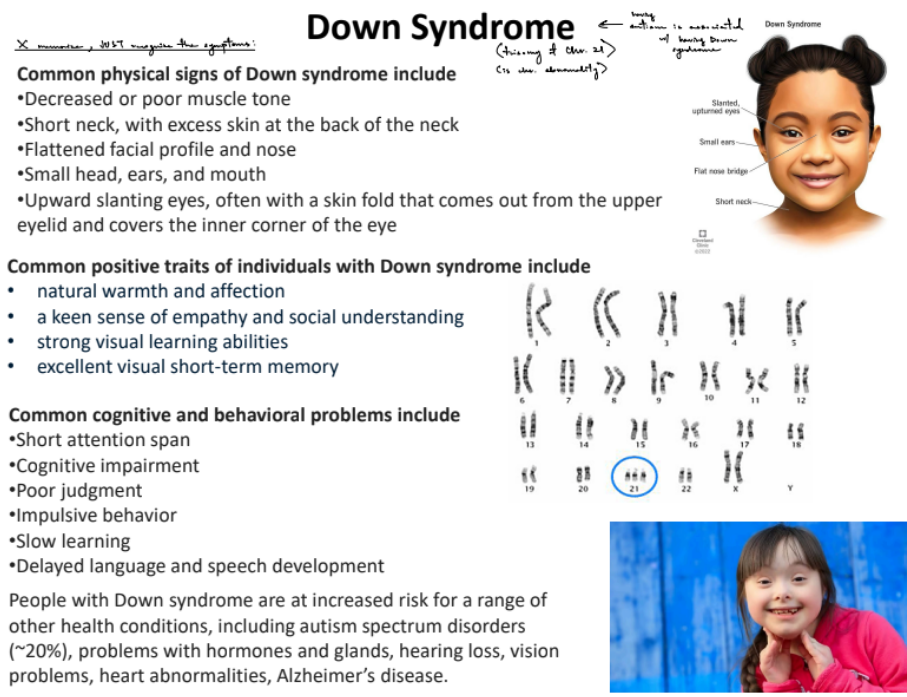
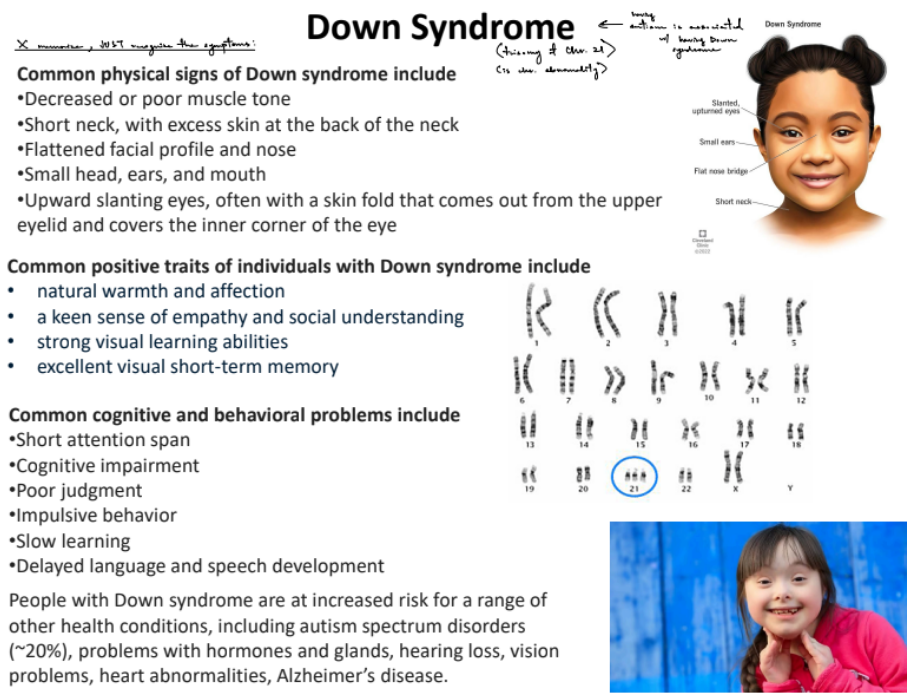
for Down’s syndrome
Down’s syndrome is syndromic to ASD and/or ID, where Down’s syndrome is a __ __, specifically a very common __ __
…
just recognize the below parts & picture:
t/f: common physical signs include short neck, small head, flattened facial features, skin fold coming out from the upper eyelid
t/f: common positive traits include natural affection, empathy, good short-term memory
t/f: common cog./behavioral problems are short attention span, impulsive behavior, delayed language & speech dev.
t/f: people w/ Down’s syndrome are at increased risk for other health conditions, like ASD
Down’s syndrome is syndromic to ASD and/or ID, where Down’s syndrome is a genetic abnormality, specifically a very common chromosomal abnormality (b/c have trisomy Ch. 21)
all 4 are true
for Rett syndrome
Rett syndrome is syndromic to ASD and/or ID, where Rett syndrome is a __ __, specifically a very common __ __ __
most cases are caused by mutations in the MeCP2 gene, which is located on the _ chromosome
SO Rett syndrome is more common in __ b/c …
t/f: is also associated with ASD symptoms
Rett syndrome is syndromic to ASD and/or ID, where Down’s syndrome is a genetic abnormality, specifically a very common single gene mutation
most cases are caused by mutations in the MeCP2 gene, which is located on the X chromosome
SO Rett syndrome is more common in females b/c males will die before birth
true
for ASD (autism spectrum disorder)
characterized by (2)
more common in __, where ratio used to be higher b/c …
…
def. disorder vs. condition
def. ASD in terms of disorder vs. condition
relate to neurodivergence
char. by:
persistent deficits/lacks in social communication & interaction
restricted, repetitive behavior, interests, or activities
more common in males, where ratio used to be higher b/c didn’t account for sex differences where girls easily mask social inabilities & they also changed the qualities that diagnose ASD
…
disorder — deviation from the norm, has negative connotation
condition — state of being, is less stigmatized
…
ASD as a disorder — moderate to severe ASD interferes w/ daily life
ASD as a condition — mild ASD is not necessarily disruptive to daily life
neurodivergence: individuals w/ ASD process the world differently from neurotypical individuals (other ex: ADHD, OCD, etc.)
def. DSM-5
published by who, when
next edition expected to be published b/w __ and __
…
is the persistent deficits/lack in social comm. and iteraction across multiple contexts, name 3 general social deficits
diagnostic & statistical manual on mental disorders 5th edition (by APA, in 2013)
next edition b/w 2023-2028
…
deficit in social-emotional reciprocity
deficit in nonverbal communication
deficit in developing, maintaining, and understanding relationships
for ASD (cont.)
t/f: people w/ ASD have a large range of intellectual abilities
explain
ASD is a __ __ __; they are not made up of discrete/fixed subcategories
meaning?
…
autism is not caused by 1 mech, BUT by a family of neurodev. processes that __ on __ brain circuit formation that occurs during __ and __ __development
t/f: autism is highly genetically heterogenous
the key biology involves brain development, esp. __ and __
many autism-linked genes converge on a relatively __ number of cellular pathways
t/f: environ. factors may contribute in some cases through interaction w/ genetics/biology
true
range from extreme intellectual disability (extreme ID) to extraordinary intellectual abilities/specialized talents
ASD is a single heterogenous spectrum; they are not made up of discrete/fixed subcategories
meaning that ASD is a spectrum (of severity of effects) that is caused by different genetic abnormalities
…
autism is not caused by 1 mech, BUT by a family of neurodev. processes that converge on altered brain circuit formation that occurs during fetal and early postnatal development
true ← autism is highly genetically heterogenous
the key biology involves brain development, esp. synapses and circuits
many autism-linked genes converge on a relatively small number of cellular pathways
true
for ASD (cont.)
t/f: ASD often has several common co-morbidities
def. co-morbid vs. syndromic
…
ASD has a strong genetic component w/ heterogenous causes, including specifically __ & __ (← what do they stand for? & def. 1 of them)
state the genetic heterogenous causes of ASD (6)
where ~ ½ variants are __, while other ½ are __
true
co-morbid — 2 (distinct) medical conditions that occur in a person at the same time
syndromic — collection of symptoms that often occur together & are linked to ONE genetic disease or cause
…
ASD has a strong genetic component w/ heterogenous causes (aka strong genetic heterogenous spectrum), including specifically CNVs (copy number variants) & SNVs (single nucleotide variants)
genetics
common variants
rare inherited CNVs
rare inherited SNVs
de novo CNVs
de novo SNVs
where ~ ½ variants are heritable/inherited, while other ½ are environmental
__
CNVs (copy number variants) — parts of chromosome are deleted or duplicated
genes ass. w/ ASD are often involved in __ brain development
__
Why do we know so much more about genes compared to the environment when it comes to ASD & ID? (3)
__
ASD is ass. w/ a range of _(3)_natal factors, where the highest magnitude associations are with __ __ use & neonatal __
__
we are confident that autism is NOT caused by childhood vaccines & SO we can conclude that …
evidence for strong genetic component to autism (2)
t/f: autism can be diagnosed earlier and earlier
give example of this & explain
__
syndromes ass. w/ ASD can be __ (due to __) or the result of __
genes ass. w/ ASD are often involved in early brain development
__
the environment includes a very broad range of factors
the exposure to environmental factors are often transient (short / temporary)
studies to look at environ. factors are too expensive & time-consuming
__
ASD is ass. w/ a range of prenatal, perinatal, and postnatal factors, where the highest magnitude associations are with maternal medication use & neonatal seizures
__
we are confident that autism is NOT caused by childhood vaccines & SO we can conclude that correlation b/w childhood vaccines & developmental abnormalities are NOT the same as causation
evidence:
twin studies: identical twins are likely to get it if the other has it; BUT likelihood for fraternal twins is the same chance as w/ non-twin siblings
animal & human studies: changes in brain circuit ass. w/ autism genes occur in utero/prenatal or in early perinatal developmental period
true
use eye tracking in young children, where visual preference for geometric shapes is an early biomarker/indicator of an ASD subtype w/ more severe symptoms
__
syndromes ass. w/ ASD can be monogenic (due to SNVs) or the result of CNVs
use syndromic ASD to study cellular mechanisms underlying ASD b/c we know the genetic causes
one of the syndromic forms of ASD and/or ID: fragile X syndrome (FXS)
fragile X syndrome (FXS) is the most common __ cause of ID and ASD
def. FXS
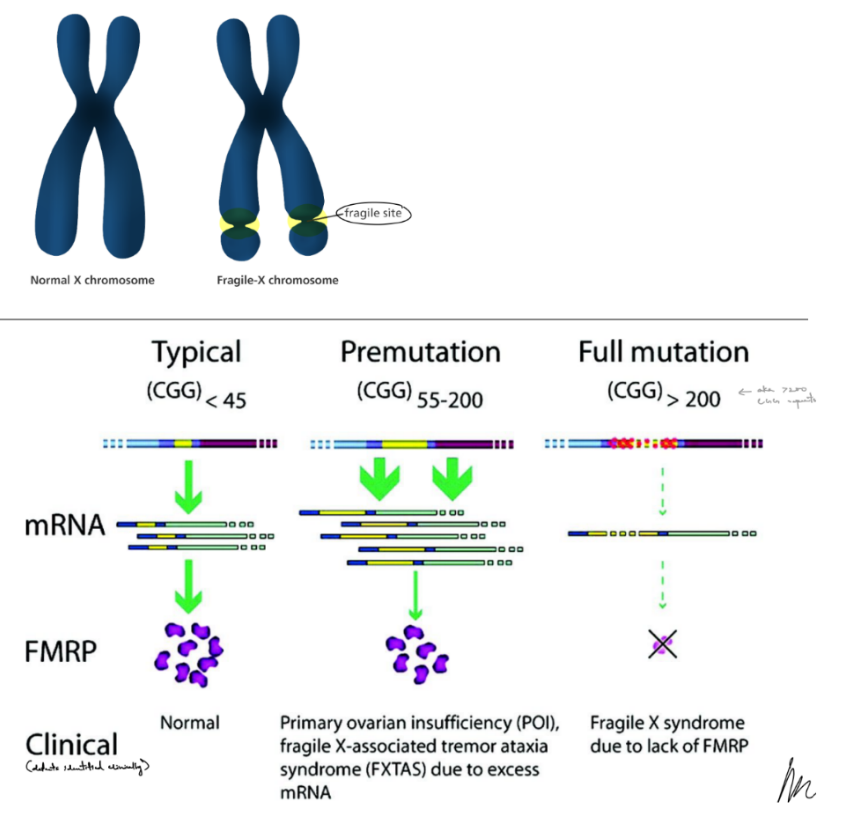
is caused by a __ __in the gene __ that encodes for (1), SO have __ of __ expression ← is what causes Fragile X syndrome
what are the 3 states depending on the amount of the specific trinucleotide repeats?
symptoms (5)
draw out how it looks like
fragile X syndrome is the most common hereditary cause of ID and ASD
a trinucleotide repeat expansion disease of CGG
is caused by gene mutation of gene FMR1 that encodes for the Fragile X Messenger ribonuclear protein (FMRP), SO have lack of FMRP expression
^ the lack of FMRP protein expression is what causes Fragile X syndrome
typical (→ get normal FMRP expression), premutation (→ have some defects), mutation (→ lack of FMRP expression)
symptoms:
ASD
ID
enlarged testicle
flat feet
seizures (in ~10% of patients)